
Abstract
Purpose
The aim was to investigate the contribution of robotics assisted total hip arthroplasty (THA) through direct anterior approach (DAA) in improving radiographic precision, functional results and complications.
Methods
This retrospective study compared 100 primary conventional THA (cTHA) to 50 primary robotic THA (rTHA) through DAA. All cups were placed with the objective of having no anterior overhang while respecting the safe zones (SZ). Radiographic analysis included cup inclination and anteversion, vertical and horizontal changes of the rotation centre (ΔVCOR, ΔHCOR), acetabular and femoral offset. SZ were 30–50° of inclination and 10–30° of anteversion. Outliers were defined as medial displacement of the COR > 5 mm, vertical displacement of the COR > 3 mm superiorly. Harris hip score (HHS) and complications were compared at one year of follow-up.
Results
The robotic cups were better oriented with 98% in the global SZ versus 68% in the cTHA group (p = 0.0002). The COR was on average better restored in the robotic group in both the horizontal and vertical planes (Δ HCOR = − 5.0 ± 5.0 vs − 3.4 ± 4.9, p = 0.03; Δ VCOR = 1.6 ± 3.3 vs 0.2 ± 2.7, p = 0.04). There were fewer outliers in the rTHA group concerning VCOR (28% versus 10%, p = 0.03). There was no significant difference in HHS and complication rate at one year.
Conclusion
The use of robotics for THA by DAA provided an advantage in controlling the orientation of the cup and the restoration of its rotation centre. Thanks to the 3D planning on CT scan, it allowed to respect the thresholds while avoiding the anterior overhangs.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Among the possible approaches to perform total hip arthroplasty (THA), the direct anterior approach (DAA) has the advantage of being a muscle preserving anatomic approach with rapid early recovery and low risk of dislocation [1,2,3,4]. The DAA is typically performed supine which facilitates the use of intra-operative fluoroscopy, allowing for more accurate assessment of acetabular component positioning, and anatomically restore leg length [1,2,3,4].
The reported disadvantages of this procedure are the steep learning curves for surgeons, the risks of injury to the lateral femoral cutaneous nerve, and the risk of femoral fracture due to the difficulties with adequate femoral exposure [4,5,6]. Surgeons transitioning from other approaches can also potentially increase the risk of malpositioning of the acetabular cup, due to familiarity with the orientation of the acetabulum of their patients placed in the lateral position on the operating table [7]. And yet, many factors depend on this acetabular position (orientation and restoration of the centre of rotation (COR)), such as stability, stem-cup and ilio-psoas impingement, function and survival [8,9,10,11,12].
Foissey et al. have already studied the importance of instrumentation in DAA and found that instrumentation without offset was sufficient to achieve good cup positioning [7]. However, there was a learning curve to overcome, and many outliers of cup placement and position were due to an excess of anteversion. In order to make the procedure reproducible and to control as many of the parameters of the cup positioning as possible, enabling technologies and robotic assisted surgery have become a widespread method of improving component accuracy [13,14,15,16,17]. However, to our knowledge, there is very few series to date that focuses solely on the contribution of robotics in DAA without traction table [18].
The aim of this study was to investigate the contribution of image-based robotics assisted THA through DAA in improving radiographic precision primarily, but also the potential differences in functional results and complications.
Methods
Patients
This retrospective case control study compared two cohorts of patients operated upon by two experimented surgeons (SL, PK) in two different centres. 100 consecutive primary THA operated conventionally (cTHA) through DAA from January 2015 to May 2019 were compared to 50 primary THA operated robotically (rTHA) through DAA between January and December 2019. The DAA is performed routinely in those departments unless in patients with BMI ≥ 40 kg/m2, with abnormal hip anatomy requiring complex THA (e.g. congenital hip dysplasia), in elderly patients (over 85 years old) with osteoporosis or when there was previous hip surgery (e.g. femoral or pelvic osteotomy). All patients with a follow-up lower than one year were considered as lost to follow-up.
