
Abstract
Purpose
Intestinal decompression using self-expandable metallic colonic stents (SEMSs) as a bridge to surgery is now considered an attractive alternative to emergency surgery. However, data regarding the optimal timing of surgery after stenting are limited.
Methods
We investigated the impact of the interval between stenting and surgery on short- and long-term outcomes in 92 obstructive colorectal cancer (OCRC) patients who had a SEMS inserted and subsequently received curative surgery.
Results
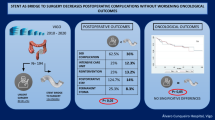
The median age of the patients was 70.5 years, and the median interval between SEMS insertion and the surgery was 17 (range 5–47) days. There were 35 postoperative complications, including seven major postoperative complications. An interval of more than 16 days was an independent predictor of a poor relapse-free survival (hazard ratio [HR] = 3.12, 95% confidence interval [CI] 1.24–7.81, p = 0.015). An interval of more than 35 days was independently associated with major postoperative complications (HR = 16.6, 95% CI 2.21–125, p = 0.006).
Conclusion
A longer interval between stenting and surgery significantly compromised the short- and long-term outcomes. Surgery within 16 days after stenting might help maximize the benefit of SEMS without interfering with short- and long-term outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) is one of the most frequent cancers in the world. In 2020, an estimated 1.9 million new cases were diagnosed, and nearly 935,000 patients died of the disease, accounting for the second-highest mortality rate [1]. Up to 30% of CRC patients present with intestinal obstruction [2], and obstructive colorectal cancer (OCRC) has been shown to account for 85% of colonic emergencies [3]. OCRC was previously treated with emergency surgery, which often required multiple-stage surgery and carried high morbidity and stoma rates. However, intestinal decompression using self-expandable metallic colonic stent (SEMS) as a bridge to surgery (BTS) is now considered an attractive alternative [4]. The decompression allows for bowel preparation, medical stabilization with correction of dehydration and electrolyte abnormalities, and optimization of comorbid illnesses, which theoretically improves the bowel condition as well as patients’ nutrition and inflammatory status. Thus, patients can undergo elective one-stage surgery with reduced morbidity and stoma rates compared to emergency surgery [5, 6].
Intestinal decompression using self-expandable metallic colonic stents (SEMSs) was originally used with palliative intent [7] due to concerns about short-term complications and the long-term survival. In the guideline of the European Society of Gastrointestinal Endoscopy (ESGE) published in 2014, SEMS placement as a BTS was not recommended as a standard treatment of symptomatic left-sided malignant colonic obstruction [8]. The guideline was updated in 2020, and SEMS placement as a BTS is now regarded as a viable treatment option in patients with potentially curable left-sided obstructing colon cancer as an alternative to emergency resection [4]. However, data regarding the optimal timing of surgery after stenting have been limited, although the ESGE guideline weakly recommends a two-week interval [4].
In this study, the impact of the interval between stenting and surgery on short- and long-term outcomes was evaluated in OCRC patients who received SEMS placement followed by curative surgery.
Methods
This was a retrospective study of 92 consecutive OCRC patients who received SEMS placement as a BTS at Sendai City Medical Center between 2013 and 2020. The patients had total or subtotal malignant colonic obstruction characterized by the following symptoms and findings: (1) obstructive symptoms, such as abdominal pain, fullness, vomiting, and constipation; (2) contrast-enhanced computed tomography (CT) findings of colorectal tumor with dilation of the proximal bowel; and (3) severe stricture or obstruction demonstrated by contrast enema and colonoscopy.
Patients were excluded if there were signs of peritonitis, perforation, or other serious complications demanding urgent surgery. Patients with benign disease, distant metastasis, positive surgical margin, and invasion from a non-colonic malignancy were also excluded from the study. There were no patients with chronic inflammation, and none of the patients were administered neoadjuvant chemoradiation therapy.
The protocol for this retrospective research project was approved by the Ethics Committee of the institution with a waiver of informed consent (#2021-0032), and it conforms to the provisions of the Declaration of Helsinki.
