
Abstract
Background
The aim of this study was to analyze different prognoses in women and men with normal myocardial perfusion gated SPECT, according to stress test results.
Methods
Differences between women and men in terms of hard events (HE) (non-fatal acute myocardial infarction or cardiac death) and HE plus coronary revascularization (HE + CR) were analyzed in 2,414 consecutive patients (mean age 62.8 ± 13.5 years, 1,438 women) with a normal stress-rest gated SPECT, taking into account their stress test results.
Results
Four hundred and seven patients (16.9 %) (15.9 % women and 17.5 % men) had a positive stress test (ST-segment depression ≥1 mm and/or angina). During a follow-up of 5.1 ± 3.4 years, there were more significant HE (6.5 % vs 2.3 %; P = .005) and HE + CR (11.6 % vs 4.8 %, P = .001) in men with a positive stress test than in men with a negative stress test. These differences were not observed in women. In multivariate regression models, HE and HE + CR were also more frequent in men with a positive stress test (HR:3.3 [95 % CI 1.1 % to 9.5 %]; HR:4.2 [95 % CI 1.8 % to 9.9 %]; respectively) vs women with a positive stress test.
Conclusions
Although patients with normal gated SPECT studies have a favorable outcome, men with an abnormal stress test have a more adverse prognosis than women.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Myocardial perfusion single photon emission computed tomography (SPECT) has been proposed as a gatekeeper to prevent unnecessary invasive cardiac procedures.1 Most studies after a normal myocardial perfusion SPECT have reported rates of hard events (HE) of <1 % per year of follow-up. However, clinical characteristics such as a history of coronary artery disease (CAD), diabetes, gender, increasing age,2-5 and type of stress6-10 yield incremental prognostic value over SPECT data in patients with normal scans.
The pathophysiologic and prognostic value of a positive ECG in the presence of negative vasodilator myocardial perfusion imaging has been already investigated, although with conflicting results.11-14 However, two recent studies15,16 with a very long follow-up (12-15 years) after normal myocardial perfusion SPECT observed that exercise parameters also can be used to identify patients with a higher risk status, because stress electrocardiogram provides further useful diagnostic and prognostic information. Although a normal SPECT with a positive stress electrocardiogram is infrequent, CAD cannot be ruled out, predominantly in men.17,18 The purpose of our study was to analyze different prognoses in women and men with a normal stress-rest myocardial perfusion gated SPECT, depending on the stress test results.
Methods
We analyzed 2,414 consecutive patients (mean age 62.8 ± 13.5 years, 1,438 female) with a normal stress-rest gated SPECT and suspected CAD. Patients were excluded in cases of cardiomyopathies, valvulopathies, myocardial infarction, coronary revascularization (CR), cardiac pacemaker, and abnormal ECG at rest before gated SPECT.
Study Design
All patients were prospectively enrolled in a research database from our Nuclear Cardiology Unit at the time of testing and were followed (mean 5.1 ± 3.4 years) after SPECT for the occurrence of two endpoints: HE (non-fatal acute myocardial infarction or cardiac death) and HE plus CR (HE + CR) post-gated SPECT. Death from cardiac causes (ICD-10 codes I00 to I99) and re-hospitalizations for acute myocardial infarction (AMI) (ICD-I21, I22) were identified using the Catalan Cause of Death Register, after obtaining the corresponding authorization. We then analyzed this population according to gender and stress test results. The research protocol conformed to the Declaration of Helsinki and was reviewed and approved by the Ethics Committee of Vall d’Hebron Hospital.
