
Abstract
Introduction and hypothesis
The mechanism of continence in women with pelvic organ prolapse (POP) before and after surgery remains unknown. Urethral pressure reflectometry (UPR) separates women with stress urinary incontinence (SUI) from continent women by measuring urethral opening pressure at an abdominal pressure of 50 cmH2O (P O-Abd 50). UPR can help identify women with POP at risk of postoperative de novo SUI. The aim of this study was to investigate the reproducibility of UPR in women with POP.
Methods
Women with anterior or posterior vaginal wall prolapse were recruited for this prospective, observational study from our outpatient clinic. The women were examined with UPR on two occasions. Measurements were done at rest, and during squeezing and straining. Statistical analyses were performed using SAS 9.4. A Bland-Altman analysis with limits of agreement and coefficients of variation was used to determine the level of agreement between measurements. Paired t tests were used to estimate the difference; a two-tailed P value of <0.05 was considered significant.
Results
We recruited 19 women with anterior vaginal wall prolapse and 11 women with posterior vaginal wall prolapse. There were no significant differences in the opening pressures at rest or during squeezing or in the values of P O-Abd 50. P O-Abd 50 showed limits of agreement of 15.3 cmH2O and a coefficient of variation of 9.9 %.
Conclusions
UPR was found to be a highly reproducible method in women with POP. UPR may be used in future studies to help reveal urodynamic features predictive of postoperative de novo SUI in women with POP.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The relationship between stress urinary incontinence (SUI) and pelvic organ prolapse (POP) is complex and not fully understood. Some women with concomitant SUI and POP find that their incontinence resolves after prolapse surgery whilst others require further treatment. De novo SUI is a known risk of POP surgery and studies have shown that postoperative de novo SUI ranges from 11 % to 44 % [1–5]. There are different theories as to why de novo SUI occurs. In patients with anterior vaginal wall prolapse the sunken bladder may mask SUI by kinking and/or compressing the urethra. Subsequently, when the bladder is repositioned during surgery, the kinking and/or compression is eliminated [6]. De novo SUI is often associated with anterior vaginal wall prolapse. However, it may be just as prevalent after surgery for posterior vaginal wall prolapse: the posterior wall is believed to compress the anterior vaginal wall, thereby compressing the urethra [7, 8]. Preoperative occult SUI, the presence of leakage on POP reduction [9] during a stress test, has been accepted as an indicator of de novo SUI. However, POP reduction tests are not reliable due to disappointing predictive values [1, 10, 11]. In addition, the association between preoperative occult SUI and postoperative de novo SUI at the individual level has been questioned [10]. This raises doubt as to the applicability of the test results when counselling patients. However, some argue that whether or not a woman has preoperative occult incontinence is indicative of whether or not she should undergo prophylactic anti-incontinence surgery at the time of POP repair. This controversial topic is an ongoing subject of debate.
There is a great need for knowledge regarding the mechanism of continence, or rather incontinence, in women with POP before and after surgery. Saaby et al. [12] were able to separate women with SUI from continent women by measuring urethral opening pressure at an abdominal pressure of 50 cmH2O by means of urethral pressure reflectometry (UPR) [13]. Measurement during straining provides an assessment of both the permanent and adjunctive closure forces that act on the urethra. The authors suggested that UPR might be used as a diagnostic test for SUI. Thus, UPR could possibly reveal the mechanism of SUI in women with POP. Since UPR has not been used in this specific population, the aim of this study was to investigate the reproducibility of UPR at rest, and during squeezing and straining, in women with POP.
Materials and methods
We conducted a prospective, observational study at the Department of Obstetrics and Gynecology, Herlev University Hospital, Denmark. Women with anterior or posterior vaginal wall prolapse were approached in the outpatient clinic from November 2013 to November 2015. Two groups of women were recruited according to the following criteria:
-
Group 1: Women with anterior vaginal wall prolapse of grade 2 or more:
-
With or without apical vaginal wall prolapse
-
Who were scheduled for anterior colporrhaphy with or without concomitant cervical amputation
-
With no concomitant posterior vaginal wall prolapse of grade 2 or more
-
-
Group 2: Women with posterior vaginal wall prolapse of grade 2 or more:
-
Who were scheduled for posterior colporrhaphy with or without concomitant perineorrhaphy
-
With no concomitant vaginal wall prolapse of grade 2 or more in any other compartment
-
The women were excluded if they had a history of previous surgery for POP or SUI or hysterectomy, had a neurological disease, used any antimuscarinic drugs, mirabegron or any other medicine for urinary incontinence, were pregnant, were under the age of 18 years, were unable to give their informed consent, or were not fluent in Danish, Swedish, Norwegian or English.