The severity of obstruction was evaluated using ColoRectal Obstruction Scoring System (CROSS) which assigns a point score based on the patient’s oral intake level: CROSS 0, requiring continuous decompression; CROSS 1, no oral intake; CROSS 2, liquid or enteral nutrient intake; CROSS 3, soft solids, low residue, and full diet with symptoms of stricture; and CROSS 4, soft solids, low residue, and full diet without symptoms of stricture [9].
Insertion of the SEMS was performed by experienced endoscopists. A guidewire was introduced across the neoplastic stenosis under endoscopic and fluoroscopic guidance. A Niti-S colonic stent (TaeWoong Medical, Gimpo-si, Korea) or HANAROSTENT (Boston Scientific, Tokyo, Japan) was deployed over the wire and through the scope without balloon dilatation. The colon proximal to the stenosis was evaluated by water-soluble contrast enema, and a colonoscopic examination was performed after the surgery. A colonoscopic examination had not been performed before the surgery for fear of damaging both the fragile bowel and the colonoscope. Just recently, we started performing a colonoscopic examination of the proximal bowel through the SEMS before surgery.
All patients subsequently underwent curative surgical resection. Postoperative complications were classified according to the Clavien–Dindo (CD) classification [10]. Pathological tumor staging was done according to the AJCC cancer staging manual (7th edition) [11]. Colonic lesions proximal to the splenic flexure were defined as right-sided tumors. Long-term outcomes were defined as the relapse-free survival (RFS) and overall survival (OS). The RFS was measured from the date of the surgery to the date of disease recurrence, and the OS was measured from the date of the surgery to the date of death due to any cause.
Continuous variables were presented as the median (range) and tested using the Mann–Whitney U test. Categorical variables were evaluated in a cross-table using Fisher's exact test. The cut-off values were determined using receiver operating characteristic (ROC) curve analyses. The cut-off value was determined using the most prominent point on the ROC curve (Youden index = maximum [sensitivity − (1 − specificity)]), and the area under the ROC (AUROC) curve was also calculated. A multivariate analysis was performed with logistic regression. The survival rate was determined according to the Kaplan–Meier method and analyzed by the log-rank test. A multivariate analysis was performed using a Cox proportional hazards model. Factors shown to have a p value of < 0.1 in the univariate analysis were included in the multivariate analysis.
EZR (Saitama medical center, Jichi medical university, Saitama, Japan), a graphical user interface for R (The R foundation for statistical computing, Vienna, Austria), was used for statistical analyses, and differences with p values < 0.05 were considered significant [12].
Results
The characteristics of the 92 OCRC patients are summarized in Table 1. There were 54 males and 38 females. The median age of the patients was 70.5 (range 37–93) years, and the median follow-up time was 30 (range 1–98) months. The tumor was located on the left in 68 (73.9%) cases and on the right in 24 cases. The median interval between SEMS insertion and the surgery was 17 (range 5–47) days (Fig. 1). The attending surgeons decided on the timing of the surgery, based mainly on the patient’s condition. The availability of a surgical team and operating room were also considered, as with other elective surgeries. There were 12 cases in which the interval was more than 30 days. Reasons for a prolonged interval were as follows: treatment of both pseudomembranous colitis and aspiration pneumonia, coronary angiography for the evaluation of coronary artery disease, and treatment of an impaired pulmonary function in one case each, and colonoscopic polypectomy in two cases. Other patients were merely scheduled without any specific reasons.

Histogram of the bridging interval of 92 obstructive colorectal cancer patients
Laparoscopic surgery was performed in 40 (43.5%) cases, with conversion to open procedure required in 4 cases (10.0%) due to severe adhesion in 3 and the tumor having direct invasion to the bladder in 1. These patients were included in the laparoscopic group in the subsequent analyses. The remaining 52 cases (56.5%) were treated with an open surgical approach. Concerning the CROSS classification, 52 patients (56.5%) were CROSS 0, 7 (7.6%) were CROSS 1, 10 (10.9%) were CROSS 2, and 23 (25.0%) were CROSS 3.
