
Abstract
Purpose
To report an unusual absent right common carotid artery with embryological and clinical emphasis.
Methods
A 63-year-old female with a multilobulated anterior communicating artery saccular aneurysm was referred to our center for definite treatment. An analysis of her carotid system on CTA and DSA with 3D modeling was performed to assess the embryology of an absent right common carotid and its association with aneurysm development.
Results
Cerebral angiogram demonstrated an absent right common carotid artery and separate origin of the internal and external right carotid arteries arising from the brachiocephalic trunk.
Conclusion
Absence of the common carotid artery is an uncommon anatomical variant, usually asymptomatic and commonly associated with other vascular abnormalities. It is important to be familiar with the association between this anatomical variant given its hemodynamic stress, high risk of stroke, and aneurysm formation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Absence of the common carotid artery is a rare anatomical variant with about 87 cases available in the literature [8]. This anatomical variant is usually asymptomatic and has no side or sex preferences [5]. Reported associations include high aortic arch, double aortic arch, aberrant subclavian artery, right aortic arch, persistent proatlantal artery, and persistent trigeminal artery [5, 6]. Herein, we present a case of a female with an absent right common carotid associated with an anterior communicating aneurysm.
Case report
A 63-year-old female with a multilobulated anterior communicating artery (Acomm) saccular aneurysm was referred to our center for definite treatment. Cerebral angiogram demonstrated an absent right common carotid artery and a separate origin of the internal and external right carotid arteries arising from the brachiocephalic trunk. Moreover, the right internal carotid artery (ICA) was small in caliber along its course through the neck and in the intracranial segments and the A1 segment of the right anterior cerebral artery was hypoplastic (Figs. 1 and 2). The patient underwent stent-assisted coil embolization of the Acomm aneurysm with successful total occlusion. As part of the embolization work up computed tomography angiogram (CTA) was performed, which confirmed complete occlusion of the Acomm aneurysm.

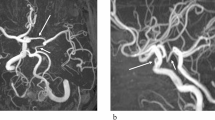
Anteroposterior and lateral digital subtraction angiogram views (a and b) demonstrate the right external (dashed arrows) and internal (arrows) carotid arteries arising from the brachiocephalic trunk. Head computed tomography angiography (CTA) coronal image (c) demonstrates the right A1 hypoplastic segment (arrow) and the Acomm aneurysm. DSA 3D volumetric reconstruction (d and e) shows a multilobulated anterior communicating aneurysm

Head CTA 3D reconstruction (a) reveals absence of the right common carotid artery and separate origin of the internal (arrow) and external (dashed arrow) right carotid arteries arising from the brachiocephalic trunk. Coronal image of CTA (b) shows the small caliber of the right internal carotid artery (short arrow). Axial CTA images (c and d) demonstrate the small caliber of the right internal carotid artery in the cervical segment (circle) and the small caliber of the right carotid canal (curved arrow)
Discussion
During embryogenesis, aortic development starts with a ventral and a dorsal segment and six paired primitive aortic arches which develop between the dorsal and ventral segments [3]. The primitive third aortic arch gives origin to the common carotid artery and the proximal segment of the internal carotid artery and the left fourth arch contributes to the development of the definite aortic arch [3]. The right fourth aortic arch with part of the dorsal aorta forms the brachiocephalic artery and the proximal segment of the right subclavian artery [10]. Moreover, the dorsal aortae which connects the third and fourth arches corresponds to the ductus caroticus which regresses by the sixth week [10] and the common carotid artery (CCA) develops from the root of the ventral aorta between the third and fourth arches [10]. Absent CCA and separate origin of the ECA and ICA results from the persistence of the ductus caroticus and regression of the third branchial arch or due to failure of the left fourth arch development or regression with subsequent cervical aortic arch [5, 6, 9, 10]. Another theory, is the origin of the ECA at a lower level as the third arch vessel, making the CCA shorter and if its origin is sufficiently caudal, the CCA can be absent [1, 9].
Absence of the CCA is associated with different branches patterns of the ECA and ICA. Including ECA arising proximal to the origin of the ICA, on the right side the ECA may arise from the brachiocephalic trunk with the ICA arising from the subclavian artery, or on the left side the ECA and ICA arise independently from the aortic arch between the brachiocephalic trunk and the left subclavian artery [10]. In our case, the right ICA and ECA arose proximally from the brachiocephalic trunk (Fig. 1a and b).
Regarding the right ICA small caliber seen in our case (Fig. 2b and c), the ICA embryogenesis has two origins, the distal part of the dorsal aorta which forms the anatomic segments C1-C6 and the distal part of the third aortic arch which forms the C7 segment. Two theories explain the etiology of the aplasia or hypoplasia of the ICA: the regression of the first and third aortic arch or the failure of the primitive anastomosis to regress causing the underdevelopment of the ICA. The common embryonic origin of the CCA and the ICA from the third aortic arch may explain the association between the absent CCA and the hypoplastic ICA [11]. Furthermore, it is well known that hypoplasia or aplasia of the ICA is associated with a small caliber of the carotid canal, a feature that was also present in our case (Fig. 2d).
