
Abstract
We investigated the prevalence and incidence of vertebral fractures worldwide. We used a systematic Medline search current to 2015 and updated as per authors’ libraries. A total of 62 articles of fair to good quality and comparable methods for vertebral fracture identification were considered. The prevalence of morphometric vertebral fractures in European women is highest in Scandinavia (26%) and lowest in Eastern Europe (18%). Prevalence rates in North America (NA) for White women ≥50 are 20–24%, with a White/Black ratio of 1.6. Rates in women ≥50 years in Latin America are overall lower than Europe and NA (11–19%). In Asia, rates in women above ≥65 are highest in Japan (24%), lowest in Indonesia (9%), and in the Middle East, Lebanon, rates are 20%. The highest–lowest ratio between countries, within and across continents, varied from 1.4–2.6. Incidence data is less abundant and more heterogeneous. Age-standardized rates in studies combining hospitalized and ambulatory vertebral fractures are highest in South Korea, USA, and Hong Kong and lowest in the UK. Neither a North-South gradient nor a relation to urbanization is evident. Conversely, the incidence of hospitalized vertebral fractures in European patients ≥50 shows a North-South gradient with 3–3.7-fold variability. In the USA, rates in Whites are approximately 4-fold higher than in Blacks. Vertebral fractures variation worldwide is lower than observed with hip fractures, and some of highest rates are unexpectedly from Asia. Better quality representative studies are needed. We investigate the occurrence of vertebral fractures, worldwide, using published data current until the present. Worldwide, the variation in vertebral fractures is lower than observed for hip fractures. Some of the highest rates are from North America and unexpectedly Asia. The highest–lowest ratio between countries, within and across continents, varied from 1.4–2.6. Better quality representative data is needed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Vertebral fractures are the most common single osteoporotic fractures worldwide, constituting an integral part of the osteoporotic syndrome; they occur in 30–50% of people over the age of 50 [1]. However, in contrast to hip fractures, many factors limit the availability of reliable information on their epidemiology: two-thirds to three-fourths of vertebral fractures are clinically silent [2, 3] and less than 10% require hospital admission [4], which itself may vary by geographic differences in access to healthcare. Additional considerations include the following: Even when there is a vertebral fracture on the spine radiograph, it is often missed by the radiologist, rarely noted in the medical records, and infrequently prompts preventive treatment [5]. As an osteoporotic fracture, the incidence rates rise exponentially with age so that differences in the age ranges included in studies can have a major impact on the findings. Rates also depend on the definition of vertebral fracture, clinical versus morphometric. Moreover, the morphometric definition is not universal; at least seven methods have been used in different studies, as will be discussed later in this article. Within the same method, varying decision thresholds (fracture grade or standard deviation from means) make the definition of vertebral fracture even more difficult [6].
Notwithstanding these limitations, we aimed to define the incidence and prevalence of vertebral fractures worldwide and to compare rates across countries, continents, and different ethnic groups. To our knowledge, such an extensive comparative review of the most common osteoporotic fracture, including data on both incidence and prevalence in almost all countries where such information is available, has not been undertaken to date.
Materials and methods
Literature search
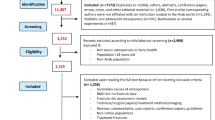
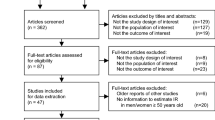
A Medline Ovid search covering the period between January 1st 1966 and October 30th 2015 was conducted. Search was limited to English language and to human adults aged 19 and above. The search consisted of the following concepts and their related terms: vertebral fracture, prevalence, incidence, and continent/country X with each concept searched singly, then merged through the AND term. Screening by title left 322 relevant articles. After abstract review, 63 articles reporting either prevalence (39 articles) or incidence (24 articles) of vertebral fractures in a specific region or country were included in the final analysis. No additional selection criteria were applied because of the scarcity of data. Other relevant articles were selected from the reference list of the evaluated articles, the authors’ libraries, and major scientific meetings.
Quality rating of the studies
The articles were rated as of good, fair, or poor quality using different criteria for prevalence and incidence papers. All authors agreed on the criteria, and the rating was performed by one author.
Prevalence studies confined to a single country were rated as good, fair, or poor if they, respectively, fulfilled three, two, or one of the following criteria: multicenter or population-based representing a large geographic area, large sample size (representing >500/10 [6] of the age and sex-matched population of the whole country), and pre-specified criteria for diagnosis of fracture by published protocols.
Prevalence studies across countries were rated as good, fair, or poor if they respectively fulfilled three, two, or one of the following criteria: any information in the methods that specifies selection of sample from a population-based database, pre-specified criteria for diagnosis of fracture by published protocols, and prevalence of vertebral fractures provided by country.
Incidence studies were graded according to criteria originally developed by our group for the FRAX International Task Force Statement to rate studies on hip fracture incidence [7] and detailed as follows:
-
Good: If at least four of the following criteria were met: prospective study, study population representative of the entire population, study duration more than 1 year, adequate definition of fracture or ICD codes used, ethnicities defined when applicable.
-
Poor: If at least four of the following criteria were met: retrospective study, study duration of 1 year or less, non-population based, inadequate definition of fracture, only abstract available, no definition of ethnicities provided.
-
Fair: Sources that did not meet the criteria for either good or poor.
Vertebral fracture definition
Comparison of vertebral fracture incidence and prevalence between different regions and countries is most reliable when vertebral fractures are morphometrically defined. However, because of multiplicity of methods, rates may differ within the same patient population: In the European Vertebral Osteoporosis Study (EVOS), O’Neill et al. [6] reported the prevalence of vertebral fractures in men and women aged 50 to 79 from 36 centers in 19 European countries (Table 1) using two methods, the McCloskey and Eastell methods. Rates reported in each age group by the Eastell method were 1.4 to 2.3 times higher than those reported by the McCloskey method.
