
Abstract
Introduction
Schizophrenia is a chronic and debilitating mental illness characterised by periods of relapse that require resource intensive management. Quantifying the cost of relapse is central to the evaluation of the cost effectiveness of treating schizophrenia.
Objectives
We aimed to undertake a comprehensive search of the available literature on the cost of relapse.
Methods
We performed a search on multiple databases (MEDLINE, Embase, PsycINFO and Health Management Information Consortium) for any study reporting a cost of relapse or data from which such a cost could be calculated. Costs are reported in 2015 international dollars.
Results
We found 16 studies reporting costs associated with relapse over a defined period of time and identified a cost associated with hospitalisation for relapse in 43 studies. Eight clinical decision analyses also provided cost estimates. Studies from the US report excess costs of relapse of $6033–$32,753 (2015 Purchasing Power Parity dollars [PPP$]) over periods of 12–15 months. European studies report excess costs of $8665–$18,676 (2015 PPP$) over periods of 6–12 months. Estimates of the cost of hospitalisation for relapse are more diverse, and associated with marked differences in typical length of stay across jurisdictions.
Conclusions
Wide ranges in the estimated cost of relapse may reflect differences in sample section and relapse definition as well as practice styles and differences in resource costs. Selection of the most appropriate cost estimate should be guided by the definition of relapse and the analysis setting.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Estimates of the excess cost of relapse in schizophrenia range from $9000 to $19,000 (2015 USD) in European settings. |
Estimates of the excess cost of relapse in schizophrenia range from $16,000 to $33,000 in US settings over periods of 6–15 months. |
Estimates of the cost of hospitalisation for relapse are more diverse due to large differences in clinical practice regarding length of stay as well as differences in unit costs across settings. |
1 Introduction
Schizophrenia is a lifelong, chronic and severely debilitating mental illness that often strikes in young adulthood [1]. Mangalore and Knapp estimated the cost of schizophrenia in England at £6.7 billion per year, £2 billion of which was direct costs falling primarily on health and social care budgets [2]. Similar estimates for the US indicate an overall cost of $156 billion (2013 USD), of which $38 billion was consumed in direct healthcare costs [3]. The annual societal cost per patient may be as high as $95,000 (2015 USD), and the lifetime costs approaching $1 million [4]. Whilst such cost-of-illness estimates are valuable in highlighting the seriousness of mental illness, they do not provide a direct estimate of the impact on costs of alternative intervention strategies to treat schizophrenia. The main goal of treatment for schizophrenia is to prevent relapse into a psychotic state. Relapse frequently necessitates hospitalisation and is potentially resource intensive. Quantifying the cost of relapse is essential to understanding the cost effectiveness of treating schizophrenia.
Quantifying the cost of relapse requires a clear definition of what constitutes a relapse. The most commonly used measure of relapse is hospitalisation due to exacerbation of symptoms [5, 6]. Relapse is also identified through clinical assessment of exacerbation of symptoms, including the use of outcome measures such as the Positive and Negative Syndrome Scale (PANSS) [7]. Violence, arrest, self-harm, suicide and suicidal ideation are also sometimes taken to indicate relapse. Ambiguity as to what constitutes a relapse probably explains the relative small number of publications purporting to report a cost of relapse despite the funding of a number of large, observational studies specifically designed to evaluate the cost of supporting schizophrenia patients over the last 20 years [8,9,10].
Three principal approaches to costing a relapse can be distinguished in the literature dependent upon how relapse is defined. The first approach accommodates any definition of relapse and relies on obtaining costs over a fixed period of time. This approach is well suited to both prospective, observational studies and analyses of administrative datasets, although the latter usually limits the method of identification of relapse. Such an approach also facilitates the estimation of the excess cost of relapse over and above the cost of patients in remission. The second approach equates relapse with hospitalisation for relapse and costs the hospital stay. This approach is not well suited to estimating the excess costs of relapse but avoids the need to define an arbitrary time period over which to collect costs with the risk that such a period is insufficiently long, or includes multiple relapse episodes. The third approach utilises expert clinical opinion on likely resource use, sometimes in combination with data from administrative databases on length of hospital stay.
The aim of this study is to review the literature on the cost of relapse in schizophrenia. Within the framework outlined above we sought to identify all de novo estimates of the cost of relapse. We included papers where such a cost is not explicitly reported but could be determined from reported data. We have calculated excess costs of relapse where reported data allowed but the authors had not explicitly done so. We also provide a cost inflated to 2015 USD after conversion at purchasing power parity rates to facilitate comparison of studies.
2 Methods
A structured search of MEDLINE, Embase, PsycINFO and Health Management Information Consortium (HMIC) was undertaken to identify articles published before January 2017 (November 2016 for HMIC) using the following search strategy: ‘Cost$’[Title/abstract/keyword] AND ‘schizophrenia’[Title/abstract/keyword] AND {‘Relapse’[Title/abstract/keyword] OR ‘Hospitali$’ [Title/abstract/keyword]}. The search strategy is reported in detail in the electronic supplementary material. The retrieved records were checked for duplicates, but no further limitations were applied prior to screening. The UK databases NHS EED (National Health Service Economic Evaluation Database), DARE (Database of Abstracts of Reviews of Effects) and HTA (Health Technology Assessment) were also searched using modified versions of the above search terms. References and citations of all identified relevant articles were also searched. We applied the following inclusion criteria:
-
1.
Publications in English.
-
2.
The relevant population were wholly or predominantly diagnosed with schizophrenia or schizoaffective disorder.
-
3.
The study provided an estimate of the cost of relapse and not simply an indication of resource use such as length of stay in hospital.
