
Abstract
Goals of work
The goal of this study is to explore the characteristics of tumor-free cancer survivors (CSs) who after their primary treatment were still working but made work changes due to cancer and compare them to survivors who did not.
Patients and methods
The sample consisted of 431 CSs (219 females with breast cancer, 212 males with testicular (N = 150) or prostate cancer (N = 62)) diagnosed 2–6 years prior to the study. All CSs had good prognosis and had returned to work after primary treatment. All CSs filled in a mailed questionnaire covering demography, morbidity, life style, mental distress, fatigue, quality of life and job strain.
Results
Seventy-two CSs (17%) had made work changes due to cancer during the observation period, and 359 (83%) had not. Among CSs who made work changes, significantly more were females; they showed significantly poorer physical and mental work ability, worked fewer hours per week, reported more comorbidity, and had lower physical and mental quality of life and more neuroticism, compared to the nonchange group. Work changes were moderately correlated with current work ability.
Conclusions
The majority of CSs did not report any work changes due to cancer during the 2–6-year observation period, which is an encouraging finding. A minority had done work changes, and this group consisted mainly of women and was also characterized by poorer physical and mental quality of life and poorer mental work ability due to cancer. The issue of work changes and work ability should be considered in the follow-up of cancer survivors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Recent improvement of prognosis of cancer due to more effective treatment has increased the population of cancer survivors (CSs), and many of them are at work when they get cancer. To illustrate, among 24,228 Norwegian patients diagnosed with cancer in 2005, 37% (males 4,113; females 4,824) were aged from 25 to 64 years and thus within the working period of their life cycle [6]. As the employment rates in Norway for person in this age range were approximately 83% for males and 76% for females in 2005 [22], we can conclude that a large proportion of cancer patients are holding jobs at the time of diagnosis and primary treatment.
The diagnosis and treatment of cancer can lead to side effects, late effects, and psychological distress that reduce the mental and physical health of CSs, either temporarily or permanently. Work ability (WA) can be defined as an individual’s physical, psychological, and social resources for participation in any kind of paid work or self-employment. WA is dependent on mental and somatic health status as well as on social skills, level of education, work demands, the work environment, and the organization of the work [15–17, 25, 39, 41]. According to Ilmarinen and Tuomi [16, 22], three sets of work-related factors have a significant impact on WA: physical work demands, hazardous work environment, and poorly organized work. In this perspective, WA is based on a balance between the individual’s resources and the demands at the workplace [16, 19].
Taskila and Lindbohm [36] published an overview of 12 studies on employment and WA in CSs. They concluded that most CSs were able to continue working, but there was a subgroup who suffered from impaired health that sometime implied reduced WA. A study from Finland [38] compared WA of CSs to a matched control group without cancer and found that WA of CSs overall did not differ from that of the controls, but the more diseases people had the poorer was their WA. Among CSs, 26% reported impaired physical WA and 19% impaired mental WA, and these results are in line with other studies [3, 4, 10, 24, 29].
To sum up, CSs are usually able to return to work after the primary treatment, but their WA ability can be reduced and eventually become insufficient in relation to their current job [28, 32, 33]. Thus reduced WA could lead to work changes, but no studies of such changes in CSs were known to us. The present study, therefore, explores characteristics of CSs who had made work changes due to cancer in a sample of Norwegian patients primarily treated for breast, prostate, and testicular cancer with good prognosis and without recurrence and distant metastases. The observation period for changes was from 2 to 6 years after diagnosis and treatment. The characteristics of those who changed their work situation due to cancer (change group) were compared to those who did not (nonchange group). The strength of associations between variables significantly associated with work changes in univariable analyses were tested in multivariable analyses. Finally, the relationship between work changes and current WA was explored.
