
Abstract
Background
The use of a tibial stem for large deformities (> 10°) would reduce the incidence of pain. The aim of this study was to compare the effect of tibial stem on postoperative pain and aseptic loosening at the tibia in patients with a preoperative deformity > 10° in the frontal plane at 2 years follow-up.
Methods
This was a retrospective single-center case–control study. Ninety-eight patients with deformities greater than 10° in the frontal plane and a BMI > 30 kg/m2 who had undergone posterior-stabilized (PS) total knee arthroplasty (TKA) with a tibial stem were matched using a propensity score to 98 patients who had undergone PS TKA without a tibial stem. The primary endpoint was the pain rate at 2 years. The secondary endpoints were the rate of aseptic loosening of the tibia at 2 years post-operatively.
Results
A significant difference was found in the rate of postoperative pain at 2 years. It was higher in the group without tibial stem compared with the group with tibial stem (41.8% vs 17.3%, p = 0.0003). In the group without tibial stem, 24.4% of pain was mild, 61% moderate and no severe pain. In the tibial stem group, 47.1% of pain was mild, 41.2% moderate and no severe pain. A radiolucent line (RLL) was present at 2 years in 26.5% of prostheses in the without tibial stem group and in 9.2% of prostheses in the tibial stem group (p = 0.002).
There was no difference between the two groups in terms of aseptic loosening.
Conclusion
The use of a tibial stem in primary TKA in patients with frontal deformities greater than 10° reduces postoperative pain and the presence of radiolucent lines.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The annual number of total knee arthroplasties (TKA) continues to increase [1, 2]. This is due to an aging population [3] and an increase in the prevalence of obesity. In 2014, 14% of the world’s population was obese [3].
Despite the forgotten goal of total knee arthroplasty [4], depending on the study, up to 30% of postoperative pain persists [5] and approximately 10% of primary TKA require revision [6]. The two main causes of revision, apart from sepsis, are aseptic loosening (mainly of the tibia) and pain of no etiology [6]. Long-term pain [7] is partially explained [6] and has multifactorial causes [5, 8]. Some of this pain is of mechanical origin [9]. Little research has been done on preoperative frontal deformities greater than 10°. To date, no study has shown a correlation between the size of the preoperative deformity and postoperative pain [10, 11].
The incidence of tibial stems in primary TKA is increasing [12] with increasingly well-defined indications. It could reduce the rate of aseptic loosening in obese patients [13, 14], osteoporotic patients [15] and in frontal deformities greater than 8° [16]. Recently, an analysis from an Australian registry found that primary stemmed TKA had lower rates of all-cause revision beyond 1.5 years [17]. The relationship between pain and the presence or absence of a tibial stem was not observed in these studies for deformities greater than > 10°.
Tibial stems allow epiphyseal stresses to be transferred to metaphyseal–diaphyseal stresses [18, 19], thereby reducing tibial micromovements at the bone–cement interface [20]. This improved stress distribution would reduce the rate of aseptic loosening, which is particularly high in severe varus due to the high mechanical stresses [21, 22]. No study has reported the effect of a tibial stem on pain or the rate of aseptic loosening in patients with severe preoperative deformity.
The aim of this study was to compare the effect of a tibial stem on postoperative pain and aseptic loosening of the tibia in patients with a preoperative frontal plane deformity of > 10° at 2-year follow-up.
Our hypothesis was that the presence of a tibial stem would reduce the rate of painful patients and the rate of aseptic loosening due to a better distribution of stress.
Materials and methods
Study design and population
This is a single-center retrospective cohort study conducted between January 2018 and December 2019 at Lariboisière Hospital. All patients who had a primary posterior-stabilized TKA HIFIT (Ceraver, France) for primary gonarthrosis and preoperative frontal deformity greater than 10° were included. After 2018, all patients with a deformity greater than 10° in frontal plane had a tibial stem. This series was matched using a propensity score to a historical cohort of patients with the same characteristics but without a tibial extension stem.
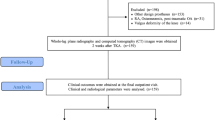
Of the 367 patients who underwent TKA for primary gonarthrosis with a preoperative deformity greater than 10°, we excluded 269 patients because of a follow-up of less than 2 years or because of a constitutional pathology (Fig. 1). After matching, 196 patients were included in the final analysis, 144 (73.5%) of whom were women. 90 (45.9%) patients underwent right knee surgery. The mean age was 68.4 years ± 8798, the mean body mass index (BMI) was 35.8 kg/m2 ± 7605, and the preoperative deformity was 196° ± 4.2.