-
4.
Conference abstracts with an estimate of the cost of relapse discernible from a published record.
-
5.
Top-down costing studies with data on the incidence of relapse or the prevalence of schizophrenia which allowed a calculation of the cost of relapse.
-
6.
Estimates based on expert opinion.
Studies were excluded if they reported length of stay (LOS) but provided no data on associated costs. We excluded decision analyses which assumed a cost of hospitalisation as a fixed reimbursement tariff for a psychiatric inpatient stay regardless of LOS. Modelling studies were excluded if relapse costs were inflated estimates from a published source. We included papers where a cost of relapse or hospitalisation for relapse could be calculated from the data presented for the entire cohort of patients relapsing; we excluded papers in which this calculation was only possible for a subgroup of relapsing patients. Data were abstracted and reviewed by the first author (MP). Studies were classified into the following categories: those reporting costs over a defined time period, those reporting a cost per hospitalisation for relapse and those drawing on expert opinion to estimate costs. The latter studies were exclusively clinical decision analyses. Studies reporting costs over a defined period were subdivided into those reporting all-cause medical costs, mental health costs and schizophrenia-related costs; where all-cause and schizophrenia-related costs were reported, we tabulated both. Given the varied nature of the studies, we did not apply a formal quality appraisal procedure.
Frequently, data were reported which allowed calculation of a cost of hospitalisation but the cost was not reported. Mean LOS and mean cost of hospitalisation was calculated by dividing total LOS and total hospital costs by the mean number of inpatient stays where such data were reported. Where data were reported for both baseline and follow-up periods, we combined data prior to calculation of mean LOS and mean hospital cost. Where data were reported by subgroup to facilitate comparison of treatment regimens, we combined the data across subgroups prior to calculating mean LOS and mean hospital costs (effectively, we calculated a weighted mean across subgroups). Where costs were reported for patients who relapsed and patients who did not, we calculated the excess cost of relapse as the difference between the two costs. Where costs are reported in USD after conversion, we report costs in both USD and home currency. Costs in home currency were converted to Purchasing Power Parity dollars (PPP$) using OECD values [11] and inflated to 2015 prices using a published conversion tool [12]. A price year was estimated for publications which failed to clarify the relevant year.
We undertook regression analysis to explore the influence of potential cost drivers on the cost of relapse and the cost of hospitalisation for relapse. We used generalised linear modelling and did not account for the relative size of different studies. The cost drivers we examined were price year (as a measure of how long ago the study was undertaken), per capita gross domestic product (GDP) for the country of origin and whether or not the study originated in the US. The latter two variables have been shown to be strong predictors of hospital costs [13]. For the cost of hospitalisation of relapse we also included mean LOS. For the cost of relapse we also included the duration of the relapse period. Price year was specified as the number of years after 1992. All costs and GDP values were expressed in 2015 PPP$. Schizophrenia-related costs were prioritised over mental-health-related costs over all-cause costs where a study reported costs in multiple categories. In the analysis of the cost of relapse, dummy variables were used to control for differences arising from the reporting of mental-health-related or all-cause costs rather than schizophrenia costs. Given the expected skew in the dependent variables, we assumed a gamma distribution. We also assumed a multiplicative effect of the independent variables as is commonly observed for cost data. Given the inevitably small sample size, tests of distributional form and link function would have been underpowered and possibly misleading so we did not use them to guide model selection. Covariate selection was guided by Akaike’s Information Criteria [14].
3 Results
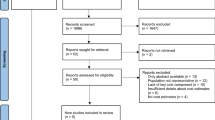
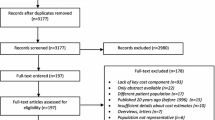
Our searches returned 1931 abstracts, of which 196 were identified as potentially relevant (Fig. 1). From these, 174 papers were retrieved and reviewed. Six conference abstracts and 57 papers were identified as providing relevant data.

Flow diagram illustrating literature selection process
3.1 Studies Reporting Costs Associated with Relapse Over a Defined Period
Sixteen papers reported costs of relapse over a defined period of observation (Table 1). The studies originated from the US (5) [10, 15,16,17,18], UK (1) [19], Germany (2) [20, 21], Brazil (1) [22], Singapore (1) [23], China (2) [24, 25], Australia (1) [26] and Sweden (1) [27], with the remaining two pan-European [28, 29]. All were based on retrospective analysis of clinical or administrative data and used a bottom-up costing approach. Thirteen studies allowed calculation of an excess cost of relapse from comparison of data on relapsing and non-relapsing patients [10, 15,16,17,18,19,20, 23,24,25,26,27,28] and one paper reported the proportional cost increase associated with relapse without reporting the raw costs [21]. The majority of studies reported costs over 1 year [10, 16, 17, 20, 22,23,24,25,26, 28]; one study reported costs over 15 months [18]; three studies reported costs over 6 months [19, 21, 27]; one study reported costs over 3 months [29] and one study reported costs over 1 week [15]. The majority of studies reported mental-health-related costs [10, 18, 19, 21,22,23, 25,26,27, 29]. Six studies reported all-cause health costs [15,16,17, 20, 24, 25], of which three also reported schizophrenia-related costs [15, 16, 20], one study also reported total costs [24], and one study reported all-cause, mental-health-related and schizophrenia-related costs [25]. One study reported solely schizophrenia-related costs [28]. Most studies included adults with a diagnosis of schizophrenia [10, 15,16,17,18,19,20,21,22,23, 26,27,28,29]. US studies exploiting administrative data generally identified patients using International Classification of Disease (ICD)-9 codes without excluding schizophreniform and schizoaffective disorder [15,16,17]; German studies used ICD-10 codes which excluded schizophreniform and schizoaffective disorder [20, 21]. The majority of studies exploiting administrative data defined relapse as a psychiatric hospitalisation, although one study included emergency room visits [16], and one study defined relapse as periods of relative or absolute increase in costs [15]. Studies collecting data prospectively typically applied wider criteria to define relapse, which included deterioration in psychiatric health status and suicide attempts [10, 28].