Myocardial Perfusion Stress-Rest Gated SPECT
All 2,414 patients underwent stress-rest gated SPECT with a one-day protocol with 99mTc-tetrofosmin. Stress testing on an exercise bicycle or treadmill was performed on 1,671 (69.2 %) patients; 390 (16.2 %) patients underwent submaximal exercise plus dipyridamole, due to their inability to achieve 5 METs or 80 % of predicted peak heart rate for their age; and 353 (14.6 %) patients received dipyridamole alone.19 Stress testing was considered positive if there was horizontal or downsloping ST-segment depression ≥1 mm in at least 2 consecutive leads and/or angina. The prevalence of ST-segment alterations during stress test with and without a hypertensive response was analyzed in patients who underwent only exercise stress (N = 1,398). Hypertensive response to physical stress was defined if systolic blood pressure (SBP) was >200 mmHg at peak exercise.20
The first dose (370 mBq administered 30-60 seconds before ending the stress test) and the second dose (900 mBq administered at rest) were separated by an interval of over 45 minutes. The study was performed using a Siemens E.CAM gamma camera with a 90° angled dual head, low-energy high-resolution collimator and 180° semicircular orbit in “step-and-shoot” mode, starting at 45° right anterior oblique, with 25 seconds/frame every 3°. Detection was synchronized with the “R wave” of the ECG, and cardiac cycle was segmented into 8 fractions. The reconstruction system used in this gamma camera was filtered backprojection (Butterworth post-filter, order 5 and cut-off frequency .5). No corrections were made for attenuation or scatter. Interpretation of the scan was performed by visual analysis. Stress and rest tomographic views were reviewed side-by-side by two experienced professionals (a nuclear physician and a cardiologist). A normal study was defined as the absence of perfusion abnormalities in the stress-rest study and a normal left ventricular ejection fraction (LVEF ≥50 %). LVEF and volumes were calculated automatically, in gated SPECT at rest, using the QGS® (Cedars-Sinai Medical Center, Los Angeles, CA) program.
Statistical Analysis
All continuous data were expressed as mean (SD, standard deviation) and all non-continuous variables were expressed as percentages. Continuous variables were compared using the Student t test for unpaired samples. Differences between proportions were compared using the χ 2 test. Fisher’s exact test was used when <5 patients were expected in any subgroup.
Variables were selected for multivariate analysis when they presented a P ≤ .05 in the univariate analysis or when they were considered of clinical relevance. Multivariate models were constructed using Cox proportional hazards analysis (ENTER method, inclusion criteria P ≤ .05; exclusion criteria P > .10) adjusted for clinical variables. There was no evidence of violation of this assumption for any covariate. Hazards ratios (HR), 95 % confidence intervals, and statistical significance for each group in the models were determined.
In the multivariable analysis, two types of models were performed considering two types of hazard: end-point specific hazard and hazard of the subdistribution. The hazard of the subdistribution may be interpreted as the probability of observing an event of interest in the next instant while knowing that either the event of interest has not yet occurred or a competing risk event has been observed. For this analysis, we used the Fine and Gray method. The model proposed by Fine and Gray21 is based on the hazard of the subdistribution (sHR) and provides a simple relationship between covariates and cumulative incidence.22
All statistical tests were two-sided. A value of P < .05 was considered as indicative of statistical significance. Statistical analysis was performed using SPSS for Windows, version 15 (SPSS Inc, Chicago), and Stata/IC 13.
Results
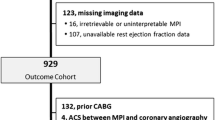
The characteristics of the study population are shown in Figure 1 and Tables 1 and 2 according to gender and stress test results. Of the 2,414 patients, 407 (16.9 %: 17.5 % women and 15.9 % men, P = .290) had a positive stress test (Figures 2 and 3). Prevalence of cardiovascular risk factors (P < .001), exercise test (P < .001), and CR (P < .001) were more frequent in men. The prevalence of high, intermediate, and low pre-test probability of CAD were 21.3 % (N = 513), 11.2 % (N = 272), and 67.5 % (N = 1,629), respectively. There were no significant differences between female and male for high pre-test probability of CAD (22 % vs 20.1 %, P = .247), and for low pre-test probability (67.9 % vs 66.9 %, P = .619), but female patient had less intermediate pre-test probability (10.1 % vs 13 %, .026).