Flow chart
Surgical procedure
The approach used was a medial parapatellar approach, with subperiosteal release of the medial collateral ligament and systematic resection of the central pivot. In order to achieve mechanical alignment, the cuts were guided by navigation (Orthokey, Miro, Italy), first in the femur and then in the tibia. Ligament balance was checked by external maneuvers and via navigation after fitting the trial implants. All implants were cemented with Palacos® genta bone cement, and the patellas resurfaced with an ultra-high molecular weight polyethylene patellar button.
A tibial extension stem, 50 mm long and of variable diameter (10–19 mm), could be fitted according to the surgeons’ habits; they were usually cemented proximally and not cemented distally.
Peri- and intraoperative pain relief was provided by a locoregional femoral analgesic block combined with a Naropin catheter removed at Day 3, and local Ropivacaine infiltration. The patients were also placed in a Game Ready® splint (analgesic cryotherapy) immediately after the operation and mobilized from Day 0 using a Kinetec® type knee arthromotor. Postoperative care was identical for all patients without immobilization and an early rehabilitation program with immediate post-operative full weight bearing on the operated limb with crutches, and educational therapy provided by a physiotherapist. Patients were reviewed in consultation with a full radiological check-up (face, profile, and EOS) at 3, 12 and 24 months and then annually.
Judging criteria
The primary outcome was the presence or absence of pain at the 2-year follow-up visit. If pain was present, it was asked to the patient to classify into 4 categories: mild, moderate, severe, and neurogenic.
Secondary endpoints were the rate of appearance of a radiolucent line on the tibia and the rate of revision surgery at 2 years post-operatively. Radiolucent line was defined as the presence of an evolving radiolucent image at the prosthesis–cement interface or bone cement of more than 2 mm or tilting of the tibial implant in zones 1–5 as defined by the Modern Knee Society Radiographic Evaluation System [23,24,25]. This radiolucent line did not have to be present on the immediate postoperative X-ray and was monitored independently by two investigators at the last follow-up.
Statistical analysis
To match the two groups and limit the impact of external factors and any potential selection bias, a propensity score matching method was applied. A propensity score was calculated considering the patient’s age at surgery, BMI, pre-operative deformity and gender. Each patient who had TKA with tibial stem was matched with a patient who had TKA without tibial stem in a 1:1 ratio. Matching was performed using a logit scale with a calibration of 0.2. For the descriptive analysis of discrete variables, we used frequencies and percentages; for continuous variables, we used the mean and standard deviation. For comparative analysis, a Fischer’s exact test was used for percentages and a Wilcoxon test for continuous variables. Kaplan–Meier analysis was used to analyze TKA survival. The significance level was 5%, with a power of 80% and a risk of the first kind at 5%. R software (version 3.5.0) was used for statistical analysis (https: //www.r-project.org/).
Results
Population characteristics
Each group consisted of 98 matched patients. The groups were similar with respect to age (68.43 ± 7.886 vs 68.36 ± 9.664; p = 0.77), BMI (35.11 ± 6.87 vs 36.49 ± 8.252; p = 0.11), male/female distribution (74.5% vs 72.4%; p = 0.87) and type of deformation (for varus, 90.8% vs 86.7%, p = 0.50). There was still a difference between the two groups in terms of preoperative deformity (13.42° vs 15.79°, respectively, in the group without tibial stem and with tibial stem; p = 0.0001). All demographic data for the two groups are summarized in Table 1.
Pain at 2 years post-operatively
Pain was present in 41.8% of patients in the group without tibial stem and only 17.3% in the tibial stem group (p = 0.0003, Fig. 2). In the group without tibial stem, there was 24.4% mild pain, 61% moderate pain, 14.6% neurogenic pain and no severe pain. In the tibial stem group, there was 47.1% mild pain, 41.2% moderate pain, 11.8% neurogenic pain and no severe pain. There was no difference between the two groups in the type of pain (p = 0.24, Table 2).

