
Abstract
Introduction and hypothesis
Studies have suggested that a posterior vaginal wall prolapse might compress the urethra and mask stress urinary incontinence (SUI), much like an anterior vaginal wall prolapse. A recent study with urethral pressure reflectometry (UPR) has shown that the urethral closure mechanism deteriorates after anterior colporrhaphy; this could explain the occurrence of postoperative de novo SUI. We hypothesized that urethral pressure would also decrease after posterior colporrhaphy.
Methods
This was a prospective, observational study where women with posterior vaginal wall prolapse ≥stage II were examined before and after posterior colporrhaphy. We performed prolapse staging according to the Pelvic Organ Prolapse Quantification system, UPR measurements at rest, during squeezing and straining, and standardized stress tests with 300 ml saline. The women filled out International Consultation on Incontinence-Urinary incontinence (ICIQ-UI) short forms. The sample size was 18, with a power of 99.9% and a level of significance of 5%. Parameters were compared using paired t tests or Fisher’s exact test, where appropriate; p values <0.05 were considered statistically significant.
Results
Eighteen women with posterior vaginal wall prolapse ≥stage II were recruited. One woman did not undergo surgery. There were no changes in urethral pressure at rest (p = 0.4), during squeezing (p = 0.2) or straining (p = 0.2), before and after surgery. The results of the stress tests and ICIQ-UI short forms were the same after surgery.
Conclusions
The urethral closure mechanism is not affected by posterior colporrhaphy. Our study does not support the theory that the posterior vaginal wall prolapse compresses the urethra and masks SUI.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prediction of de novo stress urinary incontinence (SUI) after pelvic organ prolapse (POP) surgery is an unsolved clinical challenge. Traditionally, postoperative de novo SUI is associated with surgery for anterior vaginal wall prolapse. The anterior vaginal wall prolapse is thought to mask SUI by either kinking or compressing the urethra [1]. As surgery removes this kinking or compression, postoperative SUI may be a consequence. However, studies with POP reduction (where the POP is repositioned with for instance a speculum) have revealed that posterior vaginal wall prolapse can also mask SUI, maybe even as frequently as anterior vaginal wall prolapse [2, 3]; however, the mechanism is unclear.
The predictive values of POP reduction are disappointing and of doubtful value in the preoperative counseling of patients [4,5,6]. Urethral pressure reflectometry (UPR) measures urethral pressure at rest, during squeezing and straining, and thus enables assessment of both the permanent and the adjunctive closure forces [7]; the permanent forces keep the urethra closed at rest and the adjunctive ones are recruited during stress, i.e., when abdominal pressure increases. UPR has not only proven to be superior to conventional urethral pressure profilometry [8], but it has also shown that SUI results from a weakening of these forces and it can separate between incontinent and continent women [9]. In fact, Saaby et al. found that the tension-free vaginal tape strengthens the adjunctive closure forces, which create support; this explains how and why the surgery restores continence in women with SUI [10]. The method has recently been used in a study where women with anterior vaginal wall prolapse were measured before and after anterior colporrhaphy [11]. The study showed that the urethral closure mechanism had deteriorated after surgery, suggesting it to be the most likely cause of postoperative SUI in these women. The preoperative value of urethral pressure during straining was found to be a predictor of the risk of postoperative SUI.
Little is known about the mechanism of continence in women with posterior vaginal wall prolapse, but it has been suggested that it masks SUI by compressing the urethra [12]. Seemingly, no studies have investigated how the mechanism of continence is affected by surgery for posterior vaginal wall prolapse. We hypothesized that urethral pressure would decrease after posterior colporrhaphy.
Materials and methods
This was a prospective, observational study conducted at the Department of Obstetrics and Gynecology, Herlev Gentofte University Hospital, Denmark. As our department is the largest tertiary urogynecological unit in Denmark, our patients have a variety of urogynecological conditions with a varying history of urogynecological treatments.
