
Abstract
The several types of agenesis of the internal carotid artery (ICA) are classified based on the aplastic segment of the ICA and types of collateral circulation. On magnetic resonance angiography, we incidentally found an extremely rare case in which the patient had 2 types of collateral circulation—anastomosis between the paraclinoid and supraclinoid segments of the contralateral ICA and anastomosis between the tip of the basilar artery and the posterior communicating artery. This is the first report of a case of ICA agenesis with 2 such types of collateral circulation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In daily clinical practice, most cases of agenesis of the internal carotid artery (ICA) are found incidentally on magnetic resonance (MR) angiography as a result of developed collateral circulations. Some patients have symptoms relating to ICA agenesis, such as hypopituitarism [7, 8], Horner syndrome [3], trigeminal neuralgia [12], and transient ischemic attack [4].
ICA agenesis is classified into several types according to the aplastic segment of the ICA and types of collateral circulation. We report a case of ICA agenesis with 2 rare types of collateral circulation.
Case report
A 40-year-old woman with vertigo underwent MR imaging and MR angiography examinations at a private neurosurgical clinic and was transferred to our institution with a tentative diagnosis of occlusion of the left ICA. Her neurological examination was normal, and she had no history of trauma in the head and neck region.
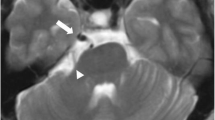
She underwent MR imaging and MR angiography of the head and neck region with a 3-T MR system (Achieva 3.0 T TX Quasar Dual, Philips Medical Systems, Best, The Netherlands). MR angiography without contrast medium was obtained using the standard 3-dimensional time-of-flight technique. MR imaging showed no abnormality in the brain. On MR angiography, the left ICA was absent, but the left and right middle cerebral arteries (MCA) were visualized (Fig. 1a). To identify collateral circulation, we created partial maximum-intensity-projection (MIP) MR angiographic images using the SYNAPSE® VINCENT (Fujifilm Medical Company, Tokyo, Japan) picture archiving and communication system (PACS). We observed these images from multiple special projections and found 2 rare collateral circulations—anastomosis between the paraclinoid right ICA and supraclinoid left ICA and anastomosis between the tip of the basilar artery (BA) and the left posterior communicating artery (PCoA) (Fig. 1b, c). There was no osseous defect at the sella floor. Because her vertigo disappeared, we observed the patient conservatively without medication.

Magnetic resonance (MR) angiography obtained using a 3-T scanner. a Anteroposterior projection of maximum-intensity-projection (MIP) image shows hypoplastic left common carotid artery (dotted arrow). Left internal carotid artery (ICA) is absent. A small connecting artery between the bilateral ICA is seen (long arrow), but this anomalous artery cannot be clearly identified due to superimposition of several arteries. A large artery arises from the tip of the basilar artery (BA) and supplies the left middle cerebral artery (MCA, short arrow). b Inferosuperior projection of partial MIP MR angiography clearly demonstrates an anomalous connecting artery arising from the paraclinoid segment of the right ICA and fusing with the supraclinoid segment of the left ICA (long arrows). The white short arrow indicates the anomalous artery arising from the tip of the BA. The black short arrow indicates the proximal short segment of the left posterior communicating artery (PCoA), which is extremely large and long. Thus, there is a small arterial ring. c Anteroinferior to posterosuperior projection of partial MIP MR angiography shows a hypoplastic A1 segment of the left anterior cerebral artery (ACA, dotted arrow). The long arrow and short arrow indicate the same arteries in b
Discussion
The circle of Willis (CW) is an anastomotic arterial ring that connects the right and left carotid systems (anterior circulation) and the vertebrobasilar system (posterior circulation), thus providing a potential source of collaterals in case of arterial occlusion [11]. Gunnal et al. [2] recently reported that normal and complete CW was found in 60 % among 150 human cadavers. There were 21 different types of CW, and maximum variations were seen in the PCoA followed by the anterior communicating artery.
Lie [5] classified several types of ICA agenesis according to the aplastic segment of the ICA and collateral circulation. In Lie’s type A, which is most prevalent, the cervical segment to the carotid siphon of the ICA is absent, the supraclinoid ICA is present, and the MCA is supplied via the PCoA (Fig. 2a). Lie’s type B is entire ICA agenesis, and the MCA is supplied via the anterior communicating artery. Lie’s type C is agenesis of the bilateral ICAs, and both MCAs are supplied via the bilateral PCoAs. Lie’s type D is the so-called intercavernous anastomosis [9] or trans-sellar anastomosis [7]. The ICA is absent from the cervical segment to the cavernous segment and present from the carotid siphon to the terminal ICA (Fig. 2b). Lie’s type E ICA is hypoplastic. Lie’s type F is segmental agenesis of the cervical and petrous ICA with multiple small collaterals that are called rete mirabile.