A plot showing the percentage of pain at final follow-up between the group with a tibial stem versus the group without tibial stem. Blue represents patient with no pain at final follow-up and red patients with pain at final follow-up
Radiolucent lines and revision surgery rates at 2 years post-operatively
A radiographic radiolucent line was present at 2 years in 26.5% prostheses in the group without tibial stem and in only 9.2% prostheses in the tibial stem subgroup (p = 0.002, Table 2). The location was 26.9% external tibial, 65.4% internal and 7.7% in both compartments in the group without tibial stem. The location was again predominantly internal in the tibial stem group, with 88.9% internal and 11.1% external. A difference was found between the two groups on survival analysis regarding the appearance of radiolucent lines in favor of the group with tibial stem (p < 0.01, Fig. 3).

Survival curve of radiolucent lines between tibial stem group and group without tibial stem. Y-axis represented survival rate (from 100 to 0%) and X-axis time in years. The plain black line represents the group without a tibial stem, and the red broken line represents the group with a tibial stem
There was no aseptic loosening at two years in either group. There was one revision for synthesis in the group without tibial stem for peri-prosthetic fracture and one revision by rotative hinge knee in the tibial stem group for posterior dislocation. There was no significant difference in the rate of revision surgery at 2 years between the two groups (p = 0.9, Fig. 4).

Survival curve of revision between tibial stem group and group without tibial stem. Y-axis represented survival rate (from 100 to 0%) and X-axis time in years. The plain black line represents the group without a tibial stem, and the red broken line represents the group with a tibial stem
Discussion
The aim of this study was to show that the addition of a tibial stem to primary TKAs in large frontal deformities reduces pain. The secondary objective was to show a reduction in aseptic loosening of the tibia and, consequently, a reduction in the number of radiological radiolucent lines.
There was a significant difference in pain between the two groups, with 41.8% of patients in the group without tibial stem and only 17.3% in the tibial stem group (p = 0.0003). This difference was particularly noticeable for moderate pain, with 25 patients in the group without tibial stem compared with 7 in the tibial stem group. Extension stem with metaphyseal support appears to be a limiting factor in postoperative pain.
The rate of aseptic loosening of the tibial component in our study was comparable between the two groups. In fact, our study found no aseptic loosening at two years in either the extension stem group or the no stem group. The rate of aseptic loosening found in the literature is mainly studied at 5 years [26]. Piedade et al. [27], who evaluated the causes of keelless TKR failure at 5 years, found an aseptic loosening rate of 2%. Hinman et al. [28] who matched 10,476 TKRs without and with stems found a rate of 0.32% and 1.4%, respectively, at 5 years. According to Sharkey et al. [29], aseptic loosening occurs more frequently from two years after the insertion of a TKR without a keel, at which point the risk of aseptic loosening is multiplied by 2.5. Recently, an analysis from Australian registry observed that primary stemmed TKA have lower rates of all-cause revision beyond 1.5 years [17].
There was therefore no early loosening in our study, but it is possible that we do not have enough hindsight to determine the rate of aseptic loosening in the longer term.
An important aspect of our study concerns the radiolucent lines which are less present in the group without tibial stem than in the tibial stem group, respectively, 26.5% versus 9.2% (p = 0.002). These results, in patients with a large preoperative frontal deformity, are in line with the results of the literature. In particular, Completo et al. [30] suggest a reduction in micromovements of the implant and a distribution of forces from the cortical and cancellous bone to the stem or, more simply, from a proximal epiphyseal load to a distal diaphyseal load. As a reminder, 20% load transfer for Completo et al. [31] and, earlier, 30% for Rawlinson et al. [32] and Murase et al. [33].
The choice of implants and the addition of a stem was determined by the surgeon’s experience and not by randomization, but this had no negative impact on the distribution of the numbers.
Complications were similar in the two groups before matching: one infection in the group without tibial stem versus two in the tibial stem group, one periprosthetic fracture in the group without tibial stem versus one in the tibial stem group, two knee stiffnesses in the group without tibial stem, none in the tibial stem group, one dislocation in the tibial stem group. Complications are correlated with the results of the literature and we found no difference in mechanical complications or early loosening (defined as less than 2 years).
