
Abstract
Ectopic (extradural) meningiomas that do not originate from either the optic fascicle or the intracranial meninges are exceedingly rare. A patient with an ectopic meningioma in the external auditory canal and mastoid was treated in our unit. The world literature of the last 20 years was reviewed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
External auditory canal (EAC) meningioma without any intracranial connection is exceedingly rare. A literature search over the last 20 years, though, reveals many reports of meningioma involving the temporal bone [1, 2, 3, 4, 5, 6, 7], but all of them had intracranial extension except for one [3]. All cases of external ear meningiomas published so far have been described as aural polyps with or without middle ear involvement. We present here a case report of aural meningioma arising from the external auditory canal presenting as a sagging of the posterior canal wall.
Case report
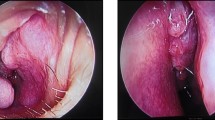
A 45-year-old man presented with progressive deafness and chronic ear discharge on the left side for 6 months. The otoscopic examination revealed a very narrow ear canal with a soft tissue swelling obstructing the ear canal completely. The tympanic membrane was not visible at all. The swelling was smooth, non-tender and covered by the skin of the external auditory canal. It did not present like a true sagging of the posterior meatal wall, but the appearance was very close to it. Pure tone audiometry indicated moderate conductive hearing loss (Fig. 1). The patient’s general examination was normal, and the neurological examination showed no abnormality. A computer tomography (CT) scan revealed opacification of the bony external auditory meatus, middle ear and mastoid, with no erosion of the ossicles or attic (Fig. 2). An exploratory modified radical mastoidectomy (MRM) was done. Extensive granulations were removed from the attic, middle ear and medial wall of the external canal. A frond-like fibrous mass was found extending from the external canal to the middle ear. The eardrum was absent, and it was replaced by a fibrous mass. Bleeding during the operation was not excessive. The incudostapedial joint was dislocated and the head of the malleas chopped off to clear the disease. The tumour was removed in total. The ossicles, dural plate and tegmen plate were intact. Histopathological examination of the specimen derived from the external auditory canal and mastoid cavity infiltrated by tumour tissue was done. This tissue was infiltrated by coalescing cords and sheets of tumour tissue composed of fairly large ovoid cells with rounded to slightly oval nuclei surrounded by eosinophilic cytoplasm (Fig. 3). The cell boundaries were indistinct, giving the tumor a syncytial appearance. Some nuclei were enlarged or somewhat irregular, and there were also cells with intranuclear cytoplasmic extensions (Fig. 4). Immunohistochemistry showed that the tumour cells expressed vimentin and EMA, but were negative for cytokeratins (MNF 116 and CAM 5.2), chromogranin A, synaptophysin, S100 protein, alpha-smooth muscle actin, desmin and CD34, and thus supported the diagnosis. This was suggestive of mesothelioma meningioma (WHO type I). Most of these tumours have intracranial extension, so a MRI scan of the head and orbit was done to rule out any intracranial extension (Fig. 5). This patient had no intracranial component of the tumour.

Audiogram suggestive of left mixed deafness

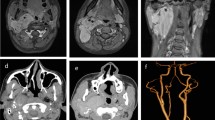
CT of the temporal bone. There is opacification of the EAM and the middle ear. The ossicles are still present, and there is no erosion of the attic or erosion around the semicircular canals. No lesion on the right side

Biopsy segment from external auditory canal covered by epidermis is infiltrated by a meningothelial meningioma. The structure in the middle is a pearl of a skin adenexum ( dark stained portion) (H&E, ×10)

Detail of meningiothelial meningioma showing tumor cells with indistinct cell borders shows intranuclear cytoplasmic extentions. In the right lower corner there is a mitotic figure. (H&E, ×40)

