
Abstract
Guided by the Risk and Resilience Model, the present study aims to generate hypotheses by investigating a wide range of variables that might buffer the association between peer victimization and internalizing symptoms from a convenience sample of African American adolescents in four neighborhoods in Chicago’s Southside. Measures for the study included internalizing symptoms, peer victimization, four protective factors (parental closeness, teacher’s care, religiosity, and positive future orientation) and covariates (age, sex, and government assistance). Controlling for the covariates, a series of multivariate regression analyses were conducted to explore the direct effects of peer victimization and internalizing symptoms and the interaction between peer victimization and the four protective factors. The study found that peer victimization was directly associated with internalizing symptoms. In terms of the interactions, the study found that parental closeness moderated the association between peer victimization and internalizing symptoms. The findings show that parental closeness is an important protective factor that needs to be considered in the research hypotheses. The findings specifically demonstrated the importance of developing hypotheses to test whether parental closeness protects adolescents from internalizing symptoms linked to peer victimization.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Peer victimization, which involves being a target of any acts of physical, verbal, and relational aggression from peers (Archer et al. 2005; Card et al. 2008), is a serious concern in schools. National data documented that approximately 20% of children and adolescents reported being victimized by their peers during the past academic year (Kann et al. 2018; Lebrun-Harris et al. 2019; Musu et al. 2019). Among African American adolescents, the rate of peer victimization is higher as indicated by the Bureau of Justice Statistics, which showed that 23% of African Americans reported being bullied compared to 16% Hispanics and 7% Asians (Musu et al. 2019). African American youth in impoverished urban areas are even at a higher risk because of structural disadvantages, such as low household income and poverty (Fontenot et al. 2018). Urban African American victims of bullying are likely to be at an elevated risk of psychosocial distress, such as depression, anxiety, and low self-esteem.
Peer victimization is generally a significant source of stress for most adolescents. As studies showed, youth who reported being victimized by their peers, physically or verbally, are more likely to develop numerous psychosocial and behavioral problems, such as feelings of humiliation, depressive symptoms, anxiety, non-suicidal self-injury, and suicidal ideation and behavior (Barzilay et al. 2017; Claes et al. 2015; Ford et al. 2017; Stapinski et al. 2015; Zwierzynska et al. 2013). Notably, a substantial amount of research has evidenced that peer victimization can contribute to internalizing symptoms (Farmer et al. 2015; Pengpid et al. 2019; Reijntjes et al. 2010; Schwartz et al. 2015). A meta-analysis of eighteen studies by Reijntjes et al. (2010) showed a significant association between peer victimization and internalizing symptoms. Farmer et al. (2015) study, using teacher- and peer-report measures to assess victimization and internalizing behaviors, found that victimized youth were more likely to display internalizing symptoms than their non-victimized peers.
Peer Victimization and Psychosocial Sequelae
It also appears that youths’ experiences in all forms of peer victimization have a negative impact on their behavior, as documented in several studies. A study conducted by Baldry (2004) reported that victims of both direct and indirect bullying were at a heightened risk of depression. Similarly, Crick et al. (2002) found that while boys were more physically victimized by their friends than girls, and girls were more relationally victimized by their friends than boys, both forms of victimization were found to be positively associated with adjustment difficulties (including internalizing symptoms) for both sexes. Similarly, Eastman et al. (2018) study, which identified profiles of internalizing and externalizing behavioral problems associated with peer victimization, reported that adolescents who were victims of direct, indirect, or both forms of bullying were in the high internalizing and externalizing profiles.
Peer victimization and internalizing symptoms are frequently reported by youth in urban areas, particularly African American youth (Goldweber et al. 2013; Joe et al. 2009) who are confronted with multiple stressors, such as discrimination and structural disadvantages on a daily basis (Estrada-Martinez et al. 2012). However, in the research literature, the common portrayal of the urban or inner-city African American youth is one that is of an individual who experiences numerous stressors on a daily basis, is being raised in a family undergoing economic hardship and is embedded within a neighborhood that is characterized as impoverished and dangerous (Li et al. 2007). Equally important and often less attended to are the resources and protective factors that are present for these youth and their families (Yoshikawa et al. 2000).
A Focus on Protective Factors
There have been growing calls for more research that illuminates the protective factors across individual characteristics and the social environment that would buffer peer risk factors among adolescents. An exploration of the protective factors that are associated with resilience for urban African American victims of bullying is highly important, especially considering that resources are limited in low-income, urban schools. More specifically, adolescents who are frequently victimized physically and/or verbally by their peers are at a heightened risk of internalizing symptoms, and identifying protective factors within multiple domains is imperative. Earlier studies have documented the protective roles of parents and teachers in adolescents’ involvement in physical and verbal bullying (Curtner-Smith et al. 2006; Wang et al. 2009), which are also likely to mitigate internalizing symptoms. Applying the Risk and Resilience Model, the present study aims to explore a wide range of variables that might buffer the linkage between peer victimization and internalizing symptoms to develop research hypotheses.
Theoretical Frameworks
Because adolescents spend a majority of their time within schools the environment can be promotive (e.g., asset-based) building on the strengths of adolescents or inhibitive (e.g., harmful) – contributing to unhealthy development. Fergus et al.’s (2005) Risk and Resilience Model focuses on positive youth development in the context of risks, which also highlights why some adolescents grow up to be healthy adults despite exposure to multiple risks and some do not. This model includes the compensatory model, which explains how protective factors operate to change the trajectory from risk exposure (e.g., peer victimization) to adverse outcomes (e.g., internalizing symptoms) (Fergus et al. 2005). Urban African American youth, for example, are at significant risk of peer victimization, but adult monitoring and social supports may help compensate for the negative outcomes.
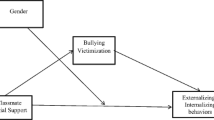
We draw on the Risk and Resilience Model to explore the protective role of parental closeness, teacher’s care, positive future orientation, and religiosity. While a bulk of research has proposed and tested research hypotheses, the current study is aimed to generate hypotheses by exploring whether peer victimization might impact psychological wellbeing and identifying protective factors that attenuate internalizing symptoms of peer victimizations from a convenience sample of African American adolescents in four neighborhoods located in Chicago’s Southside (see Fig. 1).

Protective mechanisms of the association between peer victimization and internalizing symptoms
Potential Buffers
A positive relationship with parents in the home is frequently recognized as an important protective factor in the context of peer victimization (Kotchick et al. 2020; Mann et al. 2015; Rudolph et al. 2020; Stadler et al. 2010). Youth who can communicate effectively with their parents and those who receive support from parents are shown to better cope with peer victimization. From their study consisting of 986 German adolescents, Stadler et al. (2010) found parental support (measured by parental warmth, parental involvement, parental supervision, and parental consistency) protected adolescents from mental health problems (hyperactivity and attention problems, emotional problems, conduct problems, and problems with peers) associated with peer victimization (physical attack, verbal attack, social manipulation, and destruction of property). Similarly, a study by Kotchick et al. (2020), which comprised a sample of 1,058 sixth graders from California, Oregon and Wisconsin, found that perceived supportive parenting from mothers moderated the association between physical and verbal forms of peer victimization and depressive symptom. Another recent longitudinal study of 5th to 7th graders transitioning from elementary to middle school evidenced that high-quality parent–child relationships as measured by parental warmth and support mitigated depressive symptoms and social helplessness, which were both positively associated with peer victimization (Rudolph et al. 2020).
