
Abstract
Background
The DICER1 syndrome is a tumor-predisposition disorder caused by germline pathogenic variation in DICER1 and is associated with cystic nephroma and other renal neoplasms. Dicer1 mouse and rare human DICER1 syndrome case reports describe structural kidney and collecting system anomalies. We investigated renal function and the frequency of structural abnormalities of the kidney and collecting system in individuals with germline loss-of-function variants in DICER1.
Methods
In this family-based cohort study, prospectively ascertained germline DICER1-mutation carriers (DICER1-carriers) and unaffected family controls were evaluated at the National Institutes of Health Clinical Center with renal ultrasound and comprehensive laboratory testing. Two radiologists reviewed the imaging studies from all participants for structural abnormalities, cysts, and tumors.
Results
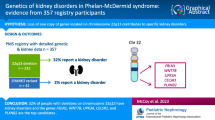
Eighty-nine DICER1-carriers and 61 family controls were studied. Renal cysts were detected in 1/33 DICER1-carrier children without history of cystic nephroma. Similar proportions of adult DICER1-carriers (8/48; 17%) and controls (11/50; 22%) had ultrasound-detected renal cysts (P = 0.504). 8/89 (9%) DICER1-carriers harbored ultrasound-detected structural abnormalities of varying severity within the collecting system or kidney, nephrolithiasis, or nephrocalcinosis. None of the family controls (0/61) had similar findings on ultrasound (P = 0.02). No meaningful differences in renal laboratory values between DICER1-carriers and unaffected family controls were observed.
Conclusions
Our report is the first to systematically characterize renal function and anatomy in a large prospective cohort of DICER1-carriers and DICER1-negative family controls. DICER1-carriers may be at increased risk of structural anomalies of the kidney or collecting system. The role for DICER1 in renal morphogenesis merits additional investigation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The DICER1 syndrome is a pleiotropic tumor-predisposition disorder secondary to pathogenic germline variants in DICER1, an endoribonuclease integral to the processing of microRNAs [1, 2]. Pleuropulmonary blastoma (PPB) is the hallmark tumor of the DICER1 syndrome. It is a rare, primitive, multipatterned lung sarcoma described in 1988 [3], and associated with high morbidity and mortality [4]. Subsequent to the recognition of PPB, it became apparent that other extra-pulmonary benign and malignant neoplasms occurred as manifestations of the DICER1 syndrome, including ovarian Sertoli-Leydig cell tumor [5], thyroid carcinoma, [6], nasal chondromesenchymal hamartoma [7], and ciliary body medulloepithelioma [8]. The familial co-occurrence of PPB with urinary system tumors was initially reported in a 2006 study, which included 15 patients with cystic nephroma (CN), one family member with Wilms tumor (WT), and intralobar nephrogenic rests and cysts either in probands with PPB or family members [9]. In a later study, germline pathogenic DICER1 variants were detected in 15/20 (75%) CN, 0/6 cystic partially differentiated nephroblastomas, and 1/3 CN-associated renal sarcomas [10]. Although the DICER1 syndrome is considered to be a rare disorder, the prevalence of germline pathogenic DICER1 variants in the general population is more common than expected (1/10,600) [11].
Humans with mosaic missense mutations in the RNase IIIb domain of DICER1, a typically severe form of the DICER1 syndrome [12], are reported to harbor unusual renal phenotypes. One patient (“case 1”) [13] with mosaic DICER1 p.D1713V at 9 months had a Wilms tumor and abnormal kidney histology, which was similar to that of Beckwith-Wiedemann syndrome, although there was no molecular genetic evidence of that disorder [13]. Another child (“patient 3”) [14] with mosaic DICER1 p.E1813D had a right renal medullary malformation with disorganized collecting system. Dicer1 knockout mice develop a spectrum of anomalies including hydronephrosis due to ureteropelvic junction obstruction [15], renal parenchymal cysts, and branching deficits [16, 17].