The morphometric methods described by Melton [8], Eastell [5], Black [9], and CaMOS [10] use four vertebral height ratios: Ha/Hp, Hm/Hp, Hp/Hp-above, and Hp/Hp-below, where Ha is anterior height, Hp is posterior height, Hm is middle height, Hp-above is posterior height of the vertebra above, and Hp-below is posterior height of the vertebra below. However, they use different reference populations to define normal ratios. McCloskey and Davies define other ratios: In the McCloskey method [11], a predicted posterior height (Hpred) is calculated for each vertebra from the posterior heights of up to four adjacent vertebrae. The Davies method [12] defines two variables for each vertebra, the wedge shape variable and the relative posterior height variable. Detailed description of these methods is provided in Appendix 1.
In addition to the quantitative methodology above, studies using a semi-quantitative methodology have been reported. The semi-quantitative method described by Genant [13] relies on visual estimation of reduction in vertebral height without the aid of direct measurements. A reduction of 20–25% in anterior, middle, and/or posterior height and a reduction of area of 10–20% define mildly deformed or grade 1 fracture, a reduction of 25–40% in any height and 20–40% in area define moderately deformed or grade 2 fracture, and a reduction of 40% or more in any height and area define severely deformed or grade 3 fracture. This method can be applied to a regular X-ray film or to the vertebral fracture assessment (VFA) on the DEXA scan.
For the purpose of synthesis of studies, we compare across the studies that used the methods described by Melton, Eastell, Black, and the CaMOS study group because they all use the same height ratios and the difference in prevalence rates provided by these methods is anticipated to be relatively minor. Indeed, a study on vertebral fractures in Beijing, China [14] recruiting 402 women aged 50 and above examined rates using both the Black and Eastell methods: prevalence provided by the Eastell method was 1.24-fold that of the Black method (18.6 and 15%, respectively). On the other hand, studies utilizing the McCloskey and Genant methods are reported and compared separately.
Age-standardized vertebral fractures incidence rates
To allow a more accurate comparison between countries, incidence rates of hospitalized and ambulatory vertebral fractures are age-standardized using the United Nations World Population estimates for both 2010 and 2015. Studies providing age-specific rates in 5-year age groups are used for standardization. We include the 2010 prospects for the purpose of comparison to previous reviews, if any, which calculated age-standardized rates. We could not perform standardization for studies providing only hospitalized vertebral fractures because the age groups included were very heterogeneous.
Results
Vertebral fractures prevalence
The prevalence of vertebral fractures is more extensively studied worldwide than incidence, and despite the differences in the morphometric methods and age groups included, studies are easier to interpret and compare. The table provides a summary of the prevalence studies in different countries grouped by continent and method of vertebral fracture ascertainment.
Studies using the Melton, Eastell, Black, and the CaMOS study group methods
The largest study on vertebral fracture prevalence from Europe is the EVOS [6] that recruited more than 15,000 men and women from 19 countries (see Table 1). Using the Eastell method, the overall vertebral fracture prevalence rate was 20% in both genders. Comparison between the different European regions showed minimal differences, with the highest recorded rates in Scandinavia and the lowest rates in Eastern Europe. Men aged 50 to 64 years had overall a higher prevalence of fractures than similarly aged women, with the reverse being observed in those aged over 65 years. This pattern suggests that the etiology of fractures in young men may relate to higher rates of trauma, whereas fractures occurring at older ages are more likely to be the result of skeletal fragility. Interestingly, there was greater heterogeneity in prevalence between countries than between genders, which raises the possibility that environmental and/or genetic factors might be more important factors in the pathogenesis of vertebral osteoporosis than estrogen deficiency. The nationwide CaMOS [10] from Canada, the Study of Osteoporotic Fractures (SOF) from USA [15], and the Rochester, USA study by Melton [16] all showed similar prevalence rates of vertebral fractures in women of 20–23% (see Table 1). These rates fall well within the range of those recorded in Europe. CaMOS is the only northern American study providing rates in men, and similarly to EVOS, it shows women-to-men ratio of 1. SOF compared prevalence rates between Black and White women aged 65 and above, and the difference was significant; however, the proportion of Black women in the studied sample was small [17]. Latin America shows somewhat lower prevalence of vertebral fractures. The Latin America Vertebral Osteoporosis Study (LAVOS) [18] revealed an overall rate of 14.8%. The highest rate in Mexico was within the same range as other continents, and the lowest rate was reported in Puerto Rico. Rates in elderly men from Latin America are reported in a small study from Mexico [19] and showed the lowest rates worldwide: 2-fold lower than rates reported in men in EVOS [6] and CaMOS [10], despite the fact that the latter two studies recruited men in younger age groups.
Prevalence rates of vertebral fractures in Asia are more heterogeneous with marked differences between countries and even within the same country (see Table 1). Comparison of studies reporting rates in women ≥50 using the 3 SD cutoff of the Eastell method shows a 1.42-fold difference between the highest rates in Vietnam [20] and the lowest rates in China 18.6% [14]. Considering men and women aged 65 and above and using the Black method, there is a 2.7-fold difference between the highest rates in Japan and the lowest rates in Hong Kong [21]. Rates reported in the same country (Hong Kong) differed markedly between studies; despite using the same definition of vertebral fracture, the small study by Kwok et al. [21] showed rates in women 3.5-fold and 2.6-fold lower than those reported by the much larger studies by Lau [22] and Tsang [23], respectively. Surprisingly, the rates in men in some Asian countries appear much higher than those of women; the multicenter study by Kwok [21] revealed women-to-men ratio of 0.6 in Japan, Thailand, Indonesia, and Hong Kong. The higher rates in men were also observed in Thailand by Jitapunkul [24], where the women-to-men ratio was 0.8. In contrast, the ratios in Vietnam (1.15) [20], Taiwan (1.65) [25], and Korea (1.24) [26] were in favor of higher rates in women.