MRI imaging showing no evidence of recurrence of primary tumour and no space-occupying lesion adjacent to the left ear
Discussion
Meningioma of the external ear is an uncommon tumour [1]. All cases, except for one, reported so far had intracranial extension. Uppal et al. presented one report of a temporal bone meningioma external ear without intracranial extension [3]. The present case is the second report on temporal bone meningioma arising from the external auditory canal extending into the middle ear without any intracranial connection. Thompson et al. published a study of 36 cases of temporal bone meningioma (four of them were in the EAC), and they admitted that because of a lack of radiological investigation they were not able to rule out intracranial extension [4] (Table 1).
Primary extracranial meningiomas involving the ear and temporal bone comprise <1% of all meningiomas and 2% of all benign and malignant primary tumours of this region [4]. Embryologically, ectopic meningiomas are postulated to arise from either “punched off” embryonal arachnoid cells outside the skull and vertebra that lie along the line of fusion of the primitive nerve or bone sheaths, or it may arise as a result of differential maturation of pleuripotent mesenchymal cells [4]. The first theory is more widely accepted. Histologically, meningiomas can be classified as globular ovoid (more common) and flat en-plaque (more invasive) [1, 4]. The WHO classifies four types of meningiomas: (1) meningotheliomatous or syncitial, (2) transitional or psammomatous, (3) fibrous and (4) angioblastic. The extracranial group of meningiomas is mainly the first or second variety [1]. Histopathological examination of the specimen derived from the external auditory canal and mastoid cavity infiltrated by tumour tissue in our case was suggestive of mesothelioma meningioma (WHO type I).
Primary meningiomas of the temporal bones are more common in middle-aged females [1, 3]. In spite of its tendency to invade the dura and the bone, meningiomas are considered benign and their symptoms are primarily caused by compression of the neighbouring neural structures. Temporal bone meningioma can either involve the middle ear and external auditory canal or the internal auditory meatus. External or middle ear meningiomas present with hearing loss (conductive or mixed), a polyp in the external ear, tinnitus, facial palsy or facial spasm, temporo-mandibuar joint dysfunction or as a neck mass [5, 6, 7]. The present case is a rare one in which meningioma presented as a sagging of the posterior canal wall.
Treatment of the primary external ear meningiomas is wide surgical excision [1]. The nature of surgery depends on the extent of the tumour, which needs careful preoperative assessment with MRI scans. Radiotherapy, though, has been proposed as a mode of treatment [5, 6]; its role is yet to be proved. As meningioma is a slow-growing tumour, a follow-up of up to 10–15 years with yearly CT or magnetic resonance (MRI) scans along with clinical and audiological examinations has been suggested to rule out any recurrence [1, 9]. The overall prognosis is good, with 83% 5-year survival [9].
Conclusion
Ectopic meningioma arising from the external ear is a very rare, but well-established clinical condition. It can present as an aural polyp or sagging of the wall of the external canal. Otolaryngologists should be well aware of the need for long-term follow-up of this group of patients with regular scanning to rule out any intracranial foci or recurrence of the tumour.
References
D’Angelo AJ Jr, Marlowe A, Marlowe FI, Mobini J (1991) Primary meningiomas of the middle ear: do they exist? Ear Nose Throat J 70:794–798
Brugler G (1992) Tumors presenting as aural polyps: a report of four cases. Pathology 24:315–319
Uppal HS, Kabbani M, Reddy V, Kaur S (2003) Ectopic extra-cranial meningioma presenting as an aural polyp. Eur Arch Otorhinolaryngol 260:322–324
Thompson LD, Bouffard JP, Sandberg GD, Mena H (2003) Primary ear and temporal bone meningiomas: a clinicopathologic study of 36 cases with a review of the literature. Mod Pathol 16:236–245
Netto AA, Redtfeldt RA, Jackson CG, Netterville JL, Hampf CR (2003) Dumbbell-type intracranial meningioma presenting as an aural polyp and a neck mass. Otolaryngol Head Neck Surg 129:457–460
Ferlito A, Devaney KO, Rinaldo A (2004) Primary extracranial meningioma in the vicinity of the temporal bone: a benign lesion which is rarely recognized clinically. Acta Otolaryngol 124:5–7
Tsunoda R, Fukaya T (1997) Extracranial meningioma presenting as a tumour of the external auditory meatus: a case report. J Laryngol Otol 111:148–151
Ishikawa N, Komatsuzaki A, Tokano H (1999) Meningioma of the internal auditory canal with extension into the vestibule. J Laringol Otol 113:1101–1103
Rietz DR, Ford CN, Kurtycz DF, Brandenburg JH, Hafez GR (1983) Significance of apparent intratympanic meningiomas. Laryngoscope 93:1397–1404
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kumar, G., Basu, S., Sen, P. et al. Ectopic meningioma: a case report with a literature review. Eur Arch Otorhinolaryngol 263, 426–429 (2006). https://doi.org/10.1007/s00405-005-1030-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-005-1030-2