
Abstract
Purpose
Acetabular component position is important for stability and wear. Fluoroscopy can improve the accuracy of acetabular component placement in the posterior approach and the direct anterior approach (DAA). The purpose of this study was to determine if the direct anterior approach in the supine position facilitates the accurate use of fluoroscopy and improves acetabular component position.
Methods
This retrospective, comparative study of 60 THAs with fluoroscopic guidance (30 in posterior approach group and 30 in DAA group) was performed by one surgeon from 2012 to 2014 at a single institution. Demographic and perioperative data were compared using the Kolmogorov-Smirnov test to determine if they were statistically different. The difference between the measured intra-operative and postoperative values for both inclination and anteversion were analysed respectively.
Results
In the posterior approach group we found an average inclination on intra-operative fluoroscopy (IFluoro) of 36.8° ± 3.72°, an average anteversion on intra-operative fluoroscopy (AFluoro) of 25.6° ± 3.64°, an average inclination on postoperative standing AP pelvis X-ray (IAP X-ray) of 39.29° ± 4.58° and an average anteversion on postoperative standing AP pelvis X-ray (AAP X-ray) of 21.31° ± 4.04°. In the DAA group we found an average DAA IFluoro of 42.32° ± 1.91°, an average DAA AFluoro of 22.3° ± 1.41°, an average DAA IAP X-ray of 42.98° ± 1.81° and an average DAA AAP X-ray of 22.88° ± 1.38°. A difference was seen in variability using Kolmogorov-Smirnov test for inclination and anteversion with significant higher variation of measurements in the posterior approach group (p = 0.022 and p < 0.001 respectively). No statistically significant difference was seen in the DAA group using the fluoroscopy for inclination and anteversion.
Conclusion
Using fluoroscopy in the direct anterior approach, we achieved better intra-operative assessment of cup orientation resulting in decreased variability of acetabular cup anteversion than when used in the posterior approach. At least some of the improvement was due to the fact that the fluoroscopic image in the supine position was more accurate as measured against the postoperative standing AP pelvis. This study may influence the choice of approach in total hip replacement.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
A review of the literature on total hip arthroplasty would suggest that accurate placement of the acetabular component is both important and difficult to achieve. Methods are available to help ensure accurate component positioning including fluoroscopy [1, 2], computer navigation [3, 4], and robotics [5, 6]. This study focuses on the use of fluoroscopy to help assure correct acetabular component orientation.
Multiple authors have assessed acetabular cup position in hip arthroplasty. Lewinnek et al. suggested a radiographic definition for ideal acetabular component position as 15° (±10°) of anteversion and 40° ± 10° of abduction [7]. Cups placed outside this zone had a higher dislocation rate [8]. Furthermore, cups placed outside this zone also experience higher biomechanical stresses leading to increased rates of polyethylene wear and osteolysis [9, 10]. Hard-on-hard bearings are possibly more sensitive to acetabular malposition than hard-on-soft bearings [11]. With metal-on-metal implants, increased abduction and anteversion angles have repeatedly correlated with higher serum metal ion levels, a marker for wear [12–14]. These studies support that both stability and wear are affected by cup position.
Several studies conducted by experienced surgeons at prominent institutions have looked at the accuracy of acetabular component position when using traditional methods utilizing mechanical guides and anatomic landmarks such as the anterior superior iliac spine and pubic symphysis [7] and transverse acetabular ligament [15, 16]. In this setting, component position is dependent on the surgeon’s interpretation of the position of the patient’s pelvis on the operating table. Internal and external landmarks, which may be obscured [17, 18] by body habitus or the use of smaller incisions/minimally invasive techniques are also utilized [19].
A recent study by Barrack et al. [20] of 1,549 total hips found that only 88 % of acetabular components were within broad target range (abduction 30–55° and anteversion 5–35°). When Callanan et al. [21] reviewed 1,823 hips, only 38 % met a more stringent component position target range (abduction 30–45° and anteversion 5–25°). These studies, and others [22, 23], would suggest that techniques that improve acetabular component position could have value.
