
Abstract
Background
Eyebrow position affects human facial expression and aesthetic appearance. However, upper-eyelid surgeries may cause brow position changes and affect the function and aesthetics of the eyebrow. The purpose of this review was to assess the influence of upper-eyelid surgeries on brow position and morphology.
Methods
PubMed, Web of Science, Cochrane Library, and EMBASE were searched for clinical trials and observational studies published between 1992 and 2022. The brow height from the center of the pupil is analyzed to show the brow height change. The change in brow morphology is measured by the change in brow height from the lateral palpebral and the medial palpebral. Studies are further divided into subgroups according to different surgical techniques, author locations, and whether to conduct skin excision.
Results
Seventeen studies met the inclusion criteria. Nine studies and 13 groups were included in the meta-analysis, indicating that brow height decreased significantly after upper-eyelid surgeries (MD = 1.45, 95% CI [0.87, 2.07], P < 0.0001), and simple blepharoplasty, double-eyelid surgery, and ptosis correction can cause the brow position to drop by 0.67, 2.52, and 2.10 mm, respectively. East Asian authors group had a significant decrease in brow height compared with the non-East Asian authors group (28 groups, p = 0.001). Skin excision during blepharoplasty does not affect brow height.
Conclusions
Brow position changes significantly following upper blepharoplasty according to the decrease in brow-pupil distance. The morphology of the brow showed no significant postoperative change. Different techniques and authors locations may result in different levels of postoperative brow descent.
Level of Evidence III
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The eyebrow plays an important role in human facial expression and aesthetic appearance [1]. The ideal brow position should be neither excessively high nor too close to the upper eyelid. McKinney et al. proposed that an aesthetically pleasing brow should be at least 2.5 cm above the center of the pupil and approximately 5 cm below the hairline [2]. However, the brow position can be affected by race, gender, and age [3]. Apart from immutable factors, some Asian plastic surgeries discovered that blepharoplasty can also affect the height and morphology of eyebrows [4,5,6]. Although upper-eyelid surgeries provide a better appearance and function to the peri-eye structure, the change in eyebrow position may modify the upper facial structure.
Different techniques are used in blepharoplasty in patients with different conditions. We divided the techniques into three types according to different procedures. Simple blepharoplasty with skin, fat tissue, and orbicularis (if necessary) excision is only performed in patients with blepharochalasis. Double-eyelid surgery is defined as skin excision (if necessary) with suture fixation, which is performed in patients who wish to have double-folded eyelids. Ptosis correction surgery contains levator or Muller muscle aponeurosis plication/advancement/resection and is performed in patients with moderate or severe upper-eyelid ptosis. Although different procedures are included in the techniques above, upper-eyelid surgeries can increase corneal exposure to achieve a better appearance and functionality of the eyes of patients. The change in postoperative brow position has been discovered by multiple surgeons using different techniques [6,7,8]. However, whether different procedures influence brow position remains undiscussed in previous studies.
The postoperative brow position of patients receiving brow ptosis correction has been discovered to decrease in at least 3-month follow-up [8]. As Hering’s law elucidated that 2 eyes are paired organs, the contralateral eyelid descends after the ptosis eyelid being corrected [9]. This can also be interpreted in the postoperative brow position change. The Hering’s law was explained by the preoperative activity of frontalis, which is relaxed after ipsilateral correction and cause descending of the contralateral brow. This happens in the same way when both side of the eyes are operated in upper blepharoplasty. Some descending brows can correct on its own after several months, while in most patients the brow position remain lowered over a long period of time. As a result, Sweis et al. presented a method to use preoperative neuromodulators on frontalis in order to predict the actual position of brow during upper blepharoplasty [10]. However, the method is still controversial that true ptosis may be caused by the denervation, while others may preserve high frontalis tension which cause misestimate of postoperative results [11]. The descending brow position can also change the facial proportions of patients [5, 6, 12], and the brow morphology change affects facial expressions [13]. Thus, understanding whether the brow position and morphology change is important in surgical planning and result prediction, and understanding the factors that affect postoperative brow position change also helps to make treatment plans of patients.
Materials and Methods
Search Strategy
A systematic review and meta-analysis of brow position change following upper blepharoplasty was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) reporting guidelines. Studies were searched in PubMed, Web of Science, Cochrane Library, and EMBASE for clinical trials and observational studies that evaluated brow position change following upper blepharoplasty and were published before August 30, 2022. The search strategy was as follows: (blepharoplasty OR double-eyelid plasty OR upper-eyelid surgery) AND (brow position OR eyebrow position OR brow change OR brow height) AND (clinical study OR observational study). References from relevant articles were additionally searched to conduct a comprehensive search.