Patients and methods
This study is a part of a Nordic project carried out by the Nordic Study Group of Cancer and Work Life (NOCWO) which aimed to examine the living conditions and work situation of tumor-free cancer survivors living in Denmark, Finland, Iceland, and Norway. The eligibility criteria of the NOCWO study were: (1) first cancer diagnosis between 25 and 57 years of age; the upper age limit was chosen in order to avoid approaching the age of natural pensioning too much; (2) primary treatment finished 2 to 6 years prior to the survey (between 1998 and 2002); (3) no evidence of any malignant disease or distant metastases after primary treatment (except basocellular skin cancer); and (4) all cancer surgery and chemotherapy had been terminated, although ongoing adjuvant systemic hormone treatment was allowed.
Procedures and response rates
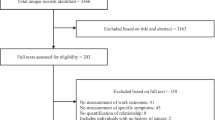
In 2004, a questionnaire covering demography, morbidity, life style, mental distress, fatigue, quality of life, impact of cancer, and job strain was mailed to 852 eligible CSs who had been treated at the Norwegian Radium Hospital in Oslo. The sample invited consisted of 427 females with breast cancer and 425 males with prostate cancer (N = 110) or testicular cancer (N = 315; Fig. 1) [10, 11]. Breast cancer is the most common form of cancer in females and affects both younger and older females. Because there is no type of cancer in males with a prevalence and age distribution corresponding to breast cancer, the age spectrum in males was covered by including testicular cancer (younger men) and prostate cancer (older men) [12].

Flowchart of subjects and recruitment. Cancer survivors
The number of patients who accepted the invitation and returned valid questionnaires was 513 (response rate 60%), among which 431 (84%) had returned to work after primary treatment. The working sample consisted of 212 males with testicular (N = 150) or prostate (N = 62) cancer and 219 females with breast cancer.
An attrition analysis of nonresponding (N = 339) and responding (N = 513) CSs did not show any statistically significant difference as to age at survey, gender, cancer diagnosis, stage, and treatment modalities. The nonresponders were younger at the time of diagnosis (p = 0.02) and had longer intervals from the diagnosis to the survey (p = 0.002). These differences were not clinically significant because the effect sizes were 0.08 and 0.11, respectively [31].
Treatment issues
All survivors with breast cancer had stage I disease and was treated with local surgery (either mastectomy (N = 58) or lumpectomy without axillary lymph node dissection (N = 161)), which was followed by radiotherapy in case of lumpectomy. After mastectomy, no radiotherapy was applied, but dependent on clinical stage, histological grade, and/or hormone receptor status of the tumor tissue, adjuvant chemotherapy, hormone treatment, and/or regional lymph node irradiation were given.
Survivors with prostate cancer had either retropubic radical prostatectomy (N = 20) or high-dose pelvic radiotherapy (N = 42), which in high-risk patients (N = 23) was combined with adjuvant hormone treatment for 3 years. Depending on the type of tumor and staging, survivors with testicular cancer had either entered into a surveillance program (N = 26), had infradiaphragmatic radiotherapy (N = 49), or had received chemotherapy (N = 75) followed by resection of residual masses.
Measurements
Nordic and Norwegian questionnaire on cancer and work
Under the direction of the Finnish Institute of Occupational Health, NOCWO developed a common Nordic questionnaire to be used in all countries. The questionnaire was based on several valid and reliable international and national measures in order to cover relevant issues concerning work in general, somatic and mental health, and work consequences of cancer. In addition, the Norwegian sample included a national questionnaire covering other socioeconomic-, social-participations-, and more work-related issues.
Change in the work situation due to cancer
The Nordic questionnaire contained five questions covering work changes namely concerning employer, occupation, work tasks, unemployment, or pensioning. In case of an affirmative answer to any of these questions, a second question then asked if the change was due to cancer. The change group was defined as those CSs who scored “Yes, partially” or “Yes, mainly” on any of the “due to cancer” items. Those who rated “No” on all the work change items or rated their changes as “not due to cancer” were defined as the nonchange group. Based on these definitions, we identified 72 CSs reporting various work changes due to cancer (change group), and 359 survivors who reported no work changes or changes not due to cancer (nonchange group).