A study by Rathod et al. [24] has shown that fluoroscopy with anterior hip arthroplasty reduced the variability of acetabular cup positioning compared with a non-guided posterior approach. Another study by Beemer et al. [2] suggested that the use of fluoroscopy with posterior hip arthroplasty may increase accurate placement of acetabular components for surgeons performing a mix of primary, revision, and complicated total joint arthroplasties. From previous studies, it is unclear if the value of fluoroscopy is similar when used in the posterior approach as compared to the anterior approach. It is the purpose of this study to determine if the direct anterior approach in the supine position facilitates the accurate use of fluoroscopy and improves acetabular component position.
Materials and methods
A prospectively maintained database of THAs performed by the senior surgeon (N. Stewart) at one centre from May 2012 to November 2014 was reviewed for this retrospective comparative study. A consecutive series of patients who underwent primary THAs, unilateral or staged bilateral, with a cementless hemispheric acetabular design and cementless tapered wedge femoral component (Stryker orthopaedics company) were included in the study.
The EMR was used to obtain information from each patient including laterality of the operatively treated hip; performing surgeon; age, sex, height, weight, and BMI of the patient; femoral head size utilized; acetabular cup outer diameter; surgical approach; and pre-operative diagnosis. Patients were required to have a standing postoperative digital anteroposterior pelvic radiograph of acceptable quality, according to criteria previously described by Callanan et al. [21]. Hips without adequate radiographs were excluded. This series consisted of 60 patients undergoing THA. The senior surgeon converted from a posterior approach to performing nearly all his primary hips from a direct anterior approach as of December 26, 2013. After this date, only patients with a severe Dorr type A femoral geometry were replaced with a posterior approach. We reviewed a consecutive number of patients with a direct anterior approach, of the first 34, 30 had adequately preserved intra-operative fluoroscopy films and a quality postoperative AP pelvis X-ray and were included. Working back in time, we again needed to review 34 patients operated upon via the posterior approach to find 30 with adequately persevered intraoperative fluoroscopic films and quality postoperative study films.
At posterior approach surgery, the patients were placed in a lateral decubitus position with firm supports on a peg board for the anterior pelvis, chest, sacrum and dorsal spine to keep the patient in a stable position throughout the surgery. Once the acetabulum component was placed, fluoroscopy was used to confirm placement. To ensure proper orientation of the fluoroscopic beam tangential to the pelvis, the C-arm was first adjusted to align the centre line of the sacrum with the pubic symphysis. Next, the C-arm was adjusted to make the shape of the obturator on the fluoroscopic image match the shape of the obturator on the pre-operative standing AP pelvis X-ray. Then the position of the acetabulum was assessed with a fluoroscopic view that placed the cup near the centre of the screen while still allowing visualisation of the pubic symphysis to provide vertical reference of the pelvic position (Fig. 1).

Fluoroscopic image allows assessing the position of the acetabular cup in a posterior approach after final cup placement
The anterior approach was performed using the Arch table extension (Orbiswiss company) on a slider table (Steris Corporation) surgical bed (Fig. 2). After anaesthesia, the patient was placed in a supine position. In the supine position, the midline of the sacrum was checked to see if it was aligned with the pubic symphysis. Then the projection of the obturator foramen was evaluated subjectively by the surgeon and the C arm manipulated to have the fluoroscopic image match the pre-operative standing AP radiograph view of the pelvis (Fig. 3a and b). At the time of acetabular insertion, a fluoroscopy view with the cup near the centre, and the pubic symphysis in the view, was used to confirm cup placement (Fig. 4). With either approach, the target inclination was 40° (±10°) and anteversion was 15° (±10°).

The Arch Table Extension is a special table attachment that allows controlled movement of the extremity during preparation of the femur and acetabulum

a Fluoroscopic image obtained with the patient in the supine position on the operating room table with the C-arm beam positioned such that the intraoperative image matches the preoperative image. b The shape of the obturator foramen and the pubic symphysis are noted by the surgeon

Fluoroscopic image allows assessing the position of the acetabular cup in the direct anterior approach (DAA) during and after final cup placement
Geometric analysis was performed on both intra-operative fluoroscopic images of final cup position and six-week postoperative anteroposterior pelvic radiographs. Geometric assessment of the radiographs was performed by an orthopaedic surgeon (WF. Ji) not involved in the surgeries. Measurements included cup abduction angle and cup anteversion angle. Pre and postoperative AP radiographs were taken with patients in the standing position with hips in neutral position, the radiation beam centred on the pubic symphysis, and film-focus distance approximately 120 cm.