Costs included were not always clearly stated but all studies appeared to include inpatient, outpatient and drug costs. Three European studies included wider costs: sickness payments (sick leave) [20], vocational costs [19, 21] and accommodation costs [21]. One study from China included direct non-medical costs and indirect costs relating to crime and productivity [24]. Unsurprisingly, costs were generally higher in US studies and where costs were reported over a longer period. Where studies reported all-cause and schizophrenia-related costs, schizophrenia-related costs were 30–92% of the all-cause costs. The difference was larger for the overall cost of relapse than for the excess cost, and for the US studies compared with the Chinese and German studies. The latter may reflect differences in the quality of diagnostic data. However, studies reporting all-cause costs did not provide the largest cost estimates; larger estimates were derived from studies reporting mental-health-related costs. This pattern might suggest that whilst hospitalisation episodes were not always correctly identified as schizophrenia-related episodes, they were generally identified as mental-health-related episodes, and further, that the majority of hospitalisations in this population are related to mental health.
The overall cost of relapse for US studies reporting over 12–15 months ranged from $16,848 to $48,442 (2015 PPP$); the excess cost of relapse for the same studies ranged from $6033 to $32,753. The study which provided the lowest cost estimate for both overall and excess costs included emergency room visits in the definition of relapse [16], which is likely to have expanded the scope of the study to include lower-cost episodes. Amongst the studies from Europe and Australia, the overall cost of relapse ranged from $10,515 to $26,865 (2015 PPP$) and the excess cost of relapse ranged from $8665 to $18,676 (2015 PPP$). Costs were generally higher for the studies reporting costs over 1 year. Costs were lower in studies undertaken outside Europe, the US and Australia; overall relapse costs ranged from $2760 to $9290 and excess relapse costs ranged from $4263 to $6524 (2015 PPP$). Across all studies, the relative cost increase associated with relapse ranged from 103% to 1137% of costs for patients who had not relapsed.
Regression analysis indicated the natural logarithm of GDP was a modest predictor of the overall cost of relapse (p = 0.037) but not the excess cost of relapse. US country of origin was not a significant predictor of overall or excess costs. After eliminating the dummy for US studies, costs rose with the length of the period defining relapse, increasing by around 15% per month for both overall and excess costs (overall costs, p = 0.001; excess costs, p = 0.002). Perhaps surprisingly, costs fell for newer studies, decreasing by around 7% for each year beyond 1992 for overall costs and by around 12% for each year beyond 1992 for excess costs (overall costs, p = 0.011; excess costs, p = 0.001).
3.2 Studies Reporting a Cost of Hospitalisation for Relapse
Forty-three studies either reported a cost per hospitalisation for relapse or provided sufficient data to calculate a mean cost (Table 2) [16, 25, 27, 28, 30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,68]. Four of these studies provided data on the cost of hospitalisation in addition to the cost of relapse over a defined period and are included in both Tables 1 and 2 [16, 25, 27, 28]. Thirteen of the studies originated from the US [16, 30,31,32,33,34,35,36,37,38,39,40,41] and a further 22 originated from Europe [27, 28, 42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61]. The majority of studies were bottom-up studies deriving costs from billing data or from LOS in combination with a reimbursement value per bed day. Only two studies [41, 68] undertook a top-down costing approach in which national estimates of expenditure on inpatient care for schizophrenia were divided by a measure of the number of inpatient episodes. Most studies excluded children. However, one US study provided data solely on children [30]. Most studies limited hospitalisations to episodes associated with a diagnosis of schizophrenia, although some studies included all mental-health-related hospitalisations and two studies limited reporting of cost data to all-cause hospitalisations [32, 39]. Most studies were retrospective analyses of clinical or administrative data.
Hospitalisation costs in the US ranged from $6383 to $28,767 (2015 PPP$). The highest costs were reported in a study of children and adolescents [30]. Of the remaining US studies, the highest cost estimate was $22,909 [31]. In Europe, Japan and New Zealand, hospitalisation costs ranged from $1615 to $39,088. The lowest cost derived from Ukrainian data [47] and the second lowest from a study set in the Czech Republic [51]. Costs in countries outside the US, Europe, Japan and New Zealand ranged from $2217 to $14,923. Regression analysis of costs indicated no significant change over time as reflected by the price year of the study. There was a strong relationship between hospitalisation cost and GDP of the relevant country (p < 0.001). US-based studies were not associated with significantly different hospitalisation costs compared with studies from other countries. LOS was significant after excluding the dummy for US-based studies (p = 0.027) and associated with a 0.8% increase in costs for each additional bed day.
