
Abstract
Purpose
The objective was to investigate if performing a sub-peak or supra-peak verification phase following a ramp test provides additional value for determining 'true' maximum oxygen uptake (\( {{\dot{\text{V}}}} \)O2).
Methods
17 and 14 well-trained males and females, respectively, performed two ramp tests each followed by a verification phase. While the ramp tests were identical, the verification phase differed in power output, wherein the power output was either 95% or 105% of the peak power output from the ramp test. The recovery phase before the verification phase lasted until capillary blood lactate concentration was ≤ 4 mmol·L−1. If a \( {{\dot{\text{V}}}} \)O2 plateau occurred during ramp test, the following verification phase was considered to provide no added value. If no \( {{\dot{\text{V}}}} \)O2 plateau occurred and the highest \( {{\dot{\text{V}}}} \)O2 (\( {{\dot{\text{V}}}} \)O2peak) during verification phase was < 97%, between 97 and 103%, or > 103% of \( {{\dot{\text{V}}}} \)O2peak achieved during the ramp test, no value, potential value, and certain value were attributed to the verification phase, respectively.
Results
Mean (standard deviation) \( {{\dot{\text{V}}}} \)O2peak during both ramp tests was 64.5 (6.0) mL·kg−1·min−1 for males and 54.8 (6.2) mL·kg−1·min−1 for females. For the 95% verification phase, 20 tests showed either a \( {{\dot{\text{V}}}} \)O2 plateau during ramp test or a verification \( {{\dot{\text{V}}}} \)O2peak < 97%, indicating no value, 11 showed potential value, and 0 certain value. For the 105% verification phase, the values were 26, 5, and 0 tests, respectively.
Conclusion
In well-trained adults, a sub-peak verification phase might add little value in determining 'true' maximum \( {{\dot{\text{V}}}} \)O2, while a supra-peak verification phase adds no value.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The maximum oxygen uptake (\( {{\dot{\text{V}}}} \)O2max) is generally considered the gold standard for assessing cardiorespiratory fitness (Hill and Lupton 1923), widely applied to evaluate the efficacy of exercise intervention programs and changes in physical fitness (Blair et al. 1995), and used to predict all-cause mortality (Blair et al. 1995; Laukkanen et al. 2016). \( {{\dot{\text{V}}}} \)O2max represents the upper limit of the physiological oxygen transport and utilization system (Bassett 2002; Fletcher et al. 2013; Franklin 2007; Poole and Jones 2017). It is determined by cardiopulmonary exercise testing (CPET) (Bassett 2002). The primary criterion for determining the attainment of a 'true' \( {{\dot{\text{V}}}} \)O2max, and thus the highest physiologically achievable value during CPET, is the occurrence of a \( {{\dot{\text{V}}}} \)O2 plateau in the severe intensity domain (Howley et al. 1995; Niemeyer et al. 2021; Poole and Jones 2017). However, even at maximum effort, a \( {{\dot{\text{V}}}} \)O2 plateau at the end of ramp-based CPET is identified in less than half of the participants (Knaier et al. 2019; Lucía et al. 2006; Wagner et al. 2020; Day et al. 2003). In the absence of a \( {{\dot{\text{V}}}} \)O2 plateau, secondary \( {{\dot{\text{V}}}} \)O2max criteria including percentage of age-predicted maximum heart rate, respiratory exchange ratio, and rating of perceived exertion are commonly used to diagnose 'true' \( {{\dot{\text{V}}}} \)O2max (Knaier et al. 2019; Midgley et al. 2007). However, the major criticism of the current \( {{\dot{\text{V}}}} \)O2max criteria, including \( {{\dot{\text{V}}}} \)O2 plateau and secondary \( {{\dot{\text{V}}}} \)O2max criteria, is that they are often sensitive to exercise test protocol, exercise type, and participant characteristics (Midgley et al. 2007). Too low or too high criteria thresholds lead to over- or underestimation, respectively, of participant's exhaustion, resulting in misclassification of 'true' \( {{\dot{\text{V}}}} \)O2max (Knaier et al. 2019).
An alternative to \( {{\dot{\text{V}}}} \)O2 plateau and secondary \( {{\dot{\text{V}}}} \)O2max criteria could be the so-called verification phase. This is an additive constant load exercise test to the limit of exercise tolerance performed directly after a brief recovery phase following a ramp-based CPET (Midgley et al. 2007; Poole and Jones 2017; Scharhag-Rosenberger et al. 2011; Rossiter et al. 2006). Concordance between the highest \( {{\dot{\text{V}}}} \)O2 (\( {{\dot{\text{V}}}} \)O2peak) values achieved in the verification phase and ramp-based CPET (usually within 2–3% according to the \( {{\dot{\text{V}}}} \)O2max test–retest reliability) provides evidence of achievement of 'true' \( {{\dot{\text{V}}}} \)O2max during CPET (Costa et al. 2021; Dalleck et al. 2012). To date, several authors have reported such verification of 'true' \( {{\dot{\text{V}}}} \)O2max (Costa et al. 2021). Accordingly, mean \( {{\dot{\text{V}}}} \)O2peak in the verification phase did not differ from mean \( {{\dot{\text{V}}}} \)O2peak determined in a ramp-based CPET (Costa et al. 2021). One argument for implementing a verification phase to determine \( {{\dot{\text{V}}}} \)O2max is that a higher incidence of successfully verified \( {{\dot{\text{V}}}} \)O2max compared with the incidence of \( {{\dot{\text{V}}}} \)O2 plateau during a ramp-based CPET has been documented (Midgley et al. 2006; Scharhag-Rosenberger et al. 2011). Although numerous studies have investigated the effectiveness of verification phase for determining \( {{\dot{\text{V}}}} \)O2max, there is currently no established recommendation for the ideal implementation of a verification phase and its clear added value. Thus, various verification phase protocols with different intensity and recovery phase duration have been applied so far (Costa et al. 2021).
Several studies have performed a verification phase with a supra-peak load, i.e., intensities above the peak power output (PPO) achieved during ramp-based CPET. The rationale underlying this is that during a constant exercise test above PPO, \( {{\dot{\text{V}}}} \)O2 increases to \( {{\dot{\text{V}}}} \)O2max and thus provides a second \( {{\dot{\text{V}}}} \)O2max value that can be compared to the previous one (Hill and Ferguson 1999; Hill and Smith 1999; Poole et al. 1988, 1990). However, this is only possible if premature exercise intolerance does not intervene (Jones et al. 2011; Poole and Jones 2017). To be considered, however, for endurance-trained participants, work rate increase in ramp-based CPET is rather high to prevent exceeding optimal test duration (Midgley et al. 2008; Yoon et al. 2007). This can cause excessive peak intensity in the verification phase that cannot be sustained long enough for \( {{\dot{\text{V}}}} \)O2 kinetics to enable \( {{\dot{\text{V}}}} \)O2max to be reached (Iannetta et al. 2020). For trained athletes with fast \( {{\dot{\text{V}}}} \)O2 kinetics, it requires approximately 2:00 min to achieve \( {{\dot{\text{V}}}} \)O2max (Caputo and Denadai 2008). However, in most studies using supra-peak intensity, verification phase duration was less than 2:00 min (Niemeyer et al. 2021). For example, a recent published study by Wagner et al. (2021) implementing a verification phase in well-trained adults with a supra-peak intensity of 105% of the PPO revealed little added value of a verification phase for determining \( {{\dot{\text{V}}}} \)O2max. This little added value was likely due to the fact that the supra-peak load, based on a previously performed ramp-based CPET with a rather high increase in work rate, could not be sustained for a sufficient duration to allow \( {{\dot{\text{V}}}} \)O2 to increase to \( {{\dot{\text{V}}}} \)O2max (Wagner et al. 2021). Hence, the question arises whether a supra-peak verification phase can have additional value in determining \( {{\dot{\text{V}}}} \)O2max. It might be beneficial to conduct a verification phase below PPO since the loading can be sustained for a longer duration due to the reduced intensity. Indeed, not the PPO but rather the critical power represents the threshold intensity beyond which \( {{\dot{\text{V}}}} \)O2max can theoretically be evoked (Hill and Ferguson 1999; Hill and Smith 1999; Poole et al. 1988, 1990). Thus, verification phase with exercise intensities above the critical power but below the PPO might be beneficial for determining \( {{\dot{\text{V}}}} \)O2max, particularly if the work rate increase of the ramp-based CPET is rather high (Iannetta et al. 2020).
