
Abstract
Agenesis of the internal carotid artery (ICA) is a rare congenital vascular disorder of the cerebral circulation. CT scan of the skull base disclosing complete absence of the bony carotid canal helps to differentiate an agenesis from aplasia or hypoplasia. Although most of the patients remain asymptomatic (thanks to the sufficient collateral circulation provided by the circle of Willis) cerebral infarcts, transient ischemic attacks or intracranial aneurysms have been rarely described in association with agenesis of the ICA. Most often, the vascular territory of the involved ICA is supplied by the contralateral carotid artery and from the vertebrobasilar circulation through the anterior and posterior communicating arteries, respectively. However, collateral supply can also be provided thanks to a transcavernous anastomosis, an aberrant vascular communication between the cavernous portions of the ICAs coursing through the sella turcica. We report here the case of a 55-year-old man with right carotid agenesis and associated transcavernous anastomosis revealed by transient ischemic attack. Embryogenesis, imaging findings, possibilities of collateral circulation and potential complications have also been discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Unilateral anomalies of the internal carotid artery (ICA) related to developmental defects include agenesis, aplasia and hypoplasia. In case of agenesis, both ICAs and bony carotid canal are absent [8]. These rare congenital anomalies occur in less than 0.01% of the population [1, 12], and are most often incidentally discovered on color doppler ultrasonography, magnetic resonance imaging (MRI) or computed tomography of the head and neck vessels. Although most patients remain asymptomatic (thanks to the sufficient collateral circulation provided by the circle of Willis), transient ischemic attacks or cerebral infarcts can occur as well as cerebral haemorrhages due to ruptured aneurysms [6, 7].
Most often, vascular supply of the involved ICA is provided thanks to the circle of Willis (through the anterior and posterior communicating arteries). However, much less commonly, collateral flow is provided by a transcavernous anastomotic vessel between the ICAs and coursing through the sella turcica.
We report here the case of a patient with right ICA agenesis and associated transcavernous anastomosis (TA), revealed by a transient ischemic attack (TIA).
Case report
A 55-year-old man with past medical history of tobacco abuse and hypertension was referred for a sudden episode of left hemibody paresthesias during 1 hour. Clinical examination showed a blood pressure of 90/60 mmHg and an isolated left hemibody hypoesthesia.
Color doppler sonography disclosed a smaller caliber of the right common carotid artery (CCA) in comparison to its opposite, the right ICA could not be observed, and we noted a changing flow pattern of the right CCA from a low peripheral resistance pattern into a high one, as observed in external carotid artery (ECA) in distality, suggesting that the right CCA only led to the right ECA.
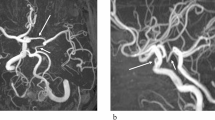
MRI with diffusion-weighted imaging sequence showed no recent infarction. 3D contrast-enhanced MR angiography sequence showed the reduced caliber of the right CCA and the absence of the right ICA (Fig. 1a).

Brain MRI. a 3D contrast-enhanced MR angiography showed a smaller caliber of the right CCA than the left one (arrowheads) as well as the absence of the right ICA. The right CCA only led to the right ECA (arrow). b, c 3D time of flight MR angiography confirmed the absence of flow-related signal within the right ICA. Note the presence of an aberrant transcavernous vessel between the cavernous portions of the ICAs coursing though the sella turcica to supply the right carotid siphon and the right MCA (arrowheads). Note that the circle of Willis is incomplete with bilateral aplasia of the PCOMs and the A1 segment of the right ACA. Both ACA originated from the left ICA
3D time of flight MR angiography confirmed the absence of flow-related signal within the right ICA. Both anterior cerebral arteries (ACAs) originated from the left ICA (the right A1 segment is not seen). An intracavernous collateral vessel arising from the contralateral ICA and coursing through the sella turcica supplied the right carotid siphon and the right middle cerebral artery (MCA). The posterior communicating arteries (PCOM) could not be seen (Figs. 1b, c, 2a). There was no associated venous intercavernous sinus.

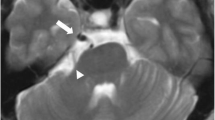
a Sagittal image of a CT angiogram also showed the intrasellar intercarotid communicating artery (arrowhead). b Axial image of a CT angiogram at the level of the petrous ICA demonstrated the absence of both right ICA and bony carotid canal (black arrow) confirming the diagnosis of right ICA agenesis. The left ICA and bony canal are present and normal (white arrow)
CT scan of the skull base disclosed complete absence of the right bony carotid canal confirming the congenital agenesis of the right ICA (Fig. 2b).
The diagnosis of low-flow TIA triggered by right ICA agenesis was suspected. The antihypertensive medication of the patient was adapted allowing a favourable clinical course without symptoms recurrence.
