
Abstract
It has been reported that metal exposure is associated with the risk of diabetes, but the results are inconsistent. The relationship between diabetes and a single metal might be attenuated or strengthened due to the complex interactions of metals and the chronic diseases comorbidity (especially in the elderly). However, the evidence of multiple metal exposure effect in participants with diabetes only is limited, particularly in the elderly. This cross-sectional study used a case-control method, involving 188 diabetes patients and 376 healthy participants aimed to evaluate the potential relationships between the concentrations of 9 metals in urine and the risk of diabetes and to access the interactive effects of metals in Chinese community-dwelling elderly. The urine levels of 9 metals (cobalt, zinc, copper, arsenic, molybdenum, cadmium, tellurium, thallium, lead) were detected by inductively coupled plasma mass spectrometry (ICP-MS) in 564 adults recruited from Yinchuan Community Health Service Center (Yinchuan, China). During the baseline survey, the demographic information of the subjects was collected through questionnaire survey, the indexes such as blood pressure, blood lipid and liver function were measured through physical examination. Logistic regression and restricted cubic spline (RCS) analysis were used to explore the associations and dose–response relationships of urine metals with diabetes. To the analysis of multi-metal exposures and diabetes risk, weighted quantile sum (WQS) regression model and the Bayesian Kernel machine regression (BKMR) model were applied. The concentrations of cobalt, zinc, copper, arsenic, molybdenum, cadmium, tellurium, thallium, and lead were higher in the diabetes group (p < 0.05). In logistic regression analysis, we found that the OR values of urinary cobalt, zinc, copper, arsenic, molybdenum, cadmium, tellurium, thallium, and lead quartiles showed an increasing trend. In the single-metal model, the adjusted ORs(95% CI) in the highest quartiles were 2.94(1.72,5.05) for cobalt,5.05 (2.85,8.93) for zinc, 2.28(1.32,3.91) for copper, 1.99(1.15,3.43) for arsenic, 2.61(1.54,4.43) for molybdenum, 2.89(1.68,4.96) for cadmium, 2.52(1.44,4.41) for tellurium, 3.53(2.03,6.12) for thallium, and 2.18(1.27,3.75) for lead compared with the lowest quartile. And in the RCS model, the concentrations of cobalt, zinc, copper, arsenic, molybdenum, cadmium, tellurium, thallium, and lead showed a nonlinear dose–response relationship with diabetes risk (P-overall < 0.05,P-nonlinear < 0.05). The results from multi-pollutant models all indicated that metal mixture was positively associated with the risk of diabetes, and zinc and thallium were the major contributors to the combined effect. Elevated levels of urine cobalt, zinc, copper, arsenic, molybdenum, cadmium, tellurium, thallium, and lead were associated with increased risk of diabetes. There is a positive interaction between zinc and thallium on diabetes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Diabetes mellitus is a group of metabolic diseases caused by carbohydrate, protein, and fat metabolism disorder, insulin secretion or its biological function impairment particularly (Ogurtsova et al. 2017; Stumvoll et al. 2005). It is currently a common chronic non-communicable disease, mainly characterized by hyperglycemia (Bruno 2022; Vaiserman 2015). The 2019 global burden of disease study showed that diabetes rose from the 20th (in 1990) to the 8th (in 2019) leading cause of death (G. D. a. I. Collaborators 2020). And the disability burden caused by diabetes had the highest increase (increase by 147.9% from 1990 to 2019) of all (G. R. F. Collaborators 2020). According to the data released by the International Diabetes Federation (IDF) in November 2021, there were currently 537 million adults (Age between 20–79) with diabetes worldwide, accounting for 10.5% of the world’s population, while the number of Chinese patients was 141 million, accounting for 13% of the Global diabetes patients(International Diabetes Federation 2021). The number of Chinese adults suffering from diabetes ranked first in the world. In addition, the aging trend of diabetes is increasing (Zheng et al. 2018). In China, as the proportion of the elderly over 60 years old increased year by year, the survey from 2015 to 2017 found that the prevalence of diabetes in the elderly population over 60 years old was close to or exceeds 30% (Li et al. 2020). Therefore, the health burden brought by diabetes poses major challenges to individuals, families, and society and has become a serious global public health problem (Zheng et al. 2018). It should be our concern to identify the potential risk factors for health intervention.
Previous studies have demonstrated that poor lifestyle behaviors, environmental hazardous agents, and genetic susceptibility exert a common influence in the development of diabetes. But in recent years, we have found that environmental factors are more important than genetic factors in the pathogenesis of diabetes (Favé et al. 2018). Compared with other environmental pollutants, metals exist widely in the atmosphere, soil, and water (Chowdhury et al. 2016; Rai et al. 2019; B. Wang et al. 2018). However, metals are non-biodegradable in the environment and can exist in the environment continuously, causing serious health problems such as accumulation and toxicity in animals (Rajkowska and Protasowicki 2013). Experimental studies have confirmed that exposure to the toxic metals could cause insulin resistance and abnormal glucose metabolism by inducing oxidation stress, inflammation, and interrupting the enzyme activation (González-Villalva et al. 2016). However, the optimal levels of metals are uncertain and still need to be investigated, since increasing epidemiology studies have suggested that deficiency or excess of metals is associated with diabetes (Ge et al. 2021; Lv et al. 2021; Wang et al. 2020a; Xu et al. 2013; Yang et al. 2017a).
However, most of the current studies have focused on the correlation between single metals and diabetes (He et al. 2020). In our daily life, we often contacted with multiple metals, and we should consider the synergistic effects of them (Ge et al. 2021). Few epidemiology studies have explored the relationships between multiple metal exposures and the prevalence of diabetes, while the results were controversial (Zhang et al. 2022). The inconsistent conclusion of the relationship between metal exposure and diabetes might be due to the different metal exposure levels of different study populations (Feng et al. 2015; Ji et al. 2021; Zhang et al. 2022). For example, a study of occupational population found that the copper and zinc levels in urinary of coke oven workers were positively associated with the risk of diabetes and hyperglycemia (Liu et al. 2016). However, in a general population study in rural China, nonlinear inverted U-shaped associations were found between fasting blood glucose levels and zinc, lead, and copper in urine(Zhang et al. 2022). People are typically exposed to multiple metals in their daily lives, and the relationship between diabetes and a single metal may be weakened or strengthened due to the complex interactions between metals and multiple chronic diseases in the population (especially in the elderly) (Guo et al. 2022).
However, evidence on the relationship between multiple metal exposures and the prevalence of diabetes is limited, especially in the elderly. Therefore, based on the elderly cohort in Yinchuan, we performed a cross-sectional analysis to explore the relationships between 9 metal levels in urine and the prevalence of diabetes only in community-dwelling elderly of Yinchuan in China and access the interactive effects of metals in the diabetic population.
Methods and Materials
Study Population
This cross-sectional study randomly selected two community health centers in two districts and two counties of Yinchuan City from June 2020 to October 2020 and recruited 500 subjects aged 60 years or older in each community health center through routine physical examination, a total of 4144 people. We excluded other patients with chronic complications from the baseline population and obtained 188 patients with diabetes alone. At the same time, we included age (±5 years) and gender to match diabetic patients with healthy individuals who were examined at the same time with a frequency of 1:2. Therefore based on the baseline of the Yinchuan community-dwelling elderly cohort (Ningxia, China), the study population included 188 diabetic patients and 376 healthy individuals. By calculating the cross-sectional sample size, the population meets the criteria. In the inclusion criteria, we excluded participants with incomplete data, cerebrovascular disease, neurological disease and coronary heart disease, malignant tumor, hypertension, hyperlipidemia, and related occupational metal exposure history.
