
Abstract
Purpose
This study examined the haematological adaptations to high-intensity interval training (HIT), i.e. total haemoglobin mass (tHb-mass), blood volume (BV), and plasma volume (PV), and its effects on VO2max in well-trained athletes.
Methods
Twenty-seven male and eight female well-trained (VO2max 63.7 ± 7.7 ml/min/kg) athletes were randomly assigned to the HIT (HITG, N = 19) or the control group (CG, N = 16). Over a 3-week period, the HITG performed 11 HIT sessions, consisting of four 4-min interval bouts at an exercise intensity of 90–95 % of the individual maximal heart rate (HRmax), separated by 4-min active recovery periods. Before and 5 ± 2 days after the intervention, tHb-mass, BV and PV were determined by the CO-rebreathing method. VO2max was assessed in a laboratory treadmill test.
Results
tHb-mass (from 753 ± 124 to 760 ± 121 g), BV (from 5.6 ± 0.8 to 5.6 ± 0.9 l) and PV (from 3.2 ± 0.5 to 3.2 ± 0.5 l) remained unchanged after HIT and did not show an interaction (group × time). Within the HITG, VO2max improved from baseline by +3.5 % (p = 0.011), but remained unchanged in the CG. No interaction (group × time) was seen for VO2max. The HITG showed a significant reduction in HRmax compared to the baseline measurement (−2.3 %, p ≤ 0.001), but HRmax remained unchanged in the CG. There was a significant interaction (group × time) for HRmax (p = 0.006). Also, oxygen pulse significantly increased only in HITG from 22.9 ± 4.4 to 23.9 ± 4.2 ml/beat, with no interaction (p = 0.150).
Conclusions
Eleven HIT sessions added to usual training did neither improve VO2max nor haematological parameters compared to the CG.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
High-intensity interval training (HIT) consisting of short bouts of vigorous intensity exercise, interspersed with low-intensity recovery periods, seems to be the most effective method to improve exercise performance not only in well-trained athletes but also in sedentary and diseased individuals (Astorino et al. 2012; Breil et al. 2010a; Helgerud et al. 2007; Iaia et al. 2009; Jacobs et al. 2013; Laursen et al. 2002). However, as the favourable effects of HIT on VO2max are well established, the underlying mechanism explaining these improvements, especially in well-trained athletes, remains partly elusive. It has been shown that in endurance-trained athletes, VO2max is predominantly determined by the oxygen supply (Steiner and Wehrlin 2011). Both blood volume (BV) and haemoglobin (Hb) particularly contribute to the amount of oxygen delivery by increasing both cardiac output (Q) and oxygen content of arterial blood (Pottgiesser and Schumacher 2013; Warburton et al. 2000). In contrast to their sedentary or not endurance-trained counterparts, endurance-trained athletes possess a considerably higher body weight-related haemoglobin mass (Hb-mass) and a higher BV (Krip et al. 1997; Schmidt et al. 2002; Steiner and Wehrlin 2011; Warburton et al. 2004). However, whether the Hb-mass and BV of already well-trained athletes can be further increased by high-intensity training and therefore contribute to enhanced VO2max, remains unclear. Several investigations demonstrated unchanged Hb-mass in trained athletes, independently of intensification of the training (Glass et al. 1969; Gore et al. 1997). In contrast, Breil et al. (2010b) have shown significantly increased Hb-mass (+9.9 %) and BV (+10.0 %) after 15 HIT sessions (4 × 4 min at 90–95 % of maximal heart rate (HRmax)) in elite junior skiers with concomitant increase of VO2max, suggesting Hb-mass and BV are responsible for improved VO2max after HIT. However, Helgerud et al. (2007) failed to demonstrate training-induced changes in BV after 8 weeks of HIT (4 × 4 min at 90–95 % HRmax) despite significantly improved VO2max in moderately trained subjects. Investigations showed exercise intensity as the main stimulus for training-induced hypervolaemia (Convertino 1991; Nagashima et al. 1999). This is manifested by significant increases in BV after short-term HIT in trained athletes (Green et al. 1984; Richardson et al. 1996). Richardson et al. (1996) reported increased PV (+4.4 %) even after 2 days of HIT in trained (VO2max 60.7 ± 6.4 ml/min/kg) men. In untrained males, 12 weeks of interval training resulted in significant increased VO2max and BV. The training-induced hypervolaemia accounted for 47 % of the VO2max changes (Warburton et al. 2004). Nevertheless, in a recent investigation, Jacobs et al. (2013) failed to demonstrate increases in total haemoglobin mass (tHb-mass), BV, PV, and maximal cardiac output (Qmax) after six HIT sessions in untrained individuals, although VO2max and endurance performance improved.