Pre-operative templating
Both conventional and CT-based templating were made by the surgeon to define the level of the femoral cut, the size and the position of the implants to recreate the native anatomy (offset, length, COR), and if necessary, to correct a leg length discrepancy or a change in the COR. Both groups were templated on standard pelvic anteroposterior radiographs using Traumacad® software (Traumacad®, Petach-Tikva, Israel). The rTHA group was templated as well on a pre-operative pelvic and proximal femur CT scan using the V3 MAKOplasty total hip application software (Mako Surgical Corporation, Kalamazoo, Michigan). In addition to allowing the surgeon to plan in 3D the abovementioned data, this system makes it possible to control the position of the cup in the transverse plane, to adjust its anteversion and to check the absence of any anterior overhang (Fig. 1). The objectives of the cup position were 40° ± 10 of inclination and 20° ± 10 of anteversion, restoration of the COR ± 5 mm in the horizontal plane (HCOR) and ± 3 mm in the vertical plane (VCOR). In case of modification of the anatomical landmarks due to osteoarthritis, the references of the healthy contralateral hip were used. When using 3D planning, particular attention was paid to the anterior overhang; if this was present with a restoration of the COR and anteversion of 20°, the anteversion was increased and the COR was medialized (Fig. 2).

Contribution of 3D template: planning of the neck resection site, femoral size and version, leg length and global offset (A), cup size and positioning, COR restitution, anterior overhang (B)

Anterior overhang observed during 3D planning with COR restoration and 20° anteversion (A). Application of a 24° anteversion and a 3 mm medialization of the COR to eliminate this overhang (B)
Operative technique
All THAs were performed through DAA in supine position without any traction table as already describe by Foissey et al. [7]. In both groups, stability and leg length were assessed manually.
Cups in cTHA patients were put with standard straight instrumentation and controlled by per-operative fluoroscopic assessment. Implant position was guided by both pre-operative templating and intra-operative anatomical landmarks (anterior and posterior walls, transverse acetabular ligament). The size of the reamers was progressively increased to remove first the cartilage until the desired size is achieved with satisfactory circumferential contact and exposure of bleeding subchondral bone. In case of anterior overhang, the cup was medialised and anteriorised. All shells were cementless cups (Quattro (Lepine®, Genay, France)), and all stems were cementless as well (Targos (Lepine®, Genay, France)).
The rTHA patients were operated using the RIO robotic arm (Mako Surgical Corporation) using the “express” procedure. This express procedure helps to ream the acetabulum, to impact the final cup, and to help to restore the ideal leg length and global offset (Fig. 3) but does not guide femoral neck resection and does not give stem anteversion and COR. One array was placed on the contralateral iliac crest. One checkpoint was placed on the proximal femur, one on the acetabular side and one distal landmark was placed at the level of the ipsilateral patella as part of the express procedure. Femur was prepared manually after a registration of the femoral checkpoint and of the distal landmark. Then, the position of the pelvis was confirmed by registering and verifying the position of patient-specific anatomical landmarks. The robotic arm with haptic control was used to guide the reaming and the impaction of the cup according to the template. After the reduction of the hip with the broach or with the final stem in place, global offset restitution and leg length restitution were assessed. All implants used in the rTHA group were cementless cups (Trident, Stryker®) and an uncemented Anato stem (Stryker®).

Per-operative contribution of robotic “express” procedure: reaming assistance (A), cup impaction assistance (B) and control of the leg length and of the global offset (C)
Radiological assessment
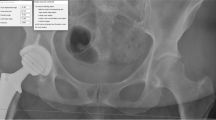
All measurements were recorded on the operated side by two independent surgeons on the standing antero-posterior X-rays at two months after surgery using the picture archive and communication (PACS) software. Magnification was corrected using the implanted acetabular component size as the reference value. Radiographic analysis included inclination and anteversion of the cup, VCOR, HCOR, acetabular offset (AO), femoral offset (FO) and leg length (LLA). Combined offset (CO) was defined as addition of AO and FO [19]. The anteversion was determined by the method described by Widmer [20]. Cup abduction was the angle between the cup axis and parallel between the inter-teardrop line. All the other assessments were performed according to the method described by Kayani et al. [21] (Fig. 4). Cup orientation was classified whether inside or outside the safe zone (SZ) concerning the inclination (30–50°), the anteversion (10–30°) or both position (combined SZ) [7]. Outliers were defined as medial displacement of the COR (ΔHCOR) > 5 mm, vertical displacement of the COR > 3 mm superiorly (ΔVCOR), as these parameters have been associated with greater wear and instability [22]. A difference of LLA > 10 mm compared to the contralateral side was considered as an outlier [19].