This study was also approved by the Ethics Committee of Ningxia Medical University, No.2020–099. All study subjects have signed the informed consent form. We collect data anonymously and also desensitize sensitive information. Adopt methods such as encrypted storage and restricted access to ensure that research data is not illegally obtained and used.
Information Collection
After obtaining informed consent, all the participants underwent questionnaire survey, physical examination, and biological sample collection. Questionnaires were conducted by the trained interviewers. The general questionnaire included demographics and lifestyle (diet, smoking, alcohol, physical activity).We recorded the participants’ history of hypertension, hyperlipidemia, coronary heart disease, and other disease from the Electronic Healthcare Record system. All participants underwent a physical examination which included anthropometry, heart rate and blood pressure measurements, and examination of tonsil, lung, heart, liver, spleen, and kidney. Standing height, body weight, waist circumference, and hip circumference were measured when the participants standing with light indoor clothing and without shoes. 10 mL early morning urine for each participant was collected, aliquoted, and stored at − 20 °C. A total of 10 mL fasting blood sample for each participant [1 × 5 mL ethylene diamine tetra acetic acid (EDTA) anticoagulation tubes and 1 × 5 mL coagulation tube for serum] was collected. Biochemical analysis of blood included fasting blood glucose, blood lipids, alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TBIL) and serum creatinine (Scre) were immediately determined in the clinical laboratory. The remaining blood was separated into plasma (3 tubes, 500 μL per tube), serum (3 tubes, 500 μL per tube), and whole blood cells (1 tubes, 500 μL per tube) and then stored at − 80 °C for further analyses.
Definition of Diabetes
Diabetes: According to the Chinese Guidelines for the Prevention and Treatment of Type 2 Diabetes (2020 Edition) Introduction reference, participants with one of the following items were defined as diabetes:
Random blood glucose ≥ 11.1 mmol/L;
Fasting blood glucose ≥ 7.0 mmol/L or diagnosed with diabetes and taking medication;
Oral glucose tolerance test 2 h blood glucose (OGTT) ≥ 11.1 mmol/L;
Glycated hemoglobin (HbA1c) ≥ 6.5%.
Determination of Metal Levels in Urine
Urinary levels of 9 metals including cobalt (Co), zinc (Zn), copper (Cu), arsenic (As), molybdenum (Mo), cadmium (Cd), tellurium (Te), thallium (Tl), and lead (Pb) were determined by Inductively Coupled Plasma Mass Spectrometry (ICP-MS, Agilent 7800x). Before determination, frozen urine sample were thawed at room temperature for dissolution and centrifuged at 3000r/min and 4 °C for 3 min. 0.5 mL of supernatant was absorbed into the polytetrafluoron microwave digestion tank and 2.5 mL 67% (v/v) HNO3 (Kermel, Tianjin China) was added. The tank cover was tightened by putting the tank into the microwave digestion instrument (CEM, MARS 6 CLASSIC) evenly and symmetrically for 40 min. After the completion of cooling, the tank was opened and placed into the electric acid driving instrument (LabTech) to drive the acid to 0.5 ml (130 °C, 150 min). Then it was transferred to the polypropylene centrifugal tube diluting with ultrapure water (18.2MΩ) to 2.5 ml. Finally it was mixed and determined. Undetected samples were filled with data at 1/2 of the detection limit.
Quality Control/Quality Assurance
To ensure the accuracy of the present method, one urine quality control sample (ClinChekR-Control urine, level II) and three random blank samples were processed every 28 samples. Besides, the recovery values for 9 metals ranged from 85.20 to 110.00% (Supplemental Table S1), with the intra-assay standard deviations (RSDs) ranging from 1.04 to 5.20% and the inter-assay standard deviations (RSDs) ranging from 2.06 to 13.21% (Supplemental Table S2). The limits of detection (LODs) for all metals were in the range of 0.00113 µg/L(Co) to 0.8589 µg/L(Zn) (Supplemental Table S3). The detection rates were in the range of 87.93% (Te) to 99.50% (Mo). The undetected samples were assigned a value of one-half the LOD. The concentrations of urinary creatinine (mQi-crograms per liter, g/L) were measured to adjust for urine dilution by automated clinical chemistry analyzer (Beckman Coulter, Au480).
Covariates
In this study, we selected the covariates we are interested in on the basis of reference to previous literature (Guo et al. 2022; Huang et al. 2022). The covariates of interest included age (continuous variable), sex(male/female), smoking status, alcohol drinking status, dietary habit, exercise frequency, body mass index, continuous variable (BMI), total cholesterol, continuous variable (TC), triglyceride, continuous variable (TG), high-density lipoprotein cholesterol, continuous variable (HDL-c), low-density lipoprotein cholesterol, continuous variable (LDL-c), systolic blood pressure, continuous variable (SBP), and diastolic blood pressure, continuous variable (DBP). Based on the baseline information in questionnaires, smoking status was further categorized into never, former, and active; alcohol drinking status was further categorized into never, < once a week, ≥ once a week, and everyday; dietary habit was further categorized into meat-vegetables balanced diet, plant-based diet and meat-based diet; exercise frequency was further categorized into every day, ≥ once a week, < once a week, and never.
Statistical Analysis
General demographic information and metal concentrations were described as mean ± standard deviation, frequencies and percentages, and medians. Differences between diseased and non-diseased groups were analyzed by t-test, chi-square test (When the theoretical frequency < 5, Fisher’s exact test was used), and Wilcoxon rank-sum test based on data distribution. All metal concentrations were natural log-transformed to approximate a normal distribution. And Spearman rank correlation analysis was used to evaluate the correlation between various metals in urine. To control for concentration dilution in urine, we also normalized by adjusting for creatinine.
We divided the urinary metal concentrations into quartiles of the control group, and the single-metal logistic regression model was conducted to estimate the odds ratios (ORs) with 95% confidence intervals (CIs) for the relationships between urinary metals and the prevalence of diabetes. Model 1 has not been adjusted. The adjusting factors of model 2 included age, gender, smoking status, drinking status, dietary habits, exercise frequency, BMI (kg/m2), TC, TG, LDL, HDL, SBP and DBP, etc. The trend test was performed using Logistic regression analysis. Moreover, relationships of urine metal levels with diabetes were further validated by the linear model in which metal levels were evaluated as continuous variables. The ln-transformed urine metal levels were divided by ln-transformed IQRs (interquartile ranges) before analysis. The multicollinearity of the model was calculated using the variance inflation factor (VIF). The dose–response relationship between each metal concentration and diabetes was analyzed using the RCS regression model. The 10th percentiles were assigned as the reference values (OR = 1.00), with knots at the 10th, 50th, and 90th percentiles of the concentrations, respectively.
We also applied WQS regression models to assess the effect of urinary metal mixture, and the weight of each metal on incident diabetes risk. WQS index comprised a weighted sum of individual metal concentrations, which were ln-transformed. A weighted index further evaluated the importance of each variable after considering the collinearity or multi-dimensionality of urinary metal. After bootstrapping 500 times, the associations between WQS indices and risk of incident diabetes were evaluated with adjustment for the same covariates as in Model 2. Furthermore, because WQS regression cannot accommodate the positive and negative modes simultaneously, we run the models twice in both positive and negative modes, and the variable weights of the assumed mode were deemed valid only when the association between the WQS index and incident diabetes risk was statistically significant. In this study, we randomly partitioned the full dataset into 40% of the data were applied as the test set and the remaining 60% as the validation set, and repeated WQS regression 100 times to simulate a distribution of validated results from the resampling population.