Patient distribution, according to gender and stress test results

Normal myocardial perfusion SPECT of a woman with downsloping ST-segment depression at the end of exercise test, and normal coronary angiography. HLA, Horizontal long axis; R rest; Rec, recovery; S stress; SA short axis; VLA vertical long axis

Normal myocardial perfusion SPECT of a men with downsloping ST-segment depression at the end of exercise of exercise test, and moderate stenoses of left main, left anterior descending, left circumflex, and right coronary arteries. HLA Horizontal long axis; R rest; Rec recovery; S stress; SA short axis; VLA vertical long axis
In this population, 55 (2.3 %) patients had ≥2 mm ST depression. Stress test results in women and men are shown in Table 3. In male patients, the hypertensive response was more frequent than female patients (18.1 % vs 10 %; P < .001). Female patients with hypertensive response (N = 92) had more basal hypertension, more ST-segment depression ≥1 mm, and more ST-segment depression ≥1 mm and/or angina than female patients without hypertensive response; without significant differences for HE, HE plus CR, and early CR (Table 4).
The prevalence of ≥1 mm ST downsloping in patients who underwent exercise stress, exercise stress plus dipyridamole stress and dipyridamole alone, was 11.2 %, 11 %, and 5.1 %, respectively; and the prevalence of angina and/or ≥1 mm ST downsloping in patients who underwent exercise stress, exercise stress plus dipyridamole stress and dipyridamole alone, was 17.5 %, 21.8 %, and 8.2 %, respectively. The probability of ST-segment depression and the probability of ST-segment depression and/or angina during stress test significantly increases with increasing age. The Cox proportional hazards analysis revealed a greater cumulative Hazard for ST-segment depression (P = .006) in male than in female patients (Figure 4A). A similar result (P = .044) was observed in patients with and without ST-segment depression and/or angina during stress test (Figure 4B).

Relationship between cumulative hazard (Cum Hazard) for predicted ≥1 mm ST downsloping during stress test and age in female and male patients, adjusted by hypertension (A). Relationship between cumulative hazard (Cum Hazard) for predicted ≥1 mm ST downsloping or angina during stress test and age in female and male patients, adjusted by hypertension (B)
During a mean follow-up of 5.1 ± 3.4 years, coronary angiography was performed in 128 patients (4.7 % of the women and 6.1 % of the men, P = .127) and of those, normal coronary arteries were observed in 61.7 % (42/68) of women and in 30 % (18/60) of men (P = .016). Only 7 (4.9 %) women with segment depression underwent coronary angiography, 1 (14.3 %) of them had 3 vessels disease and 1 (14.3 %) main stem disease. Only 11 (10.6 %) males with segment depression underwent coronary angiography, 1 (10 %) of them had 3 vessels disease.
During the follow-up, 14 patients had acute myocardial infarction; 7 (50 %) of them underwent coronary angiography. Three patients had 1 vessel disease, two patients had 2 vessels disease, and two patients 3 vessels disease. The 4 patients with 2 and 3 vessels disease were revascularized during the follow-up post SPECT. In Table 5, the coronary angiography results of patients with CR post-gated SPECT are present without significant differences between male and female patients.
CR was performed in 49 patients (2 %), HE was observed in 64 patients (2.7 %), HE + CR in 106 patients (4.4 %), and non-cardiac death in 169 patients (7 %).
Hard Events
There were no significant differences (HR 1.1 [95 % CI .5 % to 2.7 %]; P = .797) between women with and without a positive stress test in Cox regression analysis (Figure 5A) and in Fine & Gray analysis (Table 6). There were significant differences (HR 2.8 [95 % CI 1.3 % to 6.2 %]; P = .01) between men with and without a positive stress test in Cox regression analysis (Figure 5B) and in Fine & Gray analysis (Table 6). Among patients with a positive stress test (N = 407), there were significant differences (HR 3.3 [95 % CI 1.1 % to 9.5 %]; P = .027) between women and men in Cox regression analysis (Figure 5C) and in Fine & Gray analysis (Table 6).