Support from teachers appears to be crucial for adolescents. Studies consistently show that within the school environment, teacher support is associated with a low level of peer victimization and a protective role in the relationship between peer victimization and adverse outcomes (Lucas-Molina et al. 2015; Mann et al. 2015; Stadler et al. 2010; Sulkowski et al. 2018; Yeung et al. 2010). Findings from Lucas-Molina et al. (2015) whose study consisted of 1864 children, aged 8 to 13 years in 27 schools revealed that teacher support was linked to a lower risk of peer victimization reported by students, whereas hostile teacher-student relationship was associated with higher levels of peer victimization. In a study by Yeung et al. (2010), which comprised a sample of 580 youths concurrently and across two time periods (ages 12–19 and 14–21), those who received emotional support from their teachers experienced fewer emotional and behavioral problems associated with relational victimization. Sulkowski et al. (2018) also found that among high school-aged adolescents in the U.S. Southwest, positive teacher-student relations moderated the link between peer victimization and anxiety and depression. Overall, research highlights the significance of teacher support in peer victimization and adverse psychosocial outcomes.
Future orientation is another protective factor that is likely to buffer the effects of peer victimization (Hamilton et al. 2015). Future orientation is understood as the way one looks at the future; their ability to dictate the direction that their life is moving in and the role that they play in shaping their future. According to Nurmi (1991, 2005), future orientation includes thoughts, dreams, and expectations one has for future occurrences. Encouraging youth to focus on the future can motivate them to work towards and accomplish the goals that they have set for themselves (Kerpelman et al. 2008; Nurmi 1991, 2005). Studies on the significance of future orientation in adolescents bullying involvement are limited. However, one study, which included a racially diverse sample of 259 early adolescents, found that adolescents’ tendency to think about their future was found to affect whether peer and familial emotional victimization were related to a sense of hopelessness and depression (Hamilton et al. 2015).
Religiosity has been recognized as an important protective factor, especially for African American adolescents. Research on the relationship between religiosity and bullying and victimization is rare, although extant research has been inconsistent (Dutkova et al. 2017; Mercado-Crespo 2013). For example, Mercado-Crespo (2013) examined the role of religiosity in bullying involvement of 426 community-based samples of Puerto Rican pre-adolescents (ages 10–12 years). The findings appeared inconsistent across participants’ engagement in private and public religiosity practices. Private religiosity was negatively correlated to bullying perpetration and positively correlated to a bystander role. Public religiosity was positively associated with peer victimization. However, a recent study of 638 African American adolescents in an inner-city (ages 12–22 years) found that victimized youth who participate in religious services and affiliations were at lower risk of using illicit drugs than those who do not (Hong et al. 2019).
A Focus on Urban African American Adolescents
Urban African American adolescents encounter numerous risks in their neighborhood. However, many are capable of doing well despite the risks; as a result, there has been burgeoning support for examining multiple level factors that reduce negative outcomes of these youth (Gooden et al. 2016). Close relationships with parents, caring teachers, future orientation, and religiosity have been identified in the research literature as salient protective factors for urban African American adolescents who chronically experience violence (Benhorin et al. 2008; Hong et al. 2019; Salas-Wright et al. 2015; Stoddard et al. 2011). The presence of caring adults has a substantial and beneficial impact on African American adolescents, which fosters healthy psychosocial well-being and reduces adverse outcomes (e.g., internalizing symptoms) under conditions of high levels of stress (Benhorin et al. 2008). Additionally, for African American adolescents raised in a high-risk environment, a sense of hope for the future can promote positive development and diminish psychosocial problems associated with adversities (McCabe et al. 2000; So et al. 2016). Moreover, religion has been recognized as a defining feature of African American lives (Mattis et al. 2001) and not surprisingly, involvement in religion is found to help African American youth not only endorse prosocial values but also have better psychological functioning (Ball et al. 2003).
We aim to develop study hypotheses by exploring whether (1) peer victimization is positively associated with internalizing symptoms; (2) parental closeness, teacher’s care, positive future orientation, and religiosity might buffer the link between peer victimization and internalizing symptoms. The sample for the study includes early (ages 12–14) and middle adolescents (ages 15–17).
Method
Sample and Setting
The present study, a cross-sectional research, is a part of the Resilience Project (Voisin et al. 2016), which was conducted between August 2013 and January 2014. Data were collected from a convenience sampling of African American adolescents in four neighborhoods in Chicago’s Southside, which include Englewood, Woodlawn, Kenwood, and Southshore. Although a significant decline in crime was reported in Chicago, there remain disparities in crime in neighborhoods that are socially and economically disadvantaged, which includes the South and West sides of Chicago where a large proportion of African Americans live (Patton et al. 2017). Adolescents in Southside neighborhoods frequently report being exposed to violence, such as physical assaults, fighting, gun-related homicide, and murder (Patton et al. 2017).
The residents in these communities were predominantly African Americans of low income where the average annual mean income was between $24,049 and $35,946 (The average annual income in Chicago was $43,628.). The Southside of Chicago has been frequently portrayed as being seized by crime and violence in the media. However, all communities, regardless of structural hardships and disadvantages, have human and relational capital, which this study explores.
The study employs a convenience sample aimed to investigate factors that might protect adolescents from behavioral health risks in the presence of violence in the community. The adolescents were recruited from three high schools, one youth group in a church, two community programs for youth, and four public venues including parks, fast food restaurants, and movie theatres. To be eligible for the study, youth who were recruited had to self-identify as African American and between the ages of 12–24 years, which represented early to late adolescence. Adolescents who were under 18 years of age provided both informed assent and had a legal guardian who provided informed consent. Adolescents who were 18 years of age and older only provided consent. In terms of individuals who were enrolled and interviewed out of the number of individuals approached at each site, 579 out of 606 were in schools, 38 out of 42 were in community centers, 44 out of 49 were in churches, and 39 out of 56 were in public venues. The study sample reflected adolescents residing in the four neighborhoods in Chicago’s Southside. Of the 753 adolescents who were invited to participate in the study, the response rate was 87%. For the current analyses, only adolescents who were 17 years of age and younger were included, which represented early (ages 12–14) and middle (ages 15–17) adolescence (N = 546).
Procedure
Institutional Review Board was obtained prior to data collection. Permission from principals, church group leaders, and youth program leaders was first obtained before recruiting the study participants. Flyers, which included information about the study, were posted at each of the locations. Trained research assistants, undergraduate, and graduate students who completed human subjects training that included informed consent, privacy, and limits to confidentiality introduced the study to the potential participants. Each participant received a letter that included information about the study and parental consent forms. Only those who returned the signed consent forms were asked to participate in the study. Those who were recruited in public venues were asked to participate only in the presence of a parent or guardian. The surveys were administered in small groups whenever possible. The participants completed the self-administered questions in the presence of research assistants who were in charge of minimizing interruptions and maintaining confidentiality. Participants who were recruited from schools, churches, and community programs were given the questionnaire in spaces assigned by the venue. Those who were recruited from public venues (e.g., fast food venues) were given the questions in quiet areas at or near the venues. Questionnaires in those venues were only administered if a parent or guardian was present to give consent. The questionnaires lasted 45 min to complete and the participants were each given $10 for completing the questionnaire.