Regarding SEMS insertion, the technical success rate, defined as correct placement, was 100%, and the clinical success rate, defined as the resolution of occlusive symptoms, was 98.9%. There were two stenting-related complications: one patient complained of mild abdominal pain after SEMS placement, and another with inadequate drainage required insertion of a transanal decompression tube for additional drainage.
Eighty-two patients (89.1%) underwent curative resection with primary anastomosis. A stoma was created in ten patients, including five diverting stomas. There were 35 (38.0%) postoperative complications including seven major postoperative complications (CD grade ≥ III). There was one in-hospital death secondary to anastomotic leakage. The median postoperative hospital stay was 15.5 (range 8–77) days. Adjuvant chemotherapy was administered to 47 cases (51.1%).
When the RFS was used as the end-point, an ROC curve analysis revealed the optimal cut-off value for the interval between stenting and surgery to be 16 days, which provided a sensitivity of 52%, specificity of 77%, and AUROC of 0.59. There were 52 cases (56.5%) in the D ≥ 16 group. Kaplan–Meier survival curves demonstrated that the RFS was significantly shorter in the D ≥ 16 group than in the D < 16 group (p = 0.003; Fig. 2). The OS was not statistically different between the groups (p = 0.70). The relationship between the D ≥ 16 group and the clinicopathological parameters of the 92 patients is shown in Table 2. The D ≥ 16 status was significantly associated with a laparoscopic approach (p = 0.011). Other clinicopathological factors, recurrence patterns, and postoperative complications were comparable between the groups.

Survival curves of 92 obstructive colorectal cancer patients according to the interval between stenting and surgery. The relapse-free survival (a) was significantly shorter in the D ≥ 16 group than in the D < 16 group. The overall survival (b) was not significantly different between the groups
Regarding the RFS, univariate analyses revealed a D ≥ 16 status (p = 0.005), ASA ≥ 2 (p = 0.030), and CA 19–9 ≥ 37 (p = 0.002) to be significantly poor prognostic factors (Table 3). In a multivariate analysis, not receiving adjuvant chemotherapy (p = 0.055 in the univariate analysis) was also included in the model. The result showed that a D ≥ 16 status (hazard ratio [HR] = 3.12, 95% confidence interval [CI] 1.24–7.81, p = 0.015), CA19-9 ≥ 37 (HR = 4.10, 95% CI 1.61–10.44, p = 0.003), and not receiving adjuvant chemotherapy (HR = 2.43, 95% CI 1.05–5.59, p = 0.037) were independent poor prognostic factors.
When major complications (CD Grade ≥ III) were used as the end-point, an ROC curve analysis revealed the optimal cut-off value for the interval between stenting and surgery to be 35 days, which provided a sensitivity of 95%, specificity of 43%, and AUROC of 0.56. There were 7 cases (7.6%) in the D ≥ 35 group. The RFS was significantly shorter in the D ≥ 35 group than in the D < 35 group (p = 0.033), whereas the OS was not statistically different between the groups (p = 0.38). A D ≥ 35 status was significantly associated with a laparoscopic approach (p = 0.040), major postoperative complications (p = 0.008), and anastomotic leakage (p = 0.028). Other clinicopathological factors and postoperative hospital stay were comparable between the groups (Table 4).
Regarding major postoperative complications, the only factor identified as a significant predictor in the univariate analysis was D ≥ 35 status (p = 0.003). An operative time of more than 240 min (p = 0.051) was marginally significant. In a multivariate analysis, only a D ≥ 35 status (HR = 16.6, 95% CI 2.21–125, p = 0.006) was an independent predictor of major postoperative complications (Table 5).