Study Selection
Two authors (R. L and Y. S) independently evaluated the articles extracted from database search by titles and abstracts, and full-text articles were further assessed eligibility by inclusion and exclusion criteria. Studies included in the final review were determined by consensus of the two reviewers.
Selection Criteria
The articles were selected using inclusion and exclusion criteria according to abstracts and full texts. Studies were included if they met the following criteria: (1) the study was a clinical trial or an observational study, (2) the participants underwent upper blepharoplasty, and (3) the brow positions of the participants were measured before and after the surgeries. Studies were excluded when they met the following criteria: (1) the full text of the article was not available, (2) data on brow height were not available, (3) there were not enough participants for statistics in the study group, (4) there were participants with brow lift surgery or other procedures that could affect brow position, and (5) there were participants with prior frontal and occipital injection.
Definitions
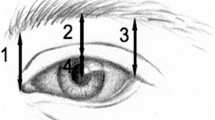
The change in brow height is indicated by the change in central pupil-to-brow height (CPBH) before and after upper blepharoplasty (Fig. 1). The change in brow morphology is indicated by the height of the medial and lateral brow position, which are represented by the change in medial palpebral fissure-to-brow height (MPBH) and the change in lateral palpebral fissure-to-brow height (LPBH), respectively (Fig. 1). The included groups were divided into simple blepharoplasty, double-eyelid surgery, and ptosis correction according to different surgical techniques.

Definitions of central pupil-to-brow height (CPBH), medial palpebral fissure-to-brow height (MPBH) and lateral palpebral fissure-to-brow height (LPBH)
The included groups were also divided into East Asian authors and non-East Asian authors groups according to the location of author’s department. Studies published by Chinese, Korean, and Japanese authors are categorized as East Asian studies, and non-East Asian studies are published by authors from European, Indian, and other regions. The divisions were made because of the different surgical modalities may exist between East Asian surgeons and non-East Asian surgeons [14]. Though differences exist in the eyelid anatomy between East Asians and non-East Asians, we assume that the development of regionally-specific modified surgical techniques was influencing surgeons subtly, leading to different results of blepharoplasties [15].
Data collection and Statistical Analysis
Data from the included studies were collected by one author and independently confirmed by another author. Study type, the number of eyelids, country, surgery technique, measurement method, brow position before surgery, brow position after surgery, brow position change, study design, and relevant outcomes were recorded. The outcome data from the included studies were recorded in Microsoft Excel. The data on brow position before and after upper blepharoplasty were analyzed by Review Manager 5.4.1 software. Random effect model was used. The continuous variables were expressed as the mean differences (MDs) with 95% confidence intervals (CIs). Only a P value <0.05 indicated a significant difference. Subgroup difference analysis required data on central-pupil brow height (CPBH) change and was analyzed by IBM SPSS Statistics 26. An independent-samples Kruskal–Wallis test was run to determine whether there were differences between simple blepharoplasty, double-eyelid surgery, and ptosis correction. A Mann–Whitney U test was run to determine whether there were differences in CPBH change between East Asian authors and non-East Asian authors groups, as well as skin excision and non-skin excision. The brow morphology change is measured as the change in medial and lateral brow height. A paired sample t test was run to determine the brow morphology change. The figures of results were produced by Review Manager 5.4.1 software and GraphPad Prism 7.0 software.
Assessment of Study Quality
Two reviewers independently assessed the study quality according to the New castle-Ottawa Scale for observational studies [16]. Consensus was reached through discussion.
Results
Study Selection
There were 212 publications identified from the initial database search, and 10 publications identified from references in relevant articles. Duplications are recognized through Endnote X9.2, irrelevant articles are excluded by title and abstract, and 86 publications were removed. Full-text articles were assessed for eligibility, and 26 publications met the inclusion criteria. The included studies were further assessed by exclusion criteria, while 1 additional study is recorded through reference search, and 17 studies were included in the final review (Fig. 2) [4, 8, 13, 17,18,19,20,21,22,23,24,25,26,27,28,29].