Women with posterior vaginal wall prolapse seen in our outpatient clinic were approached between November 2013 and March 2016. The women were recruited, regardless of their continence status, if they had posterior vaginal wall prolapse ≥stage II, measured with the Pelvic Organ Prolapse Quantification (POP-Q) system, and if they were scheduled for posterior colporrhaphy with or without concomitant perineorrhaphy. At our department, perineorrhaphy is sometimes performed simultaneously with a posterior colporrhaphy, depending on the findings in the preoperative examinations.
Exclusion criteria were a concomitant vaginal wall prolapse ≥stage II in the anterior compartment; a history of previous surgery for POP or SUI or hysterectomy; neurological diseases; use of any medicine for urinary incontinence; and pregnancy. The women were also excluded if they were under the age of 18; were unable to give their informed consent; or were not fluent in Danish.
The women were examined before and after surgery, but some of the women had an additional preoperative assessment with the purpose of investigating the reproducibility of UPR in women with POP [13]. This study only includes the first preoperative and the postoperative assessments, which were identical. We examined the women in the supine position and instructed them to relax so that any bulging POP would be repositioned, we did not perform POP reduction. We performed POP staging according to the POP-Q system. Next, we emptied the bladder with a SpeediCath Ch 10 and performed UPR measurements at rest, during squeezing, and during straining. Afterward, we emptied the bladder with a SpeediCath Ch 10, and performed a standardized stress test with 300 ml saline or up to maximum bladder capacity, using the same catheter. The women were instructed to cough vigorously three times. Finally, the women were asked to fill out International Consultation on Incontinence-Urinary incontinence (ICIQ-UI) short forms. The lead author of this paper and a study nurse conducted all assessments.
Measurements with UPR
Using acoustic reflectometry, UPR provides simultaneous and continuous measurements of pressure and cross-sectional areas along the entire length of the urethra. A bag is connected to a tube and inserted into the urethra. The tube connects to a probe (containing a microphone and a loudspeaker), which transmits sound waves. The probe connects to a syringe and a computer with an integrated pressure recorder. The syringe pumps air into the bag, thereby increasing the pressure, distending the bag and opening the urethra. As a result, the pressure needed to open the collapsed urethra, the opening pressure, is measured. Only measurements from the high-pressure zone (the position with a minimal urethral cross-sectional area at a given pressure) are evaluated. Pressures between 0 and 200 cmH2O and cross-sectional areas between 0.4 and 16 mm2 are measured [14].
We conducted ten consecutive measurements at rest, PO-rest, and calculated a mean of the 10 and 5 consecutive measurements during squeezing, PO-squeeze, and calculated a mean of the 5. Finally, we conducted 10 measurements with different intensities during straining, to ensure a wide variety of abdominal pressures. At rest, the woman was asked to relax while pressure in the bag was increased until the bag, and thereby the urethra was fully dilated, and then the pressure was decreased, all within 14 s. During each squeeze, we asked the woman to hold the squeeze for 7 s while the pressure in the bag was increased until the bag was fully dilated. We then asked the woman to relax and the bag deflated. During each measurement of straining, the woman was asked to hold the same pressure for 7 s, while the pressure in the bag was increased until the bag was fully dilated. We then asked the woman to relax again, and the bag deflated. Abdominal pressure was measured simultaneously throughout the entire measurement, using an air-filled balloon catheter placed in the rectum (T-dock, Wenonah, NJ, USA). Pressures were recorded in UDS120 Goby throughout the entire measurement, which synchronized recordings of UPR and abdominal pressures.
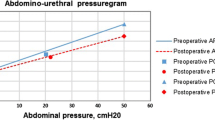
The related values of urethral and abdominal pressures were plotted into an abdomino-urethral pressuregram (Fig. 1). Saaby et al. named the slope of the line obtained from the pressuregram the abdominal to urethral pressure impact ratio (APIR) [9]. APIR expresses the effect that increasing abdominal pressure has on urethral pressure. Using APIR, the urethral opening pressure at any given abdominal pressure could be calculated. Measurements during straining were evaluated by assessing both APIR and urethral opening pressure at a standardized abdominal pressure of 50 cmH2O, PO-Abd 50.

