
Abstract
The extant literature suggests the importance of belonging in preventing and reducing internalizing symptoms. However, it is not yet clear which sources of belonging are most distinctly and robustly linked to symptoms of depression and anxiety. Further, the associations between various sources of belonging when also considering forms of peer victimization have not been readily examined. As such, the current study examined how peer, family, and school belonging are differentially associated with symptoms of depression and anxiety among middle school-age students (N = 256, Mage = 12.23 years, 52% male) when also considering the variance associated with forms of peer victimization. Further, sources of belonging were examined as moderators of the links between various forms of peer victimization and internalizing symptoms. Findings indicated that while family belonging was most robustly associated with depression symptoms, school belonging was most robustly associated with anxiety symptoms. Relational and cyber-, but not overt, victimization were distinctly and robustly associated with both symptom clusters. The only moderating effect evident was with school belonging and overt victimization, such that the association between overt victimization and depression symptoms was only evident when levels of school belonging were high. Findings contribute to our knowledge of distinct associations of various sources of belonging and further highlight the associations between peer victimization and internalizing symptoms among middle school students.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Belonging, or the companionship, affiliation, and connectedness that an individual feels within social relationships or groups (Lee & Robbins, 1995), is considered an essential human need and is often framed as a driving force for human behavior (DeWall et al., 2011; Leary & Cox, 2008). Belongingness is a multifaceted socio-ecological construct that captures individuals’ perceptions and identities within complex, overlapping social networks, and Bronfenbrenner’s ecological model of human development can be appropriately applied to describe how belongingness and its various domains are shaped by individuals’ interactions across systems (Bronfenbrenner, 1994). In turn, belongingness has consequences for the individual within their ecological systems. The current evidence suggests that having a sense of belonging, and specifically family and neighborhood belonging, is associated with lower levels of internalizing symptoms (e.g., Rejaan et al., 2022). Like belongingness, peer victimization can be conceptualized as the product of interactions across systems (Foster & Brooks-Gunn, 2013), with its own host of consequences for the individual. More research is needed to understand how various sources of belonging are more robustly and distinctly associated with symptoms of depression and anxiety and whether these associations are distinct from the links of various forms of peer victimization, with experiencing peer victimization being robustly associated with internalizing symptoms (e.g., Lucas-Molina, 2022; van der Wal, 2003; Hawker & Boulton, 2000). Further understanding of these distinct associations would be helpful in identifying these interpersonally driven pathways to symptoms of depression and anxiety and identify targets of prevention and intervention approaches. This research would allow one to know what type(s) of belonging and peer victimization are most important to address. To this end, the current study examined how peer, family, and school belonging were differentially associated with symptoms of depression and anxiety among rural middle school-age students. Additionally, whether effects held when also considering the variance associated with forms of peer victimization on symptoms of depression and anxiety was also evaluated. Finally, the potential moderating effects of various sources of belonging on links between forms of peer victimization and internalizing symptoms were examined. To date, Bronfenbrenner’s socio-ecological model has been applied to school belongingness (Allen et al., 2016, 2018, 2023). Specifically, the school environment itself can be conceptualized as a layered ecological system in which various layers influence children’s feelings of belonging (Allen et al., 2016). This application of a socio-ecological to the school environment accounts for factors across levels of the school system, including relational factors, such as peer victimization, as well as individual factors, which may contribute to adolescents’ internalizing symptoms (Allen et al., 2016, 2023). The current study aims to expand this model to include family and peer belongingness as components of youth microsystems and considers associations between belongingness and victimization with mental health outcomes for the individual.
Belonging
Belongingness serves evolutionary functions of ensuring survival (Baumeister & Leary, 1995; Malone et al., 2012) but also contributes to meaning-making (Stillman & Baumeister, 2009). Given its significance as a basic human need, it is unsurprising that belongingness is protective for psychosocial functioning. The protective influences of belongingness are consistent with the stress-buffering hypothesis, which proposes that social support has both main and moderating effects for mental health, as social support attenuates the influence of stress on health outcomes (Cohen & Wills, 1985). Unsurprisingly, belongingness may moderate the influence of stress on mental health by improving mood and meeting needs of nurturance and affiliation (Cohen & McKay, 1984). Feelings of belonging can come from many sources within an individual’s microsystem, including family, peers, and school. Family belonging may be protective for adolescents as they are transitioning to adulthood (King et al., 2018). Family belonging is modestly to moderately associated with lower levels of internalizing symptoms (Rejaän et al., 2022), including depressive symptoms (Jacobson & Rowe, 1999; King et al., 2018). Connectedness, which is often used interchangeably with belonging (e.g., Allen & Bowles, 2012), describes an individual’s social belonging as well as engagement with one’s social environment (Bowles & Scull, 2019). Family connectedness is also associated with reduced risk for suicide among adolescents (Borowsky et al., 2001). The benefits of family connectedness extend beyond depression to include anxiety. One study of Australian adolescents found that lower levels of family connectedness were moderately associated with increased anxiety (McGraw et al., 2008). In fact, family rituals predict lower levels of anxiety, and this relationship is likely mediated by family connectedness (Malaquias et al., 2015).