Measures
Internalizing symptoms were adapted from the Harvard National Depression Screening Scale (Baer et al. 2000). The variable was calculated from a sum of five items: “feeling blue”, “suddenly scared for no reason”, “spells of terror or panic”, “feeling so restless you couldn’t sit still”, and “feeling fearful or worried”. The items, which represent symptoms most frequently reported by urban youth, were selected. Each item was rated on a five-point scale: not at all (0), a little bit (1), moderately (2), quite a bit (3), and extremely (4). The internal reliability for the summary score was \(\alpha\) = 0.81. A summary score of internalizing symptoms ranges from 0 to 20, with a higher score indicating more internalizing symptoms (M = 2.80, SD = 3.84).
Peer victimization was adapted from the University of Illinois Victimization Scale (Espelage et al. 2001). The variable was measured from the sum of four items that represent both physical and verbal bullying most frequently experienced by urban youth: “other students picked on me”, “other students made fun of me”, “other students called me names”, and “I got hit and pushed by other students”. Each item was rated on a five-point scale: never (0), 1 or 2 times (1), 3 or 4 times (2), 5 or 6 times (3), and 7 or more times (4). The internal reliability for the summary score was \(\alpha\) = 0.89. A summary score of peer victimization ranges from 0 to 16, with a higher score indicating a greater frequency in peer victimization (M = 2.25, SD = 3.29).
Parental closeness was derived from the Add Health data, which consists of specific measures of parental behavior and parent–child interactions (Resnick et al. 1997). The variable was created from the sum of four items: “How close do you feel to your father?”, “How close do you feel to your mother?”, “How much do you think your father cares about you?”, and “How much do you think your mother cares about you?” Response options for each item are: not at all (0), very little (1), somewhat (2), quite a bit (3), and very much (4). The internal consistency was \(\alpha\) = 0.74. The higher score indicating a higher level of closeness with parents (M = 15.76, SD = 3.96).
Teacher’s care was from the modified Questionnaire on Teacher Interaction (Wubbels et al. 1991) and was created from the summed score of four items: “The teachers at my school treat me fairly”, “My teachers care about me”, “Teachers at my school treat kids fairly”, and “Teachers in my school really care about the feelings of their students”. The items selected represent youths’ perceptions of their teachers as caring. Response options are: strongly disagree (0), disagree (1), neither agree/disagree (2), agree (3), and strongly agree (4). The internal consistency was \(\alpha\) = 0.87. Higher scores indicated a higher level of teacher’s care (M = 14.20, SD = 3.66).
Religiosity was derived from the modified Religious Involvement Scale (Roth et al. 2012). Religiosity was calculated from the sum of three items: “In an average month, how often do you pray or meditate”; “In an average month, how often do you attend church and/or other religious services”; “In an average month, how often do you talk to others about religious or spiritual concerns”. Response options are: never (0), once in a while (1), fairly often (2), and very often (3). The internal consistency was \(\alpha\) = 0.74. Higher score indicated more involvement in religious activities (M = 7.15, SD = 2.38).
Positive future orientation was assessed with a modified version of Coopersmith’s (1967) Self-Esteem Inventory. The variable was created from the sum of three items: “What happens to my future mostly depends on me”, “I can do just about anything I really set my mind to do”, and “I have great faith in the future”. Each item was rated on a three-point scale: not true (0), somewhat or sometimes true (1), and very true or often true (2). The internal consistency was \(\alpha\) = 0.84. Higher score indicated higher level of positive future orientation (M = 7.38, SD = 1.94).
Covariates for the study included age (fill-in-the-blank), sex (female [0], male [1]) and receipt of free or reduced lunch and/or SNAP benefits (government assistance; no [0], yes [1]).
Results
A series of multivariate regression analyses were conducted to examine the main and interaction effects of peer victimization on the level of internalizing symptoms with a total sample of adolescents. Another series of analyses were conducted with two separate age groups: age 12–14 and age 15–17. The analyses utilized STATA (v.16). First, a regression model examined the main effects of an independent variable and moderating variables on the level of internalizing symptoms, independently, while controlling other covariates. Second, another regression model was constructed, including interaction terms between four moderators and peer victimization: the interaction effect between parental closeness and peer victimization on internalizing symptom; the interaction effect between teacher’s care and peer victimization; the interaction effect between religiosity and peer victimization and another interaction effect of positive future orientation with peer victimization. The independent variable and moderators were mean-centered. The multiple imputation method was used for missing values (0–8.4%).
Descriptive Statistics and Correlation Analysis
Table 1 describes the sample characteristics. The average age of the youth was 15.46 (SD = 1.12, range: 12–17), 55.31% were female and 73.63% were receiving free or reduced lunch and/or SNAP benefits. Independent variables and covariates were modestly correlated with the level of internalizing symptoms (r = -0.17–0.34). The prevalence of internalizing symptoms was significantly higher among females than males (t = 2.67, df = 522, p < 0.05).
Multiple Regression Analyses
Total Sample
Table 2 presents the result from multiple regression analyses examining the main effects of peer victimization and potential moderating variables on the level of internalizing symptoms. The overall model fit were significant (F(8, 491.2) = 11.97, p < 0.001, R2 = 0.17). Peer victimization was positively related to the level of internalizing symptoms (B = 0.37, p < 0.001), indicating that greater frequency in peer victimization was related to more internalizing symptoms. A higher level of parental closeness was marginally related to less internalizing symptoms (B = − 0.08, p = 0.06). High level of teacher’s care was related to less internalizing symptoms (B = − 0.12, p < 0.01). Also, a high level of positive future orientation was marginally related to less internalizing symptoms (B = − 0.15, p = 0.09). However, the high level of religiosity was significantly related to the more internalizing symptoms (B = 0.15, p < 0.05).
Four interaction terms were added to the initial model to examine the moderating effects of four variables (parental closeness, teacher’s care, religiosity, and positive future orientation) (see Table 2). The overall model fits are significant (F(12,485.5) = 8.61, p < 0.001, R2 = 0.18). The two-way interaction term was significant for parental closeness (B = − 0.03, p < 0.05). However, the moderating effects of the other three variables were not reported.
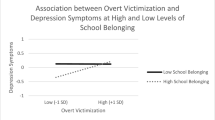
Figure 2 indicates three slopes representing the relationship between peer victimization and the level of internalizing symptoms at the three points of parental closeness (− 1SD, M, + 1SD). At all three points, more frequent peer victimization was related to higher internalizing symptoms, consistent with the results of the main effect. However, the effect of peer victimization on the internalizing symptoms was stronger when adolescents had a lower level of parental closeness (see Fig. 2).