Besides the intensity of the verification phase, the duration of the recovery phase between the ramp-based CPET and verification phase should be considered. Previous investigations found no significant effect of recovery phase duration on the difference between \( {{\dot{\text{V}}}} \)O2peak achieved in a ramp test and verification phase (Costa et al. 2021). Regardless of the recovery phase lasting less than 15 min (Foster et al. 2007; Rossiter et al. 2006; Scharhag-Rosenberger et al. 2011; Sedgeman et al. 2013) or 24 h (Scharhag-Rosenberger et al. 2011), an identical mean \( {{\dot{\text{V}}}} \)O2peak was obtained in the ramp test and verification phase. However, it is already known that prior vigorous or severe exercise increasing baseline blood lactate concentration to approximately 3–5 mmol·L−1, improves subsequent high-intensity cycling performance in well-trained adults (Burnley et al. 2005). Additionally, prior vigorous exercise has been shown to effectively accelerate the \( {{\dot{\text{V}}}} \)O2 response to exercise (Wilkerson et al. 2004) and increase the time to the limit of exercise tolerance during subsequent supra-peak exercise (Jones et al. 2003). Therefore, the question arises whether an optimal determination of the recovery phase duration, adapted to the individual blood lactate concentration of each participant, can result in an increased added value of a verification phase. To the author's knowledge, this has not been investigated in any study to date (Costa et al. 2021).
In previous analyses, \( {{\dot{\text{V}}}} \)O2peak attained during CPET has mostly been compared to verification \( {{\dot{\text{V}}}} \)O2peak only on group level (Costa et al. 2021), and the proportion of participants in whom \( {{\dot{\text{V}}}} \)O2max could actually be verified was only reported in a few studies (Bowen et al. 2012; Schaun et al. 2021; Wagner et al. 2021; Murias et al. 2018; Mier et al. 2012). In addition, most studies focused only on the incidence of 'successful' verification and failed to capture the actual added value of conducting such verification phases in consideration of previously achieved \( {{\dot{\text{V}}}} \)O2 plateaus or the attainment of secondary \( {{\dot{\text{V}}}} \)O2max criteria (Costa et al. 2021; Schaun 2017; Niemeyer et al. 2021).
Thus, this study aimed to investigate the usefulness of a verification phase protocol in which the factors of intensity and recovery phase duration are implemented optimally and individually for determining \( {{\dot{\text{V}}}} \)O2max in well-trained male and female adults. In addition, the study aimed to clarify the added value of this verification phase protocol in relation to the presence of a \( {{\dot{\text{V}}}} \)O2 plateau and achievement of secondary \( {{\dot{\text{V}}}} \)O2max criteria during previous ramp-based CPET testing.
Materials and methods
Study design
This study was a cross-sectional single-center randomized study conducted at the Department of Sport, Exercise and Health at the University of Basel, Switzerland. The study was conducted between September 2020 and June 2021 under consistent conditions (air humidity, 40–55%; room temperature, 20–22 °C). All procedures were approved by the Ethics Committee of Northwestern and Central Switzerland (EKNZ-2019-01697). Written informed consent was obtained from all participants before the start of the study. Participants attended two study visits, with a recovery phase of at least 24 h in between, and over a period of eight to ten days. To ensure equal testing conditions for all participants, standardized procedures and instructions were used. On both days, participants performed CPET using a ramp protocol followed by a verification phase. While the ramp tests were identical on both days, the verification test differed in workload. One verification phase was with sub-peak load (i.e., 95% of PPO achieved during ramp test) and the other was with supra-peak load (i.e., 105% of PPO achieved during ramp test). The order of the verification phase tests was randomized.
Participants
Eligibility criteria for the study were age between 18 and 39 years, body mass index ≤ 27 kg/m2, and high cardiorespiratory fitness. Exclusively participants with a \( {{\dot{\text{V}}}} \)O2max score ≥ 95th percentile (i.e., ≥ 55 mL·kg−1·min−1 for males and ≥ 51 mL·kg−1·min−1 for females) according to normative data of the American College of Sports Medicine references were considered eligible (ACSM 2010). Exclusion criteria were cardiovascular diseases, febrile infections within the past 14 days, any type of diabetes mellitus, hypertension (systolic blood pressure > 160 mmHg; diastolic blood pressure > 100 mmHg), and participation in another clinical trial within the past four weeks. Participants were instructed to maintain a balanced diet and adequate water intake 72 h before the laboratory appointments, refrain from exercising and drinking alcohol 24 h before, abstain from caffeine four hours before, refrain from eating two hours before, and to go to bed early the night before the measurement.
Acquisition of participant characteristics
To assess participants' pre-exercise risk stratification, a questionnaire was completed (Shephard 1988) and a resting 12-lead electrocardiogram was recorded before the first measurement. Participants answering 'yes' to any of the questions of the questionnaire and/or exhibiting abnormalities in the electrocardiogram were examined by a physician before participating in the study. Body height and weight were determined to the nearest 0.5 cm and 0.1 kg, respectively. Participants' body fat content and lean body mass were determined using a four-segment bioelectrical impedance analysis (Inbody 720; Inbody Co. Ltd., Seoul, South Korea) at both laboratory appointments before each CPET.
Cardiopulmonary exercise testing
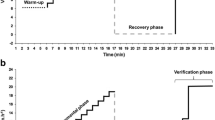
During both laboratory appointments, CPET using a ramp protocol to the limit of exercise tolerance followed by a verification phase were performed on a cycle ergometer (Sport Excalibur; Lode Medical Technology, Groningen, The Netherlands). Participants were allowed to choose their pedaling cadence as long as it was maintained above 60 rpm. Throughout the exercise test, participants were verbally encouraged to reach the limit of their exercise tolerance. After a 3-min warm-up at 50 W, the work rate increased linearly with 30 W per minute until exercise intolerance. The ramp test was followed by a recovery phase at 50 W. The recovery phase lasted until capillary blood lactate concentration was ≤ 4 mmol·L−1 ensuring sufficient recovery before the verification phase. Thus, the recovery phase duration differed among participants, but was limited to 30 min, regardless of whether the value was reached or not. The rationale for this cut-off value is that exercise tolerance might be increased during a subsequent exercise bout if the recovery phase duration is long enough to reduce blood lactate concentration below 3–5 mmol·L−1 (Bailey et al. 2009; Burnley et al. 2005). Subsequent to the recovery phase, one of the two verification phase tests was performed to confirm the 'true' \( {{\dot{\text{V}}}} \)O2max of the ramp test. Throughout the entire exercise testing, gas exchange was continuously measured breath-by-breath (MetaMax 3B; Cortex Biophysik GmbH, Leipzig, Germany). Data were averaged across 10-s intervals for analysis. \( {{\dot{\text{V}}}} \)O2peak was defined as the highest consecutive 30 s of \( {{\dot{\text{V}}}} \)O2 and maximal respiratory exchange ratio as the highest value during the exercise testing. Heart rate was continuously recorded using a 12-channel electrocardiograph (Custo med GmbH, Ottobrunn, Germany). Rating of perceived exertion was assessed using the Borg scale 6–20 (Borg 1982) at rest, after warm-up, every 3 min during the ramp test to the limit of exercise tolerance, every 3 min during the recovery phase, and at the end of the verification phase. Capillary blood lactate concentration was analyzed using 10 μL of blood drawn from the earlobe at rest, after warm-up, immediately after reaching the limit of exercise tolerance during the ramp test, every 3 min during the recovery phase, and at the end of the verification phase (SuperGL Ambulance, Hitado Diagnostic Systems, Moehnesee, Germany). The highest value measured was defined as maximum blood lactate concentration. Before each study visit, volume and two-point gas concentration calibration were performed on the respective metabolic cart.