3.3 Relapse Costs Determined from External Sources Including Expert Opinion
The literature on economic evaluations yielded eight de novo estimates of the cost of relapse derived either from publicly available data or expert opinion ranging from $1895 to $48,847 (2015 PPP$) (Table 3) [69,70,71,72,73,74,75,76]. Costs of hospital stay were predominantly estimated from national administrative data [70, 71, 74, 75] or expert opinion [72, 73, 76] on LOS, in combination with daily reimbursement rates. Assumptions on the total inpatient stay varied from 11 days [75] to 111 days [70] for admitted patients. The latter estimate was derived from UK NHS administrative data (Hospital Episode Statistics). With the exception of two studies [73, 75], inpatient costs were supplemented with estimates of additional resource use generated predominantly from expert opinion. Two studies assumed further day hospital stay following discharge of 8 days [72] and 23 days [69]. Two studies included accommodation costs following discharge from hospital [69, 76], one of which generated the largest overall cost estimate [69]. Two publications distinguished costs according to whether or not relapse required hospitalisation [72, 74], and one study distinguished costs according to whether relapse occurred during first- or second-line treatment [73]. The time period over which costs were estimated varied from 67 days to 1 year, although the selection of 3 months or 1 year was common. Longer periods were not necessarily associated with higher costs. One study estimated an annual excess cost of relapse over patients in remission of £20,294 ($33,907, 2015 PPP$) [70].
4 Discussion
We found cost estimates for relapse varying from 2590 BRL ($2760; 2015 PPP$) in Brazil [22] to 417,000 SEK ($48,847; 2015 PPP$) in a Swedish setting [69]. Most of the cost estimates are derived from literature which either reported a cost of hospitalisation for relapse or reported data from which such a cost could be calculated. These data are highly variable but strongly positively associated with GDP per capita. This accords with previous findings of a strong relationship between per capita GDP and hospital costs in general [13]. The relationship between mean LOS and hospitalisation costs is surprisingly weak. This might indicate differences in treatment intensity which compensate for differences in LOS.
The large variation in costs across different countries is not unexpected. However, there were large variations in costs estimates across European countries which might be expected to have similar healthcare unit costs, and indeed the variation in costs across the studies from the US is nearly as large as that from European studies. This might be indicative of heterogeneity of populations across studies with respect to disease severity and pharmacological treatment. Comparison of costs before and after patients initiate depot medication has the potential to select patients with more severe disease and to select patients with a recent exacerbation of symptoms. In contrast, trials and observational cohort studies may select patients with less severe disease, particularly where inclusion criteria specify the need for patients to be ‘stable’.
A smaller portion of the literature reported costs associated with relapse over a specified time period. The observed relationship between both overall and excess cost and the length of the observation period was unsurprising. However, given the small number of studies, caution should be exercised with regard to the magnitude of the increase we found and the assumption that the proportionate rise is linear over time. More surprising was the fall in costs for more recent studies. The number of studies analysed was small and this finding may be a statistical artefact. However, it might indicate a fall in the costs of managing relapse over time attributable to reductions in hospital LOS and increased emphasis on managing patients in relapse in the community. There is also a risk that the costs of intensive management of relapsing patients in the community are only partially captured in administrative databases. The relationship between GDP per capita and costs of relapse is weak. This might suggest that after adjusting for differences in purchasing power there is little difference in the overall cost of relapse across resource-rich and resource-poor settings.
Comparisons between costs of relapse estimated over a defined period and costs of hospitalisation for relapse for studies in European settings are confounded by different country settings across the two types of study. Focussing on the subgroup of studies from Sweden, Germany and the UK, the range of costs is widest for studies reporting a cost of hospitalisation, but it is not evident that studies reporting a cost of hospitalisation generate systematically higher or lower costs than studies reporting a cost of relapse over a defined period of time. From the US literature, studies estimating a cost of hospitalisation generated a similar range of costs to studies estimating an excess cost of relapse over a defined period of time, and less than studies estimating an overall cost of relapse. Hence, we might tentatively conclude that studies reporting a cost of hospitalisation for relapse are broadly capturing the excess cost of relapse over patients in remission. Some caution is needed here. It is almost certain that hospital costs for patients in relapse substitute for costs of managing patients in remission in the community. This may be offset by a tendency for studies reporting costs of hospitalisation to exclude patients with less severe disease and almost certainly less severe relapse through the inclusion of only admitted patients.
4.1 Comparisons with Previous Studies
With the exception of a conference presentation, we found no previous literature reviewing the cost of relapse. The conference abstract reported a range from US$1198 to US$50,986 across 11 studies [77]. The lower value would appear to be sourced from Daltio et al. [22] and the upper value from Ascher-Svanum et al. [10] for the subgroup of patients relapsing in both the observation year and the previous 6 months. The authors reported an average cost of €3421 (2005 Euros), although the meaningfulness of a mean cost across such disparate settings is debatable. In their review of the costs of compliance, Theida et al. provide a brief discussion of the (US) literature on the cost of relapse, citing four studies and concluding that costs lie in the range of $10,000 to $26,000 (USD, price year not reported) [78].
4.2 Methodological Quality of Literature
Methodological concerns arose largely from study design rather than implementation, although it is notable that a number of studies failed to state the year of pricing. Large observational cohort studies provide the strongest research design to generate evidence on the cost of relapse. Hence it is disappointing that many of the large observational cohort studies, with the exception of US-SCAP (United States Schizophrenia Care and Assessment Program) [10] and SOHO (Schizophrenia Outpatient Health Outcome) [28], have not reported a cost of relapse. Estimates of relapse costs derived from administrative data have some limitations: the definition of relapse is limited to a measure of resource use (typically hospitalisation); there are concerns around the quality of data capture; the scope of data collection is limited to resource use recorded in the database; and true costs may be closer to reimbursed values than billed amounts. Nevertheless, both approaches allow estimation of the excess cost of relapse. In this respect, they provide a stronger research design than studies estimating costs for a cohort of hospitalised patients. The latter study design may also inflate costs through selective inclusion of more severely ill patients. Indeed, with the exception of estimates based on expert opinion, the highest relapse costs were generated from a cost of hospitalisation study [50]. Relapse costs extracted from studies whose primary purpose was to investigate the impact of changing drug therapy also merit concern around representativeness of the population under study.