In terms of aneurysm association, there is an increased rate of aneurysm development associated to congenital absence or hypoplasia of the carotid system [4]. Some authors propose that intracranial collateral arteries with large caliber are predisposed to abnormal flow vectors and subsequent aneurysm development [4, 12]. Moreover, the incidence of aneurysm formation in patients with ICA hypoplasia or aplasia is 23-45% due to increased blood flow and abnormal flow direction causing hemodynamic stress in the compensatory circulation, usually developing in the basilar artery and/or posterior communicating arteries, although it may occur in other intracranial vessels like our case [8, 11]. In addition, vascular variations such as A1 segment aplasia or hypoplasia have been described in Acomm aneurysms with a reported incidence of about 75%, supporting the hypothesis that the additional blood flow carried by the vessels is a factor of hemodynamic stress and contributes to the pathogenesis of intracranial aneurysms [2, 7]. This abnormal hemodynamics could also be a potential source of cerebral ischemia [8]. Knowledge of these anatomical variants and their association with increased hemodynamic stress should warrant imaging workup to assess aneurysm risk and stroke risk assessment.
In conclusion, absence of the CCA is an uncommon anatomical variant, usually asymptomatic and commonly associated with other vascular abnormalities. It is important to be familiar with this anatomical variant given its hemodynamic stress, high risk of stroke, and aneurysm formation. Imaging workup, counselling and treatment must be warrant for patients with this anatomical variant.
Data availability
No datasets were generated or analysed during the current study.
References
AlAni AM, Al-Ekeer AN, Kolleri JJ, Omer Maki A (2022) Left Common Carotid Artery Agenesis With Independent Origins of the External and Internal Carotid Arteries From the Aortic Arch: A Rare Case in a Patient With Ankylosing Spondylitis. Cureus. https://doi.org/10.7759/cureus.28456
Chen L, Liu JM, Zhou D (2008) Congenital absence of the right common carotid artery, internal carotid artery and external carotid artery associated with anterior communicating artery aneurysm: a rare case. Neurol Sci 29. https://doi.org/10.1007/s10072-008-1030-2
Hanneman K, Newman B, Chan F (2017) Congenital variants and anomalies of the aortic arch. Radiographics 37. https://doi.org/10.1148/rg.2017160033
Kwak Y, Choi MK, Kim KH, Cho JH (2019) Rare case of Absent Common carotid artery likely Associated with Intracranial Aneurysm Development. J Stroke Cerebrovasc Dis 28. https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.01.017
Maybody M, Uszynski M, Morton E, Vitek JJ (2003) Absence of the common carotid artery: a rare vascular anomaly. AJNR Am J Neuroradiol 24
Ojha V, Vadher A, Chandrashekhara SH, Malhi AS, Nayak SK, Kumar S (2020) A unique case of separate origins of left internal and external carotid arteries from high aortic arch with aberrant right subclavian artery – an unreported association in tetralogy of Fallot. J Cardiovasc Comput Tomogr 14. https://doi.org/10.1016/j.jcct.2019.04.004
Orakdogen M, Emon ST, Somay H, Engin T, Is M, Hakan T (2017) Vascular variations associated with intracranial aneurysms. Turk Neurosurg 27. https://doi.org/10.5137/1019-5149.JTN.17839-16.1
Park DY, Lee B, Hwang YJ (2023) Combined anatomical anomalies of Direct Aortic Arch origins of the Left Internal Carotid, Left External Carotid, and left vertebral arteries: a Case Report. J Korean Soc Radiol 84. https://doi.org/10.3348/jksr.2022.0065
Pérez-García C, Pérez-Higueras A, Cabezudo García P (2018) Left common carotid artery agenesis with bovine origin of the left internal carotid artery. Surg Radiol Anat 40. https://doi.org/10.1007/s00276-018-2070-9
Uchino A, Uwabe K, Osawa I (2018) Absent right common carotid artery associated with aberrant right subclavian artery. Neuroradiol J 31. https://doi.org/10.1177/1971400917698980
Whitley H, Zazay A, Skalický P, Malík J, Charvát F, Beneš V, Bradáč O (2023) Congenital internal carotid artery hypoplasia: a systematic review. Neuroradiol J 36
Zink WE, Komotar RJ, Meyers PM (2007) Internal carotid aplasia/hypoplasia and intracranial saccular aneurysms: Series of three new cases and systematic review of the literature. J Neuroimaging 17. https://doi.org/10.1111/j.1552-6569.2007.00092.x
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
JAM: manuscript writing-editing and final approval. SV: manuscript writing-editing. AG: project development, manuscript writing.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to disclose.
Ethical approval
Ethical approval from the institutional review board was not required for this study. The article does not contain photographs or indication that could be traced back to a human participant. The patient gave a written informed consent for all testing during the clinical process, namely, for CT angiography and cerebral angiogram.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Mejía, J.A., Velasco, S. & Guarnizo, A. Absent right common carotid artery with associated anterior communicating aneurysm: embryology and imaging correlation. Surg Radiol Anat 46, 1355–1358 (2024). https://doi.org/10.1007/s00276-024-03402-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-024-03402-0