Discussion
Patients with OCRC usually undergo emergency surgery, which is associated with increased morbidity and mortality rates. It often results in multiple-stage surgery along with the creation of a stoma. The stoma is permanent in up to 40% of cases and significantly diminishes patients’ quality of life (QOL) [13]. Furthermore, performing surgery emergently might lead to oncologically suboptimal resection [14]. Endoscopic decompression using SEMS can convert emergency surgery into elective one-stage surgery and is considered an attractive alternative [4]. Over the last decade, a number of studies, including randomized control trials (RCTs) and meta-analyses, have advanced our understanding of SEMS used as a BTS, generally supporting the feasibility of this approach [3, 5, 6]. However, data regarding the optimal interval between stenting and surgery and its impact on short- and long-term outcomes have been limited.
In this study, a D ≥ 16 status was an independent predictor of a poor RFS. Kye et al. [15] demonstrated that the interval between stenting and surgery was an independent predictor of the RFS and OS in 174 Stage II and III OCRC patients. An interval of more than 8 days was significantly associated with a poor RFS, and an interval of more than 14 days was significantly associated with a poor OS. Broholm et al. [16] revealed that an interval of more than 18 days was significantly associated with recurrence. In contrast, a Dutch multicenter study of 182 OCRC cases showed that the bridging interval was not associated with the 3-year RFS or OS [17]. Our results were in line with the former two studies and demonstrated that a longer interval was associated with a worse RFS.
SEMSs mechanically dilate malignant stricture, prompting concerns about recurrence and the long-term survival. SEMSs are associated with overt and silent perforation [6], and their insertion has been shown to increase the viable circulating tumor cell count [18], cytokeratin 20 mRNA [19], cell-free DNA, and circulating tumor DNA levels in peripheral blood [20]. SEMSs are also associated with perineural invasion [21, 22]. A meta-analysis of five RCTs demonstrated that SEMS placement as a BTS significantly increased the overall and systemic recurrence compared to emergency surgery. The risk of locoregional recurrence was not markedly different between the groups [23]. However, these worrisome findings might not directly translate to a poor prognosis, and multiple meta-analyses have shown that the long-term outcomes of SEMS placement were comparable to those of emergency surgery when used as a BTS [3, 5, 6, 23] and as palliative therapy [24]. Compared with patients treated with a transanal decompression tube, no statistically significant differences were observed concerning recurrence patterns and the long-term survival [25]. The present findings suggest that the detrimental effects of SEMS on oncological outcomes might become apparent after 16 days.
A D ≥ 35 status was significantly associated with major postoperative complications and anastomotic leakage. Aside from anastomotic leakage, conditions graded as CD ≥ III complications were arterial thrombus of the lower extremity, intraabdominal abscess, and ileus. The results of previous studies regarding the association between the interval and complications were inconclusive. Matsuda et al. [26] reported that a short interval of less than 15 days was associated with postoperative complications. Lee et al. [27] found that all cases with anastomotic leakage underwent surgery within 10 days after stenting. A multicenter observational study of 312 participants demonstrated that the interval was not associated with anastomotic leakage, with a median interval of 16 days [28]. Two studies with more than 150 BTS cases showed no significant differences between bridging interval and postoperative complications [15, 17]. In this study, a D ≥ 35 status was the only independent predictor for severe postoperative complications, but the underlying mechanism was unclear, as the status was not associated with any clinicopathological parameters. Theoretically, a longer bridging interval should improve the bowel condition and result in a decreased risk of anastomotic leakage. In addition, a longer may provide more opportunities for the general condition of the patients to improve. Further studies are warranted to confirm the relationship between the interval and postoperative complications and elucidate the underlying mechanisms.