Studies using the McCloskey method
Studies using the McCloskey method to define vertebral fracture are confined to Europe. As mentioned earlier, the McCloskey method was applied to the EVOS population in addition to the Eastell method [6]; it showed the same geographic variability and an overall women-to-men ratio of around 1 (see Table 1). Although it included older age groups compared to the EVOS, the Rotterdam study [27] showed lower prevalence rates in both genders than those reported for the Rotterdam center in the EVOS. It is important to underscore that the Rotterdam study had a much larger sample size and was more representative of the population in the Netherlands. Similarly, a study from one center in London [28] showed a substantially lower prevalence rate compared with the rates reported in the UK centers included in the EVOS. This difference might well be explained by the difference in the age groups included, in addition to a difference in the sample size.
In conclusion, studies using the McCloskey method to define vertebral fractures are few and difficult to compare but generally show lower prevalence rates than Eastell or Black methods. The results of the EVOS study show a 1.4-fold variability in prevalence between the different European regions in men and 1.8-fold in women, much lower than the variability in hip fracture rates (4.9-fold in men 8.8-fold in women) [29], and again show an overall women to men ratio of 1.
Studies using the Genant method
Despite the same methodology to define vertebral fractures, studies using the Genant method are also heterogeneous with regard to the age groups included, the sample size, and the deformity grade considered to be a fracture likely because it relies on the clinical judgment of the investigator.
In Europe, rates reported in women in France [30] are similar to those reported in the Netherlands [31] despite the older age groups included in the former study. These rates are 1.7-fold higher than those reported in women from Norway [32], but again major differences are evident because the Norway study included a younger population and a much larger sample size (see Table 1). Rates in Spanish women [33] are slightly lower than in Norway.
Two small studies from North America used the Genant method. One study from Chicago [34] showed a similar rate of vertebral fractures between Black and White women; however, after correction for age, rates were higher in White women. Compared to Europe, the prevalence of vertebral fractures using the Genant method in the USA seems even higher than those of Northern Europe (Norway) [32]. On the other hand, rates in Canada [35] are close to those reported in Norway. Considering the poor quality of the North American studies using the Genant method, intercontinental comparison may not be accurate.
The only study to use the Genant method from South America was conducted in Brazil [36] on a relatively small sample. It showed rates close to those reported in Europe in both genders.
Studies from Asia using the Genant method were also small, except the study from Hong Kong [37]. The highest rates are reported in Vietnam [38], similar to those of the USA [34] and higher than rates in Europe [32, 33]. These rates are concordant with the high rates reported using the Eastell method in Vietnam [20]. Rates in Indian men are the highest among studies using the Genant method worldwide; rates in Indian women are also elevated (17.1%) and close to those of the USA [39]. Low rates are reported in Japan [40, 41], close to those from Southern Europe [33]. Using the Eastell method, Japan ranks among the highest rates in Asia [21]; however, the latter method was applied to a much smaller sample of older women.
The few studies on vertebral fracture prevalence in the Middle East relied only on the Genant method. One study from Morocco reports the highest rates of vertebral fractures in women worldwide [42]; however, the study is rated as poor and the reported rate is questionable. Another study from Morocco [43] reports rates in men close to rates in European men. In a representative study from Lebanon [44], rates of vertebral fractures in women are close to the US rates, whereas rates in men are similar to those in European men.
In summary, considering good quality studies using the same, mostly those that relied on the Genant method and that spanned across continents, we conclude that the prevalence of vertebral fractures varies slightly in women across countries. The highest rates are reported in Scandinavia [6] (26%), Canada [10] and the Mediterranean region [6] (23%), Hong Kong [23] (22%), Western Europe [6], USA [15], and Mexico [18] (20%), followed by Eastern Europe [6] and Taiwan [25] (18%). The lowest rates are seen in Latin America [18] (15%). The women-to-men ratio from EVOS in Europe and CAMOS in Canada is 1; however, good quality studies from other regions did not report on prevalence rates in men.
Vertebral fractures incidence
Vertebral fracture incidence data is not abundant; 24 studies, the majority of which stem from Europe and North America, will be reviewed in detail. Appendices 2 and 3 provide a summary of these studies, along with quality ratings. Eighteen of them report the incidence of clinical vertebral fractures: 16 use ICD code for vertebral fracture definition. Two studies, one from Sweden [45] and one from Australia [46], report incidence of clinical vertebral fractures based on radiologist’s report only. One study from Japan [47] reported incidence based on a morphometric method issued by the Japanese Society of Bone and Mineral Research.
Five additional studies are prospective and reported baseline prevalence and incidence on follow-up using morphometric methods, with the exception of one study from Hong Kong [48]. The latter defined clinical incident fracture by history and confirmed it by the ICD code.
Clinical vertebral fractures using ICD codes
Two major factors impact our ability to compare incidence studies using ICD codes: the ICD codes used and the age groups included in the studies. The newest version of the ICD 10 code defines many subtypes of vertebral fractures, and depending on the specific codes used by each study, they may include single or multiple fractures at different vertebral levels that can include the cervical spine, traumatic rupture of intervertebral disc, dislocation and strain of vertebrae, joints and ligaments, and collapsed vertebrae. The older ICD-9 version defines two main categories: open or closed fractures at any vertebral level with (ICD-9806) and without (ICD-9805) mention of spinal cord injury. The use of this code and the choice of the fracture location and type to be included in each study largely influence incidence rates, in addition to the fact that ICD codes do not distinguish high from low trauma fractures. The younger the population included, the lower the incidence of vertebral fractures and the higher the proportion of high trauma fractures included.