Parental closeness as a moderator of the association between peer victimization and internalizing symptoms
Age Group Differences
Table 3 presents the result from multiple regression analyses examining the main effects of peer victimization and potential moderating variables on the level of internalizing symptoms among two age groups: ages 12–14 and 15–17. The overall model fit were significant (F(8, 103.2) = 2.99, p < 0.01, R2 = 0.21) for adolescents ages 12–14 and (F(8, 391.0) = 8.79, p < 0.001, R2 = 0.16) for adolescents ages 15–17. Among adolescents ages 12–14, peer victimization was positively related to the level of internalizing symptoms (B = 0.38, p < 0.01), indicating that greater frequency in peer victimization was related to more internalizing symptoms. Among adolescents ages 15–17, peer victimization related to greater internalizing symptoms (B = 0.36, p < 0.001). High level of teacher’s care was related to less internalizing symptoms (B = − 0.14, p < 0.05).
Four interaction terms were added to the initial model to examine the moderating effects of four variables (parental closeness, teacher’s care, religiosity, and positive future orientation) (see Table 3). The overall model fits are significant (F(12, 99.2) = 2.05, p < 0.05, R2 = 0.23) for adolescents ages 12–14 and (F(12, 386.4) = 6.70, p < 0.05, R2 = 0.18) for adolescents ages 15–17. Among adolescents ages 12–14, peer victimization remained significant (B = 0.38, p < 0.05). However, the moderating effects of the other three variables were not significant. For adolescents ages 15–17, peer victimization (B = 0.36, p < 0.001), parental closeness (B = − 0.10, p < 0.05), and teacher’s care (B = − 0.14, p < 0.01) were significant. In terms of the interactions, parental closeness moderated the association between peer victimization and internalizing symptoms (B = − 0.04, p < 0.05).
Figure 3 indicates three slopes representing the association between peer victimization and the level of internalizing symptoms at the three points of parental closeness (− 1SD, M, + 1SD) for adolescents ages 15–17. All three points show that more frequent peer victimization was associated with higher internalizing symptoms. However, the effect of peer victimization on the internalizing symptoms was stronger when adolescents had a lower level of parental closeness (see Fig. 3).

Parental closeness as a moderator of the association between peer victimization and internalizing symptoms among adolescents ages 15–17
Discussion
The present study investigated whether peer victimization was positively related to internalizing symptoms from a sample of African American adolescents in four neighborhoods in Chicago’s Southside. The study also examined whether parental closeness, teacher’s care, positive future orientation, and religiosity might buffer the association between peer victimization and internalizing symptoms from a sample of early (ages 12–14) and middle (ages 15–17) adolescents. The study demonstrated the importance of developing hypotheses to test whether parental closeness buffers the linkage between peer victimization and internalizing symptoms. Our findings showed that both early and middle adolescent participants in our study who reported experiencing victimization by their peers were at an increased risk of internalizing symptoms, which was in line with prior findings (Farmer et al. 2015; Reijntjes et al. 2010; Schwartz et al. 2015). Similar to other adolescents, bullying appears to be aversive and humiliating for the participants in our study, which is likely to reinforce negative self-appraisal, depressive symptoms, and fear of social interactions (Reijntjes et al. 2010).
Our results also indicated that parental closeness moderated the positive association between peer victimization and internalizing symptoms among the total study participants, which was consistent with previous study findings (Kotchick et al. 2020; Rudolph et al. 2020; Stadler et al. 2010). Interestingly, when the sample was grouped into early and middle adolescents, we found that parental closeness buffered the association between peer victimization and internalizing symptoms among middle adolescents. This finding provided partial support for hypothesizing parental closeness as a moderator of the association between peer victimization and internalizing symptoms. The finding is also in line with Fergus et al.’s (2005) Risk and Resilience Model. In other words, adolescents who reported feeling close to their parents were less likely to exhibit internalizing symptoms when bullied. These findings support other findings (e.g., Zimmerman et al. 2000a, b) that reported parental support plays a significant role in compensating for and protecting against risks African American youth encounter in their community. The findings also appear to be consistent with the stress-buffering model, which proposes that social support and care from parents might have a buffering role on the deleterious effects (e.g., internalizing symptoms) of high levels of stressors (e.g., peer victimization) (Zimmerman et al. 2000a, b). Moreover, parental support as a moderator of the peer victimization-internalizing symptoms linkage is undergirded by parents’ unconditional acceptance of and attachment with the child, which is an example of the microsystem effect. The family context, which is a source of parent–child attachment, is relevant to positive interpersonal connections with peers and teachers. Scholars are urged to propose and test whether parental closeness moderates the association between peer victimization and internalizing symptoms from a probability sample of African American adolescents in four urban neighborhoods.
Inconsistent with prior research and the Risk and Resilience Model, teacher’s care, religiosity, and positive future orientation did not independently buffer the association between peer victimization and internalizing symptoms among early and middle adolescents. Although other studies have examined various aspects of teacher support, such as involvement, our study only considered adolescents’ perceptions of their teachers as showing care, which might have affected the results. Although teacher’s care was negatively associated with internalizing symptoms, which might suggest that teachers play an important role in students’ psychosocial well-being, teachers are likely to be limited in their ability to assist students who are bullied by their peers. Possibly, unlike suburban schools, teachers in urban schools are confronted with a lack of resources, excessive teaching or workload and school-level disorganization (Shernoff et al. 2011), which are likely to impede opportunities to assist students who are bullied. It is also possible that teachers’ display of caring attitude does not necessarily mean they are likely to intervene in bullying situations, which most frequently occur in the absence of adult authority figures.
Although widely recognized as a salient protective factor against psychosocial distress and harmful behaviors among African Americans (e.g., Chatters et al. 2011; Childs et al. 2008; Fowler et al. 2008), our findings were contrary to past research (Hong et al. 2019). Also, inconsistent with the Risk and Resilience Model, religiosity was not found to be negatively associated with internalizing symptoms nor did it buffer the link between peer victimization and internalizing symptoms. Although religiosity is recognized as an important protective factor as indicated in various findings, involvement in religious services or activities is not likely to shield urban youth from exposure to violence, which can elevate their risk of peer victimization. Also, possibly, praying or talking to others about religious or spiritual concerns might not necessarily equip adolescents to avoid or address peer victimization risks in school or in their neighborhood where violence might be a frequent occurrence.
Positive future orientation was negatively correlated with internalizing symptoms; however, it was not shown to moderate the association between peer victimization and internalizing symptoms among the sample in our study. This finding was also contradictory to other research findings (e.g., Hamilton et al. 2015) and the Risk and Resilience Model. In our study, future orientation was measured as “What happens to my future mostly depends on me,” “I can do just about anything I really set my mind to do,” and “I have great faith in the future”, which might give urban adolescents a sense of hope for their future. However, because bullying is a repeated occurrence, victims of bullying might find their situation to be unavoidable and hopeless, which can trigger internalizing symptoms, such as depression and anxiety.