Discussion
We report a symptomatic case of unilateral agenesis of the right ICA with a TA anastomosis, a very rare developmental disorder. Dysgenesis of the ICA, which include agenesis, hypoplasia or aplasia, is usually fortuitously discovered by Doppler ultrasonography or brain imaging performed for other reason. According to Lie, agenesis correspond to a total absence of the organ due to failure of the artery to develop embryologically, whereas aplasia refers to a lack of organ development but with existence of its precursor and hypoplasia correspond to incomplete organ development [8]. Agenesis of ICA was firstly described by Tode in 1787 (on postmortem examination) [14] and although both can be involved, the cases described in the literature predominate slightly in men and on the left side [4].
Intracranial circulation is maintained by collateral circulation allowing patients to stay mostly asymptomatic. According to Lie, six patterns (type A to F) of collateral circulation in association with ICA absence were described. Among them, we count three pathways of collateral circulation associated with unilateral ICA agenesis (classified into Type A, B or D). In type A (the most common), ipsilateral MCA is supplied from the vertebrobasilar circulation through an hypertrophied PCOM and ipsilateral ACA from the anterior circulation through a patent anterior communicating artery (ACOM). In type B, both ipsilateral MCA and ACA are supplied via a patent ACOM. The less common (as in our patient) is the type D in which the ipsilateral carotid siphon received blood flow through a transcavernous vessel arising from the contralateral ICA and coursing through the sella turcica [8].
Embryological segments of the ICA are derived from the dorsal aorta and the third aortic arch at the 3-mm embryonic stage; whereas, the circle of Willis develops later (7-mm to 24-mm embryonic stage). The ICA development occurs before skull base formation. The presence of an ICA is necessary for the formation of the bony carotid canal, explaining that in case of ICA agenesis, the ipsilateral carotid canal is absent [9]. Consequently, blood supply is more likely through the circle of Willis if the disruption occurs after 24-mm embryonic stage, or through a TA if it occurs earlier [2].
In our case, the existence of a TA between the carotid siphons confirmed the congenital absence of the right ICA. Moreover, the lack of the right carotid canal allowed to differentiate agenesis from aplasia.
The embryological explanation of this abnormality is controversial, because it has never been observed in developing embryo [8]. This anastomotic vessel may arise from a union between two primitive trigeminal arteries that have lost their communication with the basilar artery, or from the persistence or hypertrophy of embryologically developing vessels (remnant of the primitive maxillary artery or via the plexiform network of vessels, described by Padget, which originates from the ICAs and communicates with one another around Rathke’s pouch) [3, 8, 9].
These different theories account for the variable courses of the intercavernous communications which can be intrasellar (as in our case), transsphenoidal, paraclinoid–supraclinoid or supraclinoid–supraclinoid. Anastomosis between the paraclinoid or supraclinoid segment of the ICA and the supraclinoid segment of the other ICA so-called paraclinoid–supraclinoid or supraclinoid–supraclinoid anastomosis has been rarely reported. These types of supracavernous anastomoses which did not correspond to a previous type of Lie’s classification are considered to be an unusual variation of type D anastomosis [5, 15]. The coexistence of several types of collateral circulation in a same patient such as a paraclinoid–supraclionoid anastomosis and an anastomosis between the tip of the basilar artery and the PCOM has also been reported [15]. An another congenital anomaly described is the absence of the left CCA with separate origin of the ECA and ICA from the aortic arc (in this case, the left ICA originates from the brachiocephalic trunk (bovine origin) and the left ECA arose from the aortic arc [11]. Patients with Lie’s type D anastomosis have also a higher incidence of anterior communicating aneurysms. Such patients should also be followed up radiologically not only to check for enlargement of the existing aneurysms but also to detect new ones. It appears particularly important to diagnose these anatomical variants prior to neurosurgical approaches such as transsphenoidal or transcranial, to avoid damaging these arteries [6].
Although patients often have no symptoms, cerebral infarctions or TIA [7] has been rarely reported, as well as an increased incidence of intracranial aneurysms in case of ICA agenesis or hypoplasia [6]. Two hypotheses exist to explain this association: both conditions could occur independently during embryonic life as a result of a developmental error operating at both loci or the aneurysm may be secondary to the deranged hemodynamic forces induced by the absence of the contralateral ICA [13]. The existence of multiple associated intracranial artery segmental agenesis or aplasia is not rare [10].
Note that in our patient, in contrary to the initial description by Lie, the A1 segment of the ipsilateral ACA was absent. Consequently, both ACA originated from the contralateral ICA and the ipsilateral MCA territory is only supplied by the TA. The complete anterior circulation, therefore, depends entirely on a single carotid artery, which makes it particularly vulnerable to atherosclerotic disease involving the sole CCA or ACI.