Schematic illustration of agenesis of the internal carotid artery (ICA) modified from Reference [4]. a Lie’s type A. The middle cerebral artery (MCA) is supplied by the posterior communicating artery (PCoA), the most prevalent type of collateral circulation in cases of ICA agenesis. b Lie’s type D. There is an anastomotic artery between cavernous segments of the bilateral ICAs; this is called intercavernous anastomosis type. c Schematic illustration of our patient. There are two anastomotic arteries. The long arrow indicates anastomosis between the paraclinoid ICA and supraclinoid ICA. The short arrow indicates anastomosis between the tip of the BA and the PCoA. There is a triangular arterial ring, and a hypoplastic A1 segment of the ACA is also present
In our patient, the ICA was absent from the cervical segment to the carotid siphon and present from the supraclinoid segment to the terminal ICA, and there were two collateral channels (Fig. 2c). The first was an anastomosis between the paraclinoid ICA and supraclinoid ICA. Only three similar cases have been reported [6, 8, 10], but these demonstrated no other collateral circulation. Thus, the MCA seems to arise from the contralateral paraclinoid ICA. We propose naming this collateral a “paraclinoid-supraclinoid anastomosis.” The second collateral is an anastomosis between the tip of the BA and the PCoA. In Lie’s type A, an extremely large PCoA arises from the posterior cerebral artery, which resembles our patient’s case. However, we found that the anastomotic channel formed a small triangular arterial ring, and this type of collateral pathway has not been reported.
Most patients with ICA agenesis manifest no symptom relating to this anomaly, but as mentioned in the “Introduction”, hypopituitarism, Horner syndrome, trigeminal neuralgia, and transient ischemic attack may be seen. Patients with ICA agenesis frequently experience cerebral aneurysm, which is probably due to hemodynamic stress on the collateral circulation [9, 10]. Because ICA agenesis is congenital, aortic and cardiac malformations, especially coarctation of the aorta, are frequently associated with this anomaly [1].
Conclusions
We present a case of ICA agenesis with paraclinoid–supraclinoid anastomosis and BA-PCoA anastomosis, an extremely rare arterial variation that we diagnosed by MR angiography. When interpreting MR angiography, partial MIP images in special projections and source images are important for identifying rare variations of the cerebral arteries.
References
Fitzgerald RT, Zuccoli G (2012) Agenesis of the internal carotid artery: associated malformations including a high rate of aortic and cardiac malformations. Pediatr Radiol 42:1333–1338
Gunnal SA, Farooqui MS, Wabale RN (2014) Anatomical variations of the circulus arteriosus in cadaveric humans. Neurol Res Int 2014:687281
Khan A, Baheerathan A, Hussain N, Gosalakkal J (2012) Agenesis of the internal carotid artery associated with ipsilateral Horner syndrome in a child. Pediatr Neurol 47:68–70
Kiritsi O, Noussios G, Tsitas K, Lappas D (2012) Unilateral agenesis of the internal carotid artery presented as transient ischemic attack: a case report. Surg Radiol Anat 34:475–477
Lie TA (1968) Congenital anomalies of the carotid arteries. Excerpta Medica, Amsterdam, pp 16–51
Meder JF, Blustajn J, Trystram D, Godon-Hardy S, Devaux B, Zuber M, Frédy D (1997) Radiologic anatomy of segmental agenesis of the internal carotid artery. Surg Radiol Anat 19:385–394
Mellado JM, Merino X, Ramos A, Salvadó E, Sauri A (2001) Agenesis of the internal carotid artery with a trans-sellar anastomosis: CT and MRI findings in late-onset congenital hypopituitarism. Neuroradiology 43:237–241
Moon WJ, Porto L, Lanfermann H, Weis R, Zanella FE (2002) Agenesis of internal carotid artery associated with congenital anterior hypopituitarism. Neuroradiology 44:138–142
Quint DJ, Boulos RS, Spera TD (1989) Congenital absence of the cervical and petrous internal carotid artery with intercavernous anastomosis. AJNR Am J Neuroradiol 10:435–439
Suyama K, Mizota S, Minagawa T, Hayashi K, Miyazaki H, Nagata I (2009) A ruptured anterior communicating artery aneurysm associated with internal carotid artery agenesis and a middle cerebral artery anomaly. J Clin Neurosci 16:585–586
Takahashi S, Mugikura S (2010) The circle of Willis. In: Takahashi S (ed) Neurovascular imaging. MRI and microangiography. Springer-Verlag, London, pp 12–15
Uchino A, Sawada A, Hirakawa N, Totoki T, Kudo S (2002) Congenital absence of the internal carotid artery diagnosed during investigation of trigeminal neuralgia. Eur Radiol 12:2339–2342
Acknowledgments
We thank Prof. Masabumi Nagashima, for valuable comments. We also thank Rosalyn Uhrig, M.A., for editorial assistance in the preparation of this manuscript.
Conflict of interest
We declare that we have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Uchino, A., Saito, N. & Kohyama, S. Agenesis of the internal carotid artery with paraclinoid–supraclinoid anastomosis and basilar artery–posterior communicating artery anastomosis diagnosed by magnetic resonance angiography. Surg Radiol Anat 37, 685–687 (2015). https://doi.org/10.1007/s00276-014-1388-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-014-1388-1