Radiographic assessments: HCOR, horizontal centre of rotation; VCOR, vertical centre of rotation; LLA, radiographic leg-length assessment; ML, midline; ITL, inter-teardrop line; VTL, vertical trans-teardrop line; AO, acetabular offset; FO, femoral offset; FA, femoral anatomical axis
Clinical assessment
During the pre-operative consultation, the demographic data, pre-operative Harris hip score (HHS) were obtained. Operative time, peri and early post-operative complications and length of hospitalisation were documented during the stay. Routine follow-ups were planned at two months, one year and every two to five years. This study focused on the results that were collected at one year (HHS, complications).
Statistical analysis
Mean value, standard deviation and minimum and maximum values are presented for continuous variables that were normally distributed. Their distribution was evaluated using a Shapiro–Wilk test. The following statistical tests were used for continuous variables: Student’s t test when the variable of interest was independent and normally distributed; paired Student’s t test when the variable of interest was paired, independent and normally distributed; the Mann–Whitney U test for independent variables that were not normally distributed; and the Wilcoxon signed rank test for paired variables that were not normally distributed. Qualitative variables were summarized as percentages. A chi-square test or Fisher’s exact test was used to ascertain any difference among these. The significance threshold was set at 5%. The statistical analysis was performed using XLSTAT™ software (version 2021, AddInsoft, Paris, France).
Ethical approval
All procedures were performed in accordance with the ethical standards of the institutional and/or national research committee, the 1964 Helsinki Declaration and its later amendments, or comparable ethical standards. The Advisory Committee on Research Information Processing in the Field of Health (CCTIRS) approved this study in Paris on February 17, 2016, under number 16–140. As per institutional standards, formal patient consent was not required for this type of study.
Results
All patients in both groups reached the one year follow-up time, and there were no lost to follow-up. Pre-operative demographic and clinical data are summarized in Table 1. The two groups were comparable, 66% (66/100) were women in the cTHA group versus 46% (23/50) in the rTHA group but this difference was not statistically significant (p = 0.22).
Radiographical results
There was no significant difference in the mean orientation of the cups in the coronal and sagittal planes. The mean anteversion of the cups was greater than 23° in both groups (Table 2). The overall orientation of the cups is shown in Fig. 5. The robotic cups were better oriented with 98% (49/50) of the cups being in the global SZ in the rTHA group versus 68% (68/100) in the cTHA group (p = 0.0002) (Fig. 6). The main reason for poor positioning was excess of anteversion (21% (21/100) in the cTHA group versus 2% (1/50) in the rTHA group, p = 0.005) (Fig. 6).

Diagram depicting the number of cups inside the safe zone in the conventional group (A) and in the robotic group (B). Sixty-eight percent (68/100) of the conventional cups are in the global safe zone versus 98% (49/50) of the robotic cups (p < 0.0001)

Rates of outliers for the cup positioning for both groups
The COR was on average better restored in the robotic group in both the horizontal and vertical planes, although the cups were on average medialized by more than 3 mm in both groups (Table 2). There were fewer outliers in the rTHA group concerning VCOR (10% (5/50) versus 28% (28/100), p = 0.03) (Fig. 7).

Rates of outliers for the restoration of the centre of the rotation and the leg length for both groups. HCOR horizontal centre of rotation; VCOR, vertical centre of rotation; LLA, radiographic leg-length assessment
There was no significant difference in terms of restitution of the length of the lower limbs nor in terms of the restitution of the different offsets (Table 3, Fig. 7).
Clinical results
The robotic procedure was significantly longer by 19 min (p < 0.0001). No complication relative to the robot was reported. The length of hospital stay was similar as well as the HHS at 1 year (Table 3). There was no significant difference in terms of complications between the two groups. No iliopsoas impingement or dislocation was reported (Table 3).
Discussion
Our results favour the use of image based robotic system when performing a THA by DAA. The control of the cup placement by the robotic arm allowed to obtain a placement in the SZ in 98% of the cases as well as a better control of the COR restitution.