Due to these contradictory findings, as well the paucity of data on haematological adaptations to HIT in well-trained athletes, the present study aimed to examine the impact of HIT on changes in tHb-mass, BV, and PV, explaining VO2max in already well-trained athletes. We hypothesized that the increase in VO2max caused by HIT would be directly related to differences in training-induced hypervolaemia and increased tHb-mass.
Materials and methods
The present paper pools the main outcome variables (tHb-mass, BV, PV, VO2max and maximal oxygen pulse (O2-pulse)) of two HIT investigations. Both sought to investigate haematological adaptations to 3-week HIT in well-trained individuals with the same training intervention and main outcome variables but different treadmill protocols.
Participants
Overall, eight female and twenty-seven male well-trained sport students participated in the study. All study participants underwent a routine pre-participation screening prior to the baseline testing. Age and physical characteristics of the participants are presented in Table 1. Normal exercise load of the subjects was 9.5 ± 5.0 h/week. Possible exclusion criteria were all types of acute and chronic diseases, smoking or pregnancy.
The study was carried out according to the Declaration of Helsinki and was approved by the Institutional Review Board of the Department of Sport Science (University Innsbruck). All participants gave written informed consent to participate in the study.
Study protocol
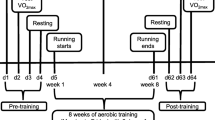
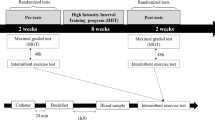
The study was designed as a randomized controlled training study including HIT and control group (HITG and CG, respectively) and two measurement times (baseline vs. post-training). Baseline measurements included the determination of haematological parameters and a laboratory treadmill test. After baseline measurements, the participants were randomly assigned, stratified by gender and VO2max (determined in the laboratory treadmill test) either to the HITG or the CG. After a break of at least 4 days, the HITG started the 3-week HIT program whereas CG maintained their usual training during this period. Post-training measurements were the same as for baseline condition and were conducted 5 ± 2 days after the last HIT session. Haematological parameters were measured by a blinded investigator.
Baseline and post-training measurements
All measurements were performed in the laboratories of the Department of Sport Science of the University Innsbruck (Austria) at an altitude of 590 m. Participants were instructed to refrain from intense exercise 24 h before the baseline and post-training measurements and to appear fully hydrated on the test day.
Haematological parameters
The carbon monoxide (CO) rebreathing method, according to Schmidt and Prommer (2005), was used to determine tHb-mass and BV. After the participants had spent 5 min in a sitting position, hyperaemized capillary blood was taken from a fingertip to analyse Hb (g/dl), Hct (%), and HbCO (Auto Counter AC 920, Swelab Instruments, Stockholm, Sweden). Subsequently, participants inhaled a bolus of carbon monoxide (CO) corresponding to 1 mL × kg−1 body mass. Then, they had to stop breathing for 10 s before they started rebreathing the gas mixture for another 1.50 min in a closed circuit (glass spirometer, Blood Tec GbR, Bayreuth, Germany). Subsequently, capillary blood samples were analysed for HbCO 6 and 8 min after the inhalation of the CO. The end-tidal CO concentration was measured with a CO gas-tester (CO-220, Fluke, Canada).
According to Schmidt and Prommer (2005, 2008), this method is valid for the estimation of tHb-mass with a typical error of 1.7 %. After familiarization with this method, a typical error between 1.5 and 1.7 % was observed in our lab derived from duplicate and triplicate determinations.
