
Abstract
Introduction and hypothesis
Urinary incontinence is common among older adults with chronic conditions. The purpose of this study is to examine the association of urinary incontinence with chronic conditions in the US population.
Methods
We used data from the 2001–2014 National Health and Nutrition Examination Survey; 7226 women and 7239 men age > 50 years answered questions regarding urinary symptoms. The analysis accounted for the complex survey design, and prevalence reflects estimates within the non-institutionalized US population.
Results
The mean age was 64.2 years [standard error (SE) 0.2] among women and 62.9 (SE 0.1) years among men. Bothersome stress, urgency and mixed incontinence were reported by 6.7% (SE 0.4), 4.8% (SE 0.4) and 19.3% (SE 0.59) of women, respectively, and 0.6% (SE 0.1), 3.5% (SE 0.2) and 1.9% (SE 0.2) of men, respectively. Among chronic conditions, heart failure was associated with higher prevalence of mixed incontinence in women and urgency incontinence in men. Among women, heart failure was associated with significantly increased odds of bothersome mixed incontinence (OR 2.35; 95% CI 1.62, 3.42) and lower odds of stress (OR 0.50; 95% CI 0.3, 0.9) or urgency incontinence (OR 0.43; 95% CI 0.19, 0.98) after adjustment for covariates. Among men, heart failure was associated with higher odds of stress (OR 1.99; 95% CI 0.39, 10.22), urgency (1.65; 95% CI 0.91, 2.99) and mixed incontinence (OR 1.54; 95% CI 0.91, 2.62) but associations were not statistically significant.
Conclusions
Heart failure is associated with higher odds of bothersome incontinence, especially among women.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
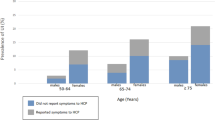
Urinary incontinence is a common and burdensome condition that affects 25–45% of older women and 11–34% of older men [1,2,3,4]. Because the US population is aging, the economic burden of urgency incontinence alone is projected to exceed 86 billion dollars within the next few years with most costs incurred by patients [5]. Primary care and other providers may not be aware of a patient’s incontinence symptoms because of either lack of reporting by the patient or lack of screening by the provider [6]. If urinary symptoms such as incontinence are never discussed, then patients will never receive counseling or interventions. In addition, incontinence can potentially interfere with self-management of chronic conditions that require diuretics such as heart failure, hypertension and chronic kidney disease (CKD). Incontinence is also associated with need for assistance in daily needs and unmet care needs [7]. Thus, identifying issues of incontinence in patients may help discern need for better social support to improve self-management.
Previous studies have found associations of urinary incontinence with several chronic conditions, including type 2 diabetes [2, 8] and obesity [2, 9]. However, information on the association of incontinence with chronic conditions such as hypertension, heart failure or CKD remains limited. These chronic conditions are often treated with diuretics and/or beta-blockers, both of which may exacerbate lower urinary tract symptoms [10, 11]. In addition, the prevalence of these conditions is increasing because of the aging of the US population.
We used data from a nationally representative sample of the US population to examine the prevalence of incontinence among adults age > 50 years by presence of chronic conditions. We also examined the association of incontinence with use of diuretics and beta-blockers, drugs commonly used to treat cardiovascular and kidney diseases. We hypothesized that incontinence prevalence is higher among older adults with chronic conditions.
Methods
Study population
We used data from the 2001–2014 National Health and Nutrition Examination Survey, a probability sample of the civilian non-institutionalized US population age > 2 months. Details of the survey design can be found in the NHANES operation manual [12]. In total, 72,216 individuals were surveyed between 2001 and 2014. Because incontinence and cardiovascular disease (CVD) and other chronic conditions are uncommon among younger adults, we limited our analyses to the 18,874 NHANES participants who were ≥ 50 years of age. Because the sample size for “other” race/ethnicity was small, our analyses included participants who reported their race as non-Hispanic white, non-Hispanic black or Mexican-American (n = 16,348). Our sample population excluded NHANES participants who did not answer questions regarding urinary incontinence (n = 1525) or had a sample weight < zero (n = 358). In the final analysis set, 7226 respondents were women and 7239 were men.