Flow diagram depicting the searching step of studies included in this Meta-analysis
Study Characteristics
For all studies included in meta-analysis, 9 studies with 13 study groups including 1428 eyelids provided mean value and standard deviation of CPBH preoperatively and postoperatively and were included in the meta-analysis. The characteristics of included studies are shown in Table 1. According to different surgical techniques, 3 studies with 6 study groups included 796 eyelids reported brow change after simple blepharoplasty, 2 studies and 2 study groups were included to report a total of 268 eyelids after double-eyelid surgery, and 5 study groups in 4 studies with 364 eyelids were included in ptosis correction. According to different location of the study authors, 5 study groups in 4 studies reporting 403 eyelids in East Asian authors studies and 8 study groups in 5 studies with 1025 eyelids were analyzed in non-East Asian authors studies. The mean (SD) value of CPBH significantly decreased from 19.16(4.95) mm preoperatively to 17.83(4.08) mm after blepharoplasty (p = 0.004). According to different surgical technologies, there were differences between preoperative and postoperative brow height in simple blepharoplasty and ptosis correction, within mean (SD) values change from 15.82(0.66) mm preoperatively into 15.15(0.73) mm postoperatively (p = 0.013), and 24.20(6.14) mm preoperatively into 22.15(4.89) mm postoperatively (p = 0.052), respectively. The mean (SD) value of CPBH changed from 22.23(1.09) mm into 19.94(1.88) mm in double-eyelid group, and no significant difference was reported (p = 0.199). As for different author location, the mean(SD) CPBH value changed significantly after blepharoplasty from 23.84(5.94) mm into 21.21(5.08) mm in East Asian authors studies (p = 0.007), and from 17.32(2.89) mm into 16.50(2.60) mm in non-East Asian authors studies (p = 0.029).
For all 17 included studies (28 study groups), a total of 2408 eyelids were included in the review. Brow position changes were reported in 7 study groups from 4 studies after simple blepharoplasty, 4 study groups from 4 studies after double-eyelid surgery, and 17 study groups from 12 studies after ptosis correction. Seven studies (11 groups, 1271 eyelids) included patients from non-East Asian authors studies, and 10 studies (17 groups, 1100 eyelids) were analyzed from East Asian authors studies. Among all included studies, 14 groups in 10 studies reported that skin excision was conducted during upper blepharoplasty in 1535 eyelids, and 6 groups in 6 studies reported non-skin excision in 402 eyelids.
Meta-Analysis of Brow Height Change
For all studies included in the meta-analysis, 13 groups provided CPBH means and standard deviations before and after the surgery. A total of 1428 eyelids were analyzed in this study. The heterogeneity test showed moderate heterogeneity among these studies (Chi2 = 56.37, P < 0.0001, I2 = 79%), and a random effect model was adopted for the evaluation. The pooled result showed a significant difference in CPBH between the preoperative value and the postoperative value (MD = 1.45, 95% CI [0.83, 2.07], P < 0.00001; Fig. 3a), indicating that the brow position decreased after receiving upper blepharoplasty, with a mean decrease of 1.45 mm.


Forest plots depicting the meta-analysis results of the CPBH change before and after upper blepharoplasty. a The brow position change of all included studies. b The brow position change of subgroups divided by different surgical techniques. c The brow position change of subgroups divided by the different author locations. The dotted lines represent the effects of each study, and the diamond represents the summary of CPBH change after upper blepharoplasty.
We further conducted subgroup analysis by the different techniques and author locations. Among all 1428 eyelids, 796 underwent simple blepharoplasty, 268 underwent double-eyelid surgery, and 364 underwent ptosis correction. For eyelids receiving simple blepharoplasty, significant difference was shown in CPBH between the preoperative value and the postoperative value (MD=0.67, 95% CI [0.35, 1.00], P < 0.0001; Fig. 3b-1.2.1). For double-eyelid surgery, only Esmaeilkhanian et al. and Zhang et al. reported the mean and standard derivation of CPBH, with a mean difference of 2.52 (95% CI [0.90, 4.14], P < 0.0001; Fig. 3b-1.2.2). For eyelids receiving ptosis correction, a significant difference was shown in CPBH before and after upper blepharoplasty (MD = 2.10, 95% CI [0.64, 3.56], P < 0.0001; Fig. 3b-1.2.3). Overall, simple blepharoplasty, double-eyelid surgery, and ptosis correction can cause the brow position to drop by 0.67, 2.52, and 2.10 mm, respectively.
For the different location of surgeons, 403 eyelids that received upper blepharoplasty were in the East Asian authors studies, and 1025 eyelids that received upper blepharoplasty were in the non-East Asian authors studies. Among the East Asian authors studies, a significant difference in CPBH was shown between the preoperative value and postoperative value (MD = 2.82, 95% CI [1.50, 4.14], P < 0.0001; Fig. 3c-1.3.1). For the non-East Asian authors studies, a significant difference was indicated in CPBH before and after upper blepharoplasty (MD = 0.81, 95% CI [0.39, 1.22], P = 0.004; Fig. 3c-1.3.2). Therefore, both East Asian authors studies and non-East Asian authors studies had a decrease in brow position after receiving upper blepharoplasty, with values of 2.82 and 0.81 mm, respectively.