Twelve of the selected incidence studies using ICD codes report data on ambulatory and hospitalized vertebral fractures. These studies are very heterogeneous in many aspects: the ICD code used, the age groups studied, and the recruitment method especially of the ambulatory vertebral fractures (emergency room cases or outpatient visits or review of treatment expenditures). This heterogeneity renders a comparison and synthesis across regions not possible. Age-specific rates for these fractures are illustrated in Appendix 4. The quality ratings applied to the studies detailing these incidence rates in the countries illustrated in the Appendix figure were good with the exception of Germany, Australia, Sweden, and Hong Kong that were rated as fair.
In Europe, the oldest study is from the UK [49] and spans from 1988 to 1998; it is a nationwide study including all patients aged 20 and above. Incidence rates reported were 32/100,000/year in men and 56/100,000/year in women, lower than those reported in most European countries. As expected, within this cohort, the rates increase with age. Rates reported in a regional study from Germany [50] for the years 2008–2009 are also lower than other European countries, especially in men and younger women. Nationwide data from Italy [51], Switzerland [52], and Iceland [53] shows similar incidence rates of hospitalized and ambulatory fractures. Age-specific nationwide rates reported from Slovenia [54] are the highest in Europe.
In North America, the study from Canada [55] on hospitalized and ambulatory vertebral fractures for the years 1981 to 1984 reports low age-specific incidence rates in Manitoba, close to those in the UK. In contrast, the US study by Melton LJ [56], reporting rates from 1989 to 1991, showed much higher age-specific incidence rates in Olmsted County, close to those reported in Slovenia for women. The most recent data from Olmsted County [57] shows even higher age-specific rates of clinical vertebral fractures in 2009–2011 compared to 1989–1991.
Recently, more studies on the incidence of vertebral fractures have emerged from Asia. One study from Hong Kong [48] reported age-specific rates close to those reported in Olmsted. Another nationwide study from Asia was conducted in South Korea [58] between 2005 and 2008. It shows no difference in the incidence between 2005 and 2008, but it reports the highest age-specific incidence rates of hospitalized and ambulatory vertebral fractures worldwide, more than the double of those reported in the USA.
Comparison of age-standardized rates of hospitalized and ambulatory vertebral fractures, as shown in Fig. 1a, b, depicts a somewhat similar ranking to the age-specific rates shown in Appendix 4. The lowest rates are again reported in the UK and Germany, followed by Italy, Australia, Iceland, Switzerland, and Sweden; the highest rates are recorded in Hong Kong, the USA, and South Korea. Moreover, Fig. 2 reveals the absence of a North to South gradient for these fractures.

Age-standardized incidence rates in women worldwide, combining hospitalized and ambulatory vertebral fractures, ranked by descending incidence. Standardization to 2010 UN population (a) and 2015 UN population (b)

Age-standardized incidence rates in women worldwide, combining hospitalized and ambulatory vertebral fractures, ranked by Latitude from North to South. Standardization implemented to 2010 UN population
More homogeneous comparisons of clinical vertebral fracture rates are available from studies reporting exclusively the incidence of hospitalized clinical vertebral fractures, yet these studies may be even more biased by economic and cultural differences that affect hospitalization rates than studies which include outpatient fracture cases. The largest among these studies was conducted in Europe from 1990 to 1997 and included eight countries [59]. Incidence rates were age-standardized to the 1990 Swedish population. The variability in rates was not as pronounced as that of hip fractures, showing a 3-fold variability of rates in men and a 3.7-fold variability in women. A north-south gradient was evident with the highest rates observed in Scandinavia for both genders and the lowest in Central and Southern Europe. The ratio of women to men varied between 0.94 and 1.75, if one excluded Slovakia where the ratio was 0.74. Two other studies from Europe reported incidence rates of hospitalized clinical vertebral fractures, one from Sweden [60] examined the incidence for the years 1997 to 2001 and the other from Spain [61] examined rates for 2002; both studies showed a sharp increase in incidence after the age of 60 in both genders, and despite an apparent similarity between the rates in both countries, the comparison may not be accurate. Indeed, the two studies used different ICD codes. Another large study reporting incidence of hospitalized vertebral fractures examined rates in Whites as compared to Blacks aged 65 and above in the USA for the years 1986 to 1989 [62]. It showed overall rates in White men and women approximately 4-fold higher than in Blacks. Moreover, incidence rates in White men and women rose exponentially with age, while the rise was linear for Black men and women. The ratio of women to men was 1.7 in Whites and 1.5 in Blacks.
Despite the difficulty in comparing across studies, the few studies reporting incidence of hospitalized clinical vertebral fractures also suggest that there is less geographic variability and less gender difference in hospitalized vertebral fractures than we previously identified for hip fractures [29].
Incidence of morphometric vertebral fractures
These studies are prospective and report baseline prevalence of vertebral fractures and incidence on follow-up using serial lateral spine films. They are difficult to compare because of differences in sample size, methods used to define vertebral fractures, and variability in duration of follow-up (Appendix 3).