Most studies were limited to a healthcare perspective by the use of clinical or administrative data. Hence, there is limited evidence of the impact of relapse on social care costs. Accommodation costs may be reduced during periods of hospitalisation but other costs seem likely to rise. We found only one report which included indirect costs [24]. That study indicates that additional indirect costs of morbidity, mortality and criminal damage related to relapse are modest. Very little data was identified on the costs of secure hospitalisation and criminal justice costs associated with relapse. Forensic hospitalisations are rarely identified in studies and many cohort studies exclude patients hospitalised for long periods of time. UK costs per bed day are 67% higher in secure units compared with non-secure psychiatric beds, and such a differential seems likely elsewhere [79]. Studies from the US that examined criminal justice costs generally reported very modest costs in comparison with medical costs (c.f. $1429, 2001 USD) [80]. Indeed, the increased medication costs of adherent patients overwhelm the reductions in criminal justice costs associated with treatment compliance [81].
4.3 Strengths and Limitations
The strengths of this review include wide inclusion criteria which sought to capture all of the available evidence on the cost of relapse. Where a cost of relapse was not reported but could be calculated we have done so. We have tabulated excess costs of relapse over defined time periods, where these costs were reported or could be calculated, to facilitate comparison across studies. We did not include studies that reported LOS data without attaching costs, although unit cost data is readily available, as it was not our aim to provide an exhaustive survey of the literature on the LOS following relapse. We searched a limited number of databases and did not undertake double review of articles retrieved by the initial search. This may have resulted in the exclusion of relevant studies. We did undertake extensive efforts to search articles cited in and citing relevant retrieved studies. Finally, we did not undertake a formal assessment of the quality of the studies. Such an assessment may not reflect the relative merit of the cost estimates which was frequently not the primary objective of the article. Instead we provide readers with contextual data which should guide the selection of the most appropriate estimates according to the setting and intended use of the data.
5 Conclusion
A number of estimates of the cost of relapse in schizophrenia are discernible from the literature. The most robust estimates are derived from prospective cohort studies and analyses of administrative databases which indicate excess costs of relapse of $6033–$32,753 (2015 PPP$) in the US, and $8665–$18,676 (2015 PPP$) in Europe. The major portion of reported costs is attributable to hospitalisation, but few studies collected cost data outside of healthcare. Costs of hospitalisation for schizophrenia cohorts in relapse showed greater variation, influenced by large variations in LOS. Whilst the scope of data collection in such studies is limited, cost estimates may be inflated by inclusion of a more severe case mix. The cost of relapse is an essential consideration in the evaluation of the cost effectiveness of treating schizophrenia. Sufficient evidence is available to challenge the reliance on expert opinion, but additional estimates, especially from large observational cohort studies, would be valuable.
References
Jablensky A, Sartorius N, Ernberg G, Anker M, Korten A, Cooper JE, Day R, Bertelsen A. schizophrenia: manifestations, incidence and course in different cultures A World Health Organization Ten-Country Study. Psychological medicine. Monogr Suppl. 1992;20:1–97.
Mangalore R, Knapp M. Cost of schizophrenia in England. J Ment Health Policy Econ. 2007;10(1):23.
Cloutier M, Aigbogun MS, Guerin A, Nitulescu R, Ramanakumar AV, Kamat SA, DeLucia M, Duffy R, Legacy SN, Henderson C, François C. The economic burden of schizophrenia in the United States in 2013. J Clin Psychiatry. 2016;77(6):764–71.
Jin H, Mosweu I. The societal cost of schizophrenia: a systematic review. Pharmacoeconomics. 2017;35(1):25–42.
Taylor M, Chaudhry I, Cross M, McDonald E, Miller P, Pilowsky L, Strickland P. Towards consensus in the long-term management of relapse prevention in schizophrenia. Hum Psychopharm Clin. 2005;20(3):175–81.
Olivares JM, Sermon J, Hemels M, Schreiner A. Definitions and drivers of relapse in patients with schizophrenia: a systematic literature review. Ann Gen Psychiatry. 2013;12(1):32.
Kay SR, Flszbein A, Opfer LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261.
Knapp M, Chisholm D, Leese M, Amaddeo F, Tansella M, Schene A, Thornicroft G, Vazquez-Barquero JL, Knudsen HC, Becker T. Comparing patterns and costs of schizophrenia care in five European countries: the EPSILON study. Acta Psychiat Scand. 2002;105(1):42–54.
Heider D, Bernert S, König HH, Matschinger H, Hogh T, Brugha TS, Bebbington PE, Azorin M, Angermeyer MC, Toumi M. Direct medical mental health care costs of schizophrenia in France, Germany and the United Kingdom—findings from the European schizophrenia Cohort (EuroSC). Eur Psychiatry. 2009;24(4):216–24.
Ascher-Svanum H, Zhu B, Faries DE, Salkever D, Slade EP, Peng X, Conley RR. The cost of relapse and the predictors of relapse in the treatment of schizophrenia. BMC Psychiatry. 2010;10(1):2.
Organisation for Economic Co-operation and Development. Purchasing Power Parities for GDP dataset. 2016. http://stats.oecd.org/Index.aspx?DataSetCode=SNA_Table4#. Accessed Apr 2017.
Shemilt I, Thomas J, Morciano M. A web-based tool for adjusting costs to a specific target currency and price year. Evid Policy: J Res Debate Pract. 2010;6(1):51–9.