A picture archiving and communications system (PACS) software (Fujifilm, Stanford, CT, USA) was used to make the measurements. With regard to validity and convenience for calculation, we chose the method described by Lewinnek and Widmer for measurement of anteversion of the acetabular component [25]. It has been shown to be a valid and reliable method for radiographic analysis of cup anteversion [26]. Acetabular inclination on the postoperative film was measured as the angle between the interteardrop line and the long axis of the acetabular cup face. On the intra-operative fluoroscopic view, the pubic symphysis was used to determine the vertical orientation of the pelvis (Fig. 4).
The difference between the measured intra-operative and postoperative value for both inclination and anteversion were calculated. Variances (square of the SDs) were used to define the variability of the outcome measure. They were compared using the Kolmogorov-Smirnov test to determine if they were statistically different. An independent t-test (two tailed) was used for normally distributed continuous data and the Mann–Whitney U test was used for nonparametric data. Chi-square and Fisher’s exact tests were used for comparing categorical data. A p value of 0.05 was set as the level of statistical significance. The 95 % limits of agreement method was used to assess the agreement between intra-operative fluoroscopy and postoperative standing AP pelvis. First, the mean and SD of the differences between the two methods were calculated. Second, the 95 % limits of agreement were calculated as mean difference ±1.96 SD. Plots of differences against means were used to examine the assumptions of the limits of agreement. Statistical analysis was performed using SPSS software (version 16; Chicago, IL, USA).
Results
Demographic and perioperative data are presented in Table 1. There was no significant difference in patient age, sex, operative side, diagnosis, cup size, or femoral head size between the two groups.
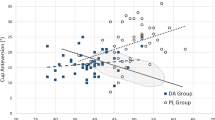
Mean acetabular inclination and anteversion values within the two groups are summarised in Table 2. A difference was seen in variability using Kolmogorov-Smirnov test for inclination and anteversion with significantly higher variation of measurements in the posterior approach group for both variables (p = 0.022 and p < 0.001 respectively).
For the evaluation of both precision and bias of intra-operative fluoroscopy, the difference between the cup inclination measured by fluoroscopy (IFluoro) and cup inclination measured by postoperative standing AP pelvis X-ray (IAP X-ray) was calculated. We did the same calculation between intraoperative anteversion (AFluoro) and postoperative anteversion (AAP X-ray). The mean difference and 95 % confidence intervals for each of these measures are shown in Fig. 5a–d.

Deviation of the intraoperative fluoroscopic values from postoperative standing AP pelvis values compared to their mean. a Direct anterior approach (DAA) inclination. b DAA anteversion. c Posterior approach inclination. d Posterior approach anteversion. Dotted lines represent the 95% limits of agreement (Bland-Altman graph)
The results in Fig. 5a and b demonstrate that 95 % of the time the fluoroscopic view in the supine position is between no more than 3.5° less or 2° more than the value found on a post operative standing AP X-ray. Similar values for anteversion are an underestimate of 3.8° to an overestimate of 2.2°.
The results in Fig. 5c and d demonstrate that 95 % of the time in the posterior position the fluoroscopic measure of inclination is between 11.6° less and 6.0° more than the inclination on the standing AP X-ray. Similar values for anteversion are an underestimate of 4.0° and an overestimate of 11.0°.
Discussion
Acetabular component position is important for endoprosthesis survival [27, 28], wear [22], hip load [29], and range of motion (ROM) [30]. Multiple techniques have been promoted to enhance the accuracy of component positioning, including the use of fluoroscopy [1, 2, 24], computer navigation [31, 32], and robotic assistance [5, 6]. Of these three, fluoroscopy is the most widely available and least expensive to adopt. This paper compares the accuracy of fluoroscopy to the postoperative standing AP radiograph in both the lateral and supine positions.