While family remains important, the influence of peers increases throughout early and middle adolescence (Sabatelli & Anderson, 1991; Schuler et al., 2019), and peer belongingness has its own implications for healthy development. Peer belonging is moderately protective for internalizing symptoms among Dutch (Rejaän et al., 2022) and Australian adolescents (McGraw et al., 2008). Moreover, peer belonging was found to be more robustly associated with internalizing symptoms than family and school belonging, with peer belonging moderately associated with internalizing symptoms and school and family belonging modestly associated with internalizing symptoms (Rejaän et al., 2022). Peer belonging may be more strongly linked to internalizing symptoms due to the fact that peers become increasingly important to youth identity and youth spend more time with peers during adolescence, and as such feeling a part of one’s peer group will impact one’s self-worth and self-evaluation (Sabatelli & Anderson, 1991; Schuler et al., 2019).
Further, youth spend much of their days and much of the year in school, and school environments provide middle school students opportunities for peer interactions and increasing independence from family (Roeser et al., 1998). One prospective study of Australian middle school-age youth found that school connectedness, a facet of school belonging, strongly predicts both depressive symptoms for boys and girls and strongly predicts anxiety symptoms for girls (Shochet et al., 2006). School belonging, in addition to peer and family belonging, is modestly associated with lower levels of loneliness and depression for urban, middle school students (Baskin et al., 2010). School belonging is also associated with reduced anxiety among low-income, urban adolescents (McMahon et al., 2008). In contrast, low levels of school connectedness are moderately associated with greater global and domain-specific (i.e., social, school-related) anxiety symptoms (Pikulski et al., 2020).
While there is compelling evidence that family, peer, and school belonging contribute to increased adolescent well-being, there is limited research on which of these three sources of belonging are most robustly and distinctly associated with symptoms of anxiety and depression in middle school (e.g., Rejaän et al., 2022).
Peer Victimization
Peer victimization refers to an individual’s experience of intentional acts of aggression by similar-aged individuals within one’s microsystem (Crick & Bigbee, 1998). Victimization can take many forms, with the most common being overt, relational, or cyber. Overt victimization consists of being physically (i.e., hit, pushed, or kicked) or verbally (i.e., intimidated or threatened) attacked that is perceived by the victim as being harmful. Relational victimization consists of rumor spreading, threats of friendship withdrawal, and ostracism, which can lead to damage to the victim’s social status and peer relationships (Armitage et al., 2021; Casper et al., 2017; Crick & Bigbee, 1998; Crick et al., 1999). Cyber-victimization is defined as being repeated intentionally harmful, offensive, derogatory, and unwanted behaviors that occur online (Kowalski et al., 2014; Wright & Wachs, 2019). Examples of this include hacking into someone’s account, sending degrading messages, and spreading rumors (Ang & Goh, 2010; Grigg, 2010; Patchin & Hinduja, 2006).
Numerous studies have shown that school-aged youth who are victims of peer victimization are more likely to experience internalizing symptoms such as anxiety and depression (Lucas-Molina, 2022; van der Wal, 2003; Hawker & Boulton, 2000), likely due to peer victimization disrupting key cognitive behavioral processes (e.g., increasing self-blaming attributions and social withdrawal; Rudolph et al., 2014; Schacter & Juvonen, 2015). More specifically, there is research supporting links between overt (e.g., Hawker & Boulton, 2000), relational (e.g., Hawker & Boulton, 2000; van der Wal, 2003), and cyber- (e.g., Lucas-Molina, 2022; Molero, 2022) victimization and symptoms of both depression and anxiety among children and adolescents. Note, however, that there is growing evidence suggesting that relational and cyber-victimization are more strongly linked to internalizing symptoms than overt victimization, with associations between relational victimization and internalizing symptoms being moderate, associations between cyber-victimization and internalizing symptoms being modest to moderate, and associations between overt victimization and internalizing symptoms being modest (e.g., Crick & Grotpeter