The Rotterdam study [27] which included more than 3000 persons, followed for 4 to 7 years, showed an overall incidence of 590/100,000 PY in men and 1470/100,000 PY in women using the McCloskey method, with women-to-men ratio of 2.5. Women with one or more vertebral fractures at baseline had a higher incidence of vertebral fractures than those without a fracture at baseline (26 and 5%, respectively). A similar but less pronounced difference was seen in men, where the incidence was 9% in men with and 3% in men without prevalent fractures at entry. Another large population-based study, the Canadian Multicenter Osteoporosis Study (CaMOS) [10], recruited more than 9000 subjects followed for 5 years; it showed that a similar proportion of men and women experienced a new vertebral fracture 13.5 and 12%, respectively, despite significantly lower BMD T-scores in women. In Asia, the Adult Health Study in Hiroshima, Japan [40], involving more than 2000 subjects followed up for a mean period of 4 years, also showed high age-specific incidence rates of vertebral fractures in this population with an exponential rise with increasing age. A smaller study from Thailand [24], using Genant Grade 1 and above, followed patients for 5 years showed much lower incidence rates and, surprisingly, higher rates in men even after the age of 70. Again, these studies are very heterogeneous regarding the sample size, sample selection, and the method of ascertainment of vertebral fracture.
Discussion
To the best of our knowledge, this study provides the most detailed synthesis regarding the prevalence and incidence of vertebral fractures worldwide to date. It used a systematic review approach and studies selected after applying a quality assessment, compiled data from studies with comparable methods, and implemented age-standardized incidence rates. It highlights the scarcity of good quality data on the most common osteoporotic fracture, in large part due to its silent nature, and identifies limitations, challenges, and knowledge gaps.
The effect of increasing age on vertebral fracture prevalence is readily apparent by evaluating results expressed by gender and age group within, but not across, several large population-based studies, such as EVOS [6], EPIDOS [30], LASA [31], and others [14, 16, 18, 21, 24, 33]. However, although it has been previously suggested that the overall vertebral fracture rates are less variable across countries and ethnicities [7, 63, 64], our review reveals that it is not possible to confidently draw such firm conclusions, either regarding vertebral fracture prevalence or incidence. While a low variability in vertebral fracture prevalence seems evident in Europe (a ratio of 1.4 between Scandinavia and eastern Europe for both genders reported in the EVOS study [6]) and North America (similar prevalence rates reported in the USA and Canada [10, 15, 16]), greater variations appear in Asia and Latin America, even when comparing studies that applied the same methods to diagnose morphometric fractures. The greatest variability is evident in Asia, with a ratio of 2.7 noted between the highest (Japan) and lowest (Hong Kong), in both genders, above the age of 65 [21]. Similarly, the LAVOS study in South America noted a ratio of 1.8 between the highest (Mexico) and lowest (Colombia) rates [18].
As to ethnic differences in vertebral fracture prevalence rates, we could only identify the SOF study [17] where adjusted rates were reported to be 45–50% lower among Black women (analyses adjusted for age, BMD, and other risk factors). Such racial difference may be attributed to inherent ethnic differences in bone structure and quality, similar to other osteoporotic fractures [65, 66].
Regardless of study methodology, the incidence of vertebral fractures in both genders above the age of 50 also rises with age, being higher in women than in men, within the same country (Appendix 2). As shown in Fig. 2, comparison of age-standardized rates, for combined ambulatory and hospitalized fractures, across countries, does not reveal a North to South gradient, nor a clear socio-economic development gradient. This lack of North to South gradient persists even when one considers studies implemented within the same time frame, for example after 2000, such as is the case for the USA, Germany, Switzerland, Italy, and South Korea. Conversely, the study by Johnell et al. conducted within the same time frame exclusively in Europe that limited reporting to the incidence of hospitalized vertebral fractures reveals higher rates in Scandinavia compared to Central and Southern countries [59]. Whereas the former method of identification may be more representative of incident fractures in populations at large, the latter could be affected by selection bias and misclassification that could vary by country. Its strength would be to only capture definite vertebral fractures, but its drawback would be the inclusion of non-osteoporotic fractures (such as thoracic or traumatic fractures).
Data on ethnic differences in the incidence of hospitalized vertebral fractures is only available in the USA, where a White-to-Black ratio of 4 was reported [62]. Such ratio, in addition to potentially reflecting inherent differences in bone quality and architecture as reported for vertebral fractures, may however be an overestimate reflecting poor access to medical care in the Black population.
Comparison of vertebral fracture epidemiology across countries and continents had been previously attempted [7, 48, 63, 67, 68]. When incidence was reported, studies were compared without distinction between hospitalized and ambulatory fractures, and only one review separated clinical from morphometric incident fractures [68]. The main conclusions from such reviews were, as expected, an increase in the incidence of vertebral fractures with age, but a higher rate in women than in men, findings that contrast with the gender variability we note in this review. Furthermore, none of the previous studies derived age-standardized rates, a major drawback when comparing across countries and regions. Although the discussions regarding the prevalence of vertebral in comparison to incident fractures were more detailed [63, 67], such comparisons ignored differences between morphometric methods in the various studies quoted and/or did not include all relevant studies. For example, one review found higher rates in Asian women compared to the USA [63], while the most recent one alluded to higher prevalence rates in Caucasians compared to Asians and Latin Americans [67]. All of the above limitations partially explain the opposing trends reported by others, and underscore the added strengths of our synthesis, and the differences in its main conclusions.
Our review still has some limitations that may, in part, be related to the search methodology applied to the literature, focusing exclusively on the Medline OVID database and only considering articles published in English. However, it was complemented by the inclusion of additional references from retrieved articles as applicable, review articles retrieved from a PubMed search current until October 2015, and related publications from the authors’ libraries. Other limitations are inherent to the quality of published studies, including the representativeness of study population, methods to identify vertebral fractures, multiplicity of morphometric methods used, and sample size considered, to name a few. For example, a 1.25 to 2-fold difference in prevalence rates was noted in the same population where different methods were applied [6, 14]. We have tried to overcome these inherent limitations by applying a formal quality assessment to all studies retrieved and combined studies that used comparable criteria to diagnose incident fractures. Specifically, only studies of fair to good quality were included and comparisons were implemented using vertebral fracture diagnosis methods that were more readily comparable for prevalent vertebral fractures and ICD codes for incident fractures. However, the use of ICD codes has its own drawbacks, as it includes any vertebral deformity at any vertebral level and does not differentiate between low and high trauma fractures.