Rathod et al. [24] demonstrated that an anterior approach with fluoroscopy allowed more accurate acetabular positioning than a posterior approach without fluoroscopy. It’s unclear if the improvement in that sense was due to the use of fluoroscopy or the change in approach. Beemer et al. [2] demonstrated that the use of fluoroscopy can improve component position in the posterior approach. Our results demonstrate that when using fluoroscopy in the anterior approach, we achieved better results than when used in the posterior approach (Fig. 6). At least some of the improvement was due to the fact that the fluoroscopic image in the supine position was more accurate as measured against the postoperative standing AP pelvis. Relying on the fluoroscopic guided direct anterior approach in the supine position, the DAA surgeons were able to improve their accuracy and consistency to position the acetabular component in the safe zone for inclination and anteversion.

A six-week postoperative anteroposterior standing pelvic radiograph showing bilateral total hip arthroplasties (THAs). The right hip was placed by the same surgeon in the direct anterior approach (DAA) using fluoroscopy assistance, whereas the left was placed in the posterior approach using fluoroscopy assistance. (Inclination: left 51.65, right 45.26; Anteversion: left 30.35, right 21.37)
While our study shows that fluoroscopy is more accurate and consistent in the supine position, it’s unclear if the degree of improvement is clinically significant. While detailed long-term studies need to determine to what extent we must optimize component position, it’s hard to argue against a technique which improves accuracy if it is relatively safe and inexpensive. Compared to computer navigation and robotics, fluoroscopy is routinely available, and thus not expensive. The radiation dose, while not measured in this study, is generally quite small.
This study may influence the choice of approach in total hip replacement. If a surgeon wishes to adopt a technology that assists with component positioning, and chooses fluoroscopy, using the direct anterior approach would make that technology more effective. There are other considerations in choosing an approach [21, 33–39], but these findings may factor into that discussion.
Continued research into accurate component positioning is needed. Comparing fluoroscopic guidance to navigation, or to robotics, would help determine which technologies provide greater benefit. Even in skilled and experienced hands, accurate component positioning is not always achieved, and so technologies that help with this task will likely continue to gain acceptance.
References
Matta JM, Shahrdar C, Ferguson T (2005) Single-incision anterior approach for total hip arthroplasty on an orthopaedic table. Clin Orthop Relat Res 441:115–124
Beamer BS, Morgan JH, Barr C, Weaver MJ, Vrahas MS (2014) Does fluoroscopy improve acetabular component placement in total hip arthroplasty? Clin Orthop Relat Res 472:3953–3962. doi:10.1007/s11999-014-3944-8
Ryan JA, Jamali AA, Bargar WL (2010) Accuracy of computer navigation for acetabular component placement in THA. Clin Orthop Relat Res 468:169–177. doi:10.1007/s11999-009-1003-7
Nogler M, Mayr E, Krismer M, Thaler M (2008) Reduced variability in cup positioning: the direct anterior surgical approach using navigation. Acta Orthop 79:789–793. doi:10.1080/17453670810016867
Nawabi DH, Conditt MA, Ranawat AS, Dunbar NJ, Jones J, Banks S, Padgett DE (2013) Haptically guided robotic technology in total hip arthroplasty: a cadaveric investigation. Proc Inst Mech Eng H 227:302–309
Domb BG, El Bitar YF, Sadik AY, Stake CE, Botser IB (2014) Comparison of robotic-assisted and conventional acetabular cup placement in THA: a matched-pair controlled study. Clin Orthop Relat Res 472:329–336. doi:10.1007/s11999-013-3253-7
Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR (1978) Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am 60:217–220
Jolles BM, Zangger P, Leyvraz PF (2002) Factors predisposing to dislocation after primary total hip arthroplasty: a multivariate analysis. J Arthroplasty 17:282–288
Patil S, Bergula A, Chen PC, Colwell CW Jr, D’Lima DD (2003) Polyethylene wear and acetabular component orientation. J Bone Joint Surg Am 85-A(Suppl 4):56–63
Little NJ, Busch CA, Gallagher JA, Rorabeck CH, Bourne RB (2009) Acetabular polyethylene wear and acetabular inclination and femoral offset. Clin Orthop Relat Res 467:2895–2900. doi:10.1007/s11999-009-0845-3
De Haan R, Pattyn C, Gill HS, Murray DW, Campbell PA, De Smet K (2008) Correlation between inclination of the acetabular component and metal ion levels in metal-on-metal hip resurfacing replacement. J Bone Joint Surg (Br) 90:1291–1297. doi:10.1302/0301-620X.90B10.20533
Langton DJ, Sprowson AP, Mahadeva D, Bhatnagar S, Holland JP, Nargol AV (2010) Cup anteversion in hip resurfacing: validation of EBRA and the presentation of a simple clinical grading system. J Arthroplasty 25:607–613. doi:10.1016/j.arth.2009.08.020
Walter LR, Marel E, Harbury R, Wearne J (2008) Distribution of chromium and cobalt ions in various blood fractions after resurfacing hip arthroplasty. J Arthroplasty 23:814–821. doi:10.1016/j.arth.2007.07.003
Langton DJ, Jameson SS, Joyce TJ, Webb J, Nargol AV (2008) The effect of component size and orientation on the concentrations of metal ions after resurfacing arthroplasty of the hip. J Bone Joint Surg (Br) 90:1143–1151. doi:10.1302/0301-620X.90B9.20785
Meftah M, Yadav A, Wong AC, Ranawat AS, Ranawat CS (2013) A novel method for accurate and reproducible functional cup positioning in total hip arthroplasty. J Arthroplasty 28:1200–1205. doi:10.1016/j.arth.2012.09.018
Inoue M, Majima T, Abe S, Nakamura T, Kanno T, Masuda T, Minami A (2013) Using the transverse acetabular ligament as a landmark for acetabular anteversion: an intra-operative measurement. J Orthop Surg (Hong Kong) 21:189–194
Epstein NJ, Woolson ST, Giori NJ (2011) Acetabular component positioning using the transverse acetabular ligament: can you find it and does it help? Clin Orthop Relat Res 469:412–416. doi:10.1007/s11999-010-1523-1
Fujita K, Kabata T, Maeda T, Kajino Y, Iwai S, Kuroda K, Hasegawa K, Tsuchiya H (2014) The use of the transverse acetabular ligament in total hip replacement: an analysis of the orientation of the trial acetabular component using a navigation system. Bone Joint J 96-B:306–311. doi:10.1302/0301-620X.96B3.32726
Zhu J, Wan Z, Dorr LD (2010) Quantification of pelvic tilt in total hip arthroplasty. Clin Orthop Relat Res 468:571–575. doi:10.1007/s11999-009-1064-7
Barrack RL, Krempec JA, Clohisy JC, McDonald DJ, Ricci WM, Ruh EL, Nunley RM (2013) Accuracy of acetabular component position in hip arthroplasty. J Bone Joint Surg Am 95:1760–1768. doi:10.2106/JBJS.L.01704
Callanan MC, Jarrett B, Bragdon CR, Zurakowski D, Rubash HE, Freiberg AA, Malchau H (2011) The John Charnley Award: risk factors for cup malpositioning: quality improvement through a joint registry at a tertiary hospital. Clin Orthop Relat Res 469:319–329. doi:10.1007/s11999-010-1487-1
Kennedy JG, Rogers WB, Soffe KE, Sullivan RJ, Griffen DG, Sheehan LJ (1998) Effect of acetabular component orientation on recurrent dislocation, pelvic osteolysis, polyethylene wear, and component migration. J Arthroplasty 13:530–534
Conroy JL, Whitehouse SL, Graves SE, Pratt NL, Ryan P, Crawford RW (2008) Risk factors for revision for early dislocation in total hip arthroplasty. J Arthroplasty 23:867–872. doi:10.1016/j.arth.2007.07.009