The assessments included two preoperative examinations on different occasions. At the first appointment, the woman were examined in the supine position and POP staging was performed according to the Pelvic Organ Prolapse Quantification (POP-Q) system. The woman was instructed to relax so that any bulging POP would be repositioned. Subsequently, the bladder was emptied with a CH 10 SpeediCath and then UPR measurements were obtained. After the measurements had been obtained, the bladder, was emptied and a standardized stress test was performed with 300 ml saline or up to maximum bladder capacity using a CH 10 SpeediCath. The woman, who was in the supine position, was instructed to cough vigorously three times. The entire examination was conducted without POP reduction. The second appointment was identical to the first one, with the exception that POP staging was omitted. The lead author of this paper (Y.K.) and a study nurse conducted all assessments.
What is UPR?
UPR allows simultaneous measurement of the pressure in the urethra and its cross-sectional area. A polyurethane bag connected to a 45 cm long PVC tube, is inserted into the urethra using a CH 5 baby feeding tube. The bag is fixed to the external urethral meatus with a DuoDERM dressing. The tube is connected to a probe (containing a microphone and a loudspeaker) which in turn is connected to a 12-ml syringe and a computer with an integrated pressure recorder. The syringe pumps air into the polyurethane bag to increase the pressure and distend the bag, thereby opening the urethra. The cross-sectional area along the entire length of the urethra is measured continuously by means of acoustic reflectometry. However, only measurements from the high-pressure zone are evaluated, as this is the section of the urethra with the smallest cross-sectional area at a given pressure. As a result, the opening pressure, which is the pressure needed to open the collapsed urethra, is measured. Pressures between 0 and 200 cmH2O and cross-sectional areas between 0.4 and 16 mm2 are measured.
The measurements
Abdominal pressure was measured with an air-filled balloon catheter placed in the rectum (T-Doc, Wenonah, NJ). Pressures were recorded in UDS120 Goby, which synchronized recordings of UPR and abdominal pressures throughout the entire measurement. Measurements were obtained at rest, during squeezing and during straining, as follows:
-
At rest (P O-Rest): Ten consecutive measurements were obtained. The woman was asked to relax, the pressure in the polyurethane bag was increased until the bag, and thereby urethra, was fully dilated, and then the pressure was decreased, all within 14 s. Abdominal pressure was recorded continuously. The mean of the ten measurements was calculated.
-
During squeezing (P O-Squeeze): Five consecutive measurements were obtained. Each time, the woman was asked to squeeze and hold the tension for 7 s. The pressure in the polyurethane bag was increased until the bag was fully dilated. The woman was then asked to relax, and the polyurethane bag was deflated. Abdominal pressure was recorded continuously. The mean of the five measurements was calculated.
-
During straining: The woman was asked to increase the abdominal pressure by straining ten times at different intensities to ensure a wide variety of abdominal pressures. The woman was asked to hold the pressure as evenly as possible for 7 s. The pressure in the polyurethane bag was increased until the bag was fully dilated. The woman was then asked to relax and the polyurethane bag was deflated. Abdominal pressure was recorded continuously.
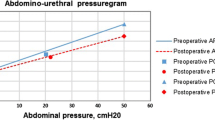
The related values of urethral and abdominal pressures were plotted as an abdominourethral pressuregram (Fig. 1). Using linear regression (y = ax + b), the slope of the line and the intercept on the y-axis were calculated. The slope represents the effect of increasing abdominal pressure on urethral pressure, Saaby et al. called the slope ‘abdominal to urethral pressure impact ratio’ (APIR) [12]. Using APIR enables the opening pressure at any given abdominal pressure to be calculated. Measurements during straining were ultimately evaluated by assessing the reproducibility of both APIR and the opening pressure at a standardized abdominal pressure of 50 cmH2O (P O-Abd 50).

Abdominourethral pressuregram with opening pressures plotted against abdominal pressures. Abdominal to urethral pressure impact ratios and opening pressures at standardized abdominal pressures can be derived from this graph. The patient will become incontinent if the abdominal pressure exceeds the urethral pressure. The data were obtained from a study patient with SUI; her P O-Abd 50 was 54 cmH2O (P O-Abd 50 opening pressure at an abdominal pressure of 50 cmH2O
Ethics
The National Committee on Health Research Ethics and the Danish Data Protection Agency approved the study (project-ID: H-4-2013-069) and all study participants gave their written consent. The study was registered at ClinicalTrials.gov (NCT02050568).