Aesthetic Impacts of Brow Position Change on Patients
The descending brow position can change the facial proportions of patients. Zhang et.al described an average on mid-face proportion changed from 0.801 preoperatively to 0.698 postoperatively [29].
The symmetry of brow in patients with brow asymmetry can also be changed by upper-eyelid surgeries as is discussed in 4 studies. Pool et al. studied the brow asymmetry change after simple blepharoplasty in 2015, and the brow change produced less asymmetry (left-right CPBH difference≥1 mm) in patient with the change of asymmetry rate from 52.3 to 47.1% [19]. Cho et.al reported a significant decrease in brow asymmetry (preoperative: mean = 2.7 mm, SD = 0.21 mm; postoperative: mean = 2.3 mm, SD = 0.19 mm, p = 0.01) in brow asymmetry patients after ptosis correction surgery [27]. Kokubo et al reported 2 of 47 patients with symmetrical eyebrows exhibited unbalanced brow height after ptosis correction, which is related to the height of preoperative margin reflex distance [8]. Fan et al. also discussed the symmetry of the brow after ptosis correction and indicated better symmetry (23.26% symmetric brow before operation and 90.7% symmetric brow after operation) and fewer frontal lines after the surgery [28]. Therefore, the brow symmetry improved after simple blepharoplasties and ptosis correction surgeries in the reviewed studies.
Change in Brow Morphology
Among the 16 studies included, 10 study groups in 6 studies reported the average change of brow height at medial canthal line or lateral canthal line, and a total of 460 eyelids were included. The characteristics of the included studies are shown in Table 2. The mean(SD) changes of MPBH and LPBH values were −1.85(1.34)mm and −1.65(1.30)mm, respectively. The paired sample t test showed no significant difference between MPBH change and LPBH change (t = −0.554, p = 0.593), indicating that the change in brow position at the medial palpebral line and lateral palpebral line was not significantly different.
Risk Factors of Brow Height Change
Of all 17 studies included, 28 study groups reported the mean CPBH change with or without the standard deviation. The characteristics of studies are shown in Table 1. Four studies (7 groups, 817 eyelids) reported the mean CPBH change after simple blepharoplasty, 4 studies (4 groups, 389 eyelids) reported the mean CPBH change after double-eyelid surgery, and 12 studies (17 groups, 1165 eyelids) reported the mean CPBH change after ptosis correction. Overall, the weighted average of CPBH change in simple blepharoplasty, double-eyelid surgery, and ptosis correction groups were −0.71 (95%CI [−0.73, −0.69]) mm, −1.84 (95%CI [−1.92, −1.75])mm, and −1.71 (95%CI [−1.78, −1.64]) mm, respectively. According to the independent-samples Kruskal–Wallis test (Fig. 4a), there were no significant differences across groups using different surgery techniques (n = 26, p = 0.116).

Difference analysis of the value of CPBH change before and after upper blepharoplasty in subgroups. a CPBH changes in different surgical technique groups. b CPBH changes in different authors location groups. c CPBH changes in skin excision group and non-skin excision group.
We further conducted a Mann–Whitney U test for a pairwise comparison, which indicated no significant difference in CPBH change between simple blepharoplasty and double-eyelid surgery (n = 11, p = 0.257), no significant difference in CPBH change between double-eyelid surgery and ptosis correction (n = 21, p = 0.929), and a significant difference in CPBH change between simple blepharoplasty and ptosis correction (n = 24, p = 0.036) (Fig. 4a). Therefore, the distribution of brow height shows a significant difference between simple blepharoplasty and ptosis correction.
To compare the difference between the East Asian authors studies and non- East Asian authors studies, 17 studies (28 groups) were analyzed. Overall, the weighted mean CPBH changes in the non-East Asian authors studies and East Asian authors studies groups were −0.71 (95% CI [−0.72, −0.70]) mm and -2.17 (95% CI [−2.24, −2.10]) mm, respectively. According to the independent-samples Mann–Whitney U test, the distribution of CPBH showed a significant difference between East Asian authors studies and non-East Asian authors studies (n = 28, p = 0.001) (Fig. 5b). In addition, brow height changes after upper blepharoplasty were different in East Asian authors and non-East Asian authors studies.

Funnel plots depicting the publication bias of studies included in meta-analysis.