Limitations and Implications for Future Research
The findings of this study shed light on the importance of proposing and hypothesizing what protective factors might mitigate the relationship between peer victimization and internalizing symptoms. However, they should be interpreted cautiously given several limitations. The cross-sectional study design impedes any ability to make causal or temporal inferences. Also, the convenience sampling used in the study limits the generalizability of the study findings to African American adolescents outside of these communities or in other urban areas. Additionally, it has been argued that inferential statistics are not suitable for research with a non-probability sample, making it difficult to determine whether there is nesting in the data (e.g., whether the participants attended the same schools or had the same teachers). The assumption of independence is a concern, particularly for variables such as teacher’s care. As a result, the convenience sampling used in this study limits confidence in the findings and probability sampling is necessary for hypothesizing protective factors that moderate the association between peer victimization and internalizing symptoms among these youth.
Moreover, the study data were collected from a self-administered questionnaire and the responses were derived exclusively from the adolescents, which likely have introduced self-selection and social desirability biases, thus limiting the validity of the findings. Although possibly challenging, future research on African American adolescents in Southside neighborhoods that considers the perspectives of multi-informants (e.g., parents, peers, teachers) is highly suggested. Also, in examining teacher’s care, future research should consider not only gathering data from youth self-reports but also from parents or caregivers about home-school relationships, which would significantly increase the validity of the study findings. Another limitation is the measures of teacher’s care, religiosity, and positive future orientation, which might have affected our results. It is important to recognize that future orientation is complex and involves the experiences of youth in the development of competencies or individual assets, such as connection (e.g., positive bonds with people and institutions), character (e.g., integrity and moral focus) and confidence (e.g., positive self-regard, caring/compassion) through external assets or relationships established in a variety of programs or institutional groups (e.g. school-sponsored activities with teachers in schools, etc.). Given that this study addresses the experiences in peer victimization of urban African American youth in economically disadvantaged neighborhoods, it might be useful to build into ecological modeling some measures of parent and adolescent satisfaction with their community as well as the availability of community resources (e.g., health services). Finally, it would be useful to develop and test these hypotheses among African American adolescents residing in higher-income communities.
These limitations aside, findings from our study demonstrate the importance of developing hypotheses to propose and test protective and promotive factors that potentially attenuate adverse mental health linked to peer victimization. Our findings also provide some empirical support for the Risk and Resilience Model and the ecological systems perspective, which emphasizes the importance of how the systems levels are nested within one another (Bronfenbrenner 1977). Our findings that parental care is a protective buffer is consistent with Bronfenbrenner’s (1977) vision of the mesosystem level, which is the interrelations between and among the microsystems. In the present study, the quality of the relationship in the home (one microsystem) can affect adolescent peer relations (another microsystem), which provides support for considering not only the microsystems but also how various systems can influence one another and adolescent mental health.
Implications for School Mental Health Practice
The study findings also have potential implications for mental health services in school settings for the adolescent sample in our study. Adolescents spend significant time with their peers in schools and, peer victimization occurs most frequently in school settings. Additionally, anti-bullying programs are largely utilized in school by school practitioners (e.g., counselors, social workers) who provide an array of mental health services for students. As our findings have shown, positive relations with parents diminish the adverse psychological outcomes of stressors. Hence, school practitioners in these schools are strongly encouraged to assess factors beyond school context, such as parental relationships and parental support in anti-bullying efforts. As indicated in two meta-analytic reviews, school-based anti-bullying programs that include parent-related factors are effective (Chen et al. 2020; Huang et al 2019). However, protective factors are rarely assessed for mental health programs in urban schools due to the fragmentation and a lack of coordination, which likely results in a system that neither allocates the needed resources effectively nor attends to the services provided (Atkins et al. 2006; Knitzer 2000).
Notwithstanding these barriers, the quality of the parent-adolescent relationship in school-based bullying intervention is critical in the school districts in the four neighborhoods in Chicago’s Southside. Although enhancing parental closeness might be necessary for diminishing the strength of the relationship between peer victimization and internalizing symptoms, it is important to understand that targeting parental closeness might be challenging in settings that are poorly resourced and in families where there are higher proportions of single-female headed households. Thus, there is a critical need for mental health service providers in these schools to assess socioeconomic factors and how they might impact the development, mode of delivery and efficacy of treatment (Farahmand et al. 2011). Over 70% of all research on treatment outcomes does not consider the socioeconomic characteristics of the participants (Weisz et al. 2005). However, school mental health practitioners in the four school districts are recommended to work closely with youth workers in urban areas to assess the availability of community resources, such as health services and community mental health centers. The prevalence of bullying coupled with negative psychological outcomes supports a schoolwide intervention to addressed bullying, which has long been advocated by researchers (Brewster et al. 2018). Such a task would require extensive training and ongoing supports of all the relevant stakeholders, including parents and school personnel (Letendre et al. 2016). More importantly, a comprehensive anti-bullying policy and communication mechanisms need to be established in the school districts, which should include identification of students who are bullying others, students who are being bullied, and bystanders (Bowllan 2011). To effectively prevent and address bullying in Chicago’s Southside neighborhoods, a coordinated effort amongst the relevant stakeholders, particularly parents, is necessary; however, this would first require identifying barriers experienced by families in these neighborhoods and how to address them.
Conclusion
Hypothesis-testing approaches to research have contributed significantly to our understanding of the relationship between peer victimization and adolescent mental health. However, hypothesis-generation is another research approach that can provide greater opportunities for further research discoveries of the results that were unanticipated or unintended by the study design (Biesecker 2013). The hypothesis-generating approach can provide critical insights into making decisions on what types of hypotheses are plausible or worth testing. For instance, contrary to other studies, our findings showed that teacher’s care, religiosity, and positive future orientation did not buffer the association between peer victimization and internalizing symptoms among our sample. Although these are salient variables that have been widely hypothesized to attenuate the relationship between peer victimization and psychosocial outcomes, they did not protect adolescents from internalizing symptoms when victimized by peers. Among the adolescents in our sample, teacher’s care, religiosity, and positive future orientation might be constrained by external factors, which requires further research to generate more viable hypotheses. Additionally, our findings indicated that parental closeness was a protective buffer for middle adolescents only, which seems to suggest that researchers consider age differences when generating hypotheses related to peer victimization of adolescents. In total, findings from our study demonstrate the importance of considering a hypothesis-generating approach, which can facilitate a better understanding of what protective factors should be seriously considered in disrupting the linkage between peer victimization and internalizing symptoms.
Data Availability
The authors assume responsibility for the accuracy of the data analysis.