Although the use of keels is associated with more complications, pain at the end of the stem [34] and the risk of peri-prosthetic fracture due to excessive load transfer to the diaphysis [31]. This risk is found above all in diaphyseal-supported prostheses. Nor were there any complications during revision surgery due to bone loss associated with metaphyseal-supported stems, as there was no revision surgery in our study.
The advantages of this study are the large cohort, with 98 patients in each group and no patients lost to follow-up, and comparable groups in terms of both pre-operative and post-operative data. Preoperatively, the patients were comparable according to gender, age and BMI.
However, according to Ritter et al. [22] large and very large preoperative deformities increase the risk of aseptic loosening, as do Oh et al. [35] who also distinguish varus > 15°. Thus, the increase in varus in the keel group reinforces the results of this study on loosening, edging and pain.
This study has several limitations, the first of which are the retrospective nature of the study, the absence of randomization, the limited follow-up date of two years and, finally, an indication bias for the choice of adding a stem.
Another limitation is that reading introduces a classification bias, as explained by Bach et al. [24]; the interpretation of X-rays is observer-dependent and not very reproducible. As described by Chalmers et al. [23] the analysis of an evolving radiolucent line of sufficient size to obtain optimum sensitivity.
A final limitation is the assessment bias associated with pain data collection. Our data collection was initially based on a VAS-type scale, grouped into 4 categories and not into a score such as the KSS like similar studies concerning tibial extension stems [36, 37]. However, according to Boeckstyns and Backer [38] who compared the knee pain questionnaire with a simple VAS pain scale, the latter was more effective in characterizing pain. There is no memory bias since the data collected were radiological and the pain assessment objective.
It is therefore necessary to continue the follow-up in order to confirm our current results, all the more so as these results are in line with the literature on both edging and pain [13, 39].
In the literature, Park et al. [39] found 3.9% of aseptic loosening at 11 years in patients with a varus deformity greater than 8° without an extension stem, but none in the group with a stem. The result may be altered by the recruitment bias of this study, in which the population was predominantly female and of Asian origin only, which is not the case in our study. Similarly, Fournier et al. [13] found an aseptic loosening rate of 3% in patients with a deformity greater than 10° without an extension stem at two years.
It should be noted that our group of patients had an average BMI of 35.8 kg/m2, 35.11 kg/m2 in the group without tibial stem and 36.49 kg/m2 in tibial stem group, with a twofold increase in the risk of aseptic loosening according to Abdel et al. [40]. According to Parratte et al. [36], the figure of 3% of aseptic loosening in patients with severe obesity without a stem compared with 0 with an extension stem at two years.
The use of tibial stem for aseptic loosening has not been widely described in the literature, except in the case of revision surgery. According to Lachiewicz and Soileau [41], the use of a cemented 3 cm tibial extension stem in revision TKA allows implant stability to be obtained despite defects; they found no aseptic loosening in their series, a result to be weighed against the fact that the cohort was small. Similarly, Fehring et al. [15] found no aseptic loosening in 107 patients with a cemented tibial extension stem. However, Angers-Goulet and Bédard [42] who followed 91 patients with complex TKRs (BMI > 35 kg/m2, ligament instability or bone defects) over 7 years, found no aseptic loosening and confirm the advantage of using cemented tibial stems in complex TKRs.
Thus, despite insufficient follow-up, our study is consistent with the literature and its 10-year follow-up concerning the very low rate, or even absence, of aseptic tibial loosening in TKA with tibial extension stem, but it should be continued.
About pain, this study showed a reduction in pain in the tibial stem group, with a reduction mainly in moderate pain. Tibial stems allow epiphyseal stresses to be transferred to metaphyseal–diaphyseal stresses [18, 19] and thus reduce tibial micromovements at the bone/cement interface [20]. Perhaps, this better distribution of stresses would reduce the pain.
Although pain at the distal end of the stem has been described [20]. The literature distinguishes between metaphyseal and diaphyseal stems and reports more pain in diaphyseal stems [43]. Our study involved TKRs with metaphyseal-supported stems and hybrid cementing. The absence of pain suggestive of pain on the tip of the stem is probably due to their short length (5 cm), the type of cementing [44] to the fact that there is no conflict with the cortex and therefore no constraint on the positioning of the tibial implant (anteroposterior or mediolateral) and to better load distribution [45].