Background variables
The following sociodemographic variables were defined: age at survey, two levels of education (<13 years and ≥13 years), marital status categorized as nonpaired (single–divorced–widow(er)) versus paired (married–cohabiting). Social class were defined as social class I, II, III according to the grouping professions in the international Erikson Goldtorpe Portocare social class schema [8, 20] using the Occupation Classification 2000 [23]. In this paper, Social class I comprised higher-grade professionals, while Social class II consisted of lower-grade professionals and administrators, and Social class III contained routine nonmanual employees [10, 11, 20]. Working time was defined as working full time (≥37 h/week) or part time (<37 h/week).
Quality of life, psychological distress, personality traits, and WA
Quality of life (QoL) was measured by the Medical Outcome Study Short Form 12 (SF-12) [40], resulting in scores on the physical (PCS) and mental component summary (MCS) scales, in which lower scores mean reduced and higher values improved QoL. Global health status was measured by item 1 of the SF-12 and was dichotomized into very good–good versus moderate–rather bad–bad health.
Anxiety–depression was measured by the Hospital Anxiety and Depression Scale (HADS), which is consisting of an anxiety subscale (HADS-A) and a depression subscale (HADS-D) [2]. Higher scores mean higher levels of anxiety or depression. Due to high correlations between HADS-A, HADS-D, and MCS, only the latter variable was included in the regression analyses. Internal consistencies of HADS-D and HADS-A were α = 0.85 and 0.81, respectively.
The Eysenck Personality Questionnaire (EPQ-18) is a short version of the original 90-item EPQ [9, 27] covering the personality dimensions of neuroticism, extraversion, and psychoticism with six items each. Neuroticism represents the tendency to be emotional and nervous and is strongly associated with vulnerability for anxiety and depression. Neuroticism was the only personality dimension included in the present analyses. Each item on the EPQ-18 is scored as 0 (no) and 1 (yes), and the six-item scores on each dimension are added, giving a sum score ranging from 0 to 6 on each dimension [27]. Internal consistency of neuroticism was α = 0.72.
The Work Ability Index (WAI) is a validated tool for measuring self-assessed WA that reveals how well a worker thinks she or he is able to perform her or his work, and it is commonly used to measure work ability in health examinations and workplace surveys [16, 43]. Current WA compared with the lifetime best is rated on an 11-point scale from 0 (completely unable to work) to 10 (WA at its best). Current physical and mental WA were also rated on 5-point Likert scales from 1 (very good) to 5 (very poor), and these ratings were dichotomized into very good–rather good and moderate–rather poor–very poor [16].
The WAI also covers the “number of current diseases diagnosed by a physician” covering: injuries from accidents, musculoskeletal disease, cardiovascular disease, respiratory disease, mental disorder, metabolic disease, neurological or sensory disease, or other severe diseases. The total number of comorbid diseases reported was dichotomized into comorbidity present (≥1 other disease) or absent.
Symptom scale measuring the referents’ own opinion of somatic symptoms has been applied in combination with the WAI in a comprehensive questionnaire among Finnish municipal employees in an 11-year follow-up study of aging workers [41, 42] and examined the association between perceived health and early retirement among men aged 42 to 60 from Eastern Finland. The symptom scale consisted of the following symptoms: tiredness, nervousness, concentration problems, headache, palpitation, vertigo, nausea, chest pain, stomach ache, and insomnia were scored on Likert scales with five response alternatives from 0 (never) to 4 (all the time). Symptom score was defined as the total symptoms score ranging from 0 (no symptoms) to 40 (maximum). The referents self estimated how often they subjectively experienced these symptoms.