Statistics
All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC). Data are presented as means or medians depending on distributions. Bland-Altman plots with limits of agreement and coefficients of variation were used to show the level of agreement between two measurements. The coefficient of variation (CV) is the standard deviation (SD) of the difference between measurements divided by the mean of the measurements and multiplied by 100. Paired t tests were used to estimate the significance of the differences (bias) between first and second measurements; a two-tailed P value < 0.05 was considered significant.
Results
A total of 30 women were recruited and examined twice for this study. In one woman, abdominal pressure was inaccurately measured during straining (probably due to a defect in the rectal balloon-catheter). This woman’s measurements during straining were excluded and her measurements at rest and during squeezing were included in the subsequent analyses. Table 1 shows the characteristics of the women. The study group comprised 19 women with anterior vaginal wall prolapse (3 with grade 2 and 16 with grade 3) and 11 women with posterior vaginal wall prolapse (9 with grade 2 and 2 with grade 3; Table 2).
Table 3 shows the reproducibility of the four parameters investigated; the results are presented for the total study group and separately for the two groups (anterior and posterior vaginal wall prolapse). There were no significant differences in the measurements between the two examinations; the opening pressures at rest, during squeezing and P O-Abd 50 were reproducible. Figure 2 shows a Bland-Altman plot for P O-Abd 50. APIR revealed large SD and CV. Measurements in the women with posterior vaginal wall prolapse showed slightly narrower limits of agreement and CVs for all parameters except P O-Abd 50. There were, however, no significant differences in the measurements between the women with anterior and posterior vaginal prolapse.

Bland-Altman plot showing the bias and the limits of agreement (2 × SD) for P O-Abd 50. The dashed line represents the bias (difference) and the solid lines represent the limits of agreement
The urethral profiles obtained during UPR indicated no signs of kinking of the urethra. In four women the first stress test was positive, and in three (75 %) of these women the second test was also positive, and in one the results of the second test were missing. In 25 women the first stress test was negative, and in 19 (76 %) of these women the second test was also negative, in 5 (20 %) the second test was positive, and in one the results of the second test were missing. In one woman the results of the first stress test were missing and the second test was negative. Of the 27 women with two stress tests, 17 had anterior vaginal prolapse and 10 had posterior vaginal prolapse. In 82 % of the women with anterior vaginal prolapse and in 80 % of the women with posterior vaginal prolapse the results of the two stress tests were the same.
Discussion
This is the first study of UPR in women with POP, and the results showed that the method is highly reproducible. Opening pressures were measured in the urethra under different conditions: at rest, during squeezing and during different degrees of straining. Measurements at rest and during squeezing were highly reproducible, as expected from the findings of a previous study [14] investigating the reproducibility of UPR in 17 women with SUI. The limits of agreement and CV for opening pressure at rest were, respectively, 8.9 and 8.9 % in the previous study and 11.7 and 11.3 % in the present study, and for squeezing were 13.3 and 11.0 % in the previous study and 13.3 and 10.2 % in the present study. The UPR procedure has been modified since publication of the study by Klarskov and Lose in 2007 [14], which makes comparing SDs and limits of agreement difficult. However, since CV is independent of the measurement itself and simply explains a relationship between SDs and mean values, it can be used to compare studies despite methodological differences. Therefore, in this study we confirmed the findings of Klarskov and Lose.
Measurements during straining were evaluated by assessing the reproducibility of APIR and P O-Abd 50, which has not been done in previous studies. P O-Abd 50 was highly reproducible with a narrow SD and a confirming CV. APIR had a large SD and high CV, making it difficult to apply in patients. However, separate analyses of the two groups of women (anterior and posterior vaginal wall prolapse) revealed narrower SDs and lower CVs in almost all parameters in women with posterior vaginal wall prolapse, which can be explained by the fact that the effect of POP on the urethra depends on its anatomical location. APIR expresses the relationship between urethral pressure and increasing abdominal pressure, and can be compared with pressure transmission ratio (PTR). PTR has been shown to have poor reproducibility in women without POP with SDs ranging from 13.0 to 18.5 and a CV of 19.8 % [15]. It is plausible that APIR is more reproducible in women without POP, but this remains to be investigated.