Laboratory treadmill testing
Tests were carried out on the electrically driven treadmill (h/p/cosmos pulsar, h/p/cosmos Sports and Medical, Nussdorf-Traunstein, Germany). As mentioned above, two different treadmill protocols were used to assess VO2max, with no differences in achieving VO2max. The following treadmill protocol, as described in detail by Burtscher et al. (2008), was used to assess VO2max in the first investigation. Exercise started at 5 km/h and 5 % inclination, after 2 min inclination was set at 10 % for 2 min. Subsequently, running speed was increased to 6 km/h and inclination was augmented by 2 % every minute until 20 %. Finally, inclination was kept constant at 20 % and running speed was increased by 1 km/h per minute (Burtscher et al. 2008). The test was completed when the athlete was subjectively exhausted despite verbal encouragement. In investigation 2, the treadmill protocol according to Burtscher et al. (2010) was used. Participants started at 10 km/h and 1 % inclination for 1 min followed by 1 min at 11 km/h and 1 % inclination. Afterwards, running speed was set to 12, 14 and 16 km/h with the same inclination, each speed level was performed for 4 min. Afterwards, speed was increased by 1 km/h every minute. When 20 km/h were reached, speed was kept constant and inclination increased by 2 % every minute (Burtscher et al. 2010).
Gas analysis was performed using an open spirometric system (Oxycon Mobile, Care Fusion, Würzburg, Germany) which was calibrated before each measurement, according to the manufacturer’s guidelines. Ventilatory parameters (i.e. VE, O2-pulse, VO2, VCO2) were recorded breath by breath during the ergospirometry. Heart rate (HR) was determined by chest belt (Wear Link, Polar, Kempele, Finland) and transmitted to the spirometric device. VAT was determined at the point at which VE/VO2 reaches the minimum value and begins to rise without a concomitant rise in VE/VCO2 (Wassermann et al. 1973). A test was considered maximal when three of the following criteria were fulfilled: (1) VO2 plateau at peak exercise (2) respiratory exchange ratio ≥1.10 (3) peak HR ≥90 % of the theoretic maximal HR (220-age), and (4) indication of maximal exhaustion by the athlete (Cunha et al. 2010). VO2max was defined as the highest 30 s average in oxygen uptake and maximal heart rate (HRmax) as the highest 5 s average during the test.
HIT program
The HITG performed 11 HIT sessions during the 3-week HIT period. Each HIT session consisted of four 4-min interval bouts at an exercise intensity of 90–95 % of the HRmax, separated by 4-min active recovery periods (work/rest ratio = 1:1). In the first week, athletes completed three HIT sessions and in the following 2 weeks four HIT sessions each week. On the remaining days, the HITG continued their individual training. For the additional training of the HITG, we recommended low-intensity, regenerative training.
All HIT sessions took place on an athletic 400 m track and were supervised by two investigators. Training intensity was controlled by continuous HR monitoring (Polar, Kempele, Finland) and the rating of perceived exertion (RPE) was determined according to the Borg scale (6–20; Borg 1982). HR after 2 min and HR at the end of the interval bout, as well as RPE, were directly listed after each interval bout. The HIT sessions were performed in training groups of 4–6 athletes and started with a standardized 15-min warm-up at 70–75 % HRmax (determined at the maximal treadmill test), five running drills and three submaximal progressive sprints over about 100 m. The athletes of the CG maintained their usual endurance and strength training during the 3-week intervention period. In particular, they were advised not to include additional high-intensity training. The training data (i.e. includes all endurance training performed during the 3-week training period) for the HITG and the CG were recorded in a training log book and the total endurance training loads were determined according to Foster et al. (2001) as perceived exertion × endurance training session time.
Statistical analysis
Statistical analyses were conducted by PASW Statistics 19 (IBM, Vienna, Austria). Statistical power for the chosen sample size of 35 (19 in the HITG and 16 in the CG) amounted to >90 %; alpha = 0.05. Power calculation (G*Power 3.1.7) was based on the findings of Warburton et al. (2004) considering expected changes in VO2max, PV and BV due to HIT. Normal distribution of data was tested by the Kolmogorov–Smirnov test. A two-way analysis (group × time) of variance (ANOVA) with repeated measurements was used to verify between-group changes. ANOVA was also applied to evaluate a possible gender effect (group × time × gender). In addition, paired student’s t tests were carried out to evaluate within-group effects. The relationships between variables were assessed by correlation analyses (Pearson). p values <0.05 (two-tailed) were considered to indicate statistical significance. Values are presented as mean ± SD.