References
Atkins, M. S., Frazier, S. L., Birman, D., Adil, J. A., Jackson, M., Graczyk, P. A., Talbott, E., Farmer, A. D., Bell, C. C., & McKay, M. M. (2006). School-based mental health services for children living in high poverty urban communities. Administration and Policy in Mental Health and Mental Health Services Research, 33(2), 146159. https://doi.org/10.1007/s10488-006-0031-9
Archer, J., & Coyne, S. M. (2005). An integrated review of indirect, relational and social aggression. Personality and Social Psychology Review, 9(3), 212–230. https://doi.org/10.1207/s15327957pspr0903_2
Baer, L., Jacobs, D. G., Meszler-Reizes, J., Blais, M., Fava, M., Kessler, R., & Leahy, L. (2000). Development of a brief screening instrument: the HANDS. Psychotherapy and Psychosomatics, 69, 35–41. https://doi.org/10.1159/000012364
Baldry, A. C. (2004). The impact of direct and indirect bullying on the mental and physical health of Italian youngsters. Aggressive Behavior, 30(5), 343–355. https://doi.org/10.1002/ab.20043
Ball, J., Armistead, L., & Austin, B. J. (2003). The relationship between religiosity and adjustment among African-American, female, urban adolescents. Journal of Adolescence, 26(4), 431–446. https://doi.org/10.1016/S0140-1971(03)00037-X
Barzilay, S., Klomek, A. B., Apter, A., Carli, V., Wasserman, C., Hadlaczky, G., & Brunner, R. (2017). Bullying victimization and suicide ideation and behavior among adolescents in Europe: A 10-country study. Journal of Adolescent Health, 61(2), 179–186. https://doi.org/10.1016/j.jadohealth.2017.02.002
Benhorin, S., & McMahon, S. D. (2008). Exposure to violence and aggression: Protective roles of social support among urban African American youth. Journal of Community Psychology, 36(6), 723–743. https://doi.org/10.1002/jcop.20252
Biesecker, L. G. (2013). Hypothesis-generating research and predictive medicine. Genome Research, 23(7), 1051–1053. https://doi.org/10.1101/gr.157826.113
Bowllan, N. M. (2011). Implementation and evaluation of a comprehensive, school-wide bullying prevention program in an urban/suburban middle school. Journal of School Health, 81(4), 167–173. https://doi.org/10.1111/j.17460-1561.2010.00576.x
Brewster, S. L., Jr., Brewster, H. J., & Kulik, K. S. (2018). Bullying victimization in schools: Why the whole school, whole community, whole child model is essential. Journal of School Health, 88(11), 794–802. https://doi.org/10.1111/josh.12686
Bronfenbrenner, U. (1977). Toward an experimental ecology of human development. American Psychologist, 32(7), 513–531. https://doi.org/10.1037/0003-066X.32.7.513
Card, N. A., & Hodges, E. V. E. (2008). Peer victimization among schoolchildren: Correlations, causes, consequences and considerations in assessment and intervention. School Psychology Quarterly, 23(4), 451–461. https://doi.org/10.1037/a0012769
Chatters, L. M., Taylor, R., Jackson, J., Lincoln, K., Nguyen, A., & Joe, S. (2011). Church-based social support and suicidality among African American and Black Caribbeans. Archives of Suicide Research, 15(4), 337–353. https://doi.org/10.1080/13811118.2011.615703
Chen, Q., Zhu, Y., & Chui, W. H. (2020). A meta-analysis on effects of parenting programs on bullying prevention. Trauma, Violence, & Abuse. https://doi.org/10.1177/1524838020915619
Childs, G., Moneyham, L., & Felton, G. (2008). Correlates of sexual abstinence and sexual activity of low-income African-American adolescent females. Journal of the Association of Nurses in AIDS Care, 19(6), 432–442. https://doi.org/10.1016/j.jana.2008.04.013
Claes, L., Luyckx, K., Baetens, I., Van de Ven, M., & Witteman, C. (2015). Bullying and victimization, depressive mood and non-suicidal self-injury in adolescents: The moderating role of parental support. Journal of Child and Family Studies, 24(11), 3363–3371. https://doi.org/10.1007/s10826-015-0138-2
Coopersmith, S. (1967). The antecedents of self-esteem. W. H. Freeman.
Crick, N. R., & Nelson, D. A. (2002). Relational and physical victimization within friendships: Nobody told me there’d be friends like these. Journal of Abnormal Child Psychology, 30(6), 599–607. https://doi.org/10.1023/A:1020811714064
Curtner-Smith, M. E., Culp, A. M., Culp, R., Scheib, C., Owens, K., Tilley, A., Murphy, M., Parkman, L., & Colemann, P. W. (2006). Mothers’ parenting and young economically disadvantaged children’s relational and overt bullying. Journal of Child and Family Studies, 15(2), 181–193. https://doi.org/10.1007/s10826-005-9016-7
Dutkova, K., Holubeikova, J., Kravcova, M., Babincak, P., Tavel, P., & Geckova, A. M. (2017). Is spiritual well-being among adolescents associated with a lower level of bullying behaviour? The mediating effect of perceived bullying behaviour of peers. Journal of Religion and Health, 56, 2212–2221. https://doi.org/10.1007/s10943-017-0392-2
Eastman, M., Foshee, V., Ennett, S., Sotres-Alvarez, D., Reyes, H. L. M., Faris, R., & North, K. (2018). Profiles of internalizing and externalizing symptoms associated with bullying victimization. Journal of Adolescence, 65, 101–110. https://doi.org/10.1016/j.adolescence.2018.03.007
Espelage, D. L., & Holt, M. K. (2001). Bullying and victimization during early adolescence: Peer influences and psychosocial correlates. Journal of Emotional Abuse, 2(2–3), 123–142. https://doi.org/10.1300/J135v02n02_08
Estrada-Martinez, L. M., Caldwell, C. H., Bauermeister, J. A., & Zimmerman, M. A. (2012). Stressors in multiple life-domains and the risk for externalizing and internalizing behaviors among African Americans during emerging adulthood. Journal of Youth and Adolescence, 41, 1600–1612. https://doi.org/10.1007/s10964-012-9778-3
Farahmand, F. K., Grant, K. E., Polo, A. J., Duffy, S. N., & DuBois, D. L. (2011). School-based mental health and behavioral programs for low-income, urban youth: A systematic and meta-analytic review. Clinical Psychology: Science and Practice, 18(4), 372–390. https://doi.org/10.1111/j.1468-2850.2011.01265.x
Farmer, T. W., Irvin, M. J., Motoca, L. M., Leung, M., Hutchins, B. C., Brooks, D. S., & Hall, C. M. (2015). Externalizing and internalizing behavior problems, peer affiliations and bullying involvement across the transition to middle school. Journal of Emotional and Behavioral Disorders, 23(1), 3–16. https://doi.org/10.1177/1063426613491286
Fergus, S., & Zimmerman, M. A. (2005). Adolescent resilience: A framework for understanding healthy development in the face of risk. Annual Review of Public Health, 26, 399–419. https://doi.org/10.1146/annurev.publhealth.26.021304.144357
Fontenot, K., Semega, J., & Kollar, M. (2018). Income and poverty in the United States: 2017. Current Population Reports P60–263. U.S. Government Printing Office.
Ford, R., King, T., Priest, N., & Kavanagh, A. (2017). Bullying and mental health and suicidal behavior among 14- to 15-year-olds in a representative sample of Australian children. Australian and New Zealand Journal of Psychiatry, 51(9), 897–908. https://doi.org/10.1177/0004867417700275
Fowler, P. J., Ahmed, S. R., Tompsett, C. J., Jozefowicz-Simbeni, D. M. H., & Toro, P. A. (2008). Community violence and externalizing problems: Moderating effects of race and religiosity in emerging adulthood. Journal of Community Psychology, 36(7), 835–850. https://doi.org/10.1002/jcop.20267
Gladden, R. M., Vivolo-Kantor, A. M., Hamburger, M. E., & Lumpkin, C. D. (2014). Bullying surveillance among youths: Uniform definitions for public health and recommended data elements, Version 1.0. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention and U.S. Department of Education.