Cox regression analysis for hard events in women (A) (adjusted by age ≥70 years, diabetes, hypertension, hypercholesterolemia, current smoker, angina, pharmacologic stress, nitrates, and coronary revascularization); in men (B) (adjusted by age ≥70 years, diabetes, hypertension, hypercholesterolemia, current smoker, angina, pharmacologic stress, nitrates, and coronary revascularization); and in women and men with positive stress test (C) (adjusted by age ≥70 years, diabetes, hypertension, hypercholesterolemia, current smoker, angina, pharmacologic stress, nitrates, and coronary revascularization)
Hard Events Plus Coronary Revascularization
There were no significant differences (HR .78 [95 % CI .4 % to 1.7 %]; P = .531) between women with and without a positive stress test in Cox regression analysis (Figure 6A) and in Fine & Gray analysis (Table 6). Among men, there were significant differences (HR 2.5 [95 % CI 1.4 % to 4.4 %]; P = .002) between patients with and without a positive stress test in Cox regression analysis (Figure 6B) and in Fine & Gray analysis (Table 6). Among patients with a positive stress test (N = 407), there were significant differences (HR 4.2 [95 % CI 1.8 % to 9.9 %]; P = .001) between women and men in Cox regression analysis (Figure 6C) and in Fine & Gray analysis (Table 6).

Cox regression analysis for hard events plus coronary revascularization in women (A) (adjusted by age ≥70 years, diabetes, hypertension, hypercholesterolemia, current smoker, angina, pharmacologic stress, and nitrates); in men (B) (adjusted by age ≥70 years, diabetes, hypertension, hypercholesterolemia, current smoker, angina, pharmacologic stress, and nitrates); and in women and men with positive stress test (C) (adjusted by age ≥70 years, diabetes, hypertension, hypercholesterolemia, current smoker, angina, pharmacologic stress, and nitrates)
Discussion
In our series of patients with normal myocardial perfusion gated SPECT, 17.5 % of the women and 15.9 % of the men had a positive stress test. During a mean follow-up of 5.1 ± 3.4 years, there were more significant HE (6.5 % vs 2.3 %; P = .005) and HE + CR (11.6 % vs 4.8 %, P = .001) in men with a positive stress test than men with a negative stress test. In multivariate regression models, HE and HE + CR were also more frequent in men with a positive stress test (HR: 2.8 [95 % CI 1.3 % to 6.3 %]; HR: 2.5 [95 % CI 1.4 % to 4.4 %]; respectively). These differences were not observed in women.
Controversial results of previous studies with vasodilator myocardial perfusion imaging have been published,11-14 but ischemic ECG changes during adenosine or dipyridamole infusion occur less commonly than during exercise. In our series, prevalence of ≥1 mm ST downsloping in patients who underwent exercise stress, exercise stress plus dipyridamole stress and dipyridamole alone, was 11.2 %, 11 %, and 5.1 % ,respectively. Rozansky et al23 observed that there has been an increase in the frequency of normal SPECT studies compared to 2-3 decades ago. The high frequency of normal SPECT results has led to increased interest in how outcomes may vary according to risk factors and other clinical variables in these patients. Thus, research in this arena should include stress variables such as those we have analyzed in our series.
Patients with normal myocardial perfusion SPECT are considered to be at low risk of cardiac events, and only 1.3 % of these patients underwent early revascularization vs 26 % with abnormal SPECT studies.1 In our series, 16.9 % of the patients with normal gated SPECT had a positive stress test, 5.3 % underwent CA and 2 % underwent CR. The indication of coronary angiography in patients with normal SPECT is more frequent in patients with a positive stress test, because ST-segment depression and/or angina is a marker of possible CAD.
As others authors17,18 have previously reported, significant CAD is more frequent in men than in women with normal SPECT and positive stress. Accuracy and specificity of exercise electrocardiography are lower in women24,25 and false positive ECG stress results can be increased in the presence of hypertensive response. However, an exaggerated blood pressure response to exercise is rarely reproducible, as Sharabi et al20 have been published. On the other hand, false negatives of myocardial perfusion SPECT in the presence of diffuse CAD with homogeneous ischemia could be more frequent in men than in women.18 All these factors could contribute to explain the adverse prognosis of men vs women with normal gated SPECT and positive stress test results.