Risk of Bias
A funnel plot was depicted to evaluate the publication bias if studies included in the meta-analysis. The funnel plot did not show obvious publication bias for studies included in meta-analysis (Fig. 5). Bias of cohort studies was evaluated through Newcastle-Ottawa Scale as depicted in Table 3. A total of 11 of 17 studies did not show comparability of the cohorts, and 2 of 17 studies did not have enough follow-up.
Discussion
This systematic review and meta-analysis evaluated changes in brow position and morphology after upper blepharoplasty. According to the 25 included studies, brow position drops following upper blepharoplasty, whereas brow morphology showed no significant change. Additionally, the technique used for upper blepharoplasty and the location of author affected the degree of the brow position change.
Several measurements were used to evaluate the brow position among all 25 included studies. The most used measurement was CPBH and vertical lines from the brow to the lateral palpebral fissure, the center of the pupil, and the medial palpebral fissure. Among all studies included, 8 studies used CPBH value only [5, 9, 17,18,19,20,21, 23]. This method is the most convenient and costless measurement, which is also convenient for statistics. Thirteen studies used 3 vertical lines to achieve a more accurate change in brow morphology [4, 8, 13, 22, 24,25,26, 28, 30,31,32,33,34]. In addition, Prado, Silva-Junior, et al. measured the change in brow morphology using angles constituted by a lateral or medial portion of the brow and lateral or medial palpebral fissure [35]. This method eliminates the influence of the central frontalis and achieves a better description of the relationship between the brow and the eye. However, the method may be prone to measurement error. To exhibit the influence of brow position on facial aesthetics, 2 studies used mid-face proportion or upper-face proportion to reflect the change in brow position [6, 33]. This measurement is clearer in reflecting the effect of brow position change on aesthetics, but the method lacks standardization, and the standard may differ among different populations. Therefore, CPBH may be a convenient and relatively accurate measurement of brow position. As the lower edge of the brow may be indistinct, the upper brow border height was measured in recent studies [3]. For the measurement of brow morphology, 5 distances defined as the horizontal distance between the brow and medial palpebral fissure, medial cornea, central pupil, lateral cornea, and lateral palpebral fissure can depict the change in brow morphology [3]. Our study also showed that the morphology of brow did not show significant difference after blepharoplasty. Therefore, we proposed that the vertical distance from central of pupil to middle of the brow could be a convenient and relatively accurate measurement of brow height.
An ideal brow position is important in the result of upper-eyelid surgeries. Some European plastic surgeons have raised various guidelines for an objectively ideal eyebrow position indicating the distance between the upper-eyelid crease and the lower edge of the brow as 15-16 mm and CPBH as 25 mm [2, 36, 37]. To be subjective, an ideal brow position should lie above the level of the supraorbital rim in females and at the level of the superior orbital rim in males [38]. However, brow position, morphology, and symmetry are affected by several factors, such as age, sex, gravity, and muscle action, while some researchers have discovered that upper blepharoplasty may cause a decrease in brow level [4, 6, 21, 24, 26, 38]. According to our result, Zhang et al. showed that the brow change after double-eyelid surgeries could result in a better ratio of the middle-face structures [29]. Moreover, some previous studies also evaluated the result after double-eyelid surgeries. It is believed that the mid-face proportion follows the golden ratio of 0.618 [12]. Xu et al. evaluated the ratio between the eyebrow–lower eyelid and the lower eyelid–nasal base, which represents the mid-face ratio. Xu et al. studied the change in the mid-face proportion after double-eyelid surgery, resulting in a ratio of 0.71 preoperatively and 0.67 postoperatively [6]. Ji et al. also observed a decrease in the mid-face ratio from 0.746 to 0.657 after ptosis correction [12]. Therefore, we proposed that brow descent with a certain extent after operation may improve appearance, and middle-face ratio should be an important indicator in predicting the postoperative aesthetic results of blepharoplasty.