Results
No gender effect was identified with regard to the parameters of interest (tHb-mass, BV, PV, VO2max, HRmax and maximal O2-pulse), allowing us to pool the main outcome variables of both sexes.
Haematological parameters
No interaction (group × time) was found for tHb-mass, BV, PV and Hct (Table 2). Within the HITG, tHb-mass (from 753 ± 124 to 760 ± 121 g), BV (from 5. 6 ± 0.8 to 5.6 ± 0.9 l) and PV (from 3.2 ± 0.5 to 3.2 ± 0.5 l) remained unchanged after HIT. Mean values for tHb-mass, BV and PV are shown in Table 2.
Laboratory treadmill testing
Outcomes of the performance testing are shown in Table 2. The participants were all sport students and appeared motivated to take the tests. Of all the participants, 88.6 % reached a plateau of VO2 during the baseline test and 85.7 % during the post-test. For the baseline test, 16 out of 35 participants and for the post-test, 10 out of 35 persons fulfilled all four criteria for a maximal test according to Cunha et al. (2010). All participants reached a RER ≥1.05. For the baseline and post-test, 80 and 71.4 %, respectively, of all participants reached a RER ≥1.1. There was no difference in attaining VO2max between both treadmill protocols.
VO2max (ml/min/kg) significantly increased in the HITG (+3.5 %, p = 0.011) from 63.6 ± 7.5 to 65.8 ± 7.1 ml/min/kg, but remained unchanged in the CG. There was no interaction (group × time) for VO2max. The HITG showed a significant reduction in HRmax compared to the baseline measurement from 196 ± 6 to 191 ± 5 bpm (−2.3 %, p ≤ 0.001), but HRmax remained unchanged in the CG. There was a significant interaction (group × time) for HRmax (p = 0.006). Maximal O2-pulse significantly increased in the HITG (+4.7 %, p = 0.012) from 22.9 ± 4.4 to 23.9 ± 4.2 ml/beat but remained unchanged in the CG. However, there was no interaction (group × time) for maximal O2-pulse. No significant correlation between changes in HRmax and changes in VO2max (r = −0.079; p = 0.748) was seen for the HITG.
Training data
All participants completed the study with no adverse events. Except for one person, who performed only 10 HIT sessions, all other athletes of the HITG completed 11 HIT sessions. Twelve out of 19 training log books were filled in completely and used for the evaluation of the entire training load. The remaining seven training report forms could not be included in the evaluation due to incomplete information (missing BORG and/or training session time). Data of endurance training loads for each week are presented in Table 3. The total training load did not differ between groups during the 3-week intervention period (HITG: 11,087 ± 5193; CG: 12,576 ± 5766; p = 0.489) nor did any other of the training data. Mean heart rate responses and mean ratings of perceived exertion over all HIT sessions are presented in Table 4. In all but the last HIT session, participants reached their target heart rate of 90–95 % of HRmax within the first 2 min and maintained it to the end of the HIT bout. Mean ratings of perceived exertion (BORG) during all eleven HIT sessions were ranged between 16.7 ± 1.4 and 17.3 ± 1.5. Two participants did not entirely reach their target heart rate in all exercise sessions (average training heart rate 88.3 and 87.3 % of HRmax, respectively).