To our knowledge, there is only one study that focused solely on the use of the robot via DAA and found excellent results with 100% of the cups in the Lewinnek SZ [18]. These results echo those found in the main series using the same robotic assistance, as they found an accuracy in terms of orientation greater than 97% [21, 23, 24]. This is an advantage that would be all the more interesting at the beginning of the DAA experience because it has been shown that changes in spatial references during the transition to the DAA in supine position could lead to an increased risk of malposition [7], whereas robotics does not present a learning curve in terms of positioning the cup [25].
Robotic restoration of the COR has been less studied than orientation. Kayani et al. also found a better restoration of the COR in the robotic group [21]. This is an important advantage because until now, traditional navigation systems have not proven their effectiveness [14, 26], wherein this restoration theoretically allows a better longevity and a better function [27,28,29]. Although this restoration of the COR has been improved, it remains medialized by 3 mm on average in the robotic group. Also the average anteversion of 23° seems important because it is the upper limit in several safe zone descriptions [30, 31]. This can be explained by the deliberate choice of few towards anterior overhangs even if it means medializing and anteverting the cup (Fig. 2). This may also explain the high outlier rates in the conventional group except that in the absence of robotic control the cup placement tended to be exaggerated with greater anteversion and medialization outside the thresholds. Also, the higher rate of women may be a secondary explanation for this high rate of outliers. Indeed, women tend to have a more marked hypoplasia of the anterior wall [32], making anteversion and greater medialization mandatory in order to avoid an outlier. This strategy seems to be successful because there was no iliopsoas-impingement diagnosed at 1 year. Finally, it should be noted that the pre-operative COR measurements were performed on hips with degenerative changes, which may artificially increase the outlier rate, especially when the surgeon wanted to restore the native COR [33].
Even if this better positioning did not result in a better clinical outcome, it is reasonable to believe that it will have a long-term benefit in terms of wear [22]. There remains an absence of high-quality level I evidence to answer this question whether or not the robot allows an improvement of functional scores after THA but a recent meta-analysis showed a significant improvement of HHS after the use of the robot assisted surgery [24].
There are several limitations to this study. First, it is a retrospective, non-randomized, unmatched study. Even if the difference in the proportion of women was not significant, this may have hindered the comparison of the groups. Secondly, the cup used in each group was not the same, which may have changed the way the implant was positioned. Finally, the measurements of the cup positioning were on radiographs and not CT scans. But a CT scan with irradiations is not recommended post-operatively.
Conclusion
The use of image-based robotic system when performing a THA by DAA provided an advantage in controlling the orientation of the cup and the restoration of its centre of rotation. Thanks to the 3D planning on pre-operative scanner, it allowed to respect the thresholds while avoiding the anterior overhangs.
Data availability
Not applicable.
Code availability
Not applicable.
References
Batailler C, Fary C, Batailler P et al (2017) Total hip arthroplasty using direct anterior approach and dual mobility cup: safe and efficient strategy against post-operative dislocation. Int Orthop 41:499–506. https://doi.org/10.1007/s00264-016-3333-x
Free MD, Owen DH, Agius PA et al (2018) Direct anterior approach total hip arthroplasty: an adjunct to an enhanced recovery pathway: outcomes and learning curve effects in surgeons transitioning from other surgical approaches. J Arthroplasty 33:3490–3495. https://doi.org/10.1016/j.arth.2018.06.033