He et al17 analyzed 23,059 patients who were studied using exercise myocardial perfusion tomography and found 813 (3.5 %) with a strongly positive electrocardiogram and normal perfusion images. Of those, 52 patients who had no conditions known to be associated with a false positive exercise electrocardiogram, and no previous revascularization, underwent coronary angiography. There was a significant gender difference in the prevalence of significant coronary stenoses (80 % in male vs 24 % in female patients, P < .0001). Candell-Riera et al,18 in a consecutive series of 7,350 myocardial perfusion SPECT studies, found 66 (.9 %) nonrevascularized patients with normal scintigraphic findings and a positive exercise test. Twenty one of the 26 women (81 %) and 1 of the 7 men (14 %) with coronary angiography had normal coronary arteries (P = .004). Similar results were observed in patients with coronary angiography in our present large series: normal coronary arteries were observed in 61.7 % of women and in 30 % of men (P = .016).
Schinkel et al15 have demonstrated that not only clinical, but also exercise test parameters can be used to identify patients at increased risk of an adverse outcome. They reported that the multivariate predictors of major adverse cardiac events after 15 years of follow-up in patients with normal exercise SPECT were age, male gender, diabetes, diastolic blood pressure at rest, rate-pressure product at rest, peak exercise heart rate, and ST-segment changes. Ottenhof et al16 also found, during a median follow-up of 12 years in patients with known CAD and normal myocardial perfusion that stress test variables can be used to identify patients at increased risk of future cardiac events. Independent predictors of cardiac mortality were age, male gender, and rate-pressure product at peak stress.
Exercise capacity measured in metabolic equivalents (METs) is an important prognostic variable derived from the exercise stress test. Higher workloads achieved during exercise predict improved survival rates, irrespective of age and gender.26 According to Bourque et al,27 in a cohort of 1,056 patients with an intermediate to high clinical risk of CAD, achieving ≥10 METs with no ischemic ST depression was associated with 0 % prevalence of significant ischemia in myocardial perfusion SPECT. Estimated METs were not evaluated as a prognostic variable in our series because 14.6 % of patients could not perform exercise.
New knowledge gained
This is the first published study that prospectively explores the different prognoses in women and men with normal gated SPECT, according to stress test results (ST depression and/or angina). Men with an abnormal stress test have a more adverse prognosis than women. Males with normal SPECT but abnormal stress test required an accurate follow-up.
Conclusions
Although patients with normal myocardial perfusion gated SPECT studies have a favorable outcome, men with an abnormal stress test have a more adverse prognosis than women. As the prognosis is worse in men with normal SPECT and positive stress test, follow-up should be closer in these patients.
Study limitations
In our study, we did not assess pulmonary uptake and transient ischemic dilatation of the left ventricle at stress.28,29 These variables are markers of severe multi-vessel CAD and could also be predictors of poor clinical outcome in our series. It is possible that the study includes false-negative tests because the sensitivity of myocardial perfusion SPECT is not 100 %. Attenuation correction, which could have improved the accuracy of SPECT, was not used in this study. Furthermore, changes in medical therapy during follow-up were not available, and during the first period when patients underwent SPECT, electrocardiogram-gated acquisition was not performed. No data about prevalence of echocardiographic left ventricular hypertrophy, as possible cause of false-positive SPECT, and prevalence of ST upsloping in aVr,30 a sign possibly associated with significant left main stenosis, were available. The low event rate in patients with positive ECG could be a limitation of the study, whose results still remain “hypothesis generating”.
References
Miller TD, Hodge DO, Milavetz JJ, Gibbons RJ. A normal stress SPECT scan is an effective gatekeeper for coronary angiography. J Nucl Cardiol 2007;14:187-93.