Abdomino-urethral pressuregram showing the results from the preoperative measurement during straining in one of the women. The pressuregram illustrates how PO-Abd 50 is derived. P O-Abd 50 urethral opening pressure at an abdominal pressure of 50 cmH2O, APIR abdominal to urethral pressure impact ratio
Ethics
The National Committee on Health Research Ethics and the Danish Data Protection Agency approved the study (project-ID: H-4-2013-069). All women gave their written consent. The study was registered at ClinicalTrials.gov (NCT02050568).
Statistics
We expected a 10-cmH2O decrease in PO-Abd 50 to be clinically relevant and assumed that the measurements would show a standard deviation (SD) of 18. With a power of 80% and a level of significance of 5%, we needed to examine 26 women and with a drop-out rate of 15%, a sample size of 30 would ensure sufficient statistical power. We conducted a study on the reproducibility of the method in women with POP [13], before completing this study. The study revealed that the SD for women with posterior vaginal wall prolapse was 7.9. At this point, we had already included 18 women. Post-hoc power calculation with the new SD, and the included 18 women, revealed that the study had a power of 99.9% to find a difference of 10 cmH2O with a level of significance of 5%. Inclusion was therefore stopped.
All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). Continuous and categorical data were analyzed using paired t tests and Chi-squared or Fisher’s exact test respectively; p values <0.05 were considered statistically significant.
All methods, definitions, and units conform to the standards set by the International Urogynecological Association and the International Continence Society, except where specifically noted [15].
Results
We recruited 18 women with posterior vaginal wall prolapse ≥stage II. One woman decided not to undergo surgery and was therefore considered a dropout. Table 1 shows the demographics of the remaining 17 women.
All the women underwent posterior colporrhaphy and 7 had concomitant perineorrhaphy. There were no other concomitant procedures. The women were examined at a median of 17 (7–83) days before surgery and 53 (42–172) days after surgery. Table 2 shows the POP-Q results from the pre- and postoperative assessments.
Table 3 shows the results of the pre- and postoperative UPR measurements. There were no changes in any of the parameters after surgery.
There were no significant differences in stress test results before and after surgery; 2 women had positive stress tests preoperatively, and 4 women postoperatively (Fisher’s exact test p = 1). One woman was excluded from this analysis because of a missing preoperative stress test result. The women’s total score on the ICIQ-UI short forms did not change after surgery (Wilcoxon signed rank test p < 0.3); preoperative median was 4 (range 0–18) and postoperative median was 4 (range 0–14).
Discussion
There were no changes in any of the urethral parameters, stress test outcomes or symptoms of SUI after posterior colporrhaphy. Our results do not support the theory that posterior prolapse masks SUI by compressing the urethra, as suggested by Myers et al. [12]. They examined women with posterior vaginal wall prolapse before and after POP reduction using a split speculum. They found that maximum urethral closure pressure (MUCP) decreased by a mean of 7 cmH2O and leakage volume increased significantly during stress tests with POP reduction in women with grade 3 prolapses (using Baden and Walker definitions). Myers et al. then suggested that severe posterior wall defects compress and thus support the anterior vaginal wall, maintaining continence in the women [12]. However, their results showed no differences when comparing women with grade 0, 1, 2, and 3 POP; all women had a decrease in mean MUCP and an increase in leakage volume during POP reduction, regardless of prolapse grade. Nguyen et al. examined women with posterior vaginal wall prolapse ≥stage II (using POP-Q) before and after POP reduction using a Pederson speculum and matched the women with controls [2]. Nguyen et al. also found that urethral parameters, in this case Valsalva leak point pressure and pressure transmission ratio, decreased significantly after the introduction of the speculum in both controls and in the women with posterior vaginal wall prolapse [2]. These results were confirmed by Zivkovic et al. [16], who examined 32 continent women with no prolapse and found that pressure transmission ratio and urethral closure pressure decreased after the introduction of a speculum. Thus, all three studies showed results indicating that urethral parameters may decrease regardless of the presence of a prolapse, simply because a speculum is introduced into the vagina. All three studies used microtip transducers for the measurement of urethral parameters. A microtip-transducer can measure a local fluid pressure, but when it is placed in a closed urethra it merely senses the force of the tissue on its transducer surface; this is not the same as measuring true urethral parameters [17]. We do not believe that POP reduction and POP surgery have the same effect on vaginal support. Therefore, using POP reduction to predict postoperative outcome is arbitrary and associated with great uncertainty [5].