There was a historical change in our management of OCRC cases (Table S1). When SEMS placement was introduced in our institution in 2013, all OCRC cases were treated with an open surgical approach. The number of cases treated via a laparoscopic approach gradually increased as we developed expertise in laparoscopic surgery. In recent years, increasing numbers of patients are temporarily discharged after stenting and undergo preoperative evaluations on an outpatient basis. As a result, recent cases are more likely to undergo laparoscopic colectomy with a longer interval after stenting. Furthermore, more patients with a CROSS score of three have been treated with SEMS in recent years. Adjuvant chemotherapy was administered to nearly half of the patients in our study throughout the study period, but the administration of oxaliplatin-containing regimens was significantly increased, chiefly due to the update of the Japanese guideline in 2019 [29]. These historical changes in our management might have affected the present results, and the presence of unrevealed high-risk factors cannot be ruled out. However, clinically important variables were included in the multivariate analysis, and the year of the operation or intensity of the chemotherapy did not affect the results (data not shown).
The limitations of this study included its retrospective nature with a small sample size and non-randomized design. The median follow-up time of 30 months was also too short to draw definitive conclusions regarding long-term oncological outcomes.
In summary, the results of the present study demonstrated that a longer interval between stenting and surgery was significantly associated with poor short- and long-term outcomes in OCRC patients treated in a BTS setting. Surgery within 16 days after stenting might maximize the benefit of SEMS placement without interfering with short- and long-term outcomes.
References
The Global Cancer Observatory. 2020. https://gco.iarc.fr/ Accessed 6 June 2021.
McCullough JA, Engledow AH. Treatment options in obstructed left-sided colonic cancer. Clin Oncol. 2010;22:764–70.
Matsuda A, Miyashita M, Matsumoto S, et al. Comparison of long-term outcomes of colonic stent as “bridge to surgery” and emergency surgery for malignant large-bowel obstruction: a meta-analysis. Ann Surg Oncol. 2015;22:497–504.
van Hooft JE, Veld JV, Arnold D, Beets-Tan RGH, Everett S, Götz M, et al. Self-expandable metal stents for obstructing colonic and extracolonic cancer: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—update 2020. Endoscopy. 2020;52:389–407.
Arezzo A, Passera R, Lo Secco G, Verra M, Bonino MA, Targarona E, et al. Stent as bridge to surgery for left-sided malignant colonic obstruction reduces adverse events and stoma rate compared with emergency surgery: results of a systematic review and meta-analysis of randomized controlled trials. Gastrointest Endosc. 2017;86:416–26.
Allievi N, Ceresoli M, Fugazzola P, Montori G, Coccolini F, Ansaloni L. Endoscopic stenting as bridge to surgery versus emergency resection for left-sided malignant colorectal obstruction: an updated meta-analysis. Int J Surg Oncol. 2017;2017:2863272.
Dohomoto M. New method-endoscopic implantation of rectal stent in palliative treatment of malignant stenosis. Endosc Dig. 1991;3:1507–12.
van Hooft JE, van Halsema EE, Vanbiervliet G, Beets-Tan RG, DeWitt JM, Donnellan F, European Society of Gastrointestinal Endoscopy, et al. Self-expandable metal stents for obstructing colonic and extracolonic cancer: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2014;46:990–1053.
Matsuzawa T, Ishida H, Yoshida S, Isayama H, Kuwai T, Maetani I, et al. A Japanese prospective multicenter study of self-expandable metal stent placement for malignant colorectal obstruction: short-term safety and efficacy within 7 days of stent procedure in 513 cases. Gastrointest Endosc. 2015;82:697–707.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, et al. AJCC cancer staging manual. 7th ed. New York: Springer; 2010.
Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013;48:452–8.
Frago R, Ramirez E, Millan M, Kreisler E, del Valle E, Biondo S. Current management of acute malignant large bowel obstruction: a systematic review. Am J Surg. 2014;207:127–38.
Gainant A. Emergency management of acute colonic cancer obstruction. J Visc Surg. 2012;149:e3-10.
Kye BH, Kim JH, Kim HJ, Lee YS, Lee IK, Kang WK, et al. The optimal time interval between the placement of self-expandable metallic stent and elective surgery in patients with obstructive colon cancer. Sci Rep. 2020;10:9502.