The frequency of structural abnormalities of the kidney or collecting system in individuals with germline loss-of-function variants in DICER1, the most common genotype in the syndrome [12], is unknown. In this study, we investigated the prevalence of ultrasound-detected renal anomalies and renal-associated clinical laboratory data in a large cohort of prospectively ascertained and systematically phenotyped individuals with a pathogenic DICER1 variant and family controls.
Patients and methods
Study participants, DICER1 genetic testing, and phenotyping
Individuals with a known or suspected DICER1-associated phenotype were recruited to participate in a natural history study of the DICER1 syndrome from physician- and self-referral, as well as collaboration with the International Pleuropulmonary Blastoma/DICER1 Registry and Ovarian and Testicular Stromal Tumor Registry. Probands and their family members were offered germline DICER1 genetic testing. All participants or their guardians completed Individual Information Questionnaires (IIQ) about past medical and surgical history, including kidney-associated pathology. Pathogenic DICER1-mutation carriers (DICER1-carriers) and family controls (no detected pathogenic germline DICER1 variants by sequencing, or inferred negative by pedigree analysis) were invited to undergo detailed phenotyping at the National Institutes of Health (NIH) Clinical Center (CC), including kidney ultrasound and comprehensive laboratory testing. Curved phased-array multifrequency transducers were routinely used to obtain longitudinal and transverse views of each kidney, supplemented by linear phased-array transducers as needed. Studies were conducted by experienced sonographers. Six individuals with negative germline DICER1 testing but with at least one known DICER1-associated tumor were also invited for Clinical Center evaluation (Supplemental Table S1); these patients are likely either mosaic or have sporadic (tumor-confined) disease “mosaic/sporadics.” A single radiologist (AL) systematically reviewed all the imaging studies for structural abnormalities, cysts, and tumors; for every lesion, length and width, number, location, laterality, and imaging characteristics (e.g., cystic, solid, partial solid/cystic, or indeterminate) were documented. A pediatric radiologist (MR) with experience in DICER1-associated CN and kidney disease then reviewed all studies deemed abnormal. Discrepancies were resolved by consensus.
Statistical analyses
Participants with DICER1-associated tumors but in whom germline (blood) DICER1 testing was negative (six mosaic/sporadic patients listed in Supplemental Table S1) were not included in statistical analyses and are reported separately. We used the chi square test for proportions or Fisher’s exact test when limited by infrequent cell counts (n < 5). We used the Wilcoxon rank-sum test for continuous variables, and calculated cumulative incidence using the complement of the Kaplan-Meier product limit estimator. The cross-sectional area of renal cysts was estimated assuming lesions are approximately elliptical in shape. We compared the proportion of laboratory values that were abnormal (high or low) at examination, as well as the continuous distribution laboratory values. Serum, plasma, or urinalysis laboratory values for which the normal range did not vary substantially by age or gender were analyzed without stratification. Select labs were stratified by gender, adulthood, or both gender and adulthood as appropriate. Qualitative and semi-quantitative urinalysis results were classified as either abnormal or normal/negative, per Supplemental Table S6, and other normal ranges were provided by the NIH Clinical Center Department of Laboratory Medicine. We considered P values ≤ 0.05 significant. All statistical tests were two-sided and conducted using Stata/SE 13.1 (Stata Corp., College Station, TX, USA).
Results
General demographics
A total of 89 pathogenic DICER1-carriers, 61 DICER1-negative family controls, and six mosaic/sporadic participants underwent evaluation at the NIH Clinical Center; all participants received kidney ultrasounds (US). Questionnaire data were available for all DICER1-carriers and 60/61 controls. Laboratory data drawn mainly from urinalysis were not available for a small minority of study participants (Table 1). Although the DICER1-carriers were younger than controls, the continuous distribution of age was not statistically different between DICER1-carriers and controls within the gender or child/adult strata (Table 1). There were 41 DICER1-carrier children and 48 DICER1-carrier adults. Clinical data on the six mosaic/sporadics are summarized in Supplemental Table S1 and are not considered further except where noted; none had a phenotype akin to those associated with mosaic DICER1 RNase IIIb domain mutations [13, 14].