Lower urinary tract symptoms are not usually associated with posterior vaginal wall prolapse. However, Mouritsen and Larsen [18] examined 110 women and asked them to fill out questionnaires concerning LUTS and bowel symptoms, amongst others. They performed pelvic examinations on the women and divided the women depending on prolapse stage (POP-Q) and compartment. They found that bowel symptoms, namely evacuation problems, were associated with women with posterior vaginal wall prolapse, but surprisingly, the women with posterior vaginal wall prolapse also had symptoms of LUTS, including complaints of SUI, to the same extent as women with anterior vaginal wall prolapse. Recently, we examined women with anterior vaginal wall prolapse before and after anterior colporrhaphy with UPR [11]. We found that PO-Abd 50 and APIR decreased to 12 cmH2O (p < 0.0001) and 0.3 (p < 0.01) respectively; PO-Abd 50 and APIR assess the adjunctive closure mechanism, which consists of the forces that support the urethra during any activity that increases abdominal pressure, such as coughing, laughing, and walking, etc. This means that the most likely cause of postoperative SUI in these women is a deteriorated urethral closure mechanism. The mechanism of continence is clearly not affected in the same way after a posterior colporrhaphy as after an anterior colporrhaphy.
To the best of our knowledge, our study is the first to examine women with urethral measurements before and after posterior colporrhaphy. We have found that the urethral closure mechanism is not affected after this surgery. One of the strengths of this study is the high reproducibility of urethral pressure reflectometry [13]; the power to detect a clinically relevant difference before and after surgery was very high, despite the relatively low number of women in this study. The aforementioned studies used microtip-transducers, which is not only a method associated with artifacts, but is also a method with low reproducibility [19]. The women in our study had not had any previous surgery for POP, SUI, or hysterectomy; thus, our study allows us to investigate the isolated effect of the posterior vaginal wall prolapse on the urethra. However, our study does have some limitations. First, we examined the women at a median of 53 days after surgery. This may have been too soon with regard to the women resuming their normal everyday life. Some of the women had not resumed their regular exercise activities, and others had not resumed their sexual lives, which may have had an impact on the women’s symptoms. Also, even though the women in our study had ≥stage II prolapses, the prolapses were small with a median of 0 cm for both POP-Q Ap and Bp.
The challenge of prolapse treatment is that women’s symptoms do not correlate well with the anatomical site of the POP [20]. A woman may very well have a posterior vaginal wall prolapse with concomitant SUI, but the two conditions may not be associated with one another. This study does not support the theory that posterior prolapse masks SUI by compressing the urethra.
References
Marinkovic SP, Stanton SL. Incontinence and voiding difficulties associated with prolapse. J Urol. 2004;171:1021–8. doi:10.1097/01.ju.0000111782.37383.e2.
Nguyen JN, Yazdany T, Burchette RJ. Urodynamic evaluation of urethral competency in women with posterior vaginal support defects. Urology. 2007;69:87–90. doi:10.1016/j.urology.2006.09.068.
Smith TM, DeLancey JOL, Fenner DE. Post-reduction stress urinary incontinence rates in posterior versus anterior pelvic organ prolapse: a secondary analysis. Int Urogynecol J. 2013;24:1355–60. doi:10.1007/s00192-012-2019-1.
Ellström Engh AM, Ekeryd A, Magnusson Å, et al. Can de novo stress incontinence after anterior wall repair be predicted? Acta Obstet Gynecol Scand. 2011;90:488–93. doi:10.1111/j.1600-0412.2011.01087.x.
Svenningsen R, Borstad E, Spydslaug AE, et al. Occult incontinence as predictor for postoperative stress urinary incontinence following pelvic organ prolapse surgery. Int Urogynecol J. 2012;23:843–9. doi:10.1007/s00192-012-1764-5.