Because of the potential for interaction effects and nonlinear relationships between elements, we used a BKMR model to assess the overall impact of multiple metals in complex environments. Its advantage is that it allows for the existence of nonlinear effects and interactions, and can flexibly evaluate the exposure response relationship. We used the Markov Chain Monte Carlo algorithm for 10,000 iterations through the BKMR model, treating the diabetes parameter as a dichotomous outcome. In this model, statistics quantifying the corresponding exposure measures are available to provide insight into the cumulative effects of the mixtures. The following estimates were reported: (a) the overall association between metal mixtures and each outcome when fixing the metal mixtures at a particular percentile compared with the median; (b) the association between an interquartile range (IQR, from 25 to 75th percentile) increase in each individual metal exposure and each outcome when fixing all other metal exposures at 25th, 50th or 75th percentiles; (c) the univariate exposure–response relationship between each metal exposure and each outcome when fixing all other metal exposures at their medians; (d) when all other metals are fixed at the median value, the bivariate exposure dose–response relationship between one metal and the outcome with the concentration level of the other metal at the 25th, 50th, and 75th percentiles, respectively.
This study analyzed using R4.1.3's “gWQS”package and “bkmr” package, as well as Stata MP17.0, and two-sided P < 0.05 was considered statistically significant.
Results
Characteristics of Study Population
Table 1 summarizes the general characteristics of the 564 participants (188 diabetics and 376 healthy subjects). The mean age of the diabetic group was 70.93 ± 4.87 years, and the mean age of the healthy group was 70.21 ± 5.13 years. The male-to-female ratio was the same in both groups. Table 1 shows that there were no differences at baseline in age, sex, alcohol drinking status, exercise frequency, TC, LDL-c,HDL-c, and blood pressure between cases and controls. However, there were significant differences between the cases and controls groups in smoking status, dietary habit, BMI, and TG (All P < 0.05).
Distributions of the Urinary Metals
The concentrations of 9 urinary metals standardized by creatinine (μg/g Cr) among the two groups are displayed in Table 2. After adjustment for urinary creatinine levels, we found higher urinary Zn, Mo, Te, As and Cu exposures and lower Co, Cd, Tl and Pb exposures. Compared with the control group, the urine samples of the diabetes group had significantly higher concentrations of Co, Zn, Cu, As, Mo, Cd, Te, Tl, and Pb (All P < 0.05).
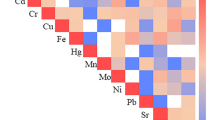
Correlation analysis was performed after ln-transformation of creatinine-corrected metal concentrations. Supplemental Fig.S1 depicts the pairwise metal correlation coefficients calculated by Spearman’s rank correlation analysis. Almost all metals show positive correlations ranging from 0.22 to 0.57. The correlation between molybdenum and arsenic was the strongest (r = 0.57, P < 0.05).
Association of Metals with Diabetes Prevalence
The relationship between urinary metal concentration levels and the prevalence of diabetes is shown in Table 3. In model 2 with additional adjustment, the adjusted ORs (95% CI) in the second quartile were 1.93(1.10,3.38) for Tl and 1.83 (1.06,3.17) for Pb in the second quartile, respectively, compared with the lowest quartile. In model 2, the adjusted ORs (95% CI) were 2.44(1.38,4.29) for Zn, 1.90(1.11,3.23) for Mo, 2.68(1.53,4.70) for Te, 2.13(1.21,3.72) for Tl, and 1.91(1.10,3.32) for Pb in the third quartile, respectively, compared with the lowest quartile. In model 2, the adjusted ORs (95% CI) in the fourth quartile were 2.94(1.72,5.05) for Co, 5.05(2.85,8.93) for Zn, 2.28(1.32,3.91) for Cu, 1.99(1.15,3.43)for As, 2.61(1.54,4.43) for Mo, 2.89(1.68,4.96) for Cd, 2.52(1.44,4.41) for Te, 3.53(2.03,6.12) for Tl, and 2.18(1.27,3.75) for Pb, respectively, compared with the lowest quartile.
The adjusted P values for trend test were significant for Co, Zn, Cu, As, Mo, Cd, Te, Tl, and Pb. The adjusted linear model also indicated positive correlation of Co, Zn, Cu, As, Mo, Cd, Te, Tl, and Pb with diabetes risk (Table 3). The VIF values of urinary Co, Zn, Cu, As, Mo, Cd, Te, Tl, and Pb were 1.36, 1.36, 1.36, 1.36, 1.35, 1.36, 1.36, 1.36, and 1.36, respectively.
Dose–Response Relationship Between Urinary Metals and Diabetes Risk
We used restricted cubic splines to assess the dose–response relationship of each metal with diabetes risk. Non-linear associations and increasing trends with diabetes risk were demonstrated, as shown by the estimated curves in Fig. 1 (Co:P-overall < 0.001, P-nonlinear = 0.015;Zn: P-overall < 0.001,P-nonlinear < 0.001;Cu:P-overall = 0.002,P-nonlinear < 0.001;As:P-overall = 0.007, P-nonlinear = 0.018;Mo:P-overall < 0.001,P-nonlinear < 0.001;Cd:P-overall < 0.001,P-nonlinear < 0.001; Te: P-overall < 0.001,P-nonlinear < 0.001; Tl:P-overall < 0.001, P-nonlinear = 0.001). Regarding the reverse U-shaped relation between predicted Pb and diabetes risk, the plot showed a substantial increase of the risk within the lower range of predicted Pb, which reached the highest risk around 2.15 (μg/g Cr) and then reduction thereafter(P-overall < 0.001,P-nonlinear < 0.001).

The restricted cubic spline for the relationships between urine metal concentrations and the risk of diabetes. The ORs (red lines) and 95% confidence intervals (red range) were calculated based on the restricted cubic spline models for the concentrations of urine metals. The 10th percentiles were set as the reference values, with knots set at 10th, 50th, and 90th percentiles of the urine metals. (A) The RCS for the relationships between Co and the risk of diabetes. (B) The RCS for the relationships between Zn and the risk of diabetes. (C) The RCS for the relationships between Cu and the risk of diabetes. (D) The RCS for the relationships between As and the risk of diabetes. (E) The RCS for the relationships between Mo and the risk of diabetes. (F) The RCS for the relationships between Cd and the risk of diabetes. (G) The RCS for the relationships between Te and the risk of diabetes. (H) The RCS for the relationships between Tl and the risk of diabetes. (I) The RCS for the relationships between Pb and the risk of diabetes
Analysis of Multi-Metal Exposures and Diabetes Risk Using WQS Model
We first used Wilcoxon rank-sum test to identify the important diabetes-related elements in metals mixture. A total of 9 metals (Co, Zn, Cu, As, Mo, Cd, Te, Tl and Pb) have all been verified to be significantly with diabetes. Subsequently, we included metals in the multivariate adjusted logistic regression analysis by quartile. Statistical test for linear trends was conducted by modeling median values of metals quartiles as a continuous variable with adjustment for the same covariates. The result indicated that there was a significant linear trend between metals and diabetes risk (p for trend < 0.05). Moreover, we employed WQS regression models to examine the relationship between metal mixtures and diabetes risk. When analyzing the positive relationship between metal mixture and diabetes, a quartile increase in WQS index was significantly associated with diabetes risk (OR 2.77, 95% CIs 1.92, 4.01). As shown in Fig. 2A and Supplemental Table S4, the WQS index was predominated by Zn (0.265), followed by Tl(0.222), Te(0.212) and Mo(0.134). When analyzing the negative relationship between metal mixture and diabetes risk, a quartile increase in WQS index was significantly associated with diabetes risk (OR 2.01; 95% CI 1.47, 2.76), and Cu made the largest single contribution (0.304) followed by Co(0.297), As(0.253), and Pb(0.146)(Fig. 2B).