Goldweber, A., Waasdorp, T. E., & Bradshaw, C. P. (2013). Examining associations between race, urbanicity and patterns of bullying involvement. Journal of Youth and Adolescence, 42, 206–219. https://doi.org/10.1007/s10964-012-9843-y
Gooden, A. S., & McMahon, S. D. (2016). Thriving among African-American adolescents: Religiosity, religious support and communalism. American Journal of Community Psychology, 57(1–2), 118–128. https://doi.org/10.1002/ajcp.12026
Hamilton, J. L., Connolly, S. L., Liu, R. T., Stange, J. P., Abramson, L. Y., & Alloy, L. B. (2015). It gets better: Future orientation buffers the development of hopelessness and depressive symptoms following emotional victimization during early adolescence. Journal of Abnormal Child Psychology, 43, 465–474. https://doi.org/10.1007/s10802-014-9913-6
Hayes, A. F. (2013). An introduction to mediation, moderation and conditional process analysis. Guilford Press.
Hong, J. S., Kim, D. H., Lee, C. A., Russ, R., Johns, S., & Voisin, D. R. (2019). Peer victimization and illicit drug use among African American adolescents in Chicago: The moderating effects of religious affiliation. Journal of the Society for Social Work and Research, 10(3), 333–348. https://doi.org/10.1086/704061
Huang, Y., Espelage, D. L., Polanin, J. R., & Hong, J. S. (2019). A meta-analytic review of school-based anti-bullying programs with a parent component. International Journal of Bullying Prevention, 1, 32–44. https://doi.org/10.1007/s42380-018-0002-1
Joe, S., Baser, R., Neighbors, H., Caldwell, C., & Jackson, J. (2009). 12-month and lifetime prevalence of suicide attempts among black adolescents in the National Survey of American Life. Journal of the American Academy of Child and Adolescent Psychiatry, 48(3), 271–282. https://doi.org/10.1097/CHI.obo13e318195bccf
Kann, L., McManus, T., Harris, W., Shanklin, S., Flint, K., Queen, B., & Ethier, K. (2018). Youth risk behavior surveillance — United States, 2017 (Surveillance Summaries). Centers for Disease Control and Prevention. https://www.cdc.gov/healthyyouth/data/yrbs/pdf/2017/ss6708.pdf
Kerpelman, J. L., Eryigit, S., & Stephens, C. J. (2008). African American adolescents’ future education orientation: Associations with self-efficacy, ethnic identity and perceived parental support. Journal of Youth and Adolescence, 37, 997–1008. https://doi.org/10.1007/s10964-007-9201-7
Knitzer, J. (2000). Helping troubled children and families: A paradigm of public responsibility. In J. Rappaport & E. Seidman (Eds.), Handbook of community psychology (pp. 541–563). Springer.
Kotchick, B. A., Papadakis, A. A., Nettles, C., & Jobe, S. L. (2020). Peer victimization and depressive symptoms in early adolescents: The protective role of perceived supportive parenting. Journal of Child and Family Studies, 29, 1350–1362. https://doi.org/10.1007/s10826-019-01610-6
Lebrun-Harris, L. A., Sherman, L. J., Limber, S. P., Miller, B. D., & Edgerton, E. A. (2019). Bullying victimization and perpetration among U.S. children and adolescents: 2016 National Survey of Children’s Health. Journal of Child and Family Studies, 28, 2543–2557. https://doi.org/10.1007/s10826-018-1170-9
Letendre, J., Ostrander, J. A., & Mickens, A. (2016). Teacher and staff voices: Implementation of a positive behavior bullying prevention program in an urban school. Children & Schools, 38(4), 237–245. https://doi.org/10.1093/cs/cdw032
Li, S. T., Nussbaum, K. M., & Richards, M. H. (2007). Risk and protective factors for urban African-American youth. American Journal of Community Psychology, 39, 21–35. https://doi.org/10.1007/s10464-007-9088-1
Lindau, S. T., Makelarski, J. A., Chin, M. H., Desautels, S., Johnson, D., Johnson, W. E., Jr., Miller, D., Peters, S., Robinson, C., Schneider, J., Thicklin, F., Watson, N. P., Wolfe, M., & Whitaker, E. (2011). Building community-engaged healthy research and discovery infrastructure on the South Side of Chicago: Science in service to community priorities. Preventive Medicine, 52(3–4), 200–207. https://doi.org/10.1016/j.ypmed.2011.01.001
Lucas-Molina, B., Williamson, A. A., Pulido, R., & Perez-Albeniz, A. (2015). Effects of teacher-student relationships on peer harassment: A multilevel study. Psychology in the Schools, 52(3), 298–315. https://doi.org/10.1002/pits.21822
Mann, M. J., Kristjansson, A. L., Sigfusdottir, I. D., & Smith, M. L. (2015). The role of community, family, peer and school factors in group bullying: Implications for school-based intervention. Journal of School Health, 85(7), 477–486. https://doi.org/10.1111/josh.12270
Mattis, J. S., & Jagers, R. J. (2001). A relational framework for the study of religiosity and spirituality in the lives of African Americans. Journal of Community Psychology, 29(5), 519–539. https://doi.org/10.1002/jcop.1034
McCabe, K., & Barnett, D. (2000). First comes work, then comes marriage: Future orientation among Africa American young adolescents. Family Relations, 49(1), 63–70. https://doi.org/10.1111/j.1741-3729.2000.00063.x
Mercado-Crespo, M. C. (2013). The role of connectedness and religious factors on bullying participation among preadolescents in Puerto Rico (Doctoral dissertation, University of South Florida). http://scholarcommons.usf.edu/etd/4545/
Musu, L., Zhang, A., Wang, K., Zhang, J., & Oudekerk, B. A. (2019). Indicators of school crime and safety: 2018 (NCES 2019–047/NCJ 252571). National Center for Education Statistics, U.S. Department of Education and Bureau of Justice Statistics, Office of Justice Programs, U.S. Department of Justice.
Nurmi, J. -E. (1991). How do adolescents see their future? A review of the development of future orientation and planning. Developmental Review, 11(1), 1–59. https://doi.org/10.1016/0273-2297(91)90002-6
Nurmi, J. -E. (2005). Thinking about and acting upon the future: Development of future orientation across the life span. In A. Stratham & J. Joireman (Eds.), Understanding behavior in the context of time: Theory, research and application (pp. 31–57). Lawrence Erlbaum Associates, Publishers.