Chronic conditions
Medical history was collected during the interview by trained personnel using standardized questionnaires. Hypertension was defined as blood pressure > 140/90 mmHg and/or use of antihypertensive medications. Fasting blood samples were collected from all participants and measured for serum creatinine. CKD was defined as presence of an estimated glomerular filtration rate < 60 ml/min/1.73 m2 based on measured serum creatinine value using the CKD-Epi equation [13]. Heart failure was defined as the respondent answering “Yes” to the question, “Have you ever been told by a physician that you had heart failure?” CVD was defined as the participant self-reporting a previous physician diagnosis of angina, coronary artery disease or myocardial infarction. Diabetes mellitus was defined as the respondent self-reporting a previous physician diagnosis of diabetes mellitus (except during pregnancy) or if the respondent had a history of taking insulin or other glucose-lowering medications. A history of prostate cancer was based on the self-report of a physician diagnosis of prostate cancer.
Incontinence
During the interview, study participants answered standardized questions which were administered in English or Spanish by trained personnel. Presence of stress incontinence was defined as responding “Yes” to the question, “During the past 12 months, have you leaked or lost control of even a small amount of urine with an activity like coughing?” and absence of urgency incontinence. Presence of urgency incontinence was defined as responding “Yes” to the question, “During the past 12 months have you leaked or lost control of even a small amount of urine with an urge or pressure to urinate and you could not get to the toilet fast enough?” and absence of stress incontinence. Mixed incontinence was defined as a “Yes” response to questions on stress and urgency incontinence. Incontinence was determined to be bothersome if the participant rated any involuntary leakage of urine, regardless of its frequency, as being “somewhat,” “very much” or “greatly” bothersome.
Covariates
Age was defined as the age at the time of the interview. Race/ethnicity data were based on self-report. Body mass index in kg/m2 was calculated from the weight and height measured during physical examination at the mobile survey center. Parity data were collected during the standardized interview. Participants were asked to bring all prescription medications taken in the past 2 weeks to their NHANES medical evaluation. Medication names were then recorded by trained personnel and coded into medication classes according to their generic equivalents. See Table S1 in Supplemental Materials for a list of medications included in the analyses.
Statistical analysis
Statistical analyses were performed with SAS®-callable SUDAAN® software version 9.0. Sample weights were incorporated to calculate prevalence estimates that would reflect the entire non-institutionalized US population. NHANES 2001–2014 data are weighted to account for the probability of selection and to adjust for nonresponse to the interview and physical examination. Sex-specific multivariable logistic regression analyses were used to calculate odds of urinary incontinence by morbidity and medication use. Model 1 adjusted for age, race and body mass index as well as parity in women. Model 2 included model 1 and further adjusted for the use of diuretics and/or beta-blockers as well as estrogen in women and alpha-blockers for treatment of benign prostatic hyperplasia in men. Model 3 included model 2 and further adjusted for the concurrent presence of hypertension, CKD, heart failure, CVD, diabetes mellitus and/or prostate cancer (men).
Results
Table 1 shows the characteristics of the study population. Race/ethnicity was reported as non-Hispanic white in 85.3% of women and 85.7% of men, non-Hispanic black in 9.3% of women and 10.1% of men, and Mexican-American in 4.9% of women and 5.1% of men. Mean age was 64.2 years [standard error (SE) 0.2] in women and 62.9 years (SE 0.1) in men while mean body mass index was 29.3 kg/m2 (SE 0.1) in women and 29.0 kg/m2 (SE 0.1) in men. The percentage of men and women age ≥ 80 years was 2.9% (SE 0.2) and 4.4% (SE 0.3), respectively. CKD, congestive heart failure and CVD were present in 19.1% (SE 0.6), 4.9% (SE 0.3) and 13.1% (SE 0.6) of women, respectively, and 14.3% (SE 0.5), 5.6% (0.4) and 19.1% (0.6) of men, respectively. Diuretic use was reported by 23.4% (SE 0.7) of the women and 17.0% (SE 0.6) of men. Beta-blocker use was documented by 18.9% (SE 0.7) of both men and women. Overall, 6.6% (SE 0.4) of women reported estrogen use while 9.6% (SE 0.4) of men reported use of alpha-blockers for benign prostatic hyperplasia. Prevalence of stress, urgency and mixed incontinence, regardless of bother, was reported by 26.8% (SE 0.7), 14.4% (SE 0.6) and 23.9% (SE 0.6) of women, respectively, and 2.9% (SE 0.3), 15.2% (SE 0.5) and 4.6% (SE 0.3) of men, respectively. Prevalence estimates of bothersome incontinence for all types were lower in men than women (see Table 2). Supplemental Table 2 shows the prevalence of bothersome incontinence by incontinence type among women and men across age and BMI groups. For both men and women, bothersome incontinence generally increased with advancing age and with higher BMI except for bothersome female stress incontinence prevalence, which was not age dependent.