The weights of each metal in positive and negative WQS model regression index for cardiovascular disease. The model was adjusted for age, sex, smoking status, alcohol drinking status, dietary habit, exercise frequency, BMI, TC,TG, HDL-c, LDL-c,SBP, and DBP. The x-axis represents the relative weight of the metal. A Positive weight, B Negative weight
Analysis of Multi-Metal Exposures and Diabetes Risk Using BKMR Model
First, the posterior inclusion probability (PIP) values of each metal exposure obtained from the BKMR model are summarized in Supplemental Table S5. Results showed that Zn had the highest PIP in the total population (PIP = 1.000), followed by Tl(0.642) and Pb(0.574) above the threshold value of 0.5. Furthermore, we constructed BKMR models to evaluate the joint effects of urinary metal levels on incident diabetes risk. The effects of mixed metals, a single metal, and metal-to-metal interaction on diabetes risk under the multi-metal exposure scenario are shown in Fig. 3. The BKMR model was used for the global correlation analysis of the mixture. Figure 3A shows the estimated difference in the probit of incident diabetes hazard when all the predictors are fixed to different percentiles, as compared with when they are all fixed to the 50th percentile, supporting a strong and linear positive association of the whole mixture with diabetes risk. Figure 3B shows the estimated change in diabetes risk as a particular metal increased from the 25th percentile to the 75th percentile when other metals were fixed at different percentiles (25th, 50th, or 75th percentile). We found that Zn and Tl displayed a positive and significant effect in this study. The association between Zn and Tl and diabetes risk appears stronger at lower percentiles of other pollutants. In addition, we found that the effects of Zn and Tl on diabetes risk decreased as other metals both increased from their 25th to their 75th percentiles. To further investigate the potential nonlinear exposure–response relationship between specific metals and diabetes risk when other metals remained at the median concentration, we estimated both univariate and bivariate exposure–response functions. Figure 3C demonstrates the univariate exposure–response functions and 95% credible intervals (shaded area) for each pollutant with the other metals fixed at the median values. Results showed that the single-metal exposure–response relationship was basically consistent with the restricted cubic splines model. Zn, Tl, and Te might have a potential positive nonlinear relationship with diabetes risk and Pb might have a reverse U-shaped nonlinear relationship with the diabetes risk. Finally, we assessed the bivariate exposure–response functions for the metals to investigate the possible interactions (Fig. 3D). The slopes for each pollutant are similar at varying levels of the other pollutants, suggesting a lack of statistically significant interaction between individual pollutants. When the concentrations of other metals were fixed at the median level, we found the interactions between urinary Tl with Zn on diabetes risk with the slope changed for Tl when Zn increased from 25 to 75th percentile. The Tl exposure–response curve gradually became steeper with the increase in Zn concentration, indicating that a potential positive interactive effect possibly occurred between Tl and Zn.


Associations between urine metals and diabetes risk in the BKMR model. All of the models have been adjusted for age, sex, smoking status, alcohol drinking status, dietary habit, exercise frequency, BMI, TC,TG, HDL-c, LDL-c,SBP, and DBP. ‘Est’ stands for ‘estimate,’ which means that the estimates of the effects include the overall, individual, and interactive effects of different metals on diabetes risk when the metal levels change. ‘Expose’ stands for metal exposure levels. Here, we use the z-score for all the exposures to have the same scale. A Overall effect of mixture estimates and 95% credible interval on diabetes risk. Estimate can be interpreted as the contribution of predictors to the response. B Single-pollutant association with diabetes risk. Association (estimate and 95% credible intervals) of each metal increased from the 25th percentile to the 75th percentile with diabetes risk was observed when other metals in the mixture have been fixed at the 25th, 50th, and 75th percentiles. Estimate can be interpreted as the contribution of predictors to the response. C The univariate concentration–response functions with 95% confidence bands (shaded areas) for each metal with the other pollutants fixed at the median. Estimate can be interpreted as the contribution of predictors to the response. D Interaction effect of urinary metal mixture on diabetes. Bivariate exposure–response functions for each of the metal presented on the upper coordinate axis when the other metal presented on the right longitudinal axis holding at different quantiles (25th, 50th, and 75th percentiles) and the other metals were held at the median. Estimate can be interpreted as the contribution of the predictors to the response
Discussion
During the past decades, extensive studies have evaluated the diabetes risk effect of long-term exposure to metals. However, few studies excluding other chronic disease comorbidity factors and investigated the joint effects of pollutant mixture in diabetes risk.
In this study, multiple statistical strategies were implemented to comprehensively assess the effects of individual and mixed heavy metal exposures on diabetes risk and to identify the metal elements in mixture that contribute significantly to the positive association. We found that urine Co, Zn, Cu, As, Mo, Cd, Te, Tl, and Pb were positively related to diabetes risk, individually and as a mixture. The dose–response relationships for the above metals were also validated in the RCS model, and the results were also stable for mixed exposure and dose–response relationships. The major contributors to the diabetes associations of the mixture, however, in WQS and BKMR models, were Zn and Tl. A potential interaction effect between Zn and Tl was also observed in participants.
Zinc
Zinc is known to be an essential trace element for human growth and development, with important catalytic and regulatory functions (Mammadova-Bach and Braun 2019). Zinc cannot be stored in the body, so it requires daily intake to maintain basal levels and support all its functions (Bonaventura et al. 2015). The highest zinc content is in the islets, and zinc accumulation in the cellular granules is regulated by Zn T8, the most highly expressed zinc transporter in pancreatic tissue and the product of the SLC30A8 gene, which is responsible for transporting zinc from the cytoplasm to the insulin secretory granules (Cruz et al. 2018). It was found that Zn T8-deficient mice had impaired pancreatic β-cell function, reduced insulin secretion, low circulating insulin levels, and impaired glucose tolerance (Wijesekara et al. 2010). Therefore, diabetes, insulin, and zinc have a complex relationship. Zn deficiency leads to decreased insulin stability, thereby affecting the body’s plasma glucose level (Cruz et al. 2018). Therefore, diabetic patients may take zinc-containing drugs in order to improve the insulin levels and control blood glucose, resulting in high urinary zinc levels in the body (Nazem et al. 2019).
The results of a cohort study of middle-aged women also showed that women with excessive urinary zinc may have an increased risk of diabetes (Wang et al. 2020b). In the present study, a nonlinear positive correlation was observed between urinary Zn and diabetes risk, which was consistent with the results of previous studies (Kazi et al. 2008; Yang et al. 2017b). This mechanism might be related to the loss of zinc in pancreatic beta cells, resulting in decreased insulin secretion (Soleimanpour et al. 2010). Second, studies have confirmed that zinc excretion is significantly increased in diabetic patients, and oral zinc supplementation is expected to provide adequate benefit and protection in diabetic patients in this condition, and zinc supplementation in type 2 diabetic patients increases serum zinc levels; improved blood glucose control and antioxidant capacity had beneficial effects, reduced the concentration of glycated hemoglobin, and increased superoxide dismutase (superoxide dismutase, SOD) expression level (Nazem et al. 2019). However, high zinc intake has also been proven to increase the mortality rate of the Chinese population, leading to the occurrence of a series of diseases (Shi et al. 2017).