Prevalence of urinary tract tumors in DICER1-carriers
Eight of the 41 DICER1-carrier children (6 males/2 females) had been diagnosed with CN (median age = 1.6 years; range = 0.4–4 years) (Supplemental Table S2); a ninth boy (a mosaic/sporadic) (76-01-001) had a CN at age 1.5 years (Supplemental Tables S1 and S2). Renal US at the Clinical Center on these nine children at a median of 2.4 years after nephrectomy or nephroureterectomy (range = 0.46–9.8 years) identified a 3.2 × 1.7 cm circumscribed multicystic mass in the right kidney (mid-pole) of a 15-month-old boy with a history of bilateral CN at age 10 months (52-01-001). A right partial nephrectomy in this child at age 20 months showed a CN with atypical spindle cell features, with a resemblance in some respects to the type I or cystic PPB. One 7-year-old female mosaic/sporadic (40-01-001) had a 3.5 × 2.5-cm area of increased echogenicity in the left upper kidney radiographically consistent with pyelonephritis. Review of abdominal computed tomography (CT) scans approximately 1 year before and after the NIH renal US exam showed a stable contour abnormality affecting the left kidney, and bilateral extrarenal pelvises.
Among DICER1-carriers in our cohort, there were no cases of known DICER1-associated malignant renal neoplasms (i.e., WT, renal sarcoma) or malignancies of the ureter or bladder. We found lesions radiographically suspicious for angiomyolipoma on renal US in one 43-year-old female family control (one tumor) and on renal US and follow-up renal CT in one 65-year-old female DICER1-carrier (four tumors in the left kidney: three mid-pole and one lower pole). One 54-year-old female control, a former smoker, had a 3 × 3 × 3.4 cm mass in the right upper kidney detected on our study US and confirmed by follow-up kidney CT scan. Urinalysis and constitutional symptoms were unremarkable. She was subsequently diagnosed with a renal cell carcinoma.
The prevalence of renal cysts in DICER1-carrier adults was comparable to family controls
Prior to Clinical Center evaluation, none of the controls reported a history of renal cysts, compared with 4/81 (4.9%) DICER1-carriers. However, similar proportions of adult DICER1-carriers and controls had renal cysts detected at Clinical Center US (Table 2): 11/50 (22%) adult controls had at least one lesion detected on US, compared with 8/48 adult DICER1-carriers (17%) (P = 0.504). The imaging characteristics of lesions in DICER1-carriers were similar to those in family controls.
Renal cysts were infrequent in DICER1-carrier children and controls
At Clinical Center US, no lesions were detected in childhood family controls. Of the 33 DICER1-carriers age ≤ 18 years without a history of CN, one (3%) girl (age 2.8 years; 28-01-002; Table 2) harbored an hypoechogenic 0.78 cm2 complex cyst in her right kidney, mid-pole. It had neither calcification nor irregular margins. There were no statistically significant differences in the frequency of renal cysts in DICER1-carrier children and controls.
Structural renal abnormalities in DICER1-carriers vs. family controls
Table 3 summarizes the results of the review of renal US and IIQ data from 89 DICER1-carriers. Excluding undefined masses, cysts, and evidence of previous nephrectomy, there were five (6%) DICER1-carriers with structural abnormalities of varying severity of the collecting system or kidney, including one child and one adult with a duplicated collecting system (83-01-001 and 82-02-002), and one child with incomplete rotation of the left kidney and collecting system (28-01-002). None of the children with a history of CN harbored additional structural abnormalities. Of the five DICER1-carriers with a collecting system abnormality, one child (80-01-001) had a history of surgery for ureteropelvic junction obstruction and one adult male (39-04-003) had a history of an unspecified renal anomaly. None of the five had abnormal renal function by blood urea nitrogen/creatinine. Two women (89-01-001 and 11-02-002) had previously-undiagnosed nephrolithiasis. A third woman (39-02-002) had previously-undiagnosed bilateral medullary nephrocalcinosis; her father (39-04-003) had non-stone hydronephrosis, caliectasis, and a low-lying left kidney.