There are few studies in the literature examining the link between extension stems in primary TKA and pain, which is included in composite scores. According to our study, stem would reduce pain in obese patients with a large deformity at 2 years and would require prolonged follow-up to see if this difference persists.
About radiolucent lines, given the absence of loosening, no link between the two could be established in this study. Few studies have looked for a correlation between extension stems in primary TKA and radiolucent lines. Angers-Goulet and Bédard [42], in their study of complex TKAs (defined above), found a lower incidence of radiolucent lines in TKAs with stem. Kajetanek et al. [37], in their study of mini-stems in the minimally invasive approach, observed a correlation between radiolucent lines and aseptic loosening. It may be assumed that there is a relationship between these lines and aseptic loosening, but further follow-up of these patients is required.
Conclusion
The addition of a tibial stem to primary TKRs in frontal deformities greater than 10° reduces postoperative pain and the presence of radiolucent lines at 2 years postoperatively. Prolonged follow-up is required to determine whether these results are maintained over the long term and whether this is associated with a reduction in aseptic loosening. We recommend to use of a short tibial stem for primary TKA with an initial frontal deformation > 10° to reduce pain.
Data availability
Data are available on requests.
References
Kurtz S, Ong K, Lau E et al (2007) Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am 89:780–785. https://doi.org/10.2106/JBJS.F.00222
Erivan R, Tardieu A, Villatte G et al (2020) Knee surgery trends and projections in France from 2008 to 2070. Orthop Traumatol Surg Res 106:893–902. https://doi.org/10.1016/j.otsr.2020.02.018
World Health Organization (2016) World health statistics 2016: monitoring health for the SDGs, sustainable development goals. World Health Organization, Geneva
Lange T, Schmitt J, Kopkow C et al (2017) What do patients expect from total knee arthroplasty? a delphi consensus study on patient treatment goals. J Arthroplast 32:2093-2099.e1. https://doi.org/10.1016/j.arth.2017.01.053
Wylde V, Beswick A, Bruce J et al (2018) Chronic pain after total knee arthroplasty. EFORT Open Rev 3:461–470. https://doi.org/10.1302/2058-5241.3.180004
Sadoghi P, Liebensteiner M, Agreiter M et al (2013) Revision surgery after total joint arthroplasty: a complication-based analysis using worldwide arthroplasty registers. J Arthroplast 28:1329–1332. https://doi.org/10.1016/j.arth.2013.01.012
Petersen KK, Arendt-Nielsen L (2016) Chronic postoperative pain after joint replacement. Pain 24:1–6
Lewis GN, Rice DA, McNair PJ, Kluger M (2015) Predictors of persistent pain after total knee arthroplasty: a systematic review and meta-analysis. Br J Anaesth 114:551–561. https://doi.org/10.1093/bja/aeu441
Iwaki H, Pinskerova V, Freeman MA (2000) Tibiofemoral movement 1: the shapes and relative movements of the femur and tibia in the unloaded cadaver knee. J Bone Joint Surg Br 82:1189–1195. https://doi.org/10.1302/0301-620x.82b8.10717
Teeny SM, Krackow KA, Hungerford DS, Jones M (1991) Primary total knee arthroplasty in patients with severe varus deformity. A comparative study. Clin Orthop Relat Res 273:19–31
Lee B-S, Lee S-J, Kim J-M et al (2011) No impact of severe varus deformity on clinical outcome after posterior stabilized total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 19:960–966. https://doi.org/10.1007/s00167-010-1316-9
Gililland JM, Gaffney CJ, Odum SM et al (2014) Clinical & radiographic outcomes of cemented vs. diaphyseal engaging cementless stems in aseptic revision TKA. J Arthroplasty 29:224–228. https://doi.org/10.1016/j.arth.2014.03.049
Fournier G, Muller B, Gaillard R et al (2020) Increased survival rate for primary TKA with tibial short extension stems for severe varus deformities at a minimum of 2 years follow-up. Knee Surg Sports Traumatol Arthrosc 28:3780–3786. https://doi.org/10.1007/s00167-020-05848-2