The Demand–Control–Support Questionnaire (DCSQ) is based on the job strain model of Karasek and Theorell [18, 26]. The DCSQ has 17 items covering three aspects of job strain that is a subjective, self-reported evaluation of the work situation seen from the worker’s perspective [7]. The demands subscale (demands caused by task of work or work load) has five items; the control subscale (decision authority over own work situation) has six items and the support subscale (social support from colleagues at work) has six items. Each item of the DCSQ items is worded as a statement and is scored on a 4-point scale from 1 (right) to 4 (wrong). In this study the internal consistencies were for demands α = 0.90, control α = 0.91 and support α = 0.96.
Statistics
The SPSS for PC version 13.0 were used for statistic analyses. Continuous variables were analyzed by t-tests, and in case of skewed distributions, nonparametric tests were applied. Categorical variables were analyzed by χ 2-tests. Significant differences between groups on continuous variables and 2 × 2 contingency tables were calculated as effect sizes, and ≥0.40 were considered as significant concerning clinical issues and work issues [21, 31]. The internal consistency of scales was examined with Cronbach’s coefficient α. The associations of relevant variables and “work changes due to cancer” were examined with univariable and multivariable logistic regression analyses. The strength of associations was expressed as odds ratios with 95% confidence intervals. The associations of various independent variable and “current work ability” were examined with univariable and multivariable linear regression analyses. Due to skewed distribution, “current work ability” was log transformed. The strength of associations of the latter method was expressed as standardized β-values. The statistical significance level was set at p < 0.05 and all tests were two tailed.
Ethics
The study was approved by the Regional Committee for Medical Research Ethics of South Norway and approved by the Norwegian Data Inspectorate. All survivors received written information about the study and returned written informed consents.
Results
Socioeconomic and demographic findings
A higher proportion of female survivors had changed work due to cancer than the male ones (p = 0.003, ES = 0.39). No other sociodemographic differences of clinical significance were found between the change and nonchange groups (Table 1).
Work situation findings
Compared to the nonchange group the change group reported a poorer current WA (p ≤ 0.001, ES 0.75), higher proportion of part-time work (p < 0.001, ES 0.83), reduced physical and mental WA both in general and due to cancer (p ≤ 0.001, ES > 0.50 for all) than found in the nonchange group. The DCSQ demands subscale score was higher (p = 0.005, ES = 0.38) while the support subscale score was lower (p = 0.005, ES = 0.38) in the change versus the nonchange group (Table 2).
Health, quality of life, and psychological distress findings
The change group had more weeks on sick leave due to cancer diagnosis and treatment (p ≤ 0.001, ES = 0.63), but they showed lower mean score on the Symptom scale (p ≤ 0.001, ES = 0.44) although they reported poorer subjective health status (p < 0.001, ES = 0.60) and more comorbid diseases (p ≤ 0.001, ES = 0.53) than the nonchange group (Table 3).
The mean scores of anxiety and depression were higher in the change group (p < 0.001, ES ≥ 0.60 for both), and that group also showed poorer physical (p < 0.001, ES = 0.74) and mental QoL (p = 0.004, ES = 0.35) and higher score on neuroticism (p < 0.001, ES = 0.54) than the nonchange group.
Factors associated with change of work due to cancer
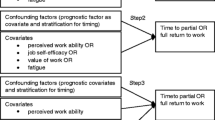
All variables that showed significant differences between the change and nonchange groups in the descriptive statistics were confirmed in the univariate logistic regression analyses (Table 4). In multivariable logistic regression analyses, however, only mental work ability reduced due to cancer was significantly associated with belonging to the change group. Female gender, increased job demands, and lower physical quality of life showed trends toward significant associations with the change group (p = 0.05–0.07).
Factors associated with current WA
Because most of the literature on CSs concerns WA rather than work changes, we examined the relationship between these two concepts. The correlation between them was r = 0.30. In univariable analyses, work changes, age, symptom score, comorbidity, PCS-12, MCS-12, physical and mental work ability due to cancer, support at work, and neuroticism were all significantly associated with current WA (Table 5). In the multivariable analyses, PCS-12 was most strongly and positively associated with current WA. MCS-12 also showed a similar but somewhat less strong association. Finally, reduced mental work ability due to cancer showed a significant but weak negative association with work ability. Work changes showed no significant association with current WA in the multivariable analysis.