There were no controls with collecting system anomalies, nephrolithiasis, or nephrocalcinosis on Clinical Center renal US (vs. cases (8/89); Fisher exact P = 0.02). There was no significant difference in cases vs. controls for structural abnormalities only (5/89 vs. 0/61; Fisher’s exact P = 0.08). We reviewed questionnaire data from controls and identified two individuals with a self-reported (unverified) history of kidney abnormalities: one 42-year-old female with a history of “ureter surgery” as an infant in the 1970s reported no subsequent kidney problems, and one 18-month-old male was reported by his mother to have had bilateral nephrocalcinosis at age 6 weeks. Review of the Clinical Center renal US for both controls showed no anomalies.
Laboratory measures of renal function were not significantly different between DICER1-carriers and family controls
Most laboratory values did not differ between DICER1-carriers and family controls in either the proportions that were abnormal or their distributions (Supplemental Table S3 and Supplemental Table S4). Selective post hoc review of medical records suggested those values that differed likely had non-DICER1-related explanations (Supplemental Table S3). The components of a standard urinalysis did not differ between DICER1-carriers and controls except for an increased prevalence of abnormal urobilinogen (9.88% vs. 0%; P = 0.021; Supplemental Table S5).
Discussion
Our report is the first to systematically characterize renal function and anatomy in a large prospective cohort of DICER1-carriers and DICER1-negative family controls. In 89 DICER1-carrier adults and children, we identified eight (9%) individuals with US-detected collecting system anomalies, nephrolithiasis, or nephrocalcinosis; no such anomalies were observed in 61 family controls, a significant difference. Laboratory measures of renal function were not significantly different between DICER1-carriers and family controls.
To our knowledge, there are two reported patients with mosaic DICER1 RNase IIIb-domain missense mutations, a particularly severe manifestation of the DICER1 syndrome, with structural kidney and/or collecting system anomalies [13, 14], but none in individuals with germline loss-of-function DICER1 variation prior to this report. For comparison, the incidence of ureteropelvic junction obstruction on routine live birth antenatal US is estimated to be 1/500 (0.2%) [18, 19]. In another multi-center study of pre-natal US performed on 709,030 fetuses (including live-birth, stillbirths, abortions), 259 (0.03%) had US-detected dilation of the upper tract [20]. We acknowledge that there was no significant difference in the frequency of structural abnormalities in our cases and controls; however, we believe that our findings are provocative. Collectively, the published Dicer1 mouse [15,16,17], human mosaic DICER1 RNase IIIb patients [13, 14], and our data suggest that DICER1-carriers may be at increased risk of structural anomalies of the kidney or collecting system. This observation needs validation in an independent cohort of DICER1-carriers. Conversely, the prevalence of DICER1 germline pathogenic variants in cohorts with collecting system anomalies is unknown and merits investigation. Careful attention to abnormalities of the collecting system is warranted for DICER1-carrier children when undergoing renal US to screen for CN or malignant renal tumors, as per current surveillance guidelines [21].
US also revealed evidence of nephrolithiasis in two asymptomatic adult DICER1-carriers, neither of whom had an underlying renal structural anomaly or a known prior history of nephrolithiasis. No stones were available for analysis. No family controls had a history of nephrolithiasis. Given the high prevalence of nephrolithiasis in the general population, absence of this phenotype in the Dicer1 mouse models, and the lack of clear pathophysiologic link between miRNA dysregulation and the biology of nephrolithiasis formation, additional evidence is needed before drawing any conclusions on this association. We observed asymptomatic, undiagnosed medullary nephrocalcinosis in one adult DICER1-carrier; one pediatric-aged control had a history of medullary nephrocalcinosis but no evidence of this was apparent on US. Renal function as measured by a variety of standard clinical blood and urine laboratory studies in DICER1-carriers was normal (or likely explained by non-DICER1 processes), which is consistent with Dicer1 mouse modeling [22]. Importantly, there was no evidence of glomerular dysfunction in mouse or man.