Druel J, Gelin N, Ollivier M et al (2024) Outcomes of short and long tibial stems for primary total knee arthroplasty in a population of obese patients at two-year follow-up: a clinical and biomechanical study. J Arthroplast S0883–5403(24):00146–00153. https://doi.org/10.1016/j.arth.2024.02.047
Fehring TK, Odum S, Olekson C et al (2003) Stem fixation in revision total knee arthroplasty: a comparative analysis. Clin Orthop Relat Res. https://doi.org/10.1097/01.blo.0000093032.56370.4b
Walsh CP, Han S, Canham CD et al (2019) Total knee arthroplasty in the osteoporotic tibia: a biomechanical evaluation of the role of stem extensions and cementing techniques. J Am Acad Orthop Surg 27:370–374. https://doi.org/10.5435/JAAOS-D-17-00736
Osan JK, Harris IA, Harries D et al (2024) Utilizing stems in primary total knee arthroplasty: analysis of the Australian orthopaedic association national joint replacement registry data. J Arthroplast 39:1692–1698. https://doi.org/10.1016/j.arth.2024.01.031
Filip AC, Cuculici SA, Cristea S et al (2022) Tibial stem extension versus standard configuration in total knee arthroplasty: a biomechanical assessment according to bone properties. Medicina 58:634. https://doi.org/10.3390/medicina58050634
Kwon HM, Hong H-T, Kim I et al (2024) Biomechanical effects of stem extension of tibial components for medial tibial bone defects in total knee arthroplasty: a finite element study. J Knee Surg. https://doi.org/10.1055/a-2344-5084
Scott CEH, Biant LC (2012) The role of the design of tibial components and stems in knee replacement. J Bone Joint Surg Br 94:1009–1015. https://doi.org/10.1302/0301-620X.94B8.28289
Ritter MA, Faris GW, Faris PM, Davis KE (2004) Total knee arthroplasty in patients with angular varus or valgus deformities of > or = 20 degrees. J Arthroplasty 19:862–866. https://doi.org/10.1016/j.arth.2004.03.009
Ritter MA, Davis KE, Davis P et al (2013) Preoperative malalignment increases risk of failure after total knee arthroplasty. J Bone Joint Surg Am 95:126–131. https://doi.org/10.2106/JBJS.K.00607
Chalmers BP, Sculco PK, Fehring KA et al (2017) A novel percentage-based system for determining aseptic loosening of total knee arthroplasty tibial components. J Arthroplast 32:2274–2278. https://doi.org/10.1016/j.arth.2017.02.020
Bach CM, Steingruber IE, Peer S et al (2001) Radiographic assessment in total knee arthroplasty. Clin Orthop Relat Res. https://doi.org/10.1097/00003086-200104000-00022
Meneghini RM, Mont MA, Backstein DB et al (2015) Development of a modern knee society radiographic evaluation system and methodology for total knee arthroplasty. J Arthroplast 30:2311–2314. https://doi.org/10.1016/j.arth.2015.05.049
Ahn JH, Back YW (2013) Comparative study of two techniques for ligament balancing in total knee arthroplasty for severe varus knee: medial soft tissue release vs. bony resection of proximal medial tibia. Knee Surg Relat Res 25:13–18. https://doi.org/10.5792/ksrr.2013.25.1.13
Piedade SR, Pinaroli A, Servien E, Neyret P (2009) Revision after early aseptic failures in primary total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 17:248–253. https://doi.org/10.1007/s00167-008-0667-y
Hinman AD, Prentice HA, Paxton EW, Kelly MP (2021) Modular tibial stem use and risk of revision for aseptic loosening in cemented primary total knee arthroplasty. J Arthroplast 36:1577–1583. https://doi.org/10.1016/j.arth.2020.11.003
Sharkey PF, Lichstein PM, Shen C et al (2014) Why are total knee arthroplasties failing today–has anything changed after 10 years? J Arthroplast 29:1774–1778. https://doi.org/10.1016/j.arth.2013.07.024
Completo et al (2008) The influence of different tibial stem designs in load sharing and stability at the cement-bone interface in revision TKA. Knee 15(3):227–32
Completo A, Simões JA, Fonseca F, Oliveira M (2008) The influence of different tibial stem designs in load sharing and stability at the cement-bone interface in revision TKA. Knee 15:227–232. https://doi.org/10.1016/j.knee.2008.01.008
Rawlinson JJ, Peters LE, Campbell DA et al (2005) Cancellous bone strains indicate efficacy of stem augmentation in constrained condylar knees. Clin Orthop Relat Res 440:107–116. https://doi.org/10.1097/01.blo.0000187340.10003.68