Visco AG, Brubaker L, Nygaard I, et al. The role of preoperative urodynamic testing in stress-continent women undergoing sacrocolpopexy: the Colpopexy and Urinary Reduction Efforts (CARE) randomized surgical trial. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19:607–14. doi:10.1007/s00192-007-0498-2.
Khayyami Y, Klarskov N, Lose G. The promise of urethral pressure reflectometry: an update. Int Urogynecol J. 2016;27:1449–58 doi:10.1007/s00192-016-2964-1.
Klarskov N, Lose G. Urethral pressure reflectometry vs urethral pressure profilometry in women: a comparative study of reproducibility and accuracy. BJU Int. 2007;100:351–6. doi:10.1111/j.1464-410X.2007.06922.x.
Saaby M-L, Klarskov N, Lose G. Urethral pressure reflectometry during intra-abdominal pressure increase—an improved technique to characterize the urethral closure function in continent and stress urinary incontinent women. Neurourol Urodyn. 2013;32:1103–8. doi:10.1002/nau.22368.
Saaby M-L, Klarskov N, Lose G. The impact of tension-free vaginal tape on the urethral closure function: mechanism of action. Neurourol Urodyn. 2015;34:50–4. doi:10.1002/nau.22513.
Khayyami Y, Klarskov N, Lose G. Abstract: urethral pressure reflectometry predicts stress urinary incontinence after anterior colporrhaphy. Neurourol Urodyn. 2016;35:S1–S471. doi:10.1002/nau.23074.
Myers DL, Lasala CA, Hogan JW, Rosenblatt PL. The effect of posterior wall support defects on urodynamic indices in stress urinary incontinence. Obstet Gynecol. 1998;91:710–4.
Khayyami Y, Lose G, Klarskov N. Urethral pressure reflectometry in women with pelvic organ prolapse: a study of reproducibility. Int Urogynecol J. 2016;28:705–10. doi:10.1007/s00192-016-3187-1.
Klarskov N. Urethral pressure reflectometry. A method for simultaneous measurements of pressure and cross-sectional area in the female urethra. Dan Med J. 2012;59:B4412.
Haylen BT, Maher CF, Barber MD, et al. An International Urogynecological association (IUGA)/International continence society (ICS) joint report on the terminology for female pelvic organ prolapse (POP). Int Urogynecol J. 2016;27:165–94. doi:10.1007/s00192-015-2932-1.
Zivkovic F, Tamussino K, Haas J. Contribution of the posterior compartment to the urinary continence mechanism. Obstet Gynecol. 1998;91:229–33.
Schäfer W. Some biomechanical aspects of continence function. Scand J Urol Nephrol Suppl. 2001;207:44–60. discussion 106–25.
Mouritsen L, Larsen JP. Symptoms, bother and POPQ in women referred with pelvic organ prolapse. Int Urogynecol J Pelvic Floor Dysfunct. 2003;14:122–7. doi:10.1007/s00192-002-1024-1.
Weber AM. Is urethral pressure profilometry a useful diagnostic test for stress urinary incontinence? Obstet Gynecol Surv. 2001;56:720–35.
Ellerkmann RM, Cundiff GW, Melick CF, et al. Correlation of symptoms with location and severity of pelvic organ prolapse. Am J Obstet Gynecol. 2001;185:1332–7; discussion 1337–8. doi:10.1067/mob.2001.119078.
Acknowledgements
We thank Nurse Berit Sejersen Larsen for her assistance with all examinations in this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The study was conducted at the Department of Gynecology and Obstetrics, Herlev Gentofte hospital and funded by the University of Copenhagen as a PhD scholarship. The University of Copenhagen was not involved in the study.
Conflicts of interest
Yasmine Khayyami, Gunnar Lose, and Niels Klarskov have received honoraria as investigators from Astellas. Gunnar Lose has also been a consultant for Contura.
Rights and permissions
About this article

Cite this article
Khayyami, Y., Lose, G. & Klarskov, N. Posterior colporrhaphy does not affect the urethral closure mechanism. Int Urogynecol J 29, 125–130 (2018). https://doi.org/10.1007/s00192-017-3401-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-017-3401-9