Thallium
Thallium is a well-known highly toxic heavy metal. Because of its odorless, tasteless, and water-soluble properties, the general population is under the low-dose exposure through the consumption of contaminated water and food, as well as skin or respiratory inhalation of polluted air chronically in their daily life (Kemnic and Coleman 2022). As one of the most harmful heavy metals to mammals and the priority pollutant determined by the United States Environmental Protection Agency, Tl, is considered to be more toxic than arsenic, nickel, mercury, lead, or cadmium (Rodríguez-Mercado and Altamirano-Lozano 2013).
However, there is some research evidence that thallium toxicity could induce reaction oxygen species (ROS) formation, and the increased oxidative stress could cause tissue damage and organ dysfunction (Wu et al. 2019). Oxidative stress has been widely proposed to be one of the underlying pathogenic mechanisms for insulin resistance and dysfunction of β-cell (Jiang et al. 2018). The results of animal experiments indicate that the pancreas may be the target organ of thallium toxicity, because the pancreas is one of the organs with the highest thallium content (Jiang et al. 2018). In addition, hyperglycemia was also noted in the case reports of acute thallium poisoning (Zhu et al. 2019).
There are some research epidemiological studies that have shown that thallium exposure in pregnant women's urine may be a risk factor for gestational diabetes (QQ Zhang et al. 2021; Zhu et al. 2019). Based on the evidences above, we think there might be an association between thallium exposure and diabetes risk. This is in agreement with the research results of ours. But, current epidemiological data concerning the health effects from human Tl exposure is still insufficient.
In our study, the BKMR model is used to explore the interaction between urinary metals and diabetes risk. Our results showed that urinary zinc and thallium levels played a positive interactive role in the development of diabetes. Some studies have shown that trace thallium can be detected in zinc sulfide and other mixtures and can lead to bioaccumulation (Pavoni et al. 2017). However, the epidemiological evidence on the impact of zinc and thallium interaction on human health is still insufficient. Therefore, more in vivo and in vitro experiments are needed to verify this result. In view of this limited and epidemiological evidence, as well as the high variability and heterogeneity of zinc and thallium exposure levels in different studies, further studies are still needed to clarify the true individual and interactive effects of zinc and thallium in urine on diabetes.
Lead
Lead is a common environmental toxic metal (B. Liu et al. 2016). As a ubiquitous heavy metal, lead is widely present in the atmosphere, soil, water, and food, and easily enters the human body through the digestive tract, respiratory tract, and skin and has health effects on the human body (Ravipati et al. 2021). Some researchers have investigated the relationship between lead exposure and the prevalence of diabetes, and believe that lead exposure may promote the occurrence and development of diabetes (Leff et al. 2018).
A possible mechanism is that Pb can activate the expression of genes related to glucose metabolism, thereby increasing the activity of hepatic gluconeogenesis enzymes, interfere with insulin secretion, eventually lead to elevated blood glucose (Tyrrell et al. 2017). There is strong evidence that lead can also cause oxidative stress, thereby promoting insulin resistance and blood glucose (Rehman et al. 2018). This is consistent with our findings. However, in the present study, we found through the univariate effect of the BKMR model that when Pb increased to a certain level, there would be a hypoglycemic effect, which may be related to the co-exposure of Pb and other metals, which is similar to Jing Zhang’s study (J. Zhang et al. 2022). However, the specific reasons for this phenomenon remain unclear.
Other Metals
Copper is the active component of many enzymes in human body and participates in various physiological activities and metabolic processes (B. Liu et al. 2016). However, excessive copper may catalyze the production of toxic reactive oxygen species, thereby damaging cells (Scheiber et al. 2013). The results of Feng et al. showed that the increase of urinary copper level was significantly associated with the increased risk of diabetes (OR = 1.770, 95% CI 1.107–2.831) (Feng et al. 2015). This was consistent with the positive correlation results obtained by our univariate regression model. The restricted cubic splines of this study also reflect the linear relationship. A large number of studies on diabetes have found that copper concentration was related to the occurrence and development of diabetes (Qiu et al. 2017). Previous studies have also found that copper was positively correlated with insulin resistance, which may be the cause of copper-induced abnormal blood glucose (Kim and Song 2014). In addition, some studies have suggested that copper excess could produce oxidative stress and become a risk factor for the onset and progression of type 2 diabetes (Bjørklund et al. 2020).
As a toxic element, cadmium exposure can cause a variety of metabolic disorders, accompanied by an imbalance of glycolipid homeostasis (Sabir et al. 2019). In the study of Hong Huihui et al., it was found that drinking water cadmium exposure increased blood glucose levels in C57/6 J mice, thereby reducing serum insulin levels, causing glucose intolerance, and inhibiting insulin expression. This study demonstrated the metabolic toxicity of cadmium exposure to pancreatic beta cells at the metabolomic level and provided new clues for the occurrence and development of cadmium exposure and diabetes (Hong et al. 2022). It also provides mechanistic evidence for our analysis results.
In a study on the relationship between urinary arsenic and insulin resistance, it was found that total urinary arsenic exposure may be related to insulin resistance (Zhou et al. 2022). Qiang Zhang et al. found that efficient arsenic metabolism was associated with higher odds of diabetes in the results of a baseline survey of the Chinese Arsenic and Non-Infectious Diseases Cohort (AsNCD)(Q Zhang et al. 2020). Urinary dimethyl arsenic acid interacts with individual factors to synergistically affect the occurrence of diabetes in Chinese population. In conclusion, this study also verified that our analysis results were consistent with them.
Our study found that Co and Mo levels were strongly correlated with increased diabetes risk in participants. Jingli Yang et al. also found that significant sex-specific and dose–response relationships were observed between urinary metals (Co and Mo) and diabetes-related indicators (J. Yang et al. 2023). According to Lai et al., Co could lead to insulin resistance and diabetes at low levels (Lai et al. 2018). Moreover, studies have also found that Co toxicity may lead to mitochondrial dysfunction, which also plays a key role in the development of diabetes (Rovira-Llopis et al. 2017). On the other hand, some studies have found that cobalt has a potential hypoglycemic effect and can prevent the development of diabetes (Nomura et al. 2005). Therefore, patients with diabetes may take cobalt containing drugs to increase the solid content in urine.
Molybdenum is a transition metal element, which is a necessary trace element for human body, animals, and plants. Xiao et al. found that high urinary molybdenum concentration will increase the risk of diabetes (Xiao et al. 2018). Rotter et al. found that molybdenum concentration was positively correlated with insulin level (Rotter et al. 2015). Molybdenum is also one of the basic components of xanthine oxidase and aldehyde oxidase in the liver and intestine of animals. But the enhancement of xanthine oxidase activity may lead to uric acid accumulation and reactive oxygen species-related diseases, such as hyperuricemia and diabetes (Ichida et al. 2012; J. Yang et al. 2023). In this study, the risk of diabetes is also positively correlated with the concentration of molybdenum in urine.