A \( {{\dot{\text{V}}}} \)O2 plateau was defined as an increase in \( {{\dot{\text{V}}}} \)O2 < 50% during the final 50 W of the ramp test compared to the individual increase in the submaximal intensity domain (Niemeyer et al. 2020). For this purpose, we calculated the slope of the \( {{\dot{\text{V}}}} \)O2-work rate relationship of the final 50 W and of the submaximal intensity domain (from 80 W to PPO-60 W) using linear regression analyses. As previously described, this definition allows the diagnosis of a \( {{\dot{\text{V}}}} \)O2 plateau with a risk of false plateau diagnoses of less than 5% (Niemeyer et al. 2020). Further, if the verification \( {{\dot{\text{V}}}} \)O2peak was ± 3% of the \( {{\dot{\text{V}}}} \)O2peak achieved in the ramp test, \( {{\dot{\text{V}}}} \)O2max verification was accepted (Costa et al. 2021; Nolan et al. 2014). Secondary \( {{\dot{\text{V}}}} \)O2max criteria were also analyzed to verify \( {{\dot{\text{V}}}} \)O2max in the ramp test. These were defined as maximal respiratory exchange ratio ≥ 1.13, maximal heart rate ≥ 93% of 208-(0.7·age), maximal heart rate ≥ 96% of 210-age, and rating of perceived exertion ≥ 19 (Knaier et al. 2019; Wagner et al. 2020).
Data analysis
Data in text are presented as mean (standard deviation [SD]) unless noted otherwise. Descriptive statistics were applied to present participant characteristics, the results of both ramp tests, and the corresponding verification phase. A scatterplot was used to display the percentage of verification \( {{\dot{\text{V}}}} \)O2peak (Fig. 1). The percentage was computed by dividing the verification \( {{\dot{\text{V}}}} \)O2peak by the \( {{\dot{\text{V}}}} \)O2peak achieved in the ramp test. To examine the additive value by performing a verification phase on the determination of the 'true' \( {{\dot{\text{V}}}} \)O2max, the percentage of tests was calculated for each of the subsequent three conditions: (1) no added value, (2) potential added value, and (3) certain added value (Fig. 2). No added value was defined if a \( {{\dot{\text{V}}}} \)O2 plateau occurred during the ramp test, indicating by itself that \( {{\dot{\text{V}}}} \)O2max was achieved, or if no \( {{\dot{\text{V}}}} \)O2 plateau occurred and verification \( {{\dot{\text{V}}}} \)O2peak was < 97% of the \( {{\dot{\text{V}}}} \)O2peak achieved in the ramp tests. Potential added value was defined if no \( {{\dot{\text{V}}}} \)O2 plateau occurred and verification \( {{\dot{\text{V}}}} \)O2peak was between 97 and 103% of the \( {{\dot{\text{V}}}} \)O2peak achieved in the ramp test. This condition can be caused by two options: first \( {{\dot{\text{V}}}} \)O2max was reached in the ramp test and confirmed by the verification \( {{\dot{\text{V}}}} \)O2peak; second \( {{\dot{\text{V}}}} \)O2max was not reached in the ramp test but the time to the limit of exercise tolerance in the verification phase was too short to disprove a low \( {{\dot{\text{V}}}} \)O2max. Certain added value was defined if no \( {{\dot{\text{V}}}} \)O2 plateau occurred and verification \( {{\dot{\text{V}}}} \)O2peak was > 103% of the \( {{\dot{\text{V}}}} \)O2peak achieved in the ramp test, suggesting that the verification phase was effective in disproving a low \( {{\dot{\text{V}}}} \)O2max. The probability of verifying the occurrence of a \( {{\dot{\text{V}}}} \)O2max during a ramp test with a verification phase depends on the time to reach the limit of exercise tolerance in the verification phase (Iannetta et al. 2020). Therefore, Pearson correlation between time to the limit of exercise tolerance in the verification phase and the difference between the \( {{\dot{\text{V}}}} \)O2peak achieved in the ramp test and verification phase was calculated. Descriptive data are reported as mean and SD. A significance level of 0.05 was used for two-sided tests. For the analyses, IBM SPSS Statistics for Mac (Version 28, IBM, Armonk, NY, USA) was used. Figures were done in R version 4.1.2 (R-Core-Team 2021).

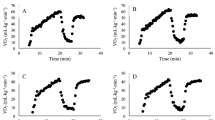
Ratio of verification \( {{\dot{\text{V}}}} \)O2peak divided by \( {{\dot{\text{V}}}} \)O2peak achieved in preliminary ramp test. Presented as a percentage for all tests conducted by participants. Tlim time to the limit of exercise tolerance, \( {{\dot{\text{V}}}} \)O2peak highest oxygen uptake

Classification of all 95% verification phases (A) and 105% verification phases (B) performed into no added value, potential added value, and certain added value
Results
Participants’ characteristics
Fifty-seven participants were assessed for eligibility. Seventeen participants did not meet the inclusion criteria for \( {{\dot{\text{V}}}} \)O2max, one participant was excluded due to the onset of the lockdown policies caused by the coronavirus disease 2019 pandemic, and one participant dropped out for personal reasons unrelated to the study participation. The remaining 38 participants completed the two laboratory appointments, whereby the values of seven of these participants had to be excluded due to technical measurement deficiencies (n = 3), face mask leakage (n = 2), and human error (n = 2). Finally, 17 males and 14 females were included in the analysis. Mean (SD) age, height, body mass, and body fat content were 23 (2) years, 176.8 (5.2) cm, 70.0 (5.2) kg, and 13.3 (5.2) %, for males (n = 17); and 22 (2) years, 165.9 (6.0) cm, 61.2 (8.2) kg, and 18.6 (6.2) %, for females (n = 14), respectively. Mean (SD) of \( {{\dot{\text{V}}}} \)O2peak reached during the ramp test prior to the sub-peak verification phase was 64.5 (6.6) mL·kg−1·min−1 for males and 54.9 (5.9) mL·kg−1·min−1 for females. During the ramp test prior to the supra-peak verification phase, this value was 64.5 (5.9) mL·kg−1·min−1 for males and 54.8 (6.7) mL·kg−1·min−1 for females.
Descriptive statistics
Descriptive findings from both ramp tests and the corresponding verification phase at 95% or 105% of the previously achieved PPO, respectively, are shown in Table 1. Twelve participants did not show a \( {{\dot{\text{V}}}} \)>O2 plateau in either ramp test, while in turn, twelve participants showed a \( {{\dot{\text{V}}}} \)O2 plateau in both ramp tests. In 15 (24.2%) of the 62 ramp tests, no \( {{\dot{\text{V}}}} \)O2 plateau was achieved and a verification \( {{\dot{\text{V}}}} \)O2peak of less than 97% was reached (Fig. 2).
Additional value of verification phase
Figure 1 shows the percentage of \( {{\dot{\text{V}}}} \)O2peak achieved in each verification phase in relation to \( {{\dot{\text{V}}}} \)O2peak achieved in the previous ramp test. Further, Fig. 2 presents the number of tests in which performing a verification phase at an intensity of 95% and 105% of the previously achieved PPO during ramp test, respectively, resulted in no added value, potential added value, and certain added value.