Hachamovitch R, Hayes S, Friedman JD, Cohen I, Shaw LJ, Germano G, et al Determinants of risk and its temporal variation in patients with normal stress myocardial perfusion scans. What is the warranty period of a normal scan? J Am Coll Cardiol 2003;41:1329-40.
Carryer DJ, Askew JW, Hodge DO, Miller TD, Gibbons RJ. The timing and impact of follow-up studies after normal stress single-photon emission computed tomography sestamibi studies. Circ Cardiovasc Imaging 2010;3:520-6.
Supariwala A, Uretsky S, Singh P, Memon S, Khokhar SS, Wever-Pinzon O, et al Synergistic effect of coronary artery disease risk factors on long-term survival in patients with normal exercise SPECT studies. J Nucl Cardiol 2011;18:207-14.
Supariwala A, Uretsky S, Depuey EG, Thotakura G, Kanneganti S, Guriginjakunta N, et al Influence of mode of stress and coronary risk factor burden upon long-term mortality following normal stress myocardial perfusion single-photon emission computed tomographic imaging. Am J Cardiol 2013;111:846-50.
Berman DS, Kang X, Hayes SW, Friedman JD, Cohen I, Abidov A, et al Adenosine myocardial perfusion single-photon emission computed tomography in women compared with men. Impact of diabetes mellitus on incremental prognostic value and effect on patient management. J Am Coll Cardiol 2003;41:1125-33.
Navare SM, Mather JF, Shaw LJ, Fowler MS, Heller GV. Comparison of risk stratification with pharmacologic and exercise stress myocardial perfusion imaging: A meta-analysis. J Nucl Cardiol 2004;11:551-61.
Sharma J, Roncari C, Giedd KN, Fox JT, Kanei Y. Patients with adenosine-induced ST-segment depressions and normal myocardial perfusion imaging: Cardiac outcomes at 24 months. J Nucl Cardiol 2010;17:874-80.
Rozanski A, Gransar H, Hayes SW, Friedman JD, Hachamovitch R, Berman DS. Comparison of long-term mortality risk following normal exercise vs adenosine myocardial perfusion SPECT. J Nucl Cardiol 2010;17:999-1008.
Johnson NP, Schimmel DR Jr, Dyer SP, Leonard SM, Holly TA. Survival by stress modality in patients with a normal myocardial perfusion study. Am J Cardiol 2011;107:986-9.
Klodas E, Miller TD, Christian TF, Hodge DO, Gibbons RJ. Prognostic significance of ischemic electrocardiographic changes during vasodilator stress testing in patients with normal SPECT images. J Nucl Cardiol 2003;10:4-8.
Abbott BG, Afshar M, Berger AK, Wackers FJT. Prognostic significance of ischemic electrocardiographic changes during adenosine infusion in patients with normal myocardial perfusion imaging. J Nucl Cardiol 2003;10:9-16.
Chow BJW, Wong JW, Yoshinaga K, Ruddy TD, Williams K, deKemp RA, et al Prognostic significance of dipyridamole-induced ST depression in patients with normal 82Rb PET myocardial perfusion imaging. J Nucl Med 2005;46:1095-101.
Hage FG, Duvovsky EV, Heo J, Iskandrian AE. Outcome of patients with adenosine-induced ST-segment depression but with normal perfusion on tomographic imaging. Am J Cardiol 2006;98:1009-11.
Schinkel AF, Boiten HJ, van der Sijde JN, Ruitinga PR, Sijbrands EJ, Valkema R, et al 15-Year outcome after normal exercise 99mTc-sestamibi myocardial perfusion imaging: What is the duration of low risk after a normal scan? J Nucl Cardiol 2012;19:901-6.
Ottenhof MJ, Wai MC, Boiten HJ, Korbee RS, Valkema R, van Domburg RT, et al 12-Year outcome after normal myocardial perfusion SPECT in patients with known coronary artery disease. J Nucl Cardiol 2013;20:748-54.