Murase K, Crowninshield RD, Pedersen DR, Chang TS (1983) An analysis of tibial component design in total knee arthroplasty. J Biomech 16:13–22. https://doi.org/10.1016/0021-9290(83)90042-8
Patel AR, Barlow B, Ranawat AS (2015) Stem length in revision total knee arthroplasty. Curr Rev Musculoskelet Med 8:407–412. https://doi.org/10.1007/s12178-015-9297-4
Oh S-M, Bin S-I, Kim J-Y et al (2019) Impact of preoperative varus deformity on postoperative mechanical alignment and long-term results of “mechanical” aligned total knee arthroplasty. Orthop Traumatol Surg Res 105:1061–1066. https://doi.org/10.1016/j.otsr.2019.04.016
Parratte S, Ollivier M, Lunebourg A et al (2017) Do stemmed tibial components in total knee arthroplasty improve outcomes in patients with obesity? Clin Orthop Relat Res 475:137–145. https://doi.org/10.1007/s11999-016-4791-6
Kajetanek C, Bouyer B, Ollivier M et al (2016) Mid-term survivorship of Mini-keel™ versus Standard keel in total knee replacements: differences in the rate of revision for aseptic loosening. Orthop Traumatol Surg Res 102:611–617. https://doi.org/10.1016/j.otsr.2016.05.007
Boeckstyns MEH, Backer M (1989) Reliability and validity of the evaluation of pain in patients with total knee replacement. Pain 38:29–33. https://doi.org/10.1016/0304-3959(89)90069-9
Park M-H, Bin S-I, Kim J-M et al (2018) Using a tibial short extension stem reduces tibial component loosening after primary total knee arthroplasty in severely varus knees: long-term survival analysis with propensity score matching. J Arthroplast 33:2512–2517. https://doi.org/10.1016/j.arth.2018.03.058
Abdel MP, Bonadurer GF, Jennings MT, Hanssen AD (2015) Increased aseptic tibial failures in patients with a bmi ≥35 and well-aligned total knee arthroplasties. J Arthroplast 30:2181–2184. https://doi.org/10.1016/j.arth.2015.06.057
Lachiewicz PF, Soileau ES (2015) A 30-mm cemented stem extension provides adequate fixation of the tibial component in revision knee arthroplasty. Clin Orthop Relat Res 473:185–189. https://doi.org/10.1007/s11999-014-3529-6
Angers-Goulet M, Bédard M (2017) Up to seven years’ follow-up of short cemented stems in complex primary total knee arthroplasty: a prospective study. Knee 24:1166–1174. https://doi.org/10.1016/j.knee.2017.05.010
Barrack RL, Stanley T, Burt M, Hopkins S (2004) The effect of stem design on end-of-stem pain in revision total knee arthroplasty. J Arthroplast 19:119–124. https://doi.org/10.1016/j.arth.2004.06.009
McLean AJ (2007) Effect of modular stems and cement fixation techniques on the initial stability of the tibial prosthesis and the strain distribution within the proximal tibia in primary and revision total knee arthroplasty
Completo A, Talaia P, Fonseca F, Simões JA (2009) Relationship of design features of stemmed tibial knee prosthesis with stress shielding and end-of-stem pain. Mater Des 30:1391–1397. https://doi.org/10.1016/j.matdes.2008.06.071
Funding
There is no funding source.
Author information
Authors and Affiliations
Contributions
R. Nizard and P. Bizot were involved in the surgery procedures. Data collection was performed by JA. Bourdier and J. Descamps. Formal analysis of data was performed by PA. Bouche and G. Odri. The first draft of the manuscript was written by JA Bourdier and PA. Bouche. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declares that there is no conflict of interest in this work.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Regional Ethics Committee of Asturias, Spain. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to Participate
All patients gave their consent to participate to the study.
Consent to publish
All authors gave their consent to publish the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bourdier, JA., Bouché, PA., Descamps, J. et al. The use of a tibial stem in primary total knee arthroplasty for patients with a frontal deformity of more than ten degrees reduces the rate of postoperative pain. Eur J Orthop Surg Traumatol 34, 3233–3240 (2024). https://doi.org/10.1007/s00590-024-04052-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-024-04052-z