Finally, possible secular trends in the incidence of vertebral fractures make the comparison of rates from different countries at different time points less accurate. Studies on combined hospitalized and ambulatory vertebral fractures covered a wide time range, spanning from 1981 (Canada) [55] to 2008–2011 (Italy [51], Germany [50], Rochester [57], and South Korea [58]). In the USA, the incidence of vertebral fractures in Rochester based on file review and radiology reports was reported to be stable rates in men and women aged 35 to 69 between 1965 and 1989 [69] in contrast to an increase in the same region and for both genders between 1989–1991 and 2009–2011 [57]. Such findings may in part be attributed to increased attention to osteoporosis and vertebral fractures by radiologists [57]. Conversely, a population-based report from Canada reported stable vertebral fracture in incidence rates, in men and women above the age of 50 years, over a span of two decades (1986–2006) [70], while a population-based cohort study from Iceland revealed a trend toward a decline in the incidence of vertebral fractures, in both genders, over an overlapping time period (1989 to 2008) [53]. Therefore, the potential impact of secular trends should be considered when comparing fracture incidence rates, including vertebral fractures, across regions and countries.
Conclusion
Osteoporotic vertebral fractures are common, increase the risk of other major fragility fractures, and incur high societal costs and mortality. However, their epidemiology is not well characterized. The available data point to a possible lower gradient of variability, across genders, ethnicities, and countries, than that of hip fractures, possibly reflecting a lower influence of environmental factors. The universal use of a unified standardized method for vertebral fracture definition, drawn from representative sections of the populations, across similar and ideally large time periods, is needed to allow an adequate assessment of the epidemiology of vertebral fractures.
References
Bouxsein M, Genant H (2010) International Osteoporosis Foundation Vertebral Fracture Audit. wwwiofbonehealthorg
Kanis JA, Oden A, McCloskey EV, Johansson H, Wahl DA, Cooper C (2012) A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int
Fink HA, Milavetz DL, Palermo L et al (2005) What proportion of incident radiographic vertebral deformities is clinically diagnosed and vice versa? J Bone Miner Res 20(7):1216–1222
Gehlbach SH, Bigelow C, Heimisdottir M, May S, Walker M, Kirkwood JR (2000) Recognition of vertebral fracture in a clinical setting. Osteoporos Int 11:577–582
Eastell R, Cedel SL, Wahner HW, Riggs BL, Melton LJΙ (1991) Classification of vertebral fractures. J Bone Miner Res 6(3):207–215
O’Neill TW, Felsenberg D, Varlow J et al (1996) The prevalence of vertebral deformity in European men and women: the European vertebral osteoporosis study. J Bone Miner Res 11(7):1010–1018
Cauley JA, El-Hajj Fuleihan G, Luckey MM (2011) FRAX(R) international task force of the 2010 joint International Society for Clinical Densitometry & international osteoporosis foundation position development conference. J Clin Densitom 14(3):237–239
Melton LJ, Kan SH, Frye KM, Wahner HW, O’Fallon WM, Riggs B (1989) Epidemiology of vertebral fractures in women. Am J Epidemiol 129:1000–1011
Black DM, Cummings SR, Stone K, Hudes E, Palermo L, Steiger P (1991) A new approach to defining normal vertebral dimensions. J Bone Miner Res 6(8):883–892
Jackson SA, Tenenhouse A, Robertson L (2000) Vertebral fracture definition from population-based data: preliminary results from the Canadian multicenter osteoporosis study (CaMos). Osteoporos Int 11(8):680–687
McCloskey EV, Spector TD, Eyres KS et al (1993) The assessment of vertebral deformity: a method for use in population studies and clinical trials. Osteoporos Int 3:138–147
Davies KM, Recker RR, Heaney RP (1989) Normal vertebral dimensions and normal variation in serial measurements of vertebrae. J Bone Miner Res 4(3):341–349
Genant HK, Wu CY, Kuijk CV, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8(9):1137–1148
Ling X, Cummings SR, Mingwei Q et al (2000) Vertebral fractures in Beijing, China: the Beijing osteoporosis project. J Bone Miner Res 15(10):2019–2025
Kado DM, Browner WS, Palermo L, Nevitt MC, Genant HK, Cummings SR (1999) Vertebral fractures and mortality in older women: a prospective study. Study of Osteoporotic Fractures Research Group. Arch Intern Med 159(11):1215–1220
Melton LJ 3rd, Lane AW, Cooper C, Eastell R, O’Fallon WM, Riggs BL (1993) Prevalence and incidence of vertebral deformities. Osteoporos Int 3(3):113–119
Cauley JA, Palermo L, Vogt M et al (2008) Prevalent vertebral fractures in black women and white women. J Bone Miner Res 23(9):1458–1467
Clark P, Cons-Molina F, Deleze M et al (2009) The prevalence of radiographic vertebral fractures in Latin American countries: the Latin American vertebral osteoporosis study (LAVOS). Osteoporos Int 20(2):275–282
Clark P, Cons-Molina F, Deleze M, Talavera JO, Palermo L, Cummings SO (2010) The prevalence of radiographic vertebral fractures in Mexican men. Osteoporos Int 21(9):1523–1528