Discussion
The main results of the present study are that after a 3-week HIT program, VO2max only increased within the HITG with concomitant decreases of HRmax and increases in maximal O2-pulse but without any changes in tHb-mass, BV and PV. However, despite a within-group change of VO2max, no interaction (group × time) was seen for VO2max, tHb-mass, BV, PV and maximal O2-pulse, indicating no significant effect of HIT. The findings from the present investigation do not support our hypothesis that VO2max changes after 3 weeks of HIT are directly related to differences in training-induced hypervolaemia and/or increases in tHb-mass. There are several studies, demonstrating no significant relationship between VO2max and tHb-mass/vascular volume after a HIT intervention in trained subjects (Glass et al. 1969; Gore et al. 1997; Laursen et al. 2005; Helgerud et al. 2007). In their study, Laursen et al. (2005) investigated the influence of three different HIT regimes on PV, anaerobic capacity and ventilatory thresholds in well-trained cyclists. The authors demonstrated increased 40 km time-trial performance, improved VO2peak, ventilatory thresholds, and anaerobic capacity while PV did not change significantly. They suspected that peripheral adaptations and not central adaptation are more likely to be responsible for performance improvements. However, previous investigations, particularly with untrained subjects, reported improved VO2max and increased vascular volume after HIT (Esfandiari et al. 2014; Warburton et al. 2004). Moreover, several investigations exist, reporting increases in tHb-mass and vascular volume after HIT in well-trained individuals (Breil et al. 2010b; Richardson et al. 1996). The considerable discrepancy is likely due to different training protocols and primarily to different participant characteristics. In endurance-trained athletes, body weight-related tHb-mass and BV levels are described as considerably higher than in untrained subjects (Krip et al. 1997; Schmidt et al. 2002; Steiner and Wehrlin 2011; Warburton et al. 2004), suggesting endurance-trained athletes may already be well adapted and seem to be at their optimal BV (Warburton et al. 1999, 2000). Thus, in well-trained athletes higher HIT doses might be necessary to generate changes in vascular volume and tHb-mass when compared to untrained individuals. In untrained individuals, tHb-mass and BV were reported to be 11.5 g/kg and 75 ml/kg, whereas endurance-trained athletes exhibit values of 15.7 g/kg and 103.4 ml/kg, respectively (Schmidt et al. 2002), showing a training-dependent increase in both tHb-mass and BV. On the other hand, in their recent investigation, Jacobs et al. (2013) reported similar findings to our present study, but in untrained individuals. After six HIT sessions within 2 weeks (8–12 × 60 s cycling intervals at 100 % peak power output), VO2max improved by 8 % while tHb-mass, BV, PV and Q remained unaltered. Although several investigations reported high-intensity training-induced PV expansion (Esfandiari et al. 2014; Richardson et al. 1996), it can therefore be assumed to be a transient effect (Jacobs et al. 2013).
We found significantly improved maximal O2-pulse only in HITG. Considering the facts that BV and Qmax are closely related (Bonne et al. 2014; Krip et al. 1997) and BV did not change significantly after the 3-week HIT, it is suggested that Q remained essentially unchanged. Thus, increased SV should have compensated for the reduced HRmax partly explaining the elevated maximal O2-pulse. If true, it will be mainly the maximal arterial–venous O2 content difference (avDO2) that explains the increased VO2max. HIT adaptations may result from peripheral adaptation as alterations in maximal avDO2, based on increased capillarization and mitochondrial density (Daussin et al. 2008; Jensen et al. 2004; Wahl et al. 2014).
The presented data demonstrate a significant improved VO2max of +3.5 % after 3 weeks of HIT in already well-trained individuals. Helgerud et al. (2007), using the same four × 4-min intervals, achieved an improvement of 7.2 % after 4 weeks of HIT. However, in contrast to the present study, baseline VO2max values were markedly lower in that study compared to our participants (55.5 ± 7.4 vs. 63.6 ± 7.5 ml/min/kg). The effect that subjects with lower baseline values benefited more than subjects with higher VO2max is in line with previous studies showing that VO2max at baseline and changes in VO2max are significantly correlated (McMillan et al. 2005). However, when considering the average increase of VO2max per training session, the present study showed an increase in VO2max of 0.32 % per session, while VO2max increased by about 0.3 % per session in the study of Helgerud et al. (2007).
Another interesting finding of the present study was that HRmax decreased due to HIT. However, changes in HRmax and changes in VO2max were unrelated, suggesting that HRmax reduction does not contribute to VO2max improvements after 3 weeks of HIT. The suppressed HRmax was already observed in other HIT investigations (Breil et al. 2010a; Etxebarria et al. 2014) and is most likely due to increased cardiac vagal activity (Kiviniemi et al. 2014) and cardiovagal baroreflex function (Zavorsky 2000).