Adam T, Evans DB, Murray CJ. Econometric estimation of country-specific hospital costs. Cost Eff Resour Alloc. 2003;1(1):3.
Akaike H. A new look at the statistical model identification. IEEE Trans Autom Control. 1974;19(6):716–23.
Lafeuille MH, Gravel J, Lefebvre P, Fastenau J, Muser E, Doshi D, Duh MS. Patterns of relapse and associated cost burden in schizophrenia patients receiving atypical antipsychotics. J Med Econ. 2013;16(11):1290–9.
Karve SJ, Panish JM, Dirani RG, Candrilli SD. Health care utilization and costs among Medicaid-enrolled patients with schizophrenia experiencing multiple psychiatric relapses. Health Outcomes Res Med. 2012;3(4):e183–94.
Crown WH, Neslusan C, Russo PA, Holzer S, Ozminkowski R, Croghan T. Hospitalization and total medical costs for privately insured persons with schizophrenia. Adm Policy Ment Health. 2001;28(5):335–51.
Kozma C, Muser E, Benson C, Mao L, Starr HL, Alphs L. Health resource and criminal justice system costs for young clinical trial patients with schizophrenia and prior incareration by treatment failure status. Value Health. 2015;18(3):A122.
Almond S, Knapp M, Francois C, Toumi M, Brugha T. Relapse in schizophrenia: costs, clinical outcomes and quality of life. Br J Psychiatry. 2004;184(4):346–51.
Zeidler J, Slawik L, Fleischmann J, Greiner W. The costs of schizophrenia and predictors of hospitalisation from the statutory health insurance perspective. Health Econ Rev. 2012;2(1):1–8.
Kilian R, Matschinger H, Becker T, Angermeyer MC. A longitudinal analysis of the impact of social and clinical characteristics on the costs of schizophrenia treatment. Acta Psychiatr Scand. 2003;107(5):351–60.
Daltio CS, Mari JJ, Ferraz MB. Direct medical costs associated with schizophrenia relapses in health care services in the city of São Paulo. Revista de Saúde Pública. 2011;45(1):14–23.
Lin L, Zhao YJ, Zhou HJ, Khoo AL, Teng M, Soh LB, Lim BP, Sim K. Comparative cost-effectiveness of 11 oral antipsychotics for relapse prevention in schizophrenia within Singapore using effectiveness estimates from a network meta-analysis. Int Clin Psychopharmacol. 2016;31(2):84–92.
Zhai J, Guo X, Chen M, Zhao J, Su Z. An investigation of economic costs of schizophrenia in two areas of China. Int J Ment Health Syst. 2013;7(1):26.
Wu J, He X, Liu L, Ye W, Montgomery W, Xue H, McCombs JS. Health care resource use and direct medical costs for patients with schizophrenia in Tianjin, People’s republic of china. Neuropsychiatr Dis Treat. 2015;11:983.
Fitzgerald P, de Castella A, Arya D, Simons WR, Eggleston A, Meere S, Kulkarni J. The cost of relapse in schizophrenia and schizoaffective disorder. Australas Psychiatry. 2009;17(4):265–72.
Lindström E, Eberhard J, Fors BM, Hansen K, Sapin C. A pharmacoeconomic analysis of sertindole in the treatment of schizophrenia in Sweden. Nord J Psychiatry. 2011;65(6):403–13.
Hong J, Windmeijer F, Novick D, Haro JM, Brown J. The cost of relapse in patients with schizophrenia in the European SOHO (schizophrenia Outpatient Health Outcomes) study. Prog Neuro-Psychophys. 2009;33(5):835–41.
Hemels M, Diels J, González B, Jensen R. PMH19 cost of relapse in schizophrenia in Europe: The Constatre Study. Value Health. 2011;14(7):A290.
Gandhi R, Figueroa C. Inpatient burden of childhood schizophrenia in the United States. J Am Acad Child Adolesc Psychiatry. 2016;55(10):S236.
Young-Xu Y, Duh MS, Muser E, DerSarkissian M, Faust E, Kageleiry A, Bhak RH, Fu DJ, Lefebvre P, Shiner B. Impact of paliperidone palmitate versus oral atypical antipsychotics on health care resource use and costs in veterans with schizophrenia. J Clin Psychiatry. 2016;77(10):e1332.
Baser O, Xie L, Pesa J, Durkin M. Healthcare utilization and costs of veterans health administration patients with schizophrenia treated with paliperidone palmitate long-acting injection or oral atypical antipsychotics. J Med Econ. 2015;18(5):357–65.
Kamat SA, Offord S, Docherty J, Lin J, Eramo A, Baker RA, Gutierrez B, Karson C. Reduction in inpatient resource utilization and costs associated with long-acting injectable antipsychotics across different age groups of Medicaid-insured schizophrenia patients. Drugs Context. 2015;4:212267.
Bera R, Offord S, Zubek D, Lau G, Lin J, Baker RA, Karson C. Impact on healthcare resource usage and costs among Medicaid-insured schizophrenia patients after initiation of treatment with long-acting injectable antipsychotics. J Med Econ. 2013;16(4):522–8.
Offord S, Lin J, Mirski D, Wong B. Impact of early nonadherence to oral antipsychotics on clinical and economic outcomes among patients with schizophrenia. Adv Ther. 2013;30(3):286–97.
Offord S, Lin J, Wong B, Mirski D, Baker RA. Impact of oral antipsychotic medication adherence on healthcare resource utilization among schizophrenia patients with medicare coverage. Community Ment Health J. 2013;49(6):625–9.