Patton, D. U., Sanchez, N., Fitch, D., Macbeth, J., & Leonard, P. (2017). I know God’s got a day 4 me: Violence, trauma and coping among gang-involved Twitter users. Social Science Computer Review, 35(2), 226–243. https://doi.org/10.1177/0894439315613319
Pengpid, S., & Peltzer, K. (2019). Bullying victimization and externalizing and internalizing symptoms among in-school adolescents from five ASEAN countries. Children and Youth Services Review, 106, 104473. https://doi.org/10.1016/j.childyouth.2019.104473
Reijntjes, A., Kamphuis, J. H., Prinzie, P., & Telch, M. J. (2010). Peer victimization and internalizing problems in children: A meta-analysis of longitudinal studies. Child Abuse & Neglect, 34(4), 244–252. https://doi.org/10.1016/j.chiabu.2009.07.009
Resnick, M. D., Bearman, P. S., Blum, R. W., Bauman, K. E., Harris, K. M., & Jones, J., Tabor, J., Beuhring, T., Sieving, R. E., Shew, M., Ireland, M., Bearinger, L. H., & Udry, J. R. (1997). Protecting adolescents from harm: Findings from the national longitudinal study on adolescent health. Journal of the American Medical Association, 287(10), 823–832. https://doi.org/10.1001/jama.1997.03550100049038
Roth, D. L., Mwase, I., Holt, C. L., Clark, E. M., Lukwago, S. N., & Kreuter, M. W. (2012). Religious involvement measurement model in a national sample of African Americans. Journal of Religion and Health, 51, 567–578. https://doi.org/10.1007/s10943-011-9475-7
Rudolph, K. D., Monti, J. D., Modi, H., Sze, W. Y., & Troop-Gordon, W. (2020). Protecting youth against the adverse effects of peer victimization: Why do parents matter? Journal of Abnormal Child Psychology, 48, 163–176. https://doi.org/10.1007/s10802-019-00576-9
Salas-Wright, C. P., Tirmazi, T., Lombe, M., & Nebbitt, V. E. (2015). Religiosity and antisocial behavior: Evidence from young African American women in public housing communities. Social Work Research, 39(2), 82–93. https://doi.org/10.1093/swr/svv010
Sanderson, R. C., & Richards, M. H. (2010). The after-school needs and resources of a low-income urban community: Surveying youth and parents for community change. American Journal of Community Psychology, 45, 430–440. https://doi.org/10.1007/s10464-010-9309-x
Schwartz, D., Lansford, J. E., Dodge, K. A., Pettit, G. S., & Bates, J. E. (2015). Peer victimization during middle childhood as a lead indicator of internalizing problems and diagnostic outcomes in late adolescence. Journal of Clinical Child & Adolescent Psychology, 44(3), 393–404. https://doi.org/10.1080/15374416.2014.881293
Shernoff, E. S., Mehta, T. G., Atkins, M. S., Torf, R., & Spencer, J. (2011). A qualitative study of the sources and impact of stress among urban teachers. School Mental Health, 3(2), 59–69. https://doi.org/10.1007/s12310-011-9051-z.
So, S., Voisin, D. R., Burnside, A., & Gaylord-Harden, H. K. (2016). Future orientation and health related factors among African American adolescents. Children and Youth Services Review, 61, 15–21. https://doi.org/10.1016/j.childyouth.2015.11.026
Stadler, C., Feifel, J., Rohrmann, S., Vermeiren, R. R. J. M., & Poustka, F. (2010). Peer-victimization and mental health problems in adolescents: Are parental and school support protective? Child Psychiatry and Human Development, 41, 371–386. https://doi.org/10.1007/s10578-010-0174-5
Stapinski, L. A., Araya, R., Heron, J., Montgomery, A. A., & Stallard, P. (2015). Peer victimization during adolescence: Concurrent and prospective impact on symptoms of depression and anxiety. Anxiety, Stress, & Coping, 28, 105–120. https://doi.org/10.1080/10615806.2014.962023
Stoddard, S. A., Zimmerman, M. A., & Bauermeister, J. A. (2011). Thinking about the future as a way to succeed in the present: A longitudinal study of future orientation and violent behaviors among African American youth. American Journal of Community Psychology, 48, 238–246. https://doi.org/10.1007/s10464-010-9383-0
Sulkowski, M. L., & Simmons, J. (2018). The protective role of teacher-student relationships against peer victimization and psychosocial distress. Psychology in the Schools, 55(2), 137–150. https://doi.org/10.1002/pits.22086
Voisin, D. R., Elsaesser, C., Kim, D. H., Patel, S., & Cantara, A. (2016). The relationship between family stress and behavioral health among African American adolescents. Journal of Child and Family Studies, 25, 2201–2210. https://doi.org/10.1007/s10826-016-0402-0
Wang, J., Iannotti, R. J., & Nansel, T. R. (2009). School bullying among US adolescents: Physical, verbal, relational and cyber. Journal of Adolescent Health, 45(4), 368–375. https://doi.org/10.1016/j.jadohealth.2009.03.021
Weisz, J. R., Doss, A., & Hawley, K. M. (2005). Youth psychotherapy outcome research: A review and critique of the evidence base. Annual Review of Psychology, 56, 337–363. https://doi.org/10.1146/annurev.psych.55.090902.141449
Wubbels, T., & Levy, J. (1991). A comparison of interpersonal behaviour of Dutch and American teachers. International Journal of Intercultural Relations, 15, 1–18. https://doi.org/10.1016/0147-1767(91)90070-W
Yeung, R., & Leadbeater, B. (2010). Adults make a difference: The protective effects of parents and teacher emotional support on emotional and behavioral problems of peer-victimized adolescents. Journal of Community Psychology, 38(1), 80–98. https://doi.org/10.1002/jcop.20353
Yoshikawa, H., & Seidman, E. (2000). Competence among urban adolescents in poverty: Multiple forms, contexts and developmental processes. In R. Montemayor, G. R. Adams, & T. P. Gullotta (Eds.), Adolescent diversity in ethnic, economic and cultural contexts (pp. 9–42). Sage Publications, Inc.
Zimmerman, M. A., Ramirez-Valles, J., Zapert, K. M. N., & Maron, K. I. (2000a). A longitudinal study of stress-buffering effects for urban African-American male adolescent problem behaviors and mental health. Journal of Community Psychology, 28, 17–33. https://doi.org/10.1002/(SICI)1520-6629(200001)28:1%3c117::AID-JCOP4%3e3.0.CO;2-1
Zimmerman, M. A., Salem, D. A., & Notaro, P. C. (2000b). Make room for daddy II: The positive effects of fathers’ role in adolescent development. In R. D. Taylor & M. C. Wang (Eds.), Resilience across contexts: Family, work, culture and community (pp. 233–253). Lawrence Erlbaum Associate Publishers.
Zwierzynska, K., Wolke, D., & Lereya, T. S. (2013). Peer victimization in childhood and internalizing problems in adolescence: A prospective longitudinal study. Journal of Abnormal Child Psychology, 41, 309–323. https://doi.org/10.1007/s10802-012-9678-8
Acknowledgements
The study was approved by the Institutional Review Board of the last author’s previous institution. The last author collected the data for the study and assumes responsibility for the integrity of the data.
Funding
This study was funded by the Center for Health Administration Studies and the STI/HIV Intervention Network at the University of Chicago, which were awarded to Dr. Dexter R. Voisin.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there is no conflict of interest.
Human or Animal Rights
There were no ethical issues regarding human participants/animals in the study.
Informed Consent
Informed consent was obtained prior to the data collection.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hong, J.S., Choi, M.J., Kim, I. et al. Identifying Protective Factors in the Association Between Peer Victimization and Internalizing Symptoms of African American Adolescents in Four Chicago’s Southside Neighborhoods. School Mental Health 13, 487–500 (2021). https://doi.org/10.1007/s12310-021-09433-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12310-021-09433-x