Renal parenchymal cysts are an established feature of multiple Dicer1 mouse models [16, 17]. A large study of US-detected renal cysts in children estimated a prevalence of 0.22% (35/16,102) [23]. We observed a non-significant excess of simple cysts in 2/41 (4.9%) DICER1-carrier children; the rate is 1/33 (3.0%) if excluding those with a history of CN. One DICER1-carrier child (28-01-002) with an apparent calyceal diverticulum also had concomitant incomplete ventral-lateral rotation of the collecting system, a rare finding (Table 3). In adults, renal cysts are more common in men than women and their incidence increases with age; one study of 14,314 individuals reported a prevalence of renal cysts in about 10% of men and 5.7% of women, aged 40–49 years [24]. These proportions are lower than those observed in our cases and controls, whose median age was about 41 years. We did not observe a significant excess of renal cysts in our adult cohort compared with family controls. This may be explained by the natural history of renal cysts or by the cross-sectional nature of our data. Although rare, renal cysts in children are frequently observed in the context of a hereditary disorder or malformation syndrome [25]. Over time, renal cysts become more common, presumably due to a variety of etiologies, and the relative contribution of one etiology (like the DICER1 syndrome) is increasingly diluted.
Limitations of this study include a modest sample size (a frequent challenge in rare disorders) and enrollment of families in the study due to ascertainment bias: families needed at least one member with a known DICER1-associated phenotype to come to clinical attention. In addition, our small sample size included a very limited number of pediatric-aged family controls and thus we had to compare the prevalence of renal cysts with previously published proportions. There are limits to the sensitivity of ultrasonography to detect renal and urinary tract malformations and structural abnormalities. Lastly, the cross-sectional nature of the study also limits our conclusions.
Conclusion
In our study of prospectively phenotyped DICER1-carriers and family controls, 6% of adults and children with a germline pathogenic DICER1 variant harbored a structural abnormality of the renal collecting system. Our findings are of importance since DICER1-carriers are more common than expected [11] and renal anomalies as described in this report may aid in the identification of families at risk. These observations and their clinical significance need replication and study in a larger cohort. In young DICER1-carrier children undergoing serial renal US to screen for CN [21], attention should also be paid to the presence of a collecting system abnormality. The prevalence of germline pathogenic DICER1 variants in individuals with collecting system anomalies remains to be determined.
References
Hill DA, Ivanovich J, Priest JR, Gurnett CA, Dehner LP, Desruisseau D, Jarzembowski JA, Wikenheiser-Brokamp KA, Suarez BK, Whelan AJ, Williams G, Bracamontes D, Messinger Y, Goodfellow PJ (2009) DICER1 mutations in familial pleuropulmonary blastoma. Science 325:965
Doros L, Schultz KA, Stewart DR, Bauer AJ, Williams G, Rossi C, Carr A, Yang J, Dehner LP, Messinger Y, Hill DA (2014) DICER1-related disorders. In: Pagon RA (ed) GeneReviews. University of Washington, Seattle (WA). On-line, non-profit, peer-reviewed genetics encyclopedia: https://www.ncbi.nlm.nih.gov/books/NBK196157/
Manivel JC, Priest JR, Watterson J, Steiner M, Woods WG, Wick MR, Dehner LP (1988) Pleuropulmonary blastoma. The so-called pulmonary blastoma of childhood. Cancer 62:1516–1526