Study limitations
Some limitations have to be mentioned. We combined the outcomes of two independent investigations to obtain a high number of participants, necessary for investigating the underlying mechanism. Therefore, two different laboratory treadmill tests were performed. Nonetheless, the intervention and the main outcome variables remained the same in both investigations (VO2max, tHb-mass, BV and PV). In addition, we did not determine HIT-related changes on the level of working muscles but this was not a study goal as we aimed at investigating possible changes of tHb-mass, BV and PV, explaining VO2max. Despite the high calculated power for the chosen sample size, we were unable to detect between-group changes of VO2max. However, power calculation was based on not well-trained subjects and therefore we cannot exclude that our study may have been underpowered particularly with regard to BV and PV. Regarding VO2max, other HIT studies (Breil et al. 2010a; Helgerud et al. 2007) with the same HIT protocol (4 × 4 min at 90–95 % of HRmax) and with well-trained subjects had only 10 and 13 subjects, respectively (in the HITG), and showed significant changes. This indicates that 19 participants in the HITG should have been sufficient do detect VO2max changes.
Conclusion
Eleven HIT sessions added to usual training did neither improve VO2max nor haematological parameters when compared to the CG. Probably, 11 HIT sessions did not provide a sufficient overload to improve VO2max and stimulate haematological changes in well-trained athletes. Future research should focus on potential performance and blood effects after more intensified HIT.
Abbreviations
- ANOVA:
-
Analysis of variance
- avDO2 :
-
Arterial–venous O2 content difference
- BV:
-
Blood volume
- CG:
-
Control group
- CO:
-
Carbon monoxide
- Hb:
-
Haemoglobin
- Hct:
-
Haematocrit
- HIT:
-
High-intensity interval training
- HITG:
-
High-intensity interval training group
- HR:
-
Heart rate
- HRmax :
-
Maximal heart rate
- O2-pulse:
-
Oxygen pulse
- PV:
-
Plasma volume
- Q:
-
Cardiac output
- Qmax :
-
Maximal cardiac output
- SV:
-
Stroke volume
- tHb-mass:
-
Total haemoglobin mass
- VO2max :
-
Maximal oxygen uptake
References
Astorino TA, Allen RP, Roberson DW, Jurancich M (2012) Effect of high-intensity interval training on cardiovascular function, VO2max, and muscular force. J Strength Cond Res 26(1):138–145. doi:10.1519/JSC.0b013e318218dd77
Bonne TC, Doucende G, Flück D, Jacobs RA, Nordsborg NB, Robach P, Walther G, Lundby C (2014) Phlebotomy eliminates the maximal cardiac output response to six weeks of exercise training. Am J Physiol Regul Integr Comp Physiol 306(10):R752–R760. doi:10.1152/ajpregu.00028.2014
Borg G (1982) Psychophysical bases of perceived exertion. Med Sci Sports Exerc 14(5):377–381
Breil FA, Weber SN, Koller S, Hoppeler H, Vogt M (2010a) Block training periodization in alpine skiing: effects of 11-day HIT on VO2max and performance. Eur J Appl Physiol 109(6):1077–1086. doi:10.1007/s00421-010-1455-1
Breil FA, Weber SN, Fontana P, Hoppeler H, Vogt M (2010b) Block periodization oh high intensity interval training (HIT): underlying adaptive mechanisms for the efficient VO2max improvement. In: Korkusuz F, Ertan H, Tsolakidis E (eds) Book of abstracts of the 15th annual congress of the European College of Sports Science, Antalya, Turkey, p 480
Burtscher M, Förster H, Burtscher J (2008) Superior endurance performance in aging mountain runners. Gerontology 54(5):268–271. doi:10.1159/000148649