Our study found that high Te levels were strongly correlated with increased diabetes risk in participants. Qing Liu et al.’s study showed that cadmium telluride quantum dots (CdTe QDs) can increase reactive oxygen species (ROS) in hepatocytes after being taken up by hepatocytes, which triggers a significant mitochondrial-dependent apoptotic pathway, leading to hepatocyte apoptosis (Q. Liu et al. 2022). In the previous review, we also found that the regulators of apoptosis signaling events in hepatocytes can modulate insulin signaling pathways and that mediators of insulin resistance in turn influence liver cell apoptosis. The liver is a central regulator of glucose homeostasis and stores or releases glucose according to metabolic demands (Gjorgjieva et al. 2019; Schattenberg & Schuchmann 2009). Therefore, liver injury may lead to glucose homeostasis imbalance and increase the risk of diabetes. In conclusion, this proves that telluride may cause glucose homeostasis imbalance through hepatocyte apoptosis, thus potentially leading to an increased risk of diabetes. However, more epidemiological evidence is still lacking.
In this study, first, to better controlling interference of confounding factors (especially chronic diseases comorbidity), we conducted a cross-sectional study after excluding the subjects of other chronic diseases except for diabetes. Second, we assessed the impact of metal mixtures, single metals, and metal-to-metal interactions on diabetes risk levels when exposed to multiple metals and used BKMR models to analyze the exposure–response relationship between each metal and risk of disease relation. Finally, this study investigated the association of multiple metal exposure with diabetes in urban areas of northwestern China. It could serve as preliminary evidence for the effect of multiple metal exposure on diabetes in the population in the region. However, our current study also has many limitations. First, we were unable to establish a causal relationship between metal exposure and diabetes outcomes due to the limitations of the cross-sectional study. Secondly, due to the inclusion and exclusion factors, the sample size of this study was relatively small. The results would be more reliable if more samples could be obtained.
Conclusions
In summary, according to our findings, environmental exposures to Co, Zn, Cu, As, Mo, Cd, Te,Tl and Pb may be associated with an increased risk of diabetes, with zinc and thallium in particular being the most closely related. In addition, there is an interaction between Zn and Tl on the risk of diabetes. The underlying mechanisms of this interaction may be related to similar biological transport modalities, signaling pathways, or other competition/synergistic effects of metals. Future studies should be conducted to explore the effects and mechanisms of metal–metal interactions on the etiology of diabetes.
Due to the increasing incidence of diabetes in China and the ubiquitous metal exposure in people's daily life and production, this study has important public health implications and provides evidence for establishing elemental intake and environmental standards for the elderly population in this region.
Data Availability
The datasets generated during and/or analyzed during the current study are not publicly available due to limited authorizations from the authors but are available from the corresponding author on reasonable request.
References
Bjørklund G, Dadar M, Pivina L, Doşa M, Semenova Y, Aaseth J (2020) The role of zinc and copper in insulin resistance and diabetes mellitus. Curr Med Chem 27(39):6643–6657. https://doi.org/10.2174/0929867326666190902122155
Bonaventura P, Benedetti G, Albarède F, Miossec P (2015) Zinc and its role in immunity and inflammation. Autoimmun Rev 14(4):277–285. https://doi.org/10.1016/j.autrev.2014.11.008
Bruno A (2022) Pre-diabetes, diabetes, hyperglycemia, and stroke: bittersweet Therapeutic Opportunities. Curr Neurol Neurosci Rep 22(11):781–787. https://doi.org/10.1007/s11910-022-01236-0
Chowdhury S, Mazumder M, Al-Attas O, Husain T (2016) Heavy metals in drinking water: occurrences, implications, and future needs in developing countries. Sci Total Environ. https://doi.org/10.1016/j.scitotenv.2016.06.166
Collaborators, G. D. a. I. (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet (London, England), 396(10258), 1204-1222. doi:https://doi.org/10.1016/s0140-6736(20)30925-9
Collaborators, G. R. F. (2020). Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet (London, England), 396(10258), 1223-1249. doi:https://doi.org/10.1016/s0140-6736(20)30752-2
Copyright © 2022, StatPearls Publishing LLC.
Cruz K, de Oliveira A, Morais J, Severo J, Mendes P, de Sousa Melo S, Marreiro D (2018) Zinc and insulin resistance: biochemical and molecular aspects. Biol Trace Elem Res 186(2):407–412. https://doi.org/10.1007/s12011-018-1308-z
Favé M, Lamaze F, Soave D, Hodgkinson A, Gauvin H, Bruat V, Awadalla P (2018) Gene-by-environment interactions in urban populations modulate risk phenotypes. Nat Commun 9(1):827. https://doi.org/10.1038/s41467-018-03202-2
Feng W, Cui X, Liu B, Liu C, Xiao Y, Lu W, Wu T (2015) Association of urinary metal profiles with altered glucose levels and diabetes risk: a population-based study in China. PloS one 10(4):e0123742. https://doi.org/10.1371/journal.pone.0123742
Ge X, Yang A, Huang S, Luo X, Hou Q, Huang L, Yang X (2021) Sex-specific associations of plasma metals and metal mixtures with glucose metabolism: An occupational population-based study in China. Sci Total Environ 760:143906. https://doi.org/10.1016/j.scitotenv.2020.143906
Gjorgjieva M, Mithieux G, Rajas F (2019) Hepatic stress associated with pathologies characterized by disturbed glucose production. Cell Stress 3(3):86–99. https://doi.org/10.15698/cst2019.03.179
González-Villalva A, Colín-Barenque L, Bizarro-Nevares P, Rojas-Lemus M, Rodríguez-Lara V, García-Pelaez I, Fortoul T (2016) Pollution by metals: Is there a relationship in glycemic control? Environ Toxicol Pharmacol 46:337–343. https://doi.org/10.1016/j.etap.2016.06.023
Guo X, Li N, Wang H, Su W, Song Q, Liang Q, Sun Y (2022) Combined exposure to multiple metals on cardiovascular disease in NHANES under five statistical models. Environ Res 215:114435. https://doi.org/10.1016/j.envres.2022.114435
He J, Fang A, Yu S, Shen X, Li K (2020) Dietary nonheme, heme, and total iron intake and the risk of diabetes in adults: results from the China Health and Nutrition Survey. Diabetes Care 43(4):776–784. https://doi.org/10.2337/dc19-2202
Hong H, Xu J, He H, Wang X, Yang L, Deng P, Zhou Z (2022) Cadmium perturbed metabolomic signature in pancreatic beta cells correlates with disturbed metabolite profile in human urine. Environ Int 161:107139. https://doi.org/10.1016/j.envint.2022.107139
Huang S, Zhong D, Lv Z, Cheng J, Zou X, Wang T, Nie Z (2022) Associations of multiple plasma metals with the risk of metabolic syndrome: a cross-sectional study in the mid-aged and older population of China. Ecotoxicol Environ Saf 231:113183. https://doi.org/10.1016/j.ecoenv.2022.113183