Influence of recovery phase duration
Mean (SD) durations of the recovery phase before the 95% and 105% verification phase were 26:02 (3:40) minutes and 25:44 (3:22) minutes, respectively. All but one male participant had a blood lactate concentration of less than 4 mmol·L−1 by the end of the maximum 30-min recovery phase prior to both verification phases. Mean (SD) blood lactate concentration, heart rate, and rating of perceived exertion at the end of the recovery phase were 3.37 (0.55) mmol·L−1, 124 (13) bpm and 7.6 (1.9), immediately before the 95% verification phase; and 3.40 (0.49) mmol·L−1, 121 (12) bpm and 7.8 (1.9), immediately before the 105% verification phase, respectively.
Influence of the time to the limit of exercise tolerance in verification phase
Mean (SD) time to the limit of exercise tolerance for the sub-peak and supra-peak verification phase were 2:23 (0:24) minutes and 1:38 (0:16) minutes, respectively. The Pearson correlation between the time to the limit of exercise tolerance in the sub-peak verification phase and the difference between the \( {{\dot{\text{V}}}} \)O2peak achieved in the ramp test and verification phase was not significant (r = – 0.258; p > 0.161). Eleven of the 31 sub-peak verification tests resulted in potential value, whereas two of these eleven are unlikely to have added value because the duration of the verification phase was too short. In the remaining nine tests with potential value and a time to the limit of exercise tolerance longer than 2:00 min, almost all secondary \( {{\dot{\text{V}}}} \)O2max criteria were reached during the previously performed ramp test. In detail, all nine participants reached a respiratory exchange ratio of ≥ 1.13 and a maximum heart rate ≥ 93% of 208-(0.7·age), whereas a maximum heart rate ≥ 96% of 210-age and a rating of perceived exertion ≥ 19 were both achieved by eight participants.
For the supra-peak workload, there was a significant negative Pearson correlation between the time to the limit of exercise tolerance in the verification phase and the difference between \( {{\dot{\text{V}}}} \)O2peak achieved in the ramp test and verification \( {{\dot{\text{V}}}} \)O2peak (r = – 0.417; p = 0.020). In only one out of five verification phases resulting in potential value, was the supra-peak power output maintained for > 2:00 min (Fig. 2b). Thus, the supra-peak verification phase might have added value in only one out of 31 participants. Of note, as already seen for the sub-peak test, this one participant reached all applied cutoffs for secondary \( {{\dot{\text{V}}}} \)O2max criteria in the previously conducted ramp test.
Discussion
The main finding of the present study is that sub-peak and supra-peak verification phases following a ramp test both add little value to determining \( {{\dot{\text{V}}}} \)O2max in well-trained male and female adults. For the sub-peak test, \( {{\dot{\text{V}}}} \)O2max could be confirmed with certain value in none and potential value in just 11 of 31 tests. Further, in only 9 of these 11 tests, the power output was sustained long enough to even enable reaching \( {{\dot{\text{V}}}} \)O2max. For the supra-peak test, \( {{\dot{\text{V}}}} \)O2max could be confirmed with certain value in none and potential value in 5 tests, of which 4 showed an insufficient verification test duration of < 2:00 min. Half of all verification tests are obsolete because a \( {{\dot{\text{V}}}} \)O2 plateau is evident during the ramp test. In further 25% of participants, \( {{\dot{\text{V}}}} \)O2 is < 97% of the ramp test, and in further 10% of participants, the verification phase cannot be sustained long enough to enable verification of \( {{\dot{\text{V}}}} \)O2max. Hence the benefits of a verification phase seem minor in comparison to the higher burden for participants and staff.
Additional value of a verification phase
In the absence of a \( {{\dot{\text{V}}}} \)O2 plateau, verification \( {{\dot{\text{V}}}} \)O2peak at 95% and 105% intensity was less than 97% in 35.3% and 64.3% of the tests, respectively, implying that the verification phase also provided no additional benefit. Furthermore, verification \( {{\dot{\text{V}}}} \)O2peak at 95% and 105% intensity was between 97 and 103% of \( {{\dot{\text{V}}}} \)O2peak achieved in the ramp test in 64.7% and 35.7% tests, respectively. Here, the performed verification phase provided a potential added value. This uncertainty relies on two options: either \( {{\dot{\text{V}}}} \)O2max was already reached in the ramp test and confirmed by verification \( {{\dot{\text{V}}}} \)O2peak, or \( {{\dot{\text{V}}}} \)O2max was not reached in the ramp test but the time to the limit of exercise tolerance in the verification phase was too short to disprove a low \( {{\dot{\text{V}}}} \)O2max. Importantly, in none of the tests failing to reach a \( {{\dot{\text{V}}}} \)O2 plateau did the implementation of a verification phase provide certain added value. This applied to both verification phases at 95% and 105% of the PPO achieved in ramp test. Hence, it is evident that performing a verification phase does not yield any additional information on \( {{\dot{\text{V}}}} \)O2max beyond what is already encompassed by the \( {{\dot{\text{V}}}} \)O2 plateau definition.
Considering the findings reported above, implementing our verification phase protocol with an optimal and individualized determination of the intensity and recovery phase duration does not seem to provide a clear additional value in determining \( {{\dot{\text{V}}}} \)O2max in well-trained male and female adults. These findings support the results of a recently published meta-analysis by Costa et al. (2021), which examined apparently healthy adults aged between 19 and 68 years. Overall, the authors concluded that although the verification phase is a robust method for confirming the attainment of \( {{\dot{\text{V}}}} \)O2max during a ramp test, the added value is questionable because the difference in \( {{\dot{\text{V}}}} \)O2peak between ramp test and verification phase is only small (Costa et al. 2021). This agreement between the achieved \( {{\dot{\text{V}}}} \)O2peak in the ramp test and verification phase was not influenced by ramp test protocol, recovery phase (type and duration), and verification phase protocol (intensity and duration) (Costa et al. 2021).
Effects of the verification phase protocol and chosen analytical approach
In this study, a newly conducted verification phase protocol was applied. Most previous studies used only supra-peak verification phase intensity, recovery durations between 3 and 20 min, and group-level analyses (Costa et al. 2021). Moreover, these studies only examined whether verification phases are valuable in determining 'true' \( {{\dot{\text{V}}}} \)O2max (Costa et al. 2021). However, a more expedient question may be, if verification phases provide added value beyond the use of a \( {{\dot{\text{V}}}} \)O2 plateau during the ramp test. The rationale for this is that the presence of a \( {{\dot{\text{V}}}} \)O2 plateau can be identified during a ramp test not necessitating additional burdensome examinations. Furthermore, a \( {{\dot{\text{V}}}} \)O2 plateau is the primary criterion to determine \( {{\dot{\text{V}}}} \)O2max (Howley et al. 1995; Niemeyer et al. 2021; Poole and Jones 2017). In contrast, the present study investigated the usefulness of a sub-peak verification phase in addition to a supra-peak verification phase, implemented exhaustion-depended recovery duration, analyzed the collected data on an individual level, and considered the added value of a verification phase beyond a \( {{\dot{\text{V}}}} \)O2 plateau during ramp test. Rationales for choosing this verification phase protocol are as follows. First, considering that during supra-peak verification phase the limit of exercise tolerance might be reached prematurely, and thus the physical strain cannot be sustained long enough for the \( {{\dot{\text{V}}}} \)O2 kinetics to allow \( {{\dot{\text{V}}}} \)O2max to be confirmed by a plateau (Caputo and Denadai 2008; Hill et al. 2002), a sub-peak verification phase was implemented additionally. Second, by monitoring the duration of the recovery phase before a verification phase through measuring blood lactate concentration, the effect of inadequate recovery can be controlled. Therefore, the occurrence of relevant disturbances in the skeletal muscle milieu due to metabolic acidosis can be excluded when analyzing the data (Schaun 2017). And third, most studies published to date have compared the \( {{\dot{\text{V}}}} \)O2peak achieved during ramp test and verification phase averaged across study participants (Costa et al. 2021). Indeed, Costa et al. (2021) concluded a successful verification, since there were no significant group-level differences between the two \( {{\dot{\text{V}}}} \)O2peak values. However, this is not sufficient for the individual athlete, as the results of the ramp test and the verification phase need to be compared at the level of the individual athlete, taking into account an existing \( {{\dot{\text{V}}}} \)O2 plateau, in order to determine whether the implementation of a verification phase can add value to determining 'true' \( {{\dot{\text{V}}}} \)O2max. To the authors' knowledge, although previous studies with healthy participants have performed individual analyses and assessed the achievement of a \( {{\dot{\text{V}}}} \)O2 plateau during the ramp test (Mier et al. 2012; Murias et al. 2018), the analytical approach described above to determine the added value of a verification phase has never been applied in this way, except in the study by Wagner et al. (2021).