Broholm M, Kobborg M, Frostberg E, Jeppesen M, Gögenür I. Delay of surgery after stent placement for resectable malignant colorectal obstruction is associated with higher risk of recurrence. Int J Colorectal Dis. 2017;32:513–6.
Veld JV, Kumcu A, Amelung FJ, Borstlap WAA, Consten ECJ, Dekker JWT, et al. Time interval between self-expandable metal stent placement or creation of a decompressing stoma and elective resection of left-sided obstructive colon cancer. Endoscopy. 2020. https://doi.org/10.1055/a-1308-1487.
Yamashita S, Tanemura M, Sawada G, Moon J, Shimizu Y, Yamaguchi T, et al. Impact of endoscopic stent insertion on detection of viable circulating tumor cells from obstructive colorectal cancer. Oncol Lett. 2018;15:400–6.
Maruthachalam K, Lash GE, Shenton BK, Horgan AF. Tumour cell dissemination following endoscopic stent insertion. Br J Surg. 2007;94:1151–4.
Takahashi G, Yamada T, Iwai T, Takeda K, Koizumi M, Shinji S, et al. Oncological assessment of stent placement for obstructive colorectal cancer from circulating cell-free DNA and circulating tumor DNA dynamics. Ann Surg Oncol. 2018;25:737–44.
Haraguchi N, Ikeda M, Miyake M, Yamada T, Sakakibara Y, Mita E, et al. Colonic stenting as a bridge to surgery for obstructive colorectal cancer: advantages and disadvantages. Surg Today. 2016;46:1310–7.
Kim HJ, Choi GS, Park JS, Park SY, Jun SH. Higher rate of perineural invasion in stent-laparoscopic approach in comparison to emergent open resection for obstructing left-sided colon cancer. Int J Colorectal Dis. 2013;28:407–14.
Foo CC, Poon SHT, Chiu RHY, Lam WY, Cheung LC, Law WL. Is bridge to surgery stenting a safe alternative to emergency surgery in malignant colonic obstruction: a meta-analysis of randomized control trials. Surg Endosc. 2019;33:293–302.
Ribeiro IB, Bernardo WM, Martins BDC, de Moura DTH, Baba ER, Josino IR, et al. Colonic stent versus emergency surgery as treatment of malignant colonic obstruction in the palliative setting: a systematic review and meta-analysis. Endosc Int Open. 2018;6:E558–67.
Sato R, Oikawa M, Kakita T, Okada T, Oyama A, Abe T, et al. Comparison of the long-term outcomes of the self-expandable metallic stent and transanal decompression tube for obstructive colorectal cancer. Ann Gastroenterol Surg. 2019;3:209–16.
Matsuda A, Miyashita M, Matsumoto S, Sakurazawa N, Kawano Y, Yamada T, et al. Optimal interval from placement of a self-expandable metallic stent to surgery in patients with malignant large bowel obstruction: a preliminary study. Surg Laparosc Endosc Percutan Tech. 2018;28:239–44.
Lee GJ, Kim HJ, Baek JH, Lee WS, Kwon KA. Comparison of short-term outcomes after elective surgery following endoscopic stent insertion and emergency surgery for obstructive colorectal cancer. Int J Surg. 2013;11:442–6.
Saito S, Yoshida S, Isayama H, Matsuzawa T, Kuwai T, Maetani I, et al. A prospective multicenter study on self-expandable metallic stents as a bridge to surgery for malignant colorectal obstruction in Japan: efficacy and safety in 312 patients. Surg Endosc. 2016;30:3976–86.
Hashiguchi Y, Muro K, Saito Y, Ito Y, Ajioka Y, Hamaguchi T, et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int J Clin Oncol. 2020;25:1–42.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We have no conflict of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Sato, R., Oikawa, M., Kakita, T. et al. A longer interval after stenting compromises the short- and long-term outcomes after curative surgery for obstructive colorectal cancer. Surg Today 52, 681–689 (2022). https://doi.org/10.1007/s00595-021-02385-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-021-02385-4