Ichida K, Amaya Y, Okamoto K, Nishino T (2012) Mutations associated with functional disorder of xanthine oxidoreductase and hereditary xanthinuria in humans. Int J Mol Sci 13(11):15475–15495. https://doi.org/10.3390/ijms131115475
International Diabetes Federation. (2021). IDF Diabetes Atlas, 10th edition. Retrieved from https://diabetesatlas.org/en/
Ji J, Jin M, Kang J, Lee S, Lee S, Kim S, Oh S (2021) Relationship between heavy metal exposure and type 2 diabetes: a large-scale retrospective cohort study using occupational health examinations. BMJ open 11(3):e039541. https://doi.org/10.1136/bmjopen-2020-039541
Jiang Y, Xia W, Zhang B, Pan X, Liu W, Jin S, Li Y (2018) Predictors of thallium exposure and its relation with preterm birth. Environ Pollut (Barking, Essex : 1987) 233:971–976. https://doi.org/10.1016/j.envpol.2017.09.080
Kazi T, Afridi H, Kazi N, Jamali M, Arain M, Jalbani N, Kandhro G (2008) Copper, chromium, manganese, iron, nickel, and zinc levels in biological samples of diabetes mellitus patients. Biol Trace Elem Res 122(1):1–18. https://doi.org/10.1007/s12011-007-8062-y
Kemnic TR, Coleman M (2022) Thallium Toxicity. In StatPearls. StatPearls Publishing, Treasure Island (FL)
Kim H, Song S (2014) Concentrations of chromium, selenium, and copper in the hair of viscerally obese adults are associated with insulin resistance. Biol Trace Elem Res 158(2):152–157. https://doi.org/10.1007/s12011-014-9934-6
Lai J, Pang W, Cai S, Lee Y, Chan J, Shek L, Chong M (2018) High folate and low vitamin B12 status during pregnancy is associated with gestational diabetes mellitus. Clin Nutr (Edinburgh, Scotland) 37(3):940–947. https://doi.org/10.1016/j.clnu.2017.03.022
Leff T, Stemmer P, Tyrrell J, Jog R (2018) Diabetes and exposure to environmental lead (Pb). Toxics. https://doi.org/10.3390/toxics6030054
Li Y, Teng D, Shi X, Qin G, Qin Y, Quan H, Shan Z (2020) Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ (Clinical Research ed.) 369:m997. https://doi.org/10.1136/bmj.m997
Liu B, Feng W, Wang J, Li Y, Han X, Hu H, He M (2016) Association of urinary metals levels with type 2 diabetes risk in coke oven workers. Environ Pollut (Barking, Essex : 1987) 210:1–8. https://doi.org/10.1016/j.envpol.2015.11.046
Liu Q, Wu D, Ma Y, Cao Y, Pang Y, Tang M, Zhang T (2022) Intracellular reactive oxygen species trigger mitochondrial dysfunction and apoptosis in cadmium telluride quantum dots-induced liver damage. NanoImpact 25:100392. https://doi.org/10.1016/j.impact.2022.100392
Lv Y, Xie L, Dong C, Yang R, Long T, Yang H, Zhang H (2021) Co-exposure of serum calcium, selenium and vanadium is nonlinearly associated with increased risk of type 2 diabetes mellitus in a Chinese population. Chemosphere 263:128021. https://doi.org/10.1016/j.chemosphere.2020.128021
Mammadova-Bach E, Braun A (2019) Zinc homeostasis in platelet-related diseases. Int J Mol Sci. https://doi.org/10.3390/ijms20215258
Nazem M, Asadi M, Jabbari N, Allameh A (2019) Effects of zinc supplementation on superoxide dismutase activity and gene expression, and metabolic parameters in overweight type 2 diabetes patients: a randomized, double-blind, controlled trial. Clin Biochem 69:15–20. https://doi.org/10.1016/j.clinbiochem.2019.05.008
Nomura Y, Okamoto S, Sakamoto M, Feng Z, Nakamura T (2005) Effect of cobalt on the liver glycogen content in the streptozotocin-induced diabetic rats. Mol Cell Biochem 277:127–130. https://doi.org/10.1007/s11010-005-5777-y
Ogurtsova K, da Rocha Fernandes J, Huang Y, Linnenkamp U, Guariguata L, Cho N, Makaroff L (2017) IDF diabetes atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Prac 128:40–50. https://doi.org/10.1016/j.diabres.2017.03.024
Pavoni E, Petranich E, Adami G, Baracchini E, Crosera M, Emili A, Covelli S (2017) Bioaccumulation of thallium and other trace metals in Biscutella laevigata nearby a decommissioned zinc-lead mine (Northeastern Italian Alps). J Environ Manag 186:214–224. https://doi.org/10.1016/j.jenvman.2016.07.022
Qiu Q, Zhang F, Zhu W, Wu J, Liang M (2017) Copper in diabetes mellitus: a meta-analysis and systematic review of plasma and serum studies. Biol Trace Elem Res 177(1):53–63. https://doi.org/10.1007/s12011-016-0877-y
Rai P, Lee S, Zhang M, Tsang Y, Kim K (2019) Heavy metals in food crops: health risks, fate, mechanisms, and management. Environ Int 125:365–385. https://doi.org/10.1016/j.envint.2019.01.067
Rajkowska M, Protasowicki M (2013) Distribution of metals (Fe, Mn, Zn, Cu) in fish tissues in two lakes of different trophy in Northwestern Poland. Environ Monit Assess 185(4):3493–3502. https://doi.org/10.1007/s10661-012-2805-8
Ravipati E, Mahajan N, Sharma S, Hatware K, Patil K (2021) The toxicological effects of lead and its analytical trends: an update from 2000 to 2018. Crit Rev Anal Chem 51(1):87–102. https://doi.org/10.1080/10408347.2019.1678381
Rehman K, Fatima F, Waheed I, Akash M (2018) Prevalence of exposure of heavy metals and their impact on health consequences. J Cell Biochem 119(1):157–184. https://doi.org/10.1002/jcb.26234
Rodríguez-Mercado J, Altamirano-Lozano M (2013) Genetic toxicology of thallium: a review. Drug Chem Toxicol 36(3):369–383. https://doi.org/10.3109/01480545.2012.710633
Rotter I, Kosik-Bogacka D, Dołęgowska B, Safranow K, Lubkowska A, Laszczyńska M (2015) Relationship between the concentrations of heavy metals and bioelements in aging men with metabolic syndrome. Int J Environ Res Public Health 12(4):3944–3961. https://doi.org/10.3390/ijerph120403944
Rovira-Llopis S, Bañuls C, Diaz-Morales N, Hernandez-Mijares A, Rocha M, Victor V (2017) Mitochondrial dynamics in type 2 diabetes: Pathophysiological implications. Redox Biol 11:637–645. https://doi.org/10.1016/j.redox.2017.01.013
Sabir S, Akash M, Fiayyaz F, Saleem U, Mehmood M, Rehman K (2019) Role of cadmium and arsenic as endocrine disruptors in the metabolism of carbohydrates: Inserting the association into perspectives. Biomed Pharmacother = Biomed Pharmacother 114:108802. https://doi.org/10.1016/j.biopha.2019.108802
Schattenberg J, Schuchmann M (2009) Diabetes and apoptosis: liver. Apoptosis : Int J Program Cell Death 14(12):1459–1471. https://doi.org/10.1007/s10495-009-0366-2
Scheiber I, Dringen R, Mercer J (2013) Copper: effects of deficiency and overload. Met Ions Life Sci 13:359–387. https://doi.org/10.1007/978-94-007-7500-8_11
Shi Z, Chu A, Zhen S, Taylor AW, Dai Y, Riley M, Samman S (2018) Association between dietary zinc intake and mortality among Chinese adults: findings from 10-year follow-up in the Jiangsu Nutrition Study. Eur J Nutr 57(8):2839–2846. https://doi.org/10.1007/s00394-017-1551-7
Soleimanpour S, Crutchlow M, Ferrari A, Raum J, Groff D, Rankin M, Stoffers D (2010) Calcineurin signaling regulates human islet {beta}-cell survival. J Biol Chem 285(51):40050–40059. https://doi.org/10.1074/jbc.M110.154955
Stumvoll M, Goldstein B, van Haeften T (2005) Type 2 diabetes: principles of pathogenesis and therapy. Lancet (london, England) 365(9467):1333–1346. https://doi.org/10.1016/s0140-6736(05)61032-x