Usefulness of sub-peak verification phase
That \( {{\dot{\text{V}}}} \)O2max achieved in a ramp test can be verified by a sub-peak verification phase has already been shown in several studies (Day et al. 2003; Niemeyer et al. 2019, 2020; Rossiter et al. 2006; Sedgeman et al. 2013). The meta-analysis by Costa et al. (2021) underlines this finding. Thus, differences between the \( {{\dot{\text{V}}}} \)O2peak achieved in a ramp test and verification phase do not differ as a function of the chosen verification phase intensity (Costa et al. 2021). However, it should be noted that verifying \( {{\dot{\text{V}}}} \)O2max using a sub-peak verification phase requires intensities above the critical power (Hill and Ferguson 1999; Hill and Smith 1999; Poole et al. 1988, 1990). Hence, determining the optimal intensity of the sub-peak power output is essential. To note, longer ramp test duration results in a PPO closer to critical power (Morton 2011; Sedgeman et al. 2013). Conceivably, intensities substantially lower than the PPO might cause verification intensity to be below critical power and, therefore, inhibiting attainment of \( {{\dot{\text{V}}}} \)O2max (Sedgeman et al. 2013). That the sub-peak intensity used in the present study is above the critical power can be confirmed by two factors: first, the sub-peak verification phase yielded a \( {{\dot{\text{V}}}} \)O2peak that was not different from the \( {{\dot{\text{V}}}} \)O2peak achieved during the ramp test, and second, the time to the limit of exercise tolerance could only be sustained over a period of 2:23 min. Since \( {{\dot{\text{V}}}} \)O2max can only be achieved above critical power during constant exercise testing (Hill and Ferguson 1999; Hill and Smith 1999; Poole et al. 1988, 1990) and intensities below critical power can be maintain for a very long time without fatigue occurring (Monod and Scherrer 1965), the aforementioned factors indicate that the intensity of 95% of the PPO must be above critical power and consequently suitable for testing \( {{\dot{\text{V}}}} \)O2max.
Usefulness of a supra-peak verification phase
As mentioned beforehand, the time to the limit of exercise tolerance is the commonest limitation in the analysis and interpretation of verification test data. Several authors concluded \( {{\dot{\text{V}}}} \)O2max is reached when the \( {{\dot{\text{V}}}} \)O2peak in the ramp test and the verification phase only deviate by 2–3% (Costa et al. 2021; Dalleck et al. 2012). However, as Wagner et al. (2021) pointed out, this is just one approach. Another explanation might be the inability to sustain the verification power output long enough for the \( {{\dot{\text{V}}}} \)O2 kinetics to allow reaching \( {{\dot{\text{V}}}} \)O2max, and that the verification \( {{\dot{\text{V}}}} \)O2 would indeed be even higher. This approach has been illustrated in Fig. 1 in Wagner et al. (2021). The importance of the time to the limit of exercise tolerance in verification phases arises from findings showing that both healthy young individuals as well as runners and cyclists with fast \( {{\dot{\text{V}}}} \)O2 kinetics appear to require approximately 2:00 min to reach their \( {{\dot{\text{V}}}} \)O2max (Caputo and Denadai 2008; Hill et al. 2002).
In our study, overall, only 3 out of 31 participants reached a sufficient duration of more than 2:00 min in the 105% verification phase. Notably, in 2 of these 3 participants, \( {{\dot{\text{V}}}} \)O2max was already confirmed by a \( {{\dot{\text{V}}}} \)O2 plateau in the previous ramp test. The observed negative correlation between the duration of the supra-peak verification phase and the difference between the highest \( {{\dot{\text{V}}}} \)O2 achieved in the ramp test and verification phase may have resulted from the participants' inability to sustain the supra-peak loading long enough for \( {{\dot{\text{V}}}} \)O2 to reach 'true' \( {{\dot{\text{V}}}} \)O2max. The small number of participants able to maintain the duration for a sufficiently long period is consistent with most studies that have assessed the validity of supra-peak verification phases in healthy untrained, non-specific or specific trained adults (Niemeyer et al. 2021). When considering studies with either specific or non-specific trained participants, fast-increasing work rates in the ramp test, ranging from 25 to 30 W per minute, result in substantially higher PPO (Morton 2011). Consequently, the power output in the verification phase should be linked to the work rate increase in the ramp test. In many studies published to date, an insufficient duration of the supra-peak verification phase to reach \( {{\dot{\text{V}}}} \)O2max was observed, regardless of the implemented intensity (between 105 and 110%) or type of exercise (running or cycling) (Astorino and DeRevere 2018; Nolan et al. 2014; Rossiter et al. 2006; Sedgeman et al. 2013). This is further emphasized in the meta-analysis from Costa et al. (2021). However, it is important to note, that just because in many previous supra-maximal verification phase protocols participants were not able to maintain the duration for a sufficiently long period, this does not mean that it is not possible. The development of “better” protocols could provide additional value in determination of \( {{\dot{\text{V}}}} \)O2max/\( {{\dot{\text{V}}}} \)O2peak in future. For example, Gaesser et al. (1995) claimed that the participants in their study were able to sustain a supra-maximal constant load for at least one minute in duration. However, they did not present the respective data. In participants with very fast \( {{\dot{\text{V}}}} \)O2-kinetics this duration could be sufficient to reach \( {{\dot{\text{V}}}} \)O2max.
Comparison between sub-peak and supra-peak verification phases
In the present study, \( {{\dot{\text{V}}}} \)O2max was more often verified by the verification phase at 95% than at 105% of PPO achieved in the ramp test (Fig. 2). While the 95% verification phase power output was maintained on average for 2:23 (0:24) minutes, the duration of the 105% verification phase averaged only 1:38 (0:16) minutes. Thus, the time to the limit of exercise tolerance in the 95% verification phase is clearly above the 2:00 min required for healthy young individuals as well as runners and cyclists to allow the \( {{\dot{\text{V}}}} \)O2 kinetic to reach 'true' \( {{\dot{\text{V}}}} \)O2max (Caputo and Denadai 2008). Hence, for well-trained male and female adults, performing a sub-peak verification phase seems to be more beneficial than performing a supra-peak verification phase. Note, although sub-peak verification phases may appear preferable, they are still of limited value in determining 'true' \( {{\dot{\text{V}}}} \)O2max in a cohort of well-trained participants, especially when considering the presence of a \( {{\dot{\text{V}}}} \)O2 plateau in the ramp test, as shown by our results.