Leak point pressure (LPP) is the abdominal pressure at which urine leakage occurs, and can be used as a measure of the severity of incontinence. There are few studies on the reproducibility of LPP so that definitive conclusions cannot be drawn [16]. In addition, the parameter can be measured in several different ways as there is no standardized method, which makes any comparison of results difficult, if not impossible [16–18]. LPP can only be measured in patients with incontinence, and therefore it does not assess urethral function per se. Since P O-Abd 50 is the opening pressure at an abdominal pressure of 50 cmH2O, it can also be considered a measure of the severity of incontinence. The parameter represents the permanent and adjunctive closure forces that act on the urethra to keep it closed during stress, and so it evaluates urethral function regardless of the patient’s diagnosis. Since UPR is a standardized method, the parameters are measured under the same conditions every time. The sensitivity and specificity of P O-Abd 50 remain to be investigated in future studies.
Since UPR provides measurements along the entire length of the urethra, it provides a profile of the entire structure revealing the presence of kinking. Thorough analysis of every profile revealed no signs of kinking, supporting the theory that POP compresses the urethra. However, this needs further investigation in women before and after POP surgery.
Saaby et al. [12] found that women with SUI had a P O-Rest of 40 cmH2O in, a P O-Abd 50 of 67 cmH2O, and an APIR of 0.72. Continent women had corresponding values of 68 cmH2O, 104 cmH2O and 1.05, respectively. The corresponding values in our study group, which consisted of women with POP but mainly without objective SUI, were higher than in women with SUI and lower than in continent women.
We found 80 % consistency in the results of the two stress tests performed at the two visits. To our knowledge, no previous study has investigated the test–retest reliability of the stress test in women with POP. Swift et al. reported 90 % consistency in women with genuine SUI, and 80 % in women with mixed urinary incontinence [19].
POP is a condition that affects a woman’s everyday life. Any treatment should lead to an improvement in quality of life, and not the opposite. Therefore, some argue that POP surgery in women with occult SUI should be performed with simultaneous anti-incontinence surgery. Unfortunately, there is no absolute answer to this dilemma since studies have shown different results [2, 3, 20]. However, no surgical procedure is without risks. Women who undergo anti-incontinence surgery are at risk of developing postoperative complications such as urinary retention, voiding dysfunction, urinary tract infection, bladder perforation, bleeding and pain [21, 22]. No urodynamic test has proven to be valid for assessing the individual risk of postoperative de novo SUI in these women [10, 11]. The most common test is the stress test which aims to reveal the presence of occult SUI. The stress test is not a standardized test and repositioning may be done with, for example, a speculum or a pessary, with the patient in the supine or standing position. The test has been shown to be reproducible in women with urinary incontinence [23], but to the best of our knowledge, there have been no studies investigating the reproducibility of stress tests in women with POP. However, studies have shown that even with occult SUI in the preoperative assessment, a woman will not necessarily develop de novo SUI postoperatively, let alone de novo SUI that will require surgical treatment [3, 10]. A study investigating changes in PTR before and after repositioning of POP in 19 women [24] showed a decrease in PTR after repositioning which was greater in the women who had a positive stress test. Unfortunately, only the mean PTRs are reported, and not the SDs in the groups, which makes it difficult to apply the results in individual women.
There is a great need for knowledge as to how best to evaluate and treat women with POP. P O-Abd 50 is highly reproducible and therefore a reliable parameter in the assessment of women with or without POP, and it can separate continent women from women with SUI [12]. This study has paved the way for the use of UPR in women with POP. Future studies can now investigate if UPR can help unveil any urodynamic characteristics in women with POP that could predict their risk of postoperative de novo SUI.
References
Ellström Engh AM, Ekeryd A, Magnusson Å, Olsson I, Otterlind L, Tobiasson G. Can de novo stress incontinence after anterior wall repair be predicted? Acta Obstet Gynecol Scand. 2011;90(5):488–493.
Lensen EJ, Withagen MI, Kluivers KB, Milani AL, Vierhout ME. Urinary incontinence after surgery for pelvic organ prolapse. Neurourol Urodyn. 2013;32(5):455–459.
Ennemoser S, Schönfeld M, von Bodungen V, Dian D, Friese K, Jundt K. Clinical relevance of occult stress urinary incontinence (OSUI) following vaginal prolapse surgery: long-term follow-up. Int Urogynecol J. 2012;23(7):851–855.
Kuribayashi M, Kitagawa Y, Narimoto K, Urata S, Kawaguchi S, Namiki M. Predictor of de novo stress urinary incontinence following TVM procedure: a further analysis of preoperative voiding function. Int Urogynecol J. 2013;24(3):407–411.