Brow position change can be caused by the removal of excessive skin during upper blepharoplasty. Fagien et al. first discovered brow position change after upper blepharoplasty in 1992, in which he raised that excessive skin removal caused brow ptosis after the surgical procedure [17]. More researchers have raised that excessive tissue including skin and fat tissue movement result in decrease in brow levels [35]. We believe it is true that the removal of upper-eyelid skin can pull the brow position downward immediately after the surgical procedure. Prado et al. measured the change in brow-eye angles to find that patients receiving excessive tissue removal during simple blepharoplasty had a significantly lower brow position after the surgery [35]. Moreover, Kokubo et al. conducted a series of studies since 2017 to determine whether extra skin excision increases the distance of brow drops following ptosis correction [8, 25, 26]. Although the study conducted in 2019 showed no significant difference between the skin excision group and the non-skin excision group after the external Müller’s muscle tucking (EMMT) procedure, it was believed that the ptosis severity affected the eyebrow position result [25]. In our analysis, we failed to compare the effect of skin excision on brow position change. Although the skin excision procedure was mentioned in some articles, in practice, whether to conduct skin excision and how much skin should be excised was decided by the actual condition. We believe that excision of excessive skin in patients with severe ptosis causes more decrease on brow height. However, whether different extent of skin excision can lead to different extent of brow descending is still unknown. And we believe understanding the safe extend of skin excision is important in both ptosis population and non-ptosis population. Therefore, more studies on relationship between skin excision and brow position should be conducted in future studies.
The brow position after blepharoplasty may correlated to the change of tension of frontalis before and after blepharoplasty. The frontalis is responsible for elevating eyebrows and increasing the field of view. Previous studies have suggested that patients have a tense frontalis before upper blepharoplasty to enlarge the field of view, and surgery can increase corneal exposure, and patients no longer need to enlarge the view field [6]. Kokubo et al. found the distance of CPBH change was correlated to the margin reflex distance of patients before blepharoplasty, which indicated that postoperative brow height may be affected by preoperative tension of frontalis [8]. Consequently, the frontalis is relaxed after surgery, resulting in a decrease in brow height [39, 40]. Kim et al. tried to test this hypothesis by using an electromyogram (EMG) to evaluate the activity of the frontalis before and after upper-eyelid surgery [33]. The study revealed that frontalis activity decreased 6 months following surgery, but no significant position or morphology changes were observed [33]. However, Fan et.al observed an upward trend following postoperative descent of brow position; however, it will not return to the original height before surgery [8]. Therefore, a hyperactive frontalis may exist in pre-blepharoplasty patients, and surgery may relieve the tension of the frontalis. According to our results, patients receiving simple blepharoplasty had a significant decrease in brow-pupil distance. We assumed that double-eyelid surgeries and ptosis correction can increase corneal exposure to achieve wider visual fields, whereas simple blepharoplasty only removes blepharochalasis. Patients with larger corneal exposure no longer need to enlarge visual fields by contracting the frontal muscle, resulting in a decrease in brow-pupil distance. The law of brow position change after blepharoplasty is summarized in Table 4. However, a longer period of time to evaluate the brow position change should be followed.
Recently, neuromodulators were used in predicting the brow position after surgeries and relax the hyperactive frontalis before or after surgeries. Before ptosis correction, some patients accept phenylephrine tests to predict the brow position change after surgery [21, 22]. Rootman et al. proposed that brow height change with the phenylephrine test is correlated with brow height change after surgery and explained that phenylephrine may compensate for frontalis tension by elevating the eyelid margin [21]. However, the method is used only in ptosis correction. Ben et al. proposed that in long-term ptosis patients, frontalis was still utilized despite the surgical improvement of vision, and botulinum A toxin are used to relax the hyperactive frontalis and help patients to relearn the set point of contracting their frontalis [41]. To better optimize the surgical outcomes of upper blepharoplasty, Sweis et al. proposed neuromodulator treatment before surgery [10]. By preoperative injection, frontalis hyperactivity is released during surgery, which helps surgeons predict the true anatomic brow position during the surgery [10]. Therefore, understanding the rule of brow position change after blepharoplasty is important in instructing the therapeutic protocols of patients, which includes the timing and population of botulinum A toxin injection in patients.
Further analyses are needed to evaluate the effect of skin excision during different techniques of blepharoplasty. Evaluation of subjective symptom before surgeries and satisfaction after surgeries are also needed to help researchers achieve better understanding on the difficulty of eye opening.
There are some limitations to our study. Brow position changes with aging, and older populations (≥61 years) may have a brow 3.5 mm higher than younger populations (18-40 years) [42]. However, our analysis failed to compare the extent of brow height change among different populations due to the lack of specific information on age. Brow morphology was also different between males and females, but no included studies established subgroups to explore the influence of sex. Meanwhile, the population of males receiving upper blepharoplasty is far smaller than that of females. For the statistics, our data showed significant heterogeneity, and the random effect model was used in the analysis. This finding may be because some influential factors are not separated into subgroups. However, studies with accessible data remain limited, and further analysis should be conducted with more comprehensive data.