Stensland M, Watson PR, Grazier KL. An examination of costs, charges, and payments for inpatient psychiatric treatment in community hospitals. Psychiatr Serv. 2012;63(7):666–71.
Desai P, Lawson K, Barner JC, Rascati KL. PMH29 estimation of direct costs of treating schizophrenia for community-dwelling United States residents. Value Health. 2011;14(3):A190–1.
Nicholl D, Akhras KS, Diels J, Schadrack J. Burden of schizophrenia in recently diagnosed patients: healthcare utilisation and cost perspective. Curr Med Res Opin. 2010;26(4):943–55.
Marcus SC, Olfson M. Outpatient antipsychotic treatment and inpatient costs of schizophrenia. Schizophr Bull. 2008;34(1):173–80.
Weiden PJ, Olfson M. Cost of relapse in schizophrenia. Schizophr Bull. 1995;21(3):419–29.
Ascenção R, Gouveia M, Fiorentino F, Alarcão J, Pascoal J, Costa J, Borges M. Hospitalized patients with schizophrenia in Portugal: clinical characterization and costs. Value Health. 2016;19(7):A527.
Zaprutko T, Göder R, Kus K, Rakhman L, Bilobryvka R, Nowakowska E. The cost of inpatient care of schizophrenia and treatment schedules used in German Academic Center: Kiel. Psychiatr Q. 2016;87(4):595–603.
Evensen S, Wisløff T, Lystad JU, Bull H, Ueland T, Falkum E. Prevalence, employment rate, and cost of schizophrenia in a high-income welfare society: a population-based study using comprehensive health and welfare registers. Schizophr Bull. 2015;42(2):476–83.
Henderson C, Knapp M, Yeeles K, Bremner S, Eldridge S, David AS, O’Connell N, Burns T, Priebe S. Cost-effectiveness of financial incentives to promote adherence to depot antipsychotic medication: economic evaluation of a cluster-randomised controlled trial. PloS One. 2015;10(10):e0138816.
Mahlich J, Nishi M, Saito Y. Modeling the budget impact of long-acting injectable paliperidone palmitate in the treatment of schizophrenia in Japan. Clinicoecono Outcomes Res: Clinicoecon Outcomes Res. 2015;7:267–72.
Zaprutko T, Nowakowska E, Kus K, Bilobryvka R, Rakhman L, Pogłodziński A. The cost of inpatient care of schizophrenia in the polish and Ukrainian Academic Centers—Poznan and Lviv. Acad Psychiatry. 2015;39(2):165–73.
Frey S, Linder R, Juckel G, Stargardt T. Cost-effectiveness of long-acting injectable risperidone versus flupentixol decanoate in the treatment of schizophrenia: a Markov model parameterized using administrative data. Eur J Health Econ. 2014;15(2):133–42.
Asseburg C, Willis M, Löthgren M, Seppälä N, Hakala M, Persson U. Hospitalisation utilisation and costs in schizophrenia patients in Finland before and after initiation of risperidone long-acting injection. Schizophr Res Treat. 2012;2012:791468. doi:10.1155/2012/791468.
Mehnert A, Nicholl D, Pudas H, Martin M, McGuire A. Cost effectiveness of paliperidone palmitate versus risperidone long-acting injectable and olanzapine pamoate for the treatment of patients with schizophrenia in Sweden. J Med Econ. 2012;15(5):844–61.
Španiel F, Hrdlicka J, Novák T, Kožený J, Hoeschl C, Mohr P, Motlova LB. Effectiveness of the information technology-aided program of relapse prevention in schizophrenia (ITAREPS): a randomized, controlled, double-blind study. J Psychiatr Pract. 2012;18(4):269–80.
Carswell C, Wheeler A, Vanderpyl J, Robinson E. Comparative effectiveness of long-acting risperidone in New Zealand. Clin Drug Investig. 2010;30(11):777–87.
Munro J, Osborne S, Dearden L, Pascoe K, Gauthier A, Price M. Hospital treatment and management in relapse of schizophrenia in the UK: associated costs. Psychiatrist. 2011;35(3):95–100.
Spill B, Konoppa S, Kissling W, Maino K, Messer T, Heres S. Long-term observation of patients successfully switched to risperidone long-acting injectable: a retrospective, naturalistic 18-month mirror-image study of hospitalization rates and therapy costs. Int J Psychiatry Clin Pract. 2010;14(1):53–62.
Willis M, Svensson M, Löthgren M, Eriksson B, Berntsson A, Persson U. The impact on schizophrenia-related hospital utilization and costs of switching to long-acting risperidone injections in Sweden. Eur J Health Econ. 2010;11(6):585–94.
Zeidler J, Slawik L, Fleischmann J, Greiner W. PMH20 impact and costs of hospitalization in schizophrenia. Value Health. 2010;13(7):A449.
Niaz OS, Haddad PM. Thirty-five months experience of risperidone long-acting injection in a UK psychiatric service including a mirror-image analysis of in-patient care. Acta Psychiatr Scand. 2007;116(1):36–46.
Peiró S, Gómez G, Navarro M, Guadarrama I, Rejas J. Length of stay and antipsychotic treatment costs of patients with acute psychosis admitted to hospital in Spain. Soc Psychiatry Psychiatr Epidemiol. 2004;39(7):507–13.
Spannheimer A, Reitberger U, Clouth J, Lothgren M. Length of hospital stay and associated costs for olanzapine vs. haloperidol in the treatment of schizophrenia relapse in Germany. Eur J Health Econ. 2003;4(2):85–9.
Garattini L, Rossi C, Tediosi F, Cornaggia C, Covelli G, Barbui C, Parazzini F. Direct costs of schizophrenia in Italian community psychiatric services. Pharmacoeconomics. 2001;19(12):1217–25.