Influence of recovery phase duration
Prior high-intensity exercise above the lactate threshold has been repeatedly shown to accelerate overall \( {{\dot{\text{V}}}} \)O2 kinetics and reduce the accumulation of blood lactate concentration during a subsequent exercise bout (Bailey et al. 2009; Burnley et al. 2005, 2011). The underlying mechanism of this exercise-induced effect is the subject of intense debate and currently obscure (Bailey et al. 2009). As Bailey et al. (2009) and Burnley et al. (2005) emphasized, myriad physiological changes, including among others enhanced blood flow and muscle O2 availability, increased activity of oxidative muscle enzymes, and altered recruitment profiles of motor units may be underlying mechanism. A significant increase in time to the limit of exercise tolerance (Jones et al. 2003) and mean power output (Burnley et al. 2005) during an exercise bout following prior high-intensity exercise was observed in regularly active individuals and well-trained cyclists, respectively. Participants in both studies exhibited mild elevation in blood lactate concentration of approximately 2.5–3 mmol·L−1 at the onset of the subsequent exercise bout (Burnley et al. 2005; Jones et al. 2003). In contrast, Koppo and Bouckaert (2002) as well as Wilkerson et al. (2004) indicated that prior exercise producing a blood lactate concentration of approximately 6–7 mmol·L−1 had no effect respectively a negative effect on the time to the limit of exercise tolerance during the subsequent exercise bout. Thus, an appropriate combination of prior exercise intensity and recovery phase duration is of paramount importance, and severe lactic acidosis at the onset of the subsequent exercise bout may be accompanied by unchanged or reduced physical performance.
By implementing a recovery phase lasting until blood lactate concentration was ≤ 4 mmol·L−1, the present study aimed to establish an optimal condition for faster \( {{\dot{\text{V}}}} \)O2 kinetics during the verification phase and to increase the probability of a successful \( {{\dot{\text{V}}}} \)O2max verification. However, considering the results of the present study, little added value could be attributed to both the sub-peak and supra-peak verification phases for the determination of 'true' \( {{\dot{\text{V}}}} \)O2max. Thus, overall \( {{\dot{\text{V}}}} \)O2peak achieved in both verification phases did not show any significant increase compared to \( {{\dot{\text{V}}}} \)O2peak from the ramp test. Considering the time to the limit of exercise tolerance of the supra-peak verification phase, compared to the study by Wagner et al. (2021) using an identical verification intensity but a remarkably shorter recovery phase duration, our participants sustained the verification phase for approximately 30 s longer. This may be related to an improved recovery, as our participants showed substantially lower blood lactate concentrations, heart rate, and rate of perceived exertion prior to the verification phase. However, despite individual adjustment of the recovery phase duration based on physiological exhaustion markers, the supra-peak verification phase in our study was preliminary terminated, i.e., a duration of at least 2:00 min was not reached. In conclusion, despite individually timed recovery phase duration, the used verification phase protocol adds little value to the determination of 'true' \( {{\dot{\text{V}}}} \)O2max. The benefit of a lactate-dependent recovery phase duration is therefore debatable, as it reduces the practicability in clinical routine due to increased time expenditure and amount of required blood samples.
Generalizability of the results
It is crucial to emphasize that the present study, as well as the referenced studies supporting our findings, focused mainly on healthy adults. Consequently, the generalizability of the finding that both a sub-peak and a supra-peak verification phase do not contribute substantially to determining 'true' \( {{\dot{\text{V}}}} \)O2max is limited to trained individuals without underlying health conditions. In the context of clinical populations, studies have investigated the usefulness of a verification phase in obese adults (Sawyer et al. 2015), patients with chronic heart disease (Bowen et al. 2012), cancer survivors (Schneider et al. 2020), as well as children, adolescents, and adults with cystic fibrosis (Saynor et al. 2013; Causer et al. 2018). While mean \( {{\dot{\text{V}}}} \)O2peak values achieved during the ramp test and verification phase were mostly not significantly different, on an individual level, the verification phase elicited a higher \( {{\dot{\text{V}}}} \)O2peak values compared to the previous ramp test in 20–66% of the participants (Saynor et al. 2013; Bowen et al. 2012; Sawyer et al. 2015; Schneider et al. 2020). Thus, assuming an underestimation of \( {{\dot{\text{V}}}} \)O2peak during a ramp test in clinical populations, the use of a verification phase may be more justified. In clinical populations a verification phase could serve two purposes. First, it could be used to determine 'true' \( {{\dot{\text{V}}}} \)O2max. It is crucial to emphasize that a higher \( {{\dot{\text{V}}}} \)O2 value measured during the verification phase compared to the ramp test neither confirms the accuracy of the \( {{\dot{\text{V}}}} \)O2peak achieved during the ramp test nor provides a definitive \( {{\dot{\text{V}}}} \)O2max value. For example, probability that the participant may not have reached the \( {{\dot{\text{V}}}} \)O2peak during the verification phase due to slow \( {{\dot{\text{V}}}} \)O2 kinetics is still substantial (Caputo and Denadai 2008). The second purpose of using a verification phase in a clinical population could be to increase the chances of detecting falsely measured \( {{\dot{\text{V}}}} \)O2peak during the incremental protocol. Risk stratification and risk prediction models are all based on \( {{\dot{\text{V}}}} \)O2peak derived from incremental testing, rather than \( {{\dot{\text{V}}}} \)O2max. However, some guidelines suggest certain thresholds to guide clinical decision making (Mancini et al. 1991). Consequently, in some patients, a verification phase test could be beneficial to support clinical decisions for the patient. However, it should be noted that clinical decisions, e.g., for heart transplantation, are not based on a single value but on the whole clinical picture.
Strengths and limitations
In addition to examining both sexes, strengths of the present study included investigating the benefit of a sub-peak verification phase in addition to a supra-peak verification phase, implementing an exhaustion-dependent recovery duration, analyzing the data collected at the individual level, and considering the added value of a verification phase beyond a \( {{\dot{\text{V}}}} \)O2 plateau during the ramp test.
The inclusion of only well-trained participants in the present study has to be acknowledged as a noteworthy limitation. Our findings can thus not be generalized to exercise naïve individuals, clinical populations and older adults unaccustomed to reaching the limits of their exercise tolerance.
Conclusion
In well-trained male and female adults, conducting a sub-peak verification phase following a ramp test may add little value to determining 'true' \( {{\dot{\text{V}}}} \)O2max, while a supra-peak verification phase may add no value. Despite the use of a verification protocol in which factors of intensity and recovery phase duration were implemented optimally and an individual-level analysis was performed, no clear additional benefit was seen by performing a verification phase. Conclusively, the little added value of conducting a sub-peak verification phase for determining \( {{\dot{\text{V}}}} \)O2max barely justifies the enhanced physical strain, time, and financial effort. Further, conducting a supra-peak verification phase showed potential value in only one of the 31 tests performed. Here, confirmation of \( {{\dot{\text{V}}}} \)O2max would already have been possible by secondary \( {{\dot{\text{V}}}} \)O2max criteria. Since a verification phase inflicts substantial additional burden on all participants in addition to the use of \( {{\dot{\text{V}}}} \)O2 plateau and secondary \( {{\dot{\text{V}}}} \)O2max criteria, its use might also be questionable. We infer that performing a verification phase in well-trained and highly motivated adults to determine 'true' \( {{\dot{\text{V}}}} \)O2max can be omitted.
Data availability
Data will be provided upon reasonable request.