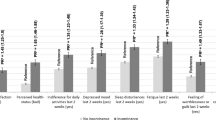
Population estimates of incontinence among the general non-institutionalized US population age > 50 years are shown in Table 2. In total, an estimated 9.6 million women and 2.2 million men age ≥ 50 years are affected by bothersome stress and/or urgency incontinence. Figures 1 and 2 show the difference in prevalence of bothersome incontinence among women and men, respectively, by presence of chronic conditions. Among both women and men, prevalence of mixed incontinence was generally higher with presence of a chronic condition such as diabetes, hypertension, heart failure and CVD. Significant differences in all types of bothersome incontinence were noted with presence of heart failure for both women and men. Small but significant differences in bothersome mixed incontinence prevalence were noted with use of diuretics or beta-blockers (Fig. 3) among women. However, after adjustment for age, BMI and chronic conditions, no significant association was noted with diuretics or beta-blockers and bothersome incontinence of any type among women or men (data not shown).

Differences in prevalence of bothersome incontinence by presence of chronic conditions among women age => 50 years. Prevalence of bothersome incontinence is shown in those witha and withoutb the chronic condition,respectively, and error bars represent 95% confidence interval in mean difference

Differences in prevalence of bothersome incontinence by presence of chronic conditions among men age => 50 years. Prevalence of bothersome incontinence is shown in those witha and withoutb the chronic condition, respectively, and error bars represent 95% confidence interval in mean difference

Mean difference in prevalence of bothersome incontinence by presence of medication use . Prevalence of bothersome incontinence is shown in those witha and withoutb medication use, respectively, and error bars represent 95% confidence interval in mean difference
The adjusted odds of bothersome incontinence for women and men by presence of a chronic condition are shown in Tables 3 and 4. Among women, no significant association was noted with hypertension, CKD, or CVD and bothersome stress, urgency or mixed incontinence. However, after adjustment for all covariates, heart failure was associated with significantly lower odds of both stress (OR 0.50; 95% CI 0.28, 0.91) and urgency (0.43; 95% CI 0.19, 0.98) incontinence, while both heart failure (OR 2.35; 95% CI 1.62, 3.42) and diabetes mellitus (OR 1.40; 95% CI 1.10, 1.77) were significantly associated with higher odds of mixed incontinence (Table 3). Among men, heart failure was associated with higher odds of stress (OR 1.99; 95% CI 0.39, 10.22) urgency (OR 1.65; 95% CI 0.91, 2.99) and mixed incontinence (OR 1.54; 95% CI 0.91, 2.62) but the 95% CI included 1.00. (Table 4). Prostate cancer history was associated with significantly higher odds of both stress incontinence (OR 22.54; 95% CI 7.85, 64.72) and mixed incontinence 3.04 (1.62, 5.68).
Discussion
Our analysis of a representative sample of the non-institutionalized US population age ≥ 50 years estimates that almost 10 million women and > 2 million men suffer from bothersome urgency or stress incontinence. Within the next 30 years, North America is expected to be the second oldest region on the globe with over 20% of the population age 65 years and older [16]. The aging of the population is compounded by an ongoing and unabated obesity epidemic [17], and obesity can increase intra-abdominal pressure, which may lead to chronic strain and weakening of the pelvic floor. Because incontinence risk increases with advancing age [2], and with obesity [2, 8, 14, 15], the population burden of incontinence will likely increase over the next several decades.