Abbreviations
- ACOM:
-
Anterior communicating artery
- ACA:
-
Anterior cerebral artery
- CCA:
-
Common carotid artery
- ECA:
-
External carotid artery
- ICA:
-
Internal carotid artery
- MCA:
-
Middle cerebral artery
- PCOM:
-
Posterior communicating artery
- TA:
-
Transcavernous anastomosis
- TIA:
-
Transient ischemic attack
References
Afifi AK, Godersky JC, Menezes A, Smoker WR, Bell WE, Jacoby CG (1987) Cerebral hemiatrophy, hypoplasia of internal carotid artery, and intracranial aneurysm: a rare association occurring in an infant. Arch Neurol 44:232–235
Cali RL, Berg R, Rama K (1993) Bilateral internal carotid artery agenesis: a case study and review of the literature. Surgery 113:227–233
Given CA 2nd, Huang-Hellinger F, Baker MD, Chepuri NB, Morris PP (2001) Congenital absence of the internal carotid artery: case reports and review of the collateral circulation. AJNR Am J Neuroradiol 22:1953–1959
Handa J, Matsuda I, Nakasu S, Nakano Y (1980) Agenesis of an internal carotid artery: angiographic, tomographic and computed tomographic correlation. Neuroradiology 19:207–211
Hong JH, Chang HW, Kim JM, Cho HC, Kim SH, Hong JH, Kim SJ, Jeong HW (2016) Internal carotid artery agenesis associated with a rare collateral pathway: supraclinoid-supraclinoid anastomosis. A case report. Surg Radiol Anat 38:261–263
Horie N, Tsutsumi K, Kaminogo M, Morikawa M, Kitagawa N, Nagata I (2008) Agenesis of the internal carotid artery with transcavernous anastomosis presenting with an anterior communicating artery aneurysm–a case report and review of the literature. Clin Neurol Neurosurg 110:622–626
Lee EJ, Chang HW, Ha EY, Kim SH, Kim MJ, Yi HA, Lee SK, Kim SJ (2012) Acute infarction in a patient with agenesis of the internal carotid artery and transcavernous anastomosis. J Clin Neurosci 19:597–599
Lie TA (1968) Congenital Anomalies of the Carotid Arteries. Excerpta Medica, Amsterdam, pp 35–51
Padget DH (1948) The development of the cranial arteries in the human embryo. Contr Embryol 32:205–261
Park YW, Yoo J, Kim DJ (2018) Double inter-internal carotid artery communication through intercavernous anastomosis and posterior communicating artery associated with multiple intracranial artery segmental agenesis/aplasia. Surg Radiol Anat 40:227–231
Pérez-Garcia C, Pérez-Higueras A, Cabezudo Garcia P (2018) Left common carotid artery agenesis with bovine origin of the left internal carotid artery. Surg Radiol Anat 40:1177–1180
Smith KR Jr, Nelson JS, Dooley JM Jr (1968) Bilateral ‘hypoplasia’ of the internal carotid arteries. Neurology 18:1149–1156
Tangchai P, Khaoborisut V (1970) Agenesis of internal carotid artery associated with aneurysm of contralateral middle cerebral artery. Neurology 20:809–812
Tode (1787) Medizinisch chirurgische Bibliothek (Kopenhgen) 10: 408. Cited by Krause W (1876) Die Varietäten der Arterien und Venen. In: Henle J (ed) Handbuch der System Anatomie des Menschen, Vol 3, part 1, 2nd ed. Vieweg, Brunswick
Uchino A, Saito N, Kohyama S (2015) Agenesis of the internal carotid artery with paraclinoid-supraclinoid anastomosis and basilar artery-posterior communicating artery anastomosis diagnosed by magnetic resonance angiography. Surg Radiol Anat 37:685–687
Funding
No targeted funding reported. The study is not industry-sponsored.
Author information
Authors and Affiliations
Contributions
BH: manuscript writing. EG: critical revision of the manuscript. CD: critical revision of the manuscript. JLM: critical revision of the manuscript. GQ: critical revision of the manuscript. RL: critical revision of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Ethical approval
Financial disclosures the authors report no disclosures relevant to the manuscript. Dr Benjamin Hebant, MD: reports no disclosures. Pr Emmanuel Gerardin, MD, PhD: reports no disclosures. Dr Céline Delpierre, MD: reports no disclosures. Dr Jean-Loup Mereaux, MD: reports no disclosures. Dr Gerald Quesney, MD: reports no disclosures. Dr Romain Lefaucheur, MD: reports no disclosures.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hebant, B., Gerardin, E., Delpierre, C. et al. A case of right internal carotid agenesis with associated transcavernous anastomosis revealed by transient ischemic attack. Surg Radiol Anat 42, 207–210 (2020). https://doi.org/10.1007/s00276-019-02318-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-019-02318-4