Tyrrell J, Hafida S, Stemmer P, Adhami A, Leff T (2017) Lead (Pb) exposure promotes diabetes in obese rodents. J Trace Elem Med Biol : Organ Soc Miner Trace Elem (GMS) 39:221–226. https://doi.org/10.1016/j.jtemb.2016.10.007
Vaiserman A (2015) Early-life exposure to substance abuse and risk of type 2 diabetes in adulthood. Curr DiabRep 15(8):48. https://doi.org/10.1007/s11892-015-0624-3
Wang B, Zhu Y, Pang Y, Xie J, Hao Y, Yan H, Ye R (2018) Indoor air pollution affects hypertension risk in rural women in Northern China by interfering with the uptake of metal elements: a preliminary cross-sectional study. Environ Pollut 240:267–272. https://doi.org/10.1016/j.envpol.2018.04.097
Wang X, Karvonen-Gutierrez C, Herman W, Mukherjee B, Harlow S, Park S (2020) Urinary metals and incident diabetes in midlife women: study of women’s health across the nation (SWAN). BMJ Open Diabetes Res Care. https://doi.org/10.1136/bmjdrc-2020-001233
Wang X, Mukherjee B, Karvonen-Gutierrez C, Herman W, Batterman S, Harlow S, Park S (2020) Urinary metal mixtures and longitudinal changes in glucose homeostasis: the study of women’s health across the nation (SWAN). Environ Int 145:106109. https://doi.org/10.1016/j.envint.2020.106109
Wijesekara N, Dai F, Hardy A, Giglou P, Bhattacharjee A, Koshkin V, Wheeler M (2010) Beta cell-specific Znt8 deletion in mice causes marked defects in insulin processing, crystallisation and secretion. Diabetologia 53(8):1656–1668. https://doi.org/10.1007/s00125-010-1733-9
Wu M, Shu Y, Song L, Liu B, Zhang L, Wang L, Wang Y (2019) Prenatal exposure to thallium is associated with decreased mitochondrial DNA copy number in newborns: evidence from a birth cohort study. Environ Int 129:470–477. https://doi.org/10.1016/j.envint.2019.05.053
Xiao L, Zhou Y, Ma J, Sun W, Cao L, Wang B, Chen W (2018) Oxidative DNA damage mediates the association between urinary metals and prevalence of type 2 diabetes mellitus in Chinese adults. Sci Total Environ 627:1327–1333. https://doi.org/10.1016/j.scitotenv.2018.01.317
Xu J, Zhou Q, Liu G, Tan Y, Cai L (2013) Analysis of serum and urinal copper and zinc in Chinese northeast population with the prediabetes or diabetes with and without complications. Oxid Med Cell Longev 2013:635214. https://doi.org/10.1155/2013/635214
Yang A, Liu S, Cheng N, Pu H, Dai M, Ding J, Bai Y (2017) Multiple metals exposure, elevated blood glucose and dysglycemia among Chinese occupational workers. J Diabetes Complicat 31(1):101–107. https://doi.org/10.1016/j.jdiacomp.2016.07.022
Yang A, Liu S, Cheng Z, Pu H, Cheng N, Ding J, Bai Y (2017) Dose-response analysis of environmental exposure to multiple metals and their joint effects with fasting plasma glucose among occupational workers. Chemosphere 186:314–321. https://doi.org/10.1016/j.chemosphere.2017.08.002
Yang J, Lu Y, Bai Y, Cheng Z (2023) Sex-specific and dose-response relationships of urinary cobalt and molybdenum levels with glucose levels and insulin resistance in U.S. adults. J Environ Sci (china) 124:42–49. https://doi.org/10.1016/j.jes.2021.10.023
Zhang Q, Hou Y, Wang D, Xu Y, Wang H, Liu J, Sun G (2020) Interactions of arsenic metabolism with arsenic exposure and individual factors on diabetes occurrence: Baseline findings from Arsenic and Non-Communicable disease cohort (AsNCD) in China. Environ Pollut (Barking, Essex : 1987) 265:114968. https://doi.org/10.1016/j.envpol.2020.114968
Zhang Q, Li J, Wang Y, Li X, Wang J, Zhou M, Zhang B (2021) Association between maternal thallium exposure and risk of gestational diabetes mellitus: evidence from a birth cohort study. Chemosphere 270:128637. https://doi.org/10.1016/j.chemosphere.2020.128637
Zhang J, Yin H, Zhu X, Xiang R, Miao Y, Zhang Y, Zhang L (2022) Effects of multi-metal exposure on the risk of diabetes mellitus among people aged 40–75 years in rural areas in southwest China. J Diabetes Investig 13(8):1412–1425. https://doi.org/10.1111/jdi.13797
Zheng Y, Ley S, Hu F (2018) Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol 14(2):88–98. https://doi.org/10.1038/nrendo.2017.151
Zhou M, Zhao E, Huang R (2022) Association of urinary arsenic with insulin resistance: Cross-sectional analysis of the National Health and Nutrition Examination Survey, 2015–2016. Ecotoxicol Environ Saf 231:113218. https://doi.org/10.1016/j.ecoenv.2022.113218
Zhu B, Liang C, Yan S, Li Z, Huang K, Xia X, Tao F (2019) Association between serum thallium in early pregnancy and risk of gestational diabetes mellitus: the Ma’anshan birth cohort study. J Trace Elem Med Biol : Organ Soc Miner Trace Elem (GMS) 52:151–156. https://doi.org/10.1016/j.jtemb.2018.12.011
Acknowledgements
We sincerely thank the laboratory staff and data collection personnel who participated in our basic work. We are particularly grateful to all the participants in this study for their questionnaires and donated biological samples.
Funding
This project was supported by the Natural Science Foundation Project of Ningxia, China (2022AAC05028), and the Special talents start-up funding of Ningxia Medical University (XT2019013, XZ2020008, and XT2019003). This work was also supported by the 2022 "Light of the West" Talent Training Plan Project of Chinese Academy of Sciences (XAB2022YM18) and the Key Research and Development Project of Ningxia (Grant No. 2021BEG02026).
Author information
Authors and Affiliations
Contributions
RW contributed to conceptualization, methodology, investigation, writing—original draft, and data curation. PH contributed to conceptualization, methodology, formal analysis, writing—original draft, and data curation. SD contributed to conceptualization, methodology, investigation, formal analysis, and data curation. ZZ contributed to methodology, formal analysis, and data Curation. YD contributed to methodology, formal analysis, and data curation. ML contributed to investigation. ZS: Investigation. XL: Writing—review & editing. YS: Investigation. YS contributed to investigation. RZ contributed to conceptualization, investigation, formal analysis, and writing—original draft, and supervision. JS contributed to conceptualization, investigation, formal analysis, writing—original draft, and supervision. HY contributed to conceptualization, investigation, formal analysis, writing – original draft, and supervision.
Corresponding authors
Ethics declarations
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
Ethical Approval
This study was also approved by the Ethics Committee of Ningxia Medical University, No.2020–099. All study subjects have signed the informed consent form.
Consent to Participate
Written informed consent was obtained from all participants.
Consent to Publish
The manuscript does not contain any individual person’s data and thus consent for publication is not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wang, R., He, P., Duan, S. et al. Correlation and interaction between urinary metals level and diabetes: A cross sectional study of community-dwelling elderly. Expo Health 16, 559–574 (2024). https://doi.org/10.1007/s12403-023-00577-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12403-023-00577-6