Conclusion
Brow position changes significantly following upper blepharoplasty according to the decrease in brow-pupil distance. The morphology of the brow shows no significant difference before and after upper blepharoplasty surgery. Different techniques result in different levels of postoperative brow descent. The brow position change in ptosis correction is significantly greater than in simple blepharoplasty. The East Asian authors studies exhibit a greater chance of a brow position change than the non-East Asian authors studies after upper blepharoplasty. We assume that the change in brow position after upper blepharoplasty is related to frontalis hyperactivity. Surgeons should consider the conditions of brow changes before surgery. More methods to predict brow position change will hopefully be discovered.
References
Yalçınkaya E, Cingi C, Söken H, Ulusoy S, Muluk NB (2016) Aesthetic analysis of the ideal eyebrow shape and position. Eur Arch Otorhinolaryngol 273(2):305–310
McKinney P, Mossie RD, Zukowski ML (1991) Criteria for the forehead lift. Aesthetic Plast Surg 15(2):141–147
Kraus D, Formoly E, Iblher N, Stark GB, Penna V (2019) A morphometric study of age- and sex-dependent changes in eyebrow height and shape(✰). J Plast Reconstr Aesthet Surg 72(6):1012–1019
Lee JM, Lee TE, Lee H, Park M, Baek S (2012) Change in brow position after upper blepharoplasty or levator advancement. J Craniofac Surg 23(2):434–436
Kim SS (2013) Effects in the upper face of far east Asians after Oriental blepharoplasty: a scientific perspective on why Oriental blepharoplasty is essential. Aesthetic Plast Surg 37(5):863–868
Xu L, Lee EI, Ma T, Zhang J, Han X, Ahn TJ (2020) Aesthetic analysis of alteration of eyebrow position after double eyelidplasty. Aesthetic Plast Surg 44(2):373–378
Frankel AS, Kamer FM (1997) The effect of blepharoplasty on eyebrow position. Arch Otolaryngol Head Neck Surg 123(4):393–396
Kokubo K, Katori N, Hayashi K, Sugawara J, Fujii A, Maegawa J (2017) Evaluation of the eyebrow position after levator resection. J Plast Reconstr Aesthet Surg 70(1):85–90
Clark TJE, Klejch WJ, Wang K et al (2018) Hering’s law in congenital ptosis: evaluation of the contralateral response to unilateral congenital ptosis repair. Ophthalmic Plast Reconstr Surg 34(3):284–290
Sweis IE, Hwang L, Cohen M (2018) Preoperative use of neuromodulators to optimize surgical outcomes in upper blepharoplasty and brow lift. Aesthet Surg J 38(9):941–948
Massry GG (2018) Commentary on: Preoperative use of neuromodulators to optimize surgical outcomes in upper blepharoplasty and brow lift. Aesthet Surg J 38(9):949–950
Ji C, Li R, He W, Zhang J (2018) The aesthetic analyzing of midface ratio after folding aponeurosis of levator palpebrae superioris muscle in the ptosis correction. J Craniofac Surg 29(2):482–485
Esmaeilkhanian H, Kashkouli MB, Abdolalizadeh P, Aghamirsalim M, Shayanfar N, Karimi N (2021) Revisiting anchor epicanthoplasty in mild to moderate asian epicanthal folds: a clinicopathological study. Aesthetic Plast Surg 45(1):181–190
Chee E, Choo CT (2011) Asian blepharoplasty—an overview. Orbit 30(1):58–61
Saonanon P (2014) Update on Asian eyelid anatomy and clinical relevance. Curr Opin Ophthalmol 25(5):436–442
Wells GA, Shea B, O’Connell D et al (2000) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Oxford.