Tarricone R, Gerzeli S, Montanelli R, Frattura L, Percudani M, Racagni G. Direct and indirect costs of schizophrenia in community psychiatric services in Italy: the GISIES study. Health Policy. 2000;51(1):1–8.
Anh NQ, Linh BN, Ha NT, Phanthunane P, Huong NT. Schizophrenia interventions in Vietnam: primary results from a cost-effectiveness study. Glob Public Health. 2015;10(sup1):S21–39.
Chen Y, Cheng Y, Shi Q, Yu X, Liu Q, Gu X, Shi J, Montgomery W. Medication use patterns, health-care resource utilization and economic burden for patients with schizophrenia in Beijing, China. Value Health. 2015;18(3):A127.
He X, Wu J, Jiang Y, Liu L, Ye W, Xue H, Montgomery W. Health care resource utilization and direct medical costs for patients with schizophrenia initiating treatment with atypical versus typical antipsychotics in Tianjin, China. BMC Health Serv Res. 2015;15(1):149.
Chang HC, Tang CH, Huang ST, McCrone P, Su KP. A cost-consequence analysis of long-acting injectable risperidone in schizophrenia: a one-year mirror-image study with national claim-based database in Taiwan. J Psychiatr Res. 2012;46(6):751–6.
Verduzco W, Escobedo O, Anaya P. PMH30 hospitalization costs for schizophrenia relapses in a public psychiatric institution. Value Health. 2009;12(3):A178.
Ayer A, Sariöz F, Kanbur B, Yapici A, Demet SM, Tatar F. PMH27 in patient cost of schizophrenia treatment in Turkey. Value Health. 2009;12(3):A177.
Lang HC, Su TP. The cost of schizophrenia treatment in Taiwan. Psychiatr Serv. 2004;55(8):928–30.
Einarson TR, Vicente C, Zilbershtein R, Piwko C, Bø CN, Pudas H, Jensen R, Hemels ME. Pharmacoeconomics of depot antipsychotics for treating chronic schizophrenia in Sweden. Nord J Psychiatry. 2014;68(6):416–27.
National Collaborating Centre for Mental Health. Psychosis and schizophrenia in adults: treatment and management. National Institute for Health and Care Excellence, National Clinical Guideline number 178. http://www.nice.org.uk/guidance/cg178/evidence/full-guideline-490503565. Accessed Jan 2016.
Davies A, Vardeva K, Loze JY, L’Italien GJ, Sennfalt K, Baardewijk MV. Cost-effectiveness of atypical antipsychotics for the management of schizophrenia in the UK. Curr Med Res Opin. 2008;24(11):3275–85.
Geitona M, Kousoulakou H, Ollandezos M, Athanasakis K, Papanicolaou S, Kyriopoulos I. Costs and effects of paliperidone extended release compared with alternative oral antipsychotic agents in patients with schizophrenia in Greece: a cost effectiveness study. Ann Gen Psychiatry. 2008;7(16):1–2.
Beard SM, Maciver F, Clouth J, Rüther E. A decision model to compare health care costs of olanzapine and risperidone treatment for schizophrenia in Germany. Eur J Health Econ. 2006;7(3):165–72.
Edwards NC, Locklear JC, Rupnow MF, Diamond RJ. Cost effectiveness of long-acting risperidone injection versus alternative antipsychotic agents in patients with schizophrenia in the USA. Pharmacoeconomics. 2005;23(1):75–89.
Palmer CS, Revicki DA, Genduso LA, Hamilton SH, Brown RE. A cost-effectiveness clinical decision analysis model for schizophrenia. Am J Man Care. 1998;4:345–55.
Almond S, O’Donnell O. Cost analysis of the treatment of schizophrenia in the UK. Pharmacoeconomics. 1998;13(5):575–88.
Li H, Song X, Yu X. PMH8 a review of consequences of relapse in schizophrenia. Value Health. 2012;15(7):A670.
Thieda P, Beard S, Richter A, Kane J. An economic review of compliance with medication therapy in the treatment of schizophrenia. Psychiatr Serv. 2003;54(4):508–16.
Centre for Mental Health. Pathways to unlocking secure mental health care. London. 2011. http://www.centreformentalhealth.org.uk/pathways-to-unlocking-secure-mental-health-care. Accessed Jan 2016.
Ascher-Svanum H, Nyhuis AW, Faries DE, Ball DE, Kinon BJ. Involvement in the US criminal justice system and cost implications for persons treated for schizophrenia. BMC Psychiatry. 2010;10(1):11. doi:10.1186/1471-244X-10-11.
Robertson AG, Swanson JW, Van Dorn RA, Swartz MS. Economic grand rounds: treatment participation and medication adherence: effects on criminal justice costs of persons with mental illness. Psychiatr Serv. 2014;65(10):1189–91.
Acknowledgements
This study was funded by Janssen-Cilag Ltd. It was not part of a specific programme. Representatives from Janssen have commented on a draft but the authors retained sole control over the design, implementation and reporting of the results.
PM was responsible for the conception of the project and editing of the manuscript. MP undertook the literature searching, extraction of data, regression analysis and drafting of the manuscript .
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
MP reports no conflicts of interest. PM reports no conflicts of interest.
Data availability statement
All data generated or analysed during this study are included in this published article.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Pennington, M., McCrone, P. The Cost of Relapse in Schizophrenia. PharmacoEconomics 35, 921–936 (2017). https://doi.org/10.1007/s40273-017-0515-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40273-017-0515-3