Homma Y, Baba T, Kobayashi H et al (2016) Safety in early experience with a direct anterior approach using fluoroscopic guidance with manual leg control for primary total hip arthroplasty: a consecutive one hundred and twenty case series. Int Orthop 40:2487–2494. https://doi.org/10.1007/s00264-016-3159-6
Foissey C, Fauvernier M, Fary C et al (2020) Total hip arthroplasty performed by direct anterior approach - Does experience influence the learning curve? SICOT-J 6:15. https://doi.org/10.1051/sicotj/2020015
Homma Y, Baba T, Sano K et al (2016) Lateral femoral cutaneous nerve injury with the direct anterior approach for total hip arthroplasty. Int Orthop 40:1587–1593. https://doi.org/10.1007/s00264-015-2942-0
Foissey C, Kenney R, Luceri F et al (2021) Greater trochanter fractures in the direct anterior approach: evolution during learning curve, risk factors and consequences. Arch Orthop Trauma Surg 141:675–681. https://doi.org/10.1007/s00402-020-03710-1
Foissey C, Fary C, Luceri F et al (2020) Transitioning the Total Hip Arthroplasty (THA) technique from posterior approach in lateral position to direct anterior approach in supine position - Risk Factors for acetabular malpositioning and the learning curve. Int Orthop. https://doi.org/10.1007/s00264-020-04583-0
Sharma AK, Cizmic Z, Dennis DA et al (2021) Low dislocation rates with the use of patient specific “Safe zones” in total hip arthroplasty. J Orthop 27:41–48. https://doi.org/10.1016/j.jor.2021.08.009
Marchetti E, Krantz N, Berton C et al (2011) Component impingement in total hip arthroplasty: Frequency and risk factors. A continuous retrieval analysis series of 416 cup. Orthop Traumatol Surg Res 97:127–133. https://doi.org/10.1016/j.otsr.2010.12.004
Batailler C, Bonin N, Wettstein M, null, et al (2017) Outcomes of cup revision for ilio-psoas impingement after total hip arthroplasty: Retrospective study of 46 patients. Orthop Traumatol Surg Res OTSR 103:1147–1153. https://doi.org/10.1016/j.otsr.2017.07.021
Cheung A, Yan CH, Fu H et al (2019) Ten- to sixteen-year follow-up of highly cross-linked polyethylene in total hip arthroplasty: what factors affect wear? J Arthroplasty 34:2016–2021. https://doi.org/10.1016/j.arth.2019.04.041
Myers CA, Laz PJ, Shelburne KB et al (2018) The impact of hip implant alignment on muscle and joint loading during dynamic activities. Clin Biomech 53:93–100. https://doi.org/10.1016/j.clinbiomech.2018.02.010
Ando W, Takao M, Hamada H et al (2021) Comparison of the accuracy of the cup position and orientation in total hip arthroplasty for osteoarthritis secondary to developmental dysplasia of the hip between the Mako robotic arm-assisted system and computed tomography-based navigation. Int Orthop 45:1719–1725. https://doi.org/10.1007/s00264-021-05015-3
Domb BG, Redmond JM, Louis SS et al (2015) Accuracy of component positioning in 1980 total hip arthroplasties: a comparative analysis by surgical technique and mode of guidance. J Arthroplasty 30:2208–2218. https://doi.org/10.1016/j.arth.2015.06.059
Han P-F, Chen C-L, Zhang Z-L et al (2019) Robotics-assisted versus conventional manual approaches for total hip arthroplasty: A systematic review and meta-analysis of comparative studies. Int J Med Robot Comput Assist Surg MRCAS 15:e1990. https://doi.org/10.1002/rcs.1990
Fontalis A, Kayani B, Thompson JW et al (2022) Robotic total hip arthroplasty: past, present and future. Orthop Trauma 36:6–13. https://doi.org/10.1016/j.mporth.2021.11.002
Kouyoumdjian P, Mansour J, Assi C et al (2020) Current concepts in robotic total hip arthroplasty. SICOT-J. 6:45. https://doi.org/10.1051/sicotj/2020041
Xu S, Bernardo LIC, Andy KS, Pang HN (2020) Robotic-Arm Assisted Direct Anterior Total Hip Arthroplasty Improving Implant Accuracy. Surg Technol Int 38:347–352. https://doi.org/10.52198/21.sti.38.os1368
Flecher X, Ollivier M, Argenson JN (2016) Lower limb length and offset in total hip arthroplasty. Orthop Traumatol Surg Res OTSR 102:S9-20. https://doi.org/10.1016/j.otsr.2015.11.001
Widmer K-H (2004) A simplified method to determine acetabular cup anteversion from plain radiographs. J Arthroplasty 19:387–390. https://doi.org/10.1016/j.arth.2003.10.016