Discussion
According to our definition of “work changes due to cancer,” 83% of CSs did report any such changes during the observation period, while 17% reported one or more changes. Significantly more women than men reported work changes, and those belonging to the change group reported significantly poorer current WA, poorer physical and mental WA both in general and due to cancer. They experienced more demands and less support at work compared to the nonchange group. The change group had a lower mean score of symptoms but poorer general health status and more comorbid diseases, psychological distress, and neuroticism, and their physical and mental quality of life were poorer compared to the nonchange group. In multivariable analyses, only poor mental WA due to cancer was significantly associated with work change, while female gender, demands at work, and physical quality of life showed trends.
Studies published during the last 10 years have mostly focus on CSs return to work and showed that the employment rates of CSs range from 30% to 90% with slightly lower labor participation than among controls [30, 36]. Recent studies show that working CSs are more likely to report poorer health and more comorbid chronic somatic conditions [5, 10, 29, 32, 33, 35] than controls without cancer. These studies also have found that a minority of CSs reported that cancer had impaired or reduced their WA in negative way [1, 13, 30, 34, 36, 38].
In our sample, work changes concerned several aspects namely: changes of workplace, prior occupation, work tasks, becoming unemployed or early retirement. One could argue that these changes are different in character, and they should not be lumped together. However, they have in common that they were attributed to the cancer illness and have many similar characteristics as CSs described in earlier studies such as weaker general health status, more comorbid diseases, and poorer quality of life. The majority of CSs in our sample did not have to do such work changes due to their cancer however, and this is an encouraging results. The implication is that cancer treatment hardly affects WA to any significant extent among the majority of tumor-free cancer patients with good prognosis.
The correlation between work changes and WA was moderate, but work changes were not significantly associated with WA in multivariable analysis. Poorer mental WA due to cancer was significantly associated with both work changes and WA in multivariable analyses and so was physical quality of life. Mental quality of life was significantly associated with WA but not with work changes. Thus, both poorer scores on both mental and physical factors were associated with the need to make work changes and to current WA in our sample.
A limitation of our study is the lack of registrations of the de facto practical working conditions in our samples, and thus we cannot reject the possibility of selection bias because there is a possibility that those with the most successful work situation are the ones who responded positively to our invitation.
That we only have examined survivors of early stage breast, prostate, and testicular cancer is another limitation of our study. Examination of other types and more advanced stages of cancer could lead to different findings concerning work change due to cancer. A response rate of approximately 60% for a questionnaire study of cancer survivors is not optimal. Patients treated at our hospital are exposed to several follow-up investigations particularly those with breast and testicular cancer, and this fact can explain the low response rate among these cancer survivors. An attrition analysis of the total sample showed no significant differences between responding and nonresponding cancer survivors in the variables available for examination. We therefore suggest that our findings can be generalized to the sample of cancer survivors who fulfill our selection criteria.
Conclusion
In this sample of tumor-free CSs after primary treatment of breast, prostate, and testicular cancer with good prognosis, who had returned to work, we found that the majority of the CSs did not have to make work change due to their cancer. In the minority of 17% who had to do so consisted mainly of women and was further characterized by poorer mental work ability due to cancer and poorer physical and mental quality of life. Both health care workers and the occupational health care system should have these factors in mind for follow-up programs for CSs.