Ho-Pham LT, Mai LD, Pham HN, Nguyen ND, Nguyen TV (2012) Reference ranges for vertebral heights and prevalence of asymptomatic (undiagnosed) vertebral fracture in Vietnamese men and women. Arch Osteoporos 7:257–266
Kwok AW, Leung JC, Chan AY et al (2012) Prevalence of vertebral fracture in Asian men and women: comparison between Hong Kong, Thailand, Indonesia and Japan. Public Health 126(6):523–531
Lau EM, Chan HH, Woo J et al (1996) Normal ranges for vertebral height ratios and prevalence of vertebral fracture in Hong Kong Chinese: a comparison with American Caucasians. J Bone Miner Res 11(9):1364–1368
Tsang SW, Bow CH, Chu EY, Yeung SC, Soong CC, Kung AW (2011) Clinical risk factor assessment had better discriminative ability than bone mineral density in identifying subjects with vertebral fracture. Osteoporos Int 22(2):667–674
Jitapunkul S, Thamarpirat J, Chaiwanichsiri D, Boonhong J (2008) Incidence of vertebral fractures in Thai women and men: a prospective population-based study. Geriatr Gerontol Int 8(4):251–258
Tsai K, Twu S, Chieng P, Yang R, Lee T (1996) Prevalence of vertebral fractures in chinese men and women in urban Taiwanese communities. Calcif Tissue Int 59(4):249–253
Shin CS, Kim MJ, Shim SM et al (2012) The prevalence and risk factors of vertebral fractures in Korea. J Bone Miner Metab 30(2):183–192
Van der Klift M, De Laet CE, McCloskey EV, Hofman A, Pols HA (2002) The incidence of vertebral fractures in men and women: the Rotterdam study. J Bone Miner Res 17(6):1051–1056
Spector TD, McCloskey EV, Doyle DV, Kanis JA (1993) Prevalence of vertebral fracture in women and the relationship with bone density and symptoms: the Chingford study. J Bone Miner Res 8(7):817–822
Ballane G, Cauley JA, Arabi A, El-Hajj Fuleihan G (2013) Geographic variability in hip and vertebral fractures. In: Marcus R, Feldman D, Dempster DW, Luckey M, Cauley CE (eds) Osteoporosis, 4th edn, pp 623–644
Grados F, Marcelli C, Dargent-Molina P et al (2004) Prevalence of vertebral fractures in French women older than 75 years from the EPIDOS study. Bone 34(2):362–367
Pluijm SM, Tromp AM, Smit JH, Deeg DJ, Lips P (2000) Consequences of vertebral deformities in older men and women. J Bone Miner Res 15(8):1564–1572
Waterloo S, Nguyen T, Ahmed LA et al (2012) Important risk factors and attributable risk of vertebral fractures in the population-based Tromso study. BMC Musculoskelet Disord 13:163
Sanfelix-Genoves J, Reig-Molla B, Sanfelix-Gimeno G et al (2010) The population-based prevalence of osteoporotic vertebral fracture and densitometric osteoporosis in postmenopausal women over 50 in Valencia, Spain (the FRAVO study). Bone 47(3):610–616
Vokes TJ, Gillen DL, Pham AT, Lovett JM (2007) Risk factors for prevalent vertebral fractures in black and white female densitometry patients. J Clin Densitom 10(1):1–9
Yakemchuk V, Beaumont LF, Webber CE, Gulenchyn KY, Jager PL (2012) Vertebral fracture prevalence in a referral population of 750 Canadian men and women. Clin Radiol 67(11):1061–1068
Lopes JB, Danilevicius CF, Takayama L et al (2011) Prevalence and risk factors of radiographic vertebral fracture in Brazilian community-dwelling elderly. Osteoporos Int 22(2):711–719
Kwok AW, Gong JS, Wang YX et al (2013) Prevalence and risk factors of radiographic vertebral fractures in elderly Chinese men and women: results of Mr. OS (Hong Kong) and Ms. OS (Hong Kong) studies. Osteoporosis international: a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA 24(3):877–885
Ho-Pham LT, Nguyen ND, Vu BQ, Pham HN, Nguyen TV (2009) Prevalence and risk factors of radiographic vertebral fracture in postmenopausal Vietnamese women. Bone 45(2):213–217
Marwaha RK, Tandon N, Gupta Y et al (2012) The prevalence of and risk factors for radiographic vertebral fractures in older Indian women and men: Delhi vertebral osteoporosis study (DeVOS). Arch Osteoporos 7:201–207
Fujiwara S, Kasagi F, Masunari N, Naito K, Suzuki G, Fukunaga M (2003) Fracture prediction from bone mineral density in Japanese men and women. J Bone Miner Res 18(8):1547–1553
Kitazawa A, Kushida K, Yamazaki K, Inoue T (2001) Prevalence of vertebral fractures in a population-based sample in Japan. J Bone Miner Metab 19(2):115–118
Rostom S, Allali F, Bennani L, Abouqal R, Hajjaj-Hassouni N (2012) The prevalence of vertebral fractures and health-related quality of life in postmenopausal women. Rheumatol Int 32(4):971–980
El Maghraoui A, Mounach A, Rezqi A, Achemlal L, Bezza A, Ghozlani I (2012) Vertebral fracture assessment in asymptomatic men and its impact on management. Bone 50(4):853–857
Baddoura R, Arabi A, Haddad-Zebouni S et al (2007) Vertebral fracture risk and impact of database selection on identifying elderly Lebanese with osteoporosis. Bone 40(4):1066–1072
Kanis JA, Johnell O, Oden A et al (2000) Long-term risk of osteoporotic fracture in Malmo. Osteoporos Int 11:669–674
Sanders KM, Seeman E, Ugoni AM et al (1999) Age- and gender-specific rate of fractures in Australia: a population-based study. Osteoporos Int 10(3):240–247