Kayani B, Konan S, Thakrar RR et al (2019) Assuring the long-term total joint arthroplasty. Bone Jt J 101-B:11–18. https://doi.org/10.1302/0301-620X.101B1.BJJ-2018-0377.R1
McGoldrick NP, Antoniades S, El Meniawy S et al (2022) Supine versus lateral position for total hip replacement: accuracy of biomechanical reconstruction. Arch Orthop Trauma Surg 142:2945–2955. https://doi.org/10.1007/s00402-021-04179-2
Domb BG, El Bitar YF, Sadik AY et al (2014) Comparison of robotic-assisted and conventional acetabular cup placement in THA: a matched-pair controlled study. Clin Orthop 472:329–336. https://doi.org/10.1007/s11999-013-3253-7
Ng N, Gaston P, Simpson PM et al (2021) Robotic arm-assisted versus manual total hip arthroplasty : a systematic review and meta-analysis. Bone Jt J 103-B(6):1009–1020. https://doi.org/10.1302/0301-620X.103B6.BJJ-2020-1856.R1
Kayani B, Konan S, Huq SS, et al (2019) The learning curve of robotic-arm assisted acetabular cup positioning during total hip arthroplasty. Hip Int J Clin Exp Res Hip Pathol Ther 1120700019889334https://doi.org/10.1177/1120700019889334
Pagkalos J, Chaudary MI, Davis ET (2014) Navigating the reaming of the acetabular cavity in total hip arthroplasty: does it improve implantation accuracy? J Arthroplasty 29:1749–1752. https://doi.org/10.1016/j.arth.2014.03.038
Yoder SA, Brand RA, Pedersen DR, O’Gorman TW (1988) Total hip acetabular component position affects component loosening rates. Clin Orthop. 228:79–87
Dastane M, Dorr LD, Tarwala R, Wan Z (2011) Hip offset in total hip arthroplasty: quantitative measurement with navigation. Clin Orthop 469:429–436. https://doi.org/10.1007/s11999-010-1554-7
McGrory BJ, Morrey BF, Cahalan TD et al (1995) Effect of femoral offset on range of motion and abductor muscle strength after total hip arthroplasty. J Bone Joint Surg Br 77:865–869
Lewinnek G, Lewis J, Tarr R et al (1978) Dislocations after total hip-replacement arthroplasties. J Bone Jt Surg 60:217–220
Callanan MC, Jarrett B, Bragdon CR et al (2011) The John Charnley Award: risk factors for cup malpositioning: quality improvement through a joint registry at a tertiary hospital. Clin Orthop 469:319–329. https://doi.org/10.1007/s11999-010-1487-1
Atkinson HD, Johal KS, Willis-Owen C et al (2010) Differences in hip morphology between the sexes in patients undergoing hip resurfacing. J Orthop Surg 5:76. https://doi.org/10.1186/1749-799X-5-76
Bonnin MP, Archbold PHA, Basiglini L et al (2012) Do we medialise the hip centre of rotation in total hip arthroplasty? Influence of acetabular offset and surgical technique. HIP Int 22:371–378. https://doi.org/10.5301/HIP.2012.9350
Author information
Authors and Affiliations
Contributions
Constant Foissey: study design, data collection, statistical analysis, literature review and manuscript writing. Cécile Batailler: study design, manuscript editing. Remy Coulomb: study design, manuscript editing. Dia Eldean Giebaly: manuscript editing. Benoit Coulin: data collection. Sébastien Lustig: study design, supervision, literature review and manuscript editing. Pascal Kouyoumdjian: study design, supervision, literature review and manuscript editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The Advisory Committee on Research Information Processing in the Field of Health (CCTIRS) approved this study on June 4, 2015 under number 15–430. For this type of study formal consent is not required.
Conflict of interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. CF, CB, RC and DEG declare that they have no conflict of interest. ES: Consultant for Corin. SL: Consultant for Stryker, Smith Nephew, Heraeus, Depuy Synthes; Institutional research support from Groupe Lepine, Amplitude; Editorial Board for Journal of Bone and Joint Surgery (Am), PK: Consultant for Stryker and for Lepine.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Foissey, C., Batailler, C., Coulomb, R. et al. Image-based robotic-assisted total hip arthroplasty through direct anterior approach allows a better orientation of the acetabular cup and a better restitution of the centre of rotation than a conventional procedure. International Orthopaedics (SICOT) 47, 691–699 (2023). https://doi.org/10.1007/s00264-022-05624-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-022-05624-6