Burtscher M, Gatterer H, Faulhaber M, Gerstgrasser W, Schenk K (2010) Effects of intermittent hypoxia on running economy. Int J Sports Med 31(9):644–650. doi:10.1055/s-0030-1255067
Convertino VA (1991) Blood volume: its adaptation to endurance training. Med Sci Sports Exerc 23(12):1338–1348
Cunha FA, Midgley AW, Monteiro WD, Farinatti PT (2010) Influence of cardiopulmonary exercise testing protocol and resting VO2 assessment on %HRmax, %HRR, %VO2max and %VO2R relationships. Int J Sports Med 31(5):319–326. doi:10.1055/s-0030-1248283
Daussin FN, Zoll J, Dufour SP, Ponsot E, Lonsdorfer-Wolf E, Doutreleau S, Mettauer B, Piquard F, Geny B, Richard R (2008) Effect of interval versus continuous training on cardiorespiratory and mitochondrial functions: relationship to aerobic performance improvements in sedentary subjects. Am J Physiol Regul Integr Comp Physiol 295(1):R264–R272. doi:10.1152/ajpregu.00875.2007
Esfandiari S, Sasson Z, Goodman JM (2014) Short-term high-intensity interval and continuous moderate-intensity training improve maximal aerobic power and diastolic filling during exercise. Eur J Appl Physiol 114(2):331–343. doi:10.1007/s00421-013-2773-x
Etxebarria N, Anson JM, Pyne DB, Ferguson RA (2014) High-intensity cycle interval training improves cycling and running performance in triathletes. Eur J Sport Sci 14(6):521–529. doi:10.1080/17461391.2013.853841
Foster C, Florhaug JA, Franklin J, Gottschall L, Hrovatin LA, Parker S, Doleshal P, Dodge C (2001) A new approach to monitoring exercise training. J Strength Cond Res 15(1):109–115
Glass HI, Edwards RH, De Garreta AC, Clark JC (1969) 11CO red cell labeling blood volume and total hemoglobin in athletes: effect of training. J Appl Physiol 26(1):131–134
Gore CJ, Hahn AG, Burge CM, Telford RD (1997) VO2max and haemoglobin mass of trained athletes during high intensity training. Int J Sports Med 18(6):477–482
Green HJ, Thomson JA, Ball ME, Hughson RL, Houston ME, Sharratt MT (1984) Alterations in blood volume following short-term supramaximal exercise. J Appl Physiol 56(1):145–149
Helgerud J, Høydal K, Wang E, Karlsen T, Berg P, Bjerkaas M, Simonsen T, Helgesen C, Hjorth N, Bach R, Hoff J (2007) Aerobic high-intensity intervals improve VO2max more than moderate training. Med Sci Sports Exerc 39(4):665–671. doi:10.1249/mss.0b013e3180304570
Iaia M, Hellsten Y, Nielsen JJ, Fernström M, Sahlin K, Bangsbo J (2009) Four weeks of speed endurance training reduces energy expenditure during exercise and maintains muscle oxidative capacity despite a reduction in training volume. J Appl Physiol (1985) 106(1):73–80. doi:10.1152/japplphysiol.90676.2008
Jacobs RA, Flück D, Bonne TC, Bürgi S, Christensen PM, Toigo M, Lundby C (2013) Improvements in exercise performance with high-intensity interval training coincide with an increase in skeletal muscle mitochondrial content and function. J Appl Physiol (1985) 115(6):785–793. doi:10.1152/japplphysiol.00445.2013
Jensen L, Bangsbo J, Hellsten Y (2004) Effect of high intensity training on capillarization and presence of angiogenic factors in human skeletal muscle. J Physiol 557(Pt2):571–582. doi:10.1113/jphysiol.2003.057711
Kiviniemi AM, Tulpo MP, Eskelinen JJ, Savolainen AM, Kapanen J, Heinonen ICH, Huikuri HV, Hannukainen JC, Kalliokoski KK (2014) Cardiac autonomic function and high-intensity interval training in middle-age men. Med Sci Sports Exerc 46(10):1960–1967. doi:10.1249/MSS.0000000000000307
Krip B, Gledhill N, Jamnik V, Warburton D (1997) Effects of alterations in blood volume on cardiac function during maximal exercise. Med Sci Sports Exerc 29(11):1469–1476