Abbreviations
- CPET:
-
Cardiopulmonary exercise testing
- PPO:
-
Peak power output
- \( {{\dot{\text{V}}}} \)O2max :
-
Maximum oxygen uptake
- \( {{\dot{\text{V}}}} \)O2peak :
-
Highest oxygen uptake
- SD:
-
Standard deviation
References
ACSM (2010) ACSM’s guidelines for exercise testing and prescription, 8th edn. Lippincott Williams & Wilkins, Baltimore, MD
Astorino TA, DeRevere J (2018) Efficacy of constant load verification testing to confirm VO2max attainment. Clin Physiol Funct Imaging 38(4):703–709. https://doi.org/10.1111/cpf.12474
Bailey SJ, Vanhatalo A, Wilkerson DP, DiMenna FJ, Jones AM (2009) Optimizing the “priming” effect: influence of prior exercise intensity and recovery duration on O2 uptake kinetics and severe-intensity exercise tolerance. J Appl Physiol 107(6):1743–1756. https://doi.org/10.1152/japplphysiol.00810.2009
Bassett DR (2002) Scientific contributions of A. V. Hill: exercise physiology pioneer. J Appl Physiol 93(5):1567–1582. https://doi.org/10.1152/japplphysiol.01246.2001
Blair SN, Kohl HW III, Barlow CE, Paffenbarger RS Jr, Gibbons LW, Macera CA (1995) Changes in physical fitness and all-cause mortality: a prospective study of healthy and unhealthy men. JAMA 273(14):1093–1098. https://doi.org/10.1001/jama.1995.03520380029031
Borg G (1982) Ratings of perceived exertion and heart rates during short-term cycle exercise and their use in a new cycling strength test. Int J Sports Med 3(3):153–158. https://doi.org/10.1055/s-2008-1026080
Bowen TS, Cannon DT, Begg G, Baliga V, Witte KK, Rossiter HB (2012) A novel cardiopulmonary exercise test protocol and criterion to determine maximal oxygen uptake in chronic heart fail. J Appl Physiol (1985) 113(3):451–458. https://doi.org/10.1152/japplphysiol.01416.2011
Burnley M, Doust JH, Jones AM (2005) Effects of prior warm-up regime on severe-intensity cycling performance. Med Sci Sports Exerc 37(5):838–845. https://doi.org/10.1249/01.mss.0000162617.18250.77
Burnley M, Davison G, Baker JR (2011) Effects of priming exercise on VO2 kinetics and the power-duration relationship. Med Sci Sports Exerc 43(11):2171–2179. https://doi.org/10.1249/MSS.0b013e31821ff26d
Caputo F, Denadai BS (2008) The highest intensity and the shortest duration permitting attainment of maximal oxygen uptake during cycling: effects of different methods and aerobic fitness level. Eur J Appl Physiol 103(1):47–57. https://doi.org/10.1007/s00421-008-0670-5
Causer AJ, Shute JK, Cummings MH, Shepherd AI, Bright V, Connett G, Allenby MI, Carroll MP, Daniels T, Saynor ZL (2018) Cardiopulmonary exercise testing with supramaximal verification produces a safe and valid assessment of VO2max in people with cystic fibrosis: a retrospective analysis. J Appl Physiol 125(4):1277–1283. https://doi.org/10.1152/japplphysiol.00454.2018
Costa VAB, Midgley AW, Carroll S, Astorino TA, de Paula T, Farinatti P, Cunha FA (2021) Is a verification phase useful for confirming maximal oxygen uptake in apparently healthy adults? A systematic review and meta-analysis. PLoS ONE 16(2):e0247057. https://doi.org/10.1371/journal.pone.0247057
Dalleck LC, Astorino TA, Erickson RM, McCarthy CM, Beadell AA, Botten BH (2012) Suitability of verification testing to confirm attainment of VO2max in middle-aged and older adults. Res Sports Med 20(2):118–128. https://doi.org/10.1080/15438627.2012.660825
Day JR, Rossiter HB, Coats EM, Skasick A, Whipp BJ (2003) The maximally attainable VO2 during exercise in humans: the peak vs. maximum issue. J Appl Physiol 95(5):1901–1907. https://doi.org/10.1152/japplphysiol.00024.2003
Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, Bittner VA, Coke LA, Fleg JL, Forman DE, Gerber TC, Gulati M, Madan K, Rhodes J, Thompson PD, Williams MA (2013) Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation 128(8):873–934. https://doi.org/10.1161/CIR.0b013e31829b5b44
Foster C, Kuffel E, Bradley N, Battista RA, Wright G, Porcari JP, Lucia A, deKoning JJ (2007) VO2max during successive maximal efforts. Eur J Appl Physiol 102(1):67–72. https://doi.org/10.1007/s00421-007-0565-x
Franklin BA (2007) Fitness: the ultimate marker for risk stratification and health outcomes? Prev Cardiol 10(1):42–45. https://doi.org/10.1111/j.1520-037x.2007.05759.x
Gaesser GA, Carnevale TJ, Garfinkel A, Walter DO, Womack CJ (1995) Estimation of critical power with nonlinear and linear models. Med Sci Sports Exerc 27(10):1430–1438
Hill DW, Ferguson CS (1999) A physiological description of critical velocity. Eur J Appl Physiol 79(3):290–293. https://doi.org/10.1007/s004210050509
Hill AV, Lupton H (1923) Muscular exercise, lactic acid, and the supply and utilization of oxygen. Proc R Soc Lond B 16(62):135–171. https://doi.org/10.1093/qjmed/os-16.62.135
Hill DW, Smith JC (1999) Determination of critical power by pulmonary gas exchange. Can J Appl Physiol 24(1):74–86. https://doi.org/10.1139/h99-008
Hill DW, Poole DC, Smith JC (2002) The relationship between power and the time to achieve VO2max. Med Sci Sports Exerc 34(4):709–714. https://doi.org/10.1097/00005768-200204000-00023
Howley ET, Bassett DR Jr, Welch HG (1995) Criteria for maximal oxygen uptake: review and commentary. Med Sci Sports Exerc 27(9):1292–1301
Iannetta D, de Almeida AR, Ingram CP, Keir DA, Murias JM (2020) Evaluating the suitability of supra-POpeak verification trials after ramp-incremental exercise to confirm the attainment of maximum O2 uptake. Am J Physiol Regul Integr Comp Physiol 319(3):R315-r322. https://doi.org/10.1152/ajpregu.00126.2020
Jones AM, Wilkerson DP, Burnley M, Koppo K (2003) Prior heavy exercise enhances performance during subsequent perimaximal exercise. Med Sci Sports Exerc 35(12):2085–2092. https://doi.org/10.1249/01.Mss.0000099108.55944.C4
Jones AM, Grassi B, Christensen PM, Krustrup P, Bangsbo J, Poole DC (2011) Slow component of VO2 kinetics: mechanistic bases and practical applications. Med Sci Sports Exerc 43(11):2046–2062. https://doi.org/10.1249/MSS.0b013e31821fcfc1
Knaier R, Niemeyer M, Wagner J, Infanger D, Hinrichs T, Klenk C, Frutig S, Cajochen C, Schmidt-Trucksäss A (2019) Which cutoffs for secondary VO2max criteria are robust to diurnal variations? Med Sci Sports Exerc 51(5):1006–1013. https://doi.org/10.1249/MSS.0000000000001869
Koppo K, Bouckaert J (2002) The decrease in VO2 slow component induced by prior exercise does not affect the time to exhaustion. Int J Sports Med 23(4):262–267. https://doi.org/10.1055/s-2002-29080
Laukkanen JA, Zaccardi F, Khan H, Kurl S, Jae SY, Rauramaa R (2016) Long-term change in cardiorespiratory fitness and all-cause mortality: a population-based follow-up study. Mayo Clin Proc 91(9):1183–1188. https://doi.org/10.1016/j.mayocp.2016.05.014
Lucía A, Rabadán M, Hoyos J, Hernández-Capilla M, Pérez M, San Juan AF, Earnest CP, Chicharro JL (2006) Frequency of the VO2max plateau phenomenon in world-class cyclists. Int J Sports Med 27(12):984–992. https://doi.org/10.1055/s-2006-923833
Mancini DM, Eisen H, Kussmaul W, Mull R, Edmunds LH Jr, Wilson JR (1991) Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation 83(3):778–786. https://doi.org/10.1161/01.cir.83.3.778
Midgley AW, McNaughton LR, Carroll S (2006) Verification phase as a useful tool in the determination of the maximal oxygen uptake of distance runners. Appl Physiol Nutr Metab 31(5):541–548. https://doi.org/10.1139/h06-023