He ZX, Dakik HA, Vaduganathan P, Qureshi U, Mahmarian JJ, Verani MS. Clinical and angiographic significance of a normal thallium-201 tomographyc study in patients with a strongly positive exercise electrocardiogram. Am J Cardiol 1996;78:638-41.
Candell-Riera J, Fernández C, Escudero F, de León G, Aguadé-Bruix S, Castell-Conesa J. Prevalence and angiographic significance of normal myocardial perfusion SPET with positive exercise electrocardiogram. Rev Esp Cardiol 2004;57:894-7.
Candell-Riera J, Santana-Boado C, Castell-Conesa J, Aguadé-Bruix S, Olona M, Palet J, Cortadellas J, et al Simultaneous dipyridamole/maximal subjective exercise with 99mTc-MIBI SPECT: Improved diagnostic yield in coronary artery disease. J Am Coll Cardiol 1997;29:531-6.
Sharabi Y, Almer Z, Hanin A, Messerli FH, Ben-Cnaan R, Grossman E. Reproducibility of exaggerated blood pressure response to exercise in healthy patients. Am Heart J 2001;141:1014-7.
Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risks. J Am Stat Assoc 1999;94:496-509.
Andersen PK, Geskus RB, de Witte T, Putter H. Competing risks in epidemiology: Possibilities and pitfalls. Int J Epidemiol 2012;41:861-70.
Rozanski A, Gransar H, Hayes SW, Min J, Friedman JD, Thomson LEJ, et al Temporal trends in the frequency of inducible myocardial ischemia during cardiac stress testing: 1991 to 2009. J Am Coll Cardiol 2013;61:1054-65.
Morise AP, Diamond GA, Detrano R, Bobbio M. Incremental value of exercise electrocardiography and thallium-201 testing in men and women for the presence and extent of coronary artery disease. Am Heart J 1995;130:267-76.
Santana-Boado C, Candell-Riera J, Castell-Conesa J, Aguadé-Bruix S, García-Burillo A, Canela T, et al Diagnostic accuracy of technetium-99m-MIBI myocardial SPECT in women and men. J Nucl Med 1998;39:751-5.
Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise capacity and mortality among men referred for exercise testing. N Engl J Med 2002;346:793-801.
Bourque JM, Holland BH, Watson DD, Beller GA. Achieving an exercise workload of ≥10 metabolic equivalents predicts a very low risk of inducible ischemia. Does myocardial perfusion imaging have a role. J Am Coll Cardiol 2009;54:538-45.
Berman DS, Kang X, Slomka PJ, Gerlach J, de Yang L, Hayes SW, et al Underestimation of extent of ischemia by gated SPECT myocardial perfusion imaging in patients with left main coronary artery disease. J Nucl Cardiol 2007;14:521-8.
Valdiviezo C, Motivala AA, Hachamovitch R, Chamarthy M, Navarro PC, Ostfeld RJ, et al The significance of transient ischemic dilation in the setting of otherwise normal SPECT radionuclide myocardial perfusion images. J Nucl Cardiol 2011;18:220-9.
Uthamalingam S, Zheng H, Leavitt M, Pomerantsev E, Ahmado I, Gurm GS, et al Exercise-induced ST-segment elevation in ECG lead aVR is a useful indicator of significant left main or ostial LAD coronary artery stenosis. J Am Coll cardiol Imaging 2011;4:176-86.
Acknowledgments
The authors are grateful to Prof. Demos Demosthenous (London) for his grammatical English correction.
Disclosure
Authors declared that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
See related editorial, doi:10.1007/s12350-014-0022-2
Rights and permissions
About this article

Cite this article
Romero-Farina, G., Candell-Riera, J., Ferreira-González, I. et al. Normal Myocardial Perfusion Gated SPECT and Positive Stress Test: Different Prognoses in Women and Men. J. Nucl. Cardiol. 22, 453–465 (2015). https://doi.org/10.1007/s12350-014-0009-z
Received:
Revised:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-014-0009-z