Advancing age and obesity are also strong risk factors for the development of multiple chronic conditions including diabetes mellitus, hypertension, CKD, CVD and heart failure [18]. This study shows generally higher prevalence of bothersome mixed incontinence among women and bothersome urgency and mixed incontinence among men, with presence of these chronic conditions. Higher odds of bothersome mixed incontinence were noted with presence of heart failure, especially among women even after adjustment for age, body mass index and medication use. Very few studies have examined incontinence or other lower urinary tract symptoms in persons with heart failure [10, 19]. Some postulate that the heightened ventricular wall tension in heart failure leads to release of natriuretic peptides, which stimulate natriuresis and urge to urinate, similar to diuretics [10]. In addition, persons with heart failure may also be less active, leading to poor pelvic muscle function. Because incontinence depends to a degree on pelvic floor function [20], any chronic illness can lead to deconditioning of pelvic floor muscle tone. Medications such as diuretics and beta-blockers are another potential reason why patients with heart failure may be at higher risk of incontinence [10]. Diuretics may exacerbate incontinence by causing large volumes of urine to enter the bladder over a shorter time [11], which leads to more times that the bladder reaches maximal capacity. When the bladder volume reaches maximal capacity, urgency incontinence can be triggered in susceptible patients. Beta-adrenergic blocking drugs may cause or worsen urgency and mixed incontinence by increasing bladder contractility, leading to an increased sense of urinary urgency and urgency incontinence [10]. In our analyses, however, we found no significant association between use of diuretics or beta-blockers and prevalence of bothersome incontinence, which may be due to behavioral adaptations [21, 22].
We also found significant associations of incontinence with diabetes mellitus and bothersome mixed incontinence among women. The link between diabetes mellitus and incontinence is likely multi-factorial and includes increased urine volumes with glucosuria and, in more advanced diabetes, neuropathy, which may impair detrusor muscle contractility, leading to large postvoid residual volume, urinary retention and eventually overflow incontinence [23]. One recent study, however, found no association between presence of neuropathy and incontinence in patients with diabetes [8], and therefore the mechanism of this association remains unclear. History of treated prostate cancer was significantly associated with incontinence among men as shown in previous studies [24, 25].
Our study has several strengths. We analyzed a representative sample of the US population, and the analyses accounted for the complex survey design and non-response. Our analyses provide estimates of the number of US adults age 50 years and older who may suffer from incontinence. The weaknesses of the study include potential recall bias because prevalence estimates relied on self-reported incontinence, which is known to yield results that are somewhat different from those based on urodynamic evaluation [26]. The recall bias could lead to over- or underestimation of urinary symptoms, depending on the individual. However, self-report has the advantage of including the participant’s subjective assessment of “bother” associated with incontinence. Women and men may have differed in their reporting of leakage symptoms based on accepted cultural norms, potentially complicating comparison of incontinence between the sexes. Presence of chronic conditions was also based on self-report. Because of these limitations, the findings of this study need to be confirmed in other population studies.
In conclusion, our analysis further supports that urinary incontinence is a bothersome symptom that affects many US women and men age > 50 years. Older adults with chronic conditions, especially heart failure, may be more likely to have bothersome incontinence. The findings from this study require confirmation in other study populations but providers should be aware of the high prevalence of bothersome incontinence among older patients. Querying presence of urinary incontinence may help guide treatment of chronic conditions in some patients.
References
Dooley Y, Kenton K, Cao G, Luke A, Durazo-Arvizu R, Kramer H, et al. Urinary incontinence prevalence: results from the National Health and nutrition examination survey. J Urol. 2008;179:656–61.
Milson I, Altman D, Lapitan MC, Nelson R, Sillen U, Thom D. Epidemiology of urinary (UI) and faecal (FI) incontinence and pelvic organ prolape. In: Abrams P, Cardozo L, Khoury S, Wein A, editors. Incontinence. Paris, France: European Association of Urology; 2009. p. 35–111.
Markland AD, Richter HE, Fwu CW, Eggers P, Kusek JW. Prevalence and trends of urinary incontinence in adults in the United States, 2001 to 2008. J Urol. 2011;186:589–93.
(2008) Prevalence of and risk factors for urine leakage in a racially and ethnically diverse population of adults: the Boston Area Community Health (BACH) Survey. Am J Epidemiol 167:390–399.
Coyne KS, Wein A, Nicholson S, Kvasz M, Chen CI, Milsom I. Economic burden of urgency urinary incontinence in the United States: a systematic review. J Manag Care Pharm. 2014;20:130–40.
Dugan E, Roberts CP, Cohen SJ, Preisser JS, Davis CC, Bland DR, et al. Why older community-dwelling adults do not discuss urinary incontinence with their primary care physicians. J Am Geriatr Soc. 2001;49:462–5.