Fagien S (1992) Eyebrow analysis after blepharoplasty in patients with brow ptosis. Ophthalmic Plast Reconstr Surg 8(3):210–214
Moore GH, Rootman DB, Karlin J, Goldberg RA (2015) Mueller’s muscle conjunctival resection with skin-only blepharoplasty: effects on eyelid and eyebrow position. Ophthalmic Plast Reconstr Surg 31(4):290–292
Pool SM, van der Lei B (2015) Asymmetry in upper blepharoplasty: a retrospective evaluation study of 365 bilateral upper blepharoplasties conducted between January 2004 and December 2013. J Plast Reconstr Aesthet Surg 68(4):464–468
Nakra T, Modjtahedi S, Vrcek I, Mancini R, Saulny S, Goldberg RA (2016) The effect of upper eyelid blepharoplasty on eyelid and brow position. Orbit 35(6):324–327
Rootman DB, Karlin J, Moore G, Goldberg R (2016) The effect of ptosis surgery on brow position and the utility of preoperative phenylephrine testing. Ophthalmic Plast Reconstr Surg 32(3):195–198
Rubinstein TJ, Woolley AJ, Costin BR, Perry JD (2016) Preoperative phenylephrine testing as a predictor of postoperative eyebrow position. Int J Ophthalmol 9(3):472–474
Zheng X, Kakizaki H, Goto T, Shiraishi A (2016) Digital analysis of eyelid features and eyebrow position following CO(2) laser-assisted blepharoptosis surgery. Plast Reconstr Surg Glob Open 4(10):e1063
Park KS, Park DD (2017) Objective outcome measurement after upper blepharoplasty: an analysis of different operative techniques. Aesthetic Plast Surg 41(1):64–72
Kokubo K, Katori N, Hayashi K et al (2019) Evaluation of the eyebrow position after external Müller’s muscle tucking: a new technique for ptosis repair. J Plast Reconstr Aesthet Surg 72(4):662–668
Kokubo K, Katori N, Hayashi K et al (2019) Evaluation of the eyebrow position after aponeurosis advancement. J Plast Surg Hand Surg 53(1):60–64
Cho H, Kim NY, Ahn HB (2021) The effect of eyebrow asymmetry by ptosis correction operation on senile upper lid ptosis patients. J Korean Ophthalmol Soc 62(1):6–11
Fan X, Hao D-Y, Cao J et al (2022) Aesthetic changes of brow-eyelid continuum after correction of moderate-severe blepharoptosis with conjoint fascial sheath suspension. Aesthetic Plast Surg
Zhang Y, Xiao Z (2022) Upper eyelid blepharoplasty improved the overall periorbital aesthetics ratio by enhancing harmony between the eyes and eyebrows. Clin Cosmet Investig Dermatol 15:1969–1978
Dar SA, Rubinstein TJ, Perry JD (2015) Eyebrow position following upper blepharoplasty. Orbit 34(6):327–330
Hassanpour SE, Khajouei KH (2016) Brow Ptosis after upper blepharoplasty: findings in 70 patients. World J Plast Surg 5(1):58–61
Huijing MA, van der Palen J, van der Lei B (2014) The effect of upper eyelid blepharoplasty on eyebrow position. J Plast Reconstr Aesthet Surg 67(9):1242–1247
Kim D, Son D, Kim M, Harijan A, Yang S, Lee S (2015) Does upper blepharoplasty affect frontalis tonicity? J Plast Reconstr Aesthet Surg 68(5):638–644
Starck WJ, Griffin JE, Jr., Epker BN (1996) Objective evaluation of the eyelids and eyebrows after blepharoplasty. J Oral Maxillofac Surg 54(3): 297–302; discussion -3.
Prado RB, Silva-Junior DE, Padovani CR, Schellini SA (2012) Assessment of eyebrow position before and after upper eyelid blepharoplasty. Orbit 31(4):222–226
Connell BF, Lambros VS, Neurohr GH (1989) The forehead lift: techniques to avoid complications and produce optimal results. Aesthetic Plast Surg 13(4):217–237
Matarasso A, Terino EO (1994) Forehead-brow rhytidoplasty: reassessing the goals. Plast Reconstr Surg 93(7):1378-1389; discussion 90-1.
Patel BC, Malhotra R (2002) Mid Forehead brow lift. StatPearls. Treasure Island (FL): StatPearls Publishing. Copyright © 2022, StatPearls Publishing LLC.
Flowers RS, Caputy GG, Flowers SS (1993) The biomechanics of brow and frontalis function and its effect on blepharoplasty. Clin Plast Surg 20(2):255–268
Karacalar A, Korkmaz A, Kale A, Kopuz C (2005) Compensatory brow asymmetry: anatomic study and clinical experience. Aesthetic Plast Surg 29(2):119–123
Ben Simon GJ, Blaydon SM, Schwarcz RM, Nakra T, Goldberg RA, McCann JD (2005) Paradoxical use of frontalis muscle and the possible role of botulinum a toxin in permanent motor relearning. Ophthalmology 112(5):918–922
Yoon NS, Ahn HB (2019) Exploring brow position changes with age in Koreans. Korean J Opthalmol KJO 33(1):91–94
Funding
The authors have no support or funding to report.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest to disclose.
Statement of Human and Animal Rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
For this type of study, informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Liu, R., Sun, Y., Huang, J. et al. Brow Position Change and its Potential Risk Factors Following Upper Blepharoplasty: A Systematic Review and Meta-Analysis. Aesth Plast Surg 47, 1394–1409 (2023). https://doi.org/10.1007/s00266-023-03288-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-023-03288-0