Midgley AW, McNaughton LR, Polman R, Marchant D (2007) Criteria for determination of maximal oxygen uptake: a brief critique and recommendations for future research. Sports Med 37(12):1019–1028. https://doi.org/10.2165/00007256-200737120-00002
Midgley AW, Bentley DJ, Luttikholt H, McNaughton LR, Millet GP (2008) Challenging a dogma of exercise physiology: does an incremental exercise test for valid VO2max determination really need to last between 8 and 12 minutes? Sports Med 38(6):441–447. https://doi.org/10.2165/00007256-200838060-00001
Mier CM, Alexander RP, Mageean AL (2012) Achievement of VO2max criteria during a continuous graded exercise test and a verification stage performed by college athletes. J Strength Cond Res 26(10):2648–2654. https://doi.org/10.1519/JSC.0b013e31823f8de9
Monod H, Scherrer J (1965) The work capacity of a synergic muscular group. Ergonomics 8(3):329–338. https://doi.org/10.1080/00140136508930810
Morton RH (2011) Why peak power is higher at the end of steeper ramps: an explanation based on the “critical power” concept. J Sports Sci 29(3):307–309. https://doi.org/10.1080/02640414.2010.534809
Murias JM, Pogliaghi S, Paterson DH (2018) Measurement of a true VO2max during a ramp incremental test is not confirmed by a verification phase. Front Physiol 9:143. https://doi.org/10.3389/fphys.2018.00143
Niemeyer M, Leithaeuser R, Beneke R (2019) Oxygen uptake plateau occurrence depends on oxygen kinetics and oxygen deficit accumulation. Scand J Med Sci Sports 29(10):1466–1472. https://doi.org/10.1111/sms.13493
Niemeyer M, Bergmann TGJ, Beneke R (2020) Oxygen uptake plateau: calculation artifact or physiological reality? Eur J Appl Physiol 120(1):231–242. https://doi.org/10.1007/s00421-019-04267-7
Niemeyer M, Knaier R, Beneke R (2021) The oxygen uptake plateau – a critical review of the frequently misunderstood phenomenon. Sports Med 51(9):1815–1834. https://doi.org/10.1007/s40279-021-01471-4
Nolan PB, Beaven ML, Dalleck L (2014) Comparison of intensities and rest periods for VO2max verification testing procedures. Int J Sports Med 35(12):1024–1029. https://doi.org/10.1055/s-0034-1367065
Poole DC, Jones AM (2017) Measurement of the maximum oxygen uptake VO2max: VO2peak is no longer acceptable. J Appl Physiol 122(4):997–1002. https://doi.org/10.1152/japplphysiol.01063.2016
Poole DC, Ward SA, Gardner GW, Whipp BJ (1988) Metabolic and respiratory profile of the upper limit for prolonged exercise in man. Ergonomics 31(9):1265–1279. https://doi.org/10.1080/00140138808966766
Poole DC, Ward SA, Whipp BJ (1990) The effects of training on the metabolic and respiratory profile of high-intensity cycle ergometer exercise. Eur J Appl Physiol Occup Physiol 59(6):421–429. https://doi.org/10.1007/bf02388623
R-Core-Team (2021) R: a language and environment for statistical computing. Available from: https://www.R-project.org/
Rossiter HB, Kowalchuk JM, Whipp BJ (2006) A test to establish maximum O2 uptake despite no plateau in the O2 uptake response to ramp incremental exercise. J Appl Physiol 100(3):764–770. https://doi.org/10.1152/japplphysiol.00932.2005
Sawyer BJ, Tucker WJ, Bhammar DM, Gaesser GA (2015) Using a verification test for determination of VO2max in sedentary adults with obesity. J Strength Cond Res 29(12):3432–3438. https://doi.org/10.1519/jsc.0000000000001199
Saynor ZL, Barker AR, Oades PJ, Williams CA (2013) A protocol to determine valid VO2max in young cystic fibrosis patients. J Sci Med Spor 16(6):539–544. https://doi.org/10.1016/j.jsams.2013.01.010
Scharhag-Rosenberger F, Carlsohn A, Cassel M, Mayer F, Scharhag J (2011) How to test maximal oxygen uptake: a study on timing and testing procedure of a supramaximal verification test. Appl Physiol Nutr Metab 36(1):153–160. https://doi.org/10.1139/h10-099
Schaun GZ (2017) The maximal oxygen uptake verification phase: a light at the end of the tunnel? Sports Med Open 3(1):44. https://doi.org/10.1186/s40798-017-0112-1
Schaun GZ, Alberton CL, Gomes MLB, Santos LP, Bamman MM, Mendes GF, Häfele MS, Andrade LS, Alves L, De Ataides VA, Carmona MA, Lázaro R, Botton CE, Umpierre D, Pinto SS, Wilhelm EN (2021) Maximal oxygen uptake is underestimated during incremental testing in hypertensive older adults: findings from the HAEL study. Med Sci Sports Exerc 53(7):1452–1459. https://doi.org/10.1249/mss.0000000000002598
Schneider J, Schlüter K, Wiskemann J, Rosenberger F (2020) Do we underestimate maximal oxygen uptake in cancer survivors? Findings from a supramaximal verification test. Appl Physiol Nutr Metab 45(5):486–492. https://doi.org/10.1139/apnm-2019-0560
Sedgeman D, Dalleck L, Clark IE, Jamnick N, Pettitt RW (2013) Analysis of square-wave bouts to verify VO2max. Int J Sports Med 34(12):1058–1062. https://doi.org/10.1055/s-0033-1341436
Shephard RJ (1988) PAR-Q, canadian home fitness test and exercise screening alternatives. Sports Med 5(3):185–195. https://doi.org/10.2165/00007256-198805030-00005
Wagner J, Niemeyer M, Infanger D, Hinrichs T, Streese L, Hanssen H, Myers J, Schmidt-Trucksäss A, Knaier R (2020) New data-based cutoffs for maximal exercise criteria across the lifespan. Med Sci Sports Exerc 52(9):1915–1923. https://doi.org/10.1249/mss.0000000000002344
Wagner J, Niemeyer M, Infanger D, Hinrichs T, Guerra C, Klenk C, Königstein K, Cajochen C, Schmidt-Trucksäss A, Knaier R (2021) Verification-phase tests show low reliability and add little value in determining VO2max in young trained adults. PLoS ONE 16(1):e0245306. https://doi.org/10.1371/journal.pone.0245306
Wilkerson DP, Koppo K, Barstow TJ, Jones AM (2004) Effect of prior multiple-sprint exercise on pulmonary O2 uptake kinetics following the onset of perimaximal exercise. J Appl Physiol 97(4):1227–1236. https://doi.org/10.1152/japplphysiol.01325.2003
Yoon BK, Kravitz L, Robergs R (2007) VO2max, protocol duration, and the VO2 plateau. Med Sci Sports Exerc 39(7):1186–1192. https://doi.org/10.1249/mss.0b13e318054e304
Acknowledgements
We thank all the participants who made this study possible by their participation.
Funding
Open access funding provided by University of Basel. F.B. and R.K. are funded by the Swiss National Science Foundation, Grant No. PZ00P3_208999.
Author information
Authors and Affiliations
Contributions
FB wrote the original draft of the article. RK, MN, JW, FS, RS, and AS-T participated in the review and editing of the article. FB, FS, and RK participated in the visualization of the data. RK, MN, JW, and AST participated in the concept and design. FB and RS participated in the data acquisition. FB, RK, and MN participated in the data analysis and interpretation.
Corresponding author
Ethics declarations
Conflict of interest
None of the authors involved in the present study have any conflict of interest, financial, personal, or otherwise, which would influence this research.
Additional information
Communicated by Susan Hopkins.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bruggisser, F., Wagner, J., Niemeyer, M. et al. A verification phase adds little value to the determination of maximum oxygen uptake in well-trained adults. Eur J Appl Physiol 124, 1669–1681 (2024). https://doi.org/10.1007/s00421-023-05388-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-023-05388-w