Yang E, Lisha NE, Walter L, Obedin-Maliver J, Huang AJ. Urinary incontinence in a National Cohort of older women: implications for caregiving and care dependence. J Women's Health (Larchmt). 2018;27:1097–103.
Phelan S, Kanaya AM, Subak LL, Hogan PE, Espeland MA, Wing RR, et al. Prevalence and risk factors for urinary incontinence in overweight and obese diabetic women: action for health in diabetes (look ahead) study. Diabetes Care. 2009;32:1391–7.
(2006) Prevalence of lower urinary tract symptoms and effect on quality of life in a racially and ethnically diverse random sample: the Boston Area Community Health (BACH) Survey. Arch Intern Med 166:2381–2387.
Tannenbaum C, Johnell K. Managing therapeutic competition in patients with heart failure, lower urinary tract symptoms and incontinence. Drugs Aging. 2014;31:93–101.
Tsakiris P, Oelke M, Michel MC. Drug-induced urinary incontinence. Drugs Aging. 2008;25:541–9.
Zipf G, Chiappa M, Porter KS, Ostchega Y, Lewis BG, Dostal J. National health and nutrition examination survey: plan and operations, 1999-2010. Vital Health Stat. 2013;1(56):1–37.
Inker LA, Schmid CH, Tighiouart H, Eckfeldt JH, Feldman HI, Greene T, et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012;367:20–9.
Tsui A, Kuh D, Cardozo L, Davis D. Vascular risk factors for male and female urgency urinary incontinence at age 68 years from a British birth cohort study. BJU Int. 2018;122:118–25.
Coyne KS, Wein A, Nicholson S, Kvasz M, Chen CI, Milsom I. Comorbidities and personal burden of urgency urinary incontinence: a systematic review. Int J Clin Pract. 2013;67:1015–33.
Roberts AW, Ogunwole SU, Blakeslee L, Rabe MA (2018) The population 65 years and older in the United States: 2016. Economics and statistics administration. US Census Bureau. https://www.census.gov/content/dam/Census/library/publications/2018/acs/ACS-38.pdf accessed may 15, 2019. American community survey reports ACS-38.
Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL. Trends in obesity among adults in the United States, 2005 to 2014. JAMA. 2016;315:2284–91.
Bhupathiraju SN, Hu FB. Epidemiology of obesity and diabetes and their cardiovascular complications. Circ Res. 2016;118:1723–35.
Hwang R, Chuan F, Peters R, Kuys S. Frequency of urinary incontinence in people with chronic heart failure. Heart Lung. 2013;42:26–31.
Nie XF, Ouyang YQ, Wang L, Redding SR. A meta-analysis of pelvic floor muscle training for the treatment of urinary incontinence. Int J Gynaecol Obstet. 2017;138:250–5.
Diokno AC, Burgio K, Fultz NH, Kinchen KS, Obenchain R, Bump RC. Medical and self-care practices reported by women with urinary incontinence. Am J Manag Care. 2004;10:69–78.
Mitteness LS. The management of urinary incontinence by community-living elderly. Gerontologist. 1987;27:185–93.
DuBeau CE. Interpreting the effect of common medical conditions on voiding dysfunction in the elderly. Urol Clin North Am. 1996;23:11–8.
Potosky AL, Legler J, Albertsen PC, Stanford JL, Gilliland FD, Hamilton AS, et al. Health outcomes after prostatectomy or radiotherapy for prostate cancer: results from the prostate cancer outcomes study. J Natl Cancer Inst. 2000;92:1582–92.
Chen RC, Basak R, Meyer AM, Kuo TM, Carpenter WR, Agans RP, et al. Association between choice of radical prostatectomy, external beam radiotherapy, brachytherapy, or active surveillance and patient-reported quality of life among men with localized prostate cancer. JAMA. 2017;317:1141–50.
Sandvik H, Hunskaar S, Vanvik A, Bratt H, Seim A, Hermstad R. Diagnostic classification of female urinary incontinence: an epidemiological survey corrected for validity. J Clin Epidemiol. 1995;48:339–43.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors report no conflicts of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 26 kb)
Rights and permissions
About this article

Cite this article
Daugirdas, S.P., Markossian, T., Mueller, E.R. et al. Urinary incontinence and chronic conditions in the US population age 50 years and older. Int Urogynecol J 31, 1013–1020 (2020). https://doi.org/10.1007/s00192-019-04137-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-019-04137-y