Messinger YH, Stewart DR, Priest JR, Williams GM, Harris AK, Schultz KA, Yang J, Doros L, Rosenberg PS, Hill DA, Dehner LP (2015) Pleuropulmonary blastoma: a report on 350 central pathology-confirmed pleuropulmonary blastoma cases by the International Pleuropulmonary Blastoma Registry. Cancer 121:276–285
Schultz KA, Pacheco MC, Yang J, Williams GM, Messinger Y, Hill DA, Dehner LP, Priest JR (2011) Ovarian sex cord-stromal tumors, pleuropulmonary blastoma and DICER1 mutations: a report from the International Pleuropulmonary Blastoma Registry. Gynecol Oncol 122:246–250
Khan NE, Bauer AJ, Schultz KAP, Doros L, Decastro RM, Ling A, Lodish MB, Harney LA, Kase RG, Carr AG, Rossi CT, Field A, Harris AK, Williams GM, Dehner LP, Messinger YH, Hill DA, Stewart DR (2017) Quantification of thyroid cancer and multinodular goiter risk in the DICER1 syndrome: a family-based cohort study. J Clin Endocrinol Metab 102:1614–1622
Stewart DR, Messinger Y, Williams GM, Yang J, Field A, Schultz KA, Harney LA, Doros LA, Dehner LP, Hill DA (2014) Nasal chondromesenchymal hamartomas arise secondary to germline and somatic mutations of DICER1 in the pleuropulmonary blastoma tumor predisposition disorder. Hum Genet 133:1443–1450
Priest JR, Williams GM, Manera R, Jenkinson H, Brundler MA, Davis S, Murray TG, Galliani CA, Dehner LP (2011) Ciliary body medulloepithelioma: four cases associated with pleuropulmonary blastoma--a report from the International Pleuropulmonary Blastoma Registry. Br J Ophthalmol 95:1001–1005
Boman F, Hill DA, Williams GM, Chauvenet A, Fournet JC, Soglio DB, Messinger Y, Priest JR (2006) Familial association of pleuropulmonary blastoma with cystic nephroma and other renal tumors: a report from the International Pleuropulmonary Blastoma Registry. J Pediatr 149:850–854
Doros LA, Rossi CT, Yang J, Field A, Williams GM, Messinger Y, Cajaiba MM, Perlman EJ, Schultz KA, Cathro HP, Legallo RD, LaFortune KA, Chikwava KR, Faria P, Geller JI, Dome JS, Mullen EA, Gratias EJ, Dehner LP, Hill DA (2014) DICER1 mutations in childhood cystic nephroma and its relationship to DICER1-renal sarcoma. Mod Pathol 27:1267–1280
Kim J, Field A, Schultz KAP, Hill DA, Stewart DR (2017) The prevalence of DICER1 pathogenic variation in population databases. Int J Cancer 141:2030–2036
Brenneman MA, Field A, Yang J, Williams G, Doros L, Rossi CT, Schultz KA, Rosenberg A, Ivanovich J, Turner J, Gordish-Dressman H, Stewart DR, Yu W, Harris A, Schoettler P, Goodfellow PJ, Dehner L, Messinger Y, Hill DA (2015) Temporal order of RNase IIIb and loss-of-function mutations during development determines phenotype in DICER1 syndrome: a unique variant of the two-hit tumor suppression model. F1000 Res 4:214
Klein S, Lee H, Ghahremani S, Kempert P, Ischander M, Teitell MA, Nelson SF, Martinez-Agosto JA (2014) Expanding the phenotype of mutations in DICER1: mosaic missense mutations in the RNase IIIb domain of DICER1 cause GLOW syndrome. J Med Genet 51:294–302
de Kock L, Wang YC, Revil T, Badescu D, Rivera B, Sabbaghian N, Wu M, Weber E, Sandoval C, Hopman SM, Merks JH, van Hagen JM, Bouts AH, Plager DA, Ramasubramanian A, Forsmark L, Doyle KL, Toler T, Callahan J, Engelenberg C, Bouron-Dal Soglio D, Priest JR, Ragoussis J, Foulkes WD (2016) High-sensitivity sequencing reveals multi-organ somatic mosaicism causing DICER1 syndrome. J Med Genet 53:43–52
Bartram MP, Hohne M, Dafinger C, Volker LA, Albersmeyer M, Heiss J, Gobel H, Bronneke H, Burst V, Liebau MC, Benzing T, Schermer B, Muller RU (2013) Conditional loss of kidney microRNAs results in congenital anomalies of the kidney and urinary tract (CAKUT). J Mol Med (Berl) 91:739–748
Pastorelli LM, Wells S, Fray M, Smith A, Hough T, Harfe BD, McManus MT, Smith L, Woolf AS, Cheeseman M, Greenfield A (2009) Genetic analyses reveal a requirement for Dicer1 in the mouse urogenital tract. Mamm Genome 20:140–151