References
Amir Z, Moran T, Walsh L, Iddende R, Luker K (2007) Return to work after cancer: a British experience. J Cancer Surviv 1:129–136
Bjelland I, Dahl AA, Haug TT, Neckelmann D (2002) The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res 52:69–77
Bradley CJ, Bednarek HL (2002) Employment patterns of long-term cancer survivors. Psychooncology 11:88–98
Bradley CJ, Neuman KD, Luo Z, Bednarek H, Schenk M (2005) Employment outcome of men treated for prostate cancer. J Natl Cancer Inst 97:958–965
Bradley CJ, Oberst K, Schenk M (2006) Absenteeism from work: the experience of employed breast and prostate cancer patients in the months following diagnosis. Psychooncology 15:739–747
Cancer Registry of Norway, Institute of Population-based Cancer Research (2006) Cancer in Norway 2005. Cancer Registry of Norway, Institute of Population-based Cancer Research, Oslo
De Lange A, Taris T, Kompier M, Houtman I, Bongers P (2003) The very best of the millennium, longitudinal research and the Demand–Control–(Support) Model. J Occup Health Psychol 8:282–305
Erikson R, Goldtorpe JH (1992) The constant flux. A study of class mobility in industrial societies. Clarendon, Oxford
Eysenck SBG, Tambs K (1990) Cross-cultural comparison of personality: Norway and England. Scand J Psychol 31:191–197
Gudbergsson SB, Fossaa SD, Boregeraas E, Dahl AA (2006) A comparative study of living conditions in cancer patients who have returned to work after curative treatment. Support Care Cancer 14:1020–1029
Gudbergsson SB, Fossaa SD, Sanne B, Dahl AA (2007) A controlled study of job strain in primary-treated caner patients without metastases. Acta Oncol 46:534–544
Gudbergsson SB, Fossaa SD, Ganz PA, Zebrack BJ, Dahl AA (2007) The association between living conditions, demography, and the ‘impact of cancer scale’ in tumor-free cancer survivors: a NOCWO study. Support Care Cancer 15:1309–1318
Hewitt M, Breesn DS (1999) Cancer prevalence and survivorship issues: analyses of the 1992 National Health Interview Survey. J Natl Cancer Inst 91:1480–1486
Hewitt M, Rowland JH, Yancik R (2003) Cancer survivors in the United States. Age, health, and disability. J Gerontol A Biol Sci Med Sci 58:82–91
Ilmarinen J (2001) Aging workers. Occup Environ Med 58:546–552
Ilmarinen J, Tuomi K (2004) Past, present and future of work ability. In: Ilmarinen J, Lehtinen S (eds) Past, present and future of work ability. People and work, research reports 65. Finnish Institute of Occupational Health Finland, Helsinki, pp 1–25
Ilmarinen J, Tuomi K, Klockars M (1997) Changes in the work ability of active employees over an 11-year period. Scand J Work Environ Health 23(suppl 1):49–57
Karaksek RA (1985) Job content instrument: questionnaire and user’s guide. University of South California, Los Angeles
Karpansalo M, Manninen P, Kauhanen J, Lakka TA, Salonen JT (2004) Perceived health as a predictor of early retirement. Scand J Work Environ Health 30:287–292
Krokstad S, Westin S (2002) Health inequalities by socioeconomic status among men in the Nord–Trøndelag Health Study, Norway. Scan J Public Health 30:113–124
Lipsey MW, Wilson DB (2001) Practical meta-analysis. Sage, Thousand Oaks
Nordic Council of Minister (2006) Nordic Statistical Yearbook 2006, Nord 2006: 1. Nordic Council of Ministers, Copenhagen
Office for National Statistic (2000) Standard occupational classification 2000 (SOC2000). http://www.statistics.gov.uk/methods_quality/ns_sec/soc2000.asp
Pryce J, Munir F, Haslam C (2007) Cancer survivorship and work: symptoms, supervisor response, co-worker disclosure and work adjustment. J Occup Rehabil 17:83–92