Brubaker L, Cundiff GW, Fine P, Nygaard I, Richter HE, Visco AG, et al. Abdominal sacrocolpopexy with Burch colposuspension to reduce urinary stress incontinence. N Engl J Med. 2006;354(15):1557–1566.
Marinkovic SP, Stanton SL. Incontinence and voiding difficulties associated with prolapse. J Urol. 2004;171(3):1021–1028.
Mouritsen L, Larsen JP. Symptoms, bother and POPQ in women referred with pelvic organ prolapse. Int Urogynecol J Pelvic Floor Dysfunct. 2003;14(2):122–127.
Myers DL, Lasala CA, Hogan JW, Rosenblatt PL. The effect of posterior wall support defects on urodynamic indices in stress urinary incontinence. Obstet Gynecol. 1998;91(5 Pt 1):710–714.
Haylen BT, Maher CF, Barber MD, Camargo S, Dandolu V, Digesu A, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic organ prolapse (POP). Int Urogynecol J. 2016;27(2):165–194.
Svenningsen R, Borstad E, Spydslaug AE, Sandvik L, Staff AC. Occult incontinence as predictor for postoperative stress urinary incontinence following pelvic organ prolapse surgery. Int Urogynecol J. 2012;23(7):843–849.
Visco AG, Brubaker L, Nygaard I, Richter HE, Cundiff G, Fine P, et al. The role of preoperative urodynamic testing in stress-continent women undergoing sacrocolpopexy: the Colpopexy and Urinary Reduction Efforts (CARE) randomized surgical trial. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(5):607–614.
Saaby M-L, Klarskov N, Lose G. Urethral pressure reflectometry during intra-abdominal pressure increase – an improved technique to characterize the urethral closure function in continent and stress urinary incontinent women. Neurourol Urodyn. 2013;32(8):1103–1108.
Klarskov N. Urethral pressure reflectometry. A method for simultaneous measurements of pressure and cross-sectional area in the female urethra. Dan Med J. 2012;59(3):B4412.
Klarskov N, Lose G. Urethral pressure reflectometry vs urethral pressure profilometry in women: a comparative study of reproducibility and accuracy. BJU Int. 2007;100(2):351–356.
Weber AM. Is urethral pressure profilometry a useful diagnostic test for stress urinary incontinence? Obstet Gynecol Surv. 2001;56(11):720–735.
Weber AM. Leak point pressure measurement and stress urinary incontinence. Curr Womens Health Rep. 2001;1(1):45–52.
Siltberg H, Larsson G, Victor A. Cough-induced leak-point pressure – a valid measure for assessing treatment in women with stress incontinence. Acta Obstet Gynecol Scand. 1998;77(10):1000–1007.
McLennan MT, Melick CF, Bent AE. Leak-point pressure: clinical application of values at two different volumes. Int Urogynecol J. 2000;11(3):136–141.
Swift SE, Yoon EA. Test-retest reliability of the cough stress test in the evaluation of urinary incontinence. Obstet Gynecol. 1999;94(1):99–102.
Brubaker L, Nygaard I, Richter HE, Visco A, Weber AM, Cundiff GW, et al. Two-year outcomes after sacrocolpopexy with and without Burch to prevent stress urinary incontinence. Obstet Gynecol. 2008;112(1):49–55.
Schraffordt Koops SE, Bisseling TM, Heintz AP, Vervest HA. Prospective analysis of complications of tension-free vaginal tape from The Netherlands Tension-free Vaginal Tape study. Am J Obstet Gynecol. 2005;193(1):45–52.
Wei JT, Nygaard I, Richter HE, Nager CW, Barber MD, Kenton K, et al. A midurethral sling to reduce incontinence after vaginal prolapse repair. N Engl J Med. 2012;366(25):2358–2367.
Berild GH, Kulseng-Hanssen S. Reproducibility of a cough and jump stress test for the evaluation of urinary incontinence. Int Urogynecol J. 2012;23(10):1449–1453.
de Gregorio DG, Hillemanns HG. Urethral closure function in women with prolapse. Int Urogynecol J. 1990;1(3):143–145.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Y. Khayyami and G. Lose have received honoraria as investigators from Astellas. G. Lose has also been a consultant for Contura. N. Klarskov has received honoraria as a speaker/investigator and travel grants from Astellas.
Rights and permissions
About this article

Cite this article
Khayyami, Y., Lose, G. & Klarskov, N. Urethral pressure reflectometry in women with pelvic organ prolapse: a study of reproducibility. Int Urogynecol J 28, 705–710 (2017). https://doi.org/10.1007/s00192-016-3187-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-016-3187-1