Rathod PA, Bhalla S, Deshmukh AJ, Rodriguez JA (2014) Does fluoroscopy with anterior hip arthroplasty decrease acetabular cup variability compared with a nonguided posterior approach? Clin Orthop Relat Res 472:1877–1885. doi:10.1007/s11999-014-3512-2
Widmer KH (2004) A simplified method to determine acetabular cup anteversion from plain radiographs. J Arthroplasty 19:387–390
Nho JH, Lee YK, Kim HJ, Ha YC, Suh YS, Koo KH (2012) Reliability and validity of measuring version of the acetabular component. J Bone Joint Surg (Br) 94:32–36. doi:10.1302/0301-620X.94B1.27621
Wera GD, Ting NT, Moric M, Paprosky WG, Sporer SM, Della Valle CJ (2012) Classification and management of the unstable total hip arthroplasty. J Arthroplasty 27:710–715. doi:10.1016/j.arth.2011.09.010
Moskal JT, Capps SG (2011) Acetabular component positioning in total hip arthroplasty: an evidence-based analysis. J Arthroplasty 26:1432–1437. doi:10.1016/j.arth.2010.11.011
Bicanic G, Delimar D, Delimar M, Pecina M (2009) Influence of the acetabular cup position on hip load during arthroplasty in hip dysplasia. Int Orthop 33:397–402. doi:10.1007/s00264-008-0683-z
D’Lima DD, Urquhart AG, Buehler KO, Walker RH, Colwell CW Jr (2000) The effect of the orientation of the acetabular and femoral components on the range of motion of the hip at different head-neck ratios. J Bone Joint Surg Am 82:315–321
Gandhi R, Marchie A, Farrokhyar F, Mahomed N (2009) Computer navigation in total hip replacement: a meta-analysis. Int Orthop 33:593–597. doi:10.1007/s00264-008-0539-6
Beckmann J, Stengel D, Tingart M, Gotz J, Grifka J, Luring C (2009) Navigated cup implantation in hip arthroplasty. Acta Orthop 80:538–544. doi:10.3109/17453670903350073
Kwon MS, Kuskowski M, Mulhall KJ, Macaulay W, Brown TE, Saleh KJ (2006) Does surgical approach affect total hip arthroplasty dislocation rates? Clin Orthop Relat Res 447:34–38. doi:10.1097/01.blo.0000218746.84494.df
Bosker BH, Verheyen CC, Horstmann WG, Tulp NJ (2007) Poor accuracy of freehand cup positioning during total hip arthroplasty. Arch Orthop Trauma Surg 127:375–379. doi:10.1007/s00402-007-0294-y
Myers GJ, Morgan D, McBryde CW, O’Dwyer K (2009) Does surgical approach influence component positioning with Birmingham Hip Resurfacing? Int Orthop 33:59–63. doi:10.1007/s00264-007-0469-8
Dienstknecht T, Luring C, Tingart M, Grifka J, Sendtner E (2013) A minimally invasive approach for total hip arthroplasty does not diminish early post-operative outcome in obese patients: a prospective, randomised trial. Int Orthop 37:1013–1018. doi:10.1007/s00264-013-1833-5
Jacquot F, Ait Mokhtar M, Sautet A, Doursounian L, Masquelet AC, Feron JM (2013) The mini postero-postero-lateral mini incision in total hip arthroplasty. Int Orthop 37:1891–1895. doi:10.1007/s00264-013-1970-x
Reichert JC, Volkmann MR, Koppmair M, Rackwitz L, Ludemann M, Rudert M, Noth U (2015) Comparative retrospective study of the direct anterior and transgluteal approaches for primary total hip arthroplasty. Int Orthop. doi:10.1007/s00264-015-2732-8
Waldstein W, Merle C, Schmidt-Braekling T, Boettner F (2014) Does stem design influence component positioning in total hip arthroplasty using a minimal invasive posterolateral approach? Int Orthop 38:1347–1352. doi:10.1007/s00264-014-2299-9
Acknowledgments
The authors wish to thank Carol for the fluoroscopic image and the standing AP pelvis X-ray acquisition, and Shen Jing M.D., for assisting the statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ji, W., Stewart, N. Fluoroscopy assessment during anterior minimally invasive hip replacement is more accurate than with the posterior approach. International Orthopaedics (SICOT) 40, 21–27 (2016). https://doi.org/10.1007/s00264-015-2803-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-015-2803-x