Reiso H, Nygard JF, Brage S, Gulbrandsen P, Tellnes G (2000) Work ability assessed by patients and their GPs in new episodes of sickness certification. Fam Pract 17:139–144
Sanne B, Torp S, Mykletun A, Dahl AA (2005) The Swedish Demands–Control–Support Questionnaire (DCSQ): factor structure, item analyse, and internal consistency in a large population. Scand J Public Health 33:166–174
Schou I, Ekeberg Ø, Ruland CM, Sandvik L, Kåresen R (2004) Pessimism as a predictor of emotional morbidity one year following breast cancer surgery. Psychooncology 13:309–320
Schultz PN, Beck ML, Stava C, Sellin R (2002) Cancer survivors. Work related issues. AAOHN J 50:220–226
Short PF, Vasey JJ, Tunceli K (2005) Employment pathways in a large cohort of adult survivors. Cancer 103:1292–1301
Short PF, Vasey JJ, BeLue R (2007) Work disability associated with cancer survivorship and other chronic conditions. Psychooncology 17:91–97
Sloan JA, Vargas-Chanas KCC, Sargent DJ, Novotny P, Athertum P, Allmer C, Fridley L, (2003) Detecting worms, ducks, and elephants: A simple approach for defining clinically relevant effects in quality-of-life measures. J Cancer Integr Med 1:41–47
Spelten ER, Sprangers MAG, Verbeek JHAM (2002) Factors reported to influence the return to work of cancer survivors: A litterature review. Psychooncology 11:124–131
Spelten ER, Verbeek JH, Uitterhoeve AL, Ansink AC, van der Lelie J, de Riejke TM, Kammeijer M, de Haes JC, Sprangers MA (2003) Cancer, fatigue and the return of patients to work—a prospective cohort study. Eur J Cancer 39:1562–1567
Steiner JF, Cavender TA, Main DS, Bradley CJ (2005) Assessing the impact of cancer on work outcomes. What are the research needs? Cancer 8:1703–1711
Steiner JF, Cavender TA, Nawels CT, Beaty BL, Bradley CJ et al (2007) The impact of physical and psychosocial factors on work characteristic after cancer. Psychooncology 17:138–147
Taskila T, Lindbohm M-L (2007) Factors affecting cancer survivors’ employment and work ability. Acta Oncol 46:446–451
Taskila T, Martikainen R, Virtanen SV, Pukkala E, Hietanen P, Lindbohm M-L (2004) The impact of education and occupation on employment status of cancer survivors. Eur J Cancer 40:2488–2493
Taskila T, Martikainen R, Hietanen P, Lindbohom M-L (2007) Comparative study of work ability between cancer survivors and their referents. Eur J Cancer 43:914–920
Taskila-Åbrandt T, Pukkala E, Martikainen R, Karjalainen A, Hietanen A (2005) Employment status of Finnish cancer patients in 1997. Psychooncolgy 14:221–226
Ware JE, Kosinski M, Keller SD (1996) A 12-item short-form health survey: construction of scales and preliminary test of reliability and validity. Med Care 34:220–233
Tuomi K, Ilmarinen J, Martikainen R, Aalto L, Klockars M (1997) Aging, work, life-style and work ability among Finnish municipal workers in 1981–1992. Scand J Work Environ Health 23(suppl 1):58–65
Tuomi K, Ilmarinen J, Seitsam J, Huuhtanen P, Martikainen R, Nygård C-H (1997) Summary of the Finnish research project (1981-1992) to promote the health and work ability of aging workers. Scand J Work Environ Health 23(suppl 1):66–71
Tuomi K, Ilmarinen J, Jahkola A, Katajarinne L, Tulkki A (1998) Work ability index 2nd edition. Finnish Institute of Occupational Health, Finland
Acknowledgement
The Norwegian Foundation for Health and Rehabilitation and the Nordic Cancer Union sponsored this study (Grant no H0-5010/002).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gudbergsson, S.B., Fosså, S.D. & Dahl, A.A. A study of work changes due to cancer in tumor-free primary-treated cancer patients. A NOCWO study. Support Care Cancer 16, 1163–1171 (2008). https://doi.org/10.1007/s00520-008-0407-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-008-0407-3