Laursen PB, Shing CM, Peake JM, Coombes JS, Jenkins DG (2002) Interval training program optimization in highly trained endurance cyclists. Med Sci Sports Exerc 34(11):1801–1807
Laursen PB, Shing CM, Peake JM, Coombes JS, Jenkins DG (2005) Influence of high-intensity interval training on adaptations in well-trained cyclists. J Strength Cond Res 19(3):527–533
McMillan K, Helgerud J, Macdonald R, Hoff J (2005) Physiological adaptations to soccer specific endurance training in professional youth soccer players. Br J Sports Med 39(5):273–277. doi:10.1136/bjsm.2004.012526
Nagashima K, Mack GW, Haskell A, Nishiyasu T, Nadel ER (1999) Mechanism for the posture-specific plasma volume increase after a single intense exercise protocol. J Appl Physiol (1985) 86(3):867–873
Pottgiesser T, Schumacher YO (2013) Current strategies of blood doping detection. Anal Bioanal Chem 405(30):9625–9639. doi:10.1007/s00216-013-7270-x
Richardson RS, Verstraete D, Johnson SC, Luetkemeier MJ, Stray-Gundersen J (1996) Evidence of a secondary hypervolemia in trained man following acute high intensity exercise. Int J Sports Med 17(4):243–247. doi:10.1055/s-2007-972840
Schmidt W, Prommer N (2005) The optimised CO-rebreathing method: a new tool to determine total haemoglobin mass routinely. Eur J Appl Physiol 95(5–6):486–495. doi:10.1007/s00421-005-0050-3
Schmidt W, Prommer N (2008) Effects of various training modalities on blood volume. Scan J Med Sci Sports 18:59–71. doi:10.1111/j.1600-0838.2008.00833.x
Schmidt W, Heinicke K, Rojas J, Manuel Gomez J, Serrato M, Mora M, Wolfarth B, Schmid A, Keul J (2002) Blood volume and hemoglobin mass in endurance athletes from moderate altitude. Med Sci Sports Exerc 34(12):1934–1940
Steiner T, Wehrlin JP (2011) Does hemoglobin mass increase from age 16 to 21 and 28 in elite endurance athletes? Med Sci Sports Exerc 43(9):1735–1743. doi:10.1249/MSS.0b013e3182118760
Wahl P, Jansen F, Achtzehn S, Schmitz T, Bloch W, Mester J, Werner N (2014) Effects of high intensity training and high volume training on endothelial microparticles and angiogenic growth factors. PLoS One 9(4):e96024. doi:10.1371/journal.pone.0096024
Warburton DE, Gledhill N, Jamnik VK, Krip B, Card N (1999) Induced hypervolemia, cardiac function, VO2max, and performance of elite cyclists. Med Sci Sports Exerc 31(6):800–808
Warburton DE, Gledhill N, Quinney HA (2000) Blood volume, aerobic power, and endurance performance: potential ergogenic effect of volume loading. Clin J Sport Med 10(1):59–66
Warburton DE, Haykowsky MJ, Quinney HA, Blackmore D, Teo KK, Taylor DA, McGavock J, Humen DP (2004) Blood volume expansion and cardiorespiratory function: effects of training modality. Med Sci Sports Exerc 36(6):991–1000
Wassermann K, Whipp BJ, Koyal SN, Beaver WL (1973) Anaerobic threshold and respiratory gas-exchange during exercise. J Appl Physiol 35(2):236–243
Zavorsky GS (2000) Evidence and possible mechanisms of altered maximum heart rate with endurance training and tapering. Sports Med 29(1):13–26. doi:10.2165/00007256-200029010-00002
Acknowledgments
This project was supported by the University of Innsbruck, Vice Rector for Research (“Doktoratsstipendium aus der Nachwuchsförderung”).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Communicated by Carsten Lundby.
Rights and permissions
About this article

Cite this article
Menz, V., Strobl, J., Faulhaber, M. et al. Effect of 3-week high-intensity interval training on VO2max, total haemoglobin mass, plasma and blood volume in well-trained athletes. Eur J Appl Physiol 115, 2349–2356 (2015). https://doi.org/10.1007/s00421-015-3211-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-015-3211-z