Oinuma T, Sakuma M, Endo N (2010) Secular change of the incidence of four fracture types associated with senile osteoporosis in Sado, Japan: the results of a 3-year survey. J Bone Miner Metab 28(1):55–59
Bow CH, Cheung E, Cheung CL et al (2012) Ethnic difference of clinical vertebral fracture risk. Osteoporos Int 23(3):879–885
van Staa TP, Dennison EM, Leufkens HG, Cooper C (2001) Epidemiology of fractures in England and Wales. Bone 29(6):517–522
Bassgen K, Westphal T, Haar P, Kundt G, Mittlmeier T, Schober HC (2013) Population-based prospective study on the incidence of osteoporosis-associated fractures in a German population of 200,413 inhabitants. Journal of public health 35(2):255–261
Piscitelli P, Tarantino U, Chitano G et al (2011) Updated incidence rates of fragility fractures in Italy: extension study 2002-2008. Clinical cases in mineral and bone metabolism: the official journal of the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases 8(3):54–61
Lippuner K, Johansson H, Kanis JA, Rizzoli R (2009) Remaining lifetime and absolute 10-year probabilities of osteoporotic fracture in Swiss men and women. Osteoporos Int 20(7):1131–1140
Siggeirsdottir K, Aspelund T, Jonsson BY et al Epidemiology of fractures in Iceland and secular trends in major osteoporotic fractures 1989-2008. Osteoporos Int:2013
Dzajkovska B, Wertheimer AI, Mrhar A (2007) The burden-of-illness study on osteoporosis in the Slovenian female population. Pharm World Sci 29(4):404–411
Hu R, Mustard CA, Burns C (1996) Epidemiology of incident spinal fracture in a complete population. Spine (Phila Pa 1976) 21(4):492–499
Melton LJ 3rd, Crowson CS, O’Fallon WM (1999) Fracture incidence in Olmsted County, Minnesota: comparison of urban with rural rates and changes in urban rates over time. Osteoporos Int 9(1):29–37
Amin S, Achenbach SJ, Atkinson EJ, Khosla S, Melton LJ 3rd (2013) Trends in fracture incidence: a population-based study over 20 years. J Bone Miner Res
Lee YK, Jang S, Jang S et al (2012) Mortality after vertebral fracture in Korea: analysis of the National Claim Registry. Osteoporosis international: a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA 23(7):1859–1865
Johnell O, Gullberg B, Kanis JA (1997) The hospital burden of vertebral fracture in Europe: a study of national register sources. Osteoporos Int 7(2):138–144
Jansson KA, Blomqvist P, Svedmark P et al (2010) Thoracolumbar vertebral fractures in Sweden: an analysis of 13,496 patients admitted to hospital. Eur J Epidemiol 25(6):431–437
Bouza C, Lopez T, Palma M, Amate JM (2007) Hospitalised osteoporotic vertebral fractures in Spain: analysis of the national hospital discharge registry. Osteoporos Int 18(5):649–657
Jacobsen SJ, Cooper C, Gottlieb MS, Goldberg J, Yahnke DP, Melton LJ 3rd (1992) Hospitalization with vertebral fracture among the aged: a national population-based study, 1986-1989. Epidemiology 3(6):515–518
Cummings SR, Melton LJ (2002) Epidemiology and outcomes of osteoporotic fractures. Lancet 359(9319):1761–1767
Cooper C, Cole ZA, Holroyd CR et al (2011) Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos Int 22(5):1277–1288
Parisien M, Cosman F, Morgan D et al (1997) Histomorphometric assessment of bone mass, structure, and remodeling: a comparison between healthy black and white premenopausal women. J Bone Miner Res Off J Am Soc Bone Miner Res 12(6):948–957
Qiu S, Rao DS, Palnitkar S, Parfitt AM (2006) Differences in osteocyte and lacunar density between black and white American women. Bone 38(1):130–135
Schousboe JT (2015) Epidemiology of Vertebral Fractures. Journal of clinical densitometry: the official journal of the International Society for Clinical Densitometry
Cauley JA, Chalhoub D, Kassem AM, Fuleihan Gel H (2014) Geographic and ethnic disparities in osteoporotic fractures. Nat Rev Endocrinol 10(6):338–351
Cooper C, Atkinson EJ, Kotowicz M, O’Fallon WM, Melton LJ 3rd (1992) Secular trends in the incidence of postmenopausal vertebral fractures. Calcif Tissue Int 51(2):100–104
Leslie WD, Sadatsafavi M, Lix LM et al (2011) Secular decreases in fracture rates 1986-2006 for Manitoba, Canada: a population-based analysis. Osteoporos Int 22(7):2137–2143
Acknowledgments
Special thanks to Ms. Aida Farha, Medical Information Specialist, Saab Medical Library, American University of Beirut, for her advice and assistance in designing comprehensive and complex searches of the various medical literature resources, and provision of selected articles. The authors also thank Mr. Ali Hammoudi for his help with the tables and figures.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Electronic supplementary material
ESM 1
(DOCX 32 kb)
ESM 2
(DOCX 61 kb)
ESM 3
(DOCX 45 kb)
Appendix 4
Fig. Age-specific incidence rates for vertebral fractures in men and women worldwide. (JPEG 608 kb)
Rights and permissions
About this article

Cite this article
Ballane, G., Cauley, J.A., Luckey, M.M. et al. Worldwide prevalence and incidence of osteoporotic vertebral fractures. Osteoporos Int 28, 1531–1542 (2017). https://doi.org/10.1007/s00198-017-3909-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-017-3909-3