Nagalakshmi VK, Ren Q, Pugh MM, Valerius MT, McMahon AP, Yu J (2011) Dicer regulates the development of nephrogenic and ureteric compartments in the mammalian kidney. Kidney Int 79:317–330
Baskin LS (2017) Congenital uretopelvic junction obstruction. UpToDate, Waltham, MA. On-line, peer-reviewed medical textbook: www.uptodate.com
Termos S, AlKabbani M, Ulinski T, Sanjad S, Kotobi H, Chalard F, Aoun B (2017) Ureteropelvic junction obstruction and parathyroid adenoma: coincidence or link? Case Rep Nephrol. https://doi.org/10.1155/2017/9852912
Wiesel A, Queisser-Luft A, Clementi M, Bianca S, Stoll C, EUROSCAN Study Group (2005) Prenatal detection of congenital renal malformations by fetal ultrasonographic examination: an analysis of 709,030 births in 12 European countries. Eur J Med Genet 48:131–144
Schultz KAP, Williams GM, Kamihara J, Stewart DR, Harris AK, Bauer AJ, Turner J, Shah R, Schneider K, Schneider KW, Carr AG, Harney LA, Baldinger S, Frazier AL, Orbach D, Schneider DT, Malkin D, Dehner LP, Messinger YH, Hill DA (2018) DICER1 and associated conditions: identification of at-risk individuals and recommended surveillance strategies. Clin Cancer Res 24:2251–2261
Ho JJ, Marsden PA (2008) Dicer cuts the kidney. J Am Soc Nephrol 19:2043–2046
McHugh K, Stringer DA, Hebert D, Babiak CA (1991) Simple renal cysts in children: diagnosis and follow-up with US. Radiology 178:383–385
Terada N, Ichioka K, Matsuta Y, Okubo K, Yoshimura K, Arai Y (2002) The natural history of simple renal cysts. J Urol 167:21–23
Mir S, Rapola J, Koskimies O (1983) Renal cysts in pediatric autopsy material. Nephron 33:189–195
Acknowledgments
The authors wish to thank the Pine Tree Apple Tennis Classic and St. Baldrick’s Foundation for their ongoing support of children’s cancer research. The authors also wish to thank the many patients, families, and treating physicians who participate in the NCI DICER1-related Pleuropulmonary Blastoma Cancer Predisposition Syndrome study, the International OTST Registry, and/or the International Pleuropulmonary Blastoma/DICER1 Registry. We thank Rosamma Decastro, CRNP for clinical contributions.
Funding
This work was supported by the Intramural Research Program of the Division of Cancer Epidemiology and Genetics of the National Cancer Institute (NCI), Bethesda, MD. DAH is supported by NCI 2R01CA143167.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All participants provided written, informed consent, and the study was approved by the National Cancer Institute’s Institutional Review Board (IRB). In addition, clinical, radiographic, and genetic data on participants enrolled in the International Pleuropulmonary/DICER1 Registry and the International Ovarian and Testicular Stromal Tumor Registry were abstracted and reviewed. Both registries are overseen by the IRB at Children’s Minnesota (protocols 98107, 0909-082, 1111-112). Participants in both registries provided informed, written consent for use of their registry data in the current analysis. The study adhered to the precepts in the Declaration of Helsinki.
Conflict of interest
The authors declare that they have no conflict of interest.
Disclaimer
The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products or organizations imply endorsement by the US Government.
Electronic supplementary material
ESM 1
(DOCX 33 kb)
Rights and permissions
About this article

Cite this article
Khan, N.E., Ling, A., Raske, M.E. et al. Structural renal abnormalities in the DICER1 syndrome: a family-based cohort study. Pediatr Nephrol 33, 2281–2288 (2018). https://doi.org/10.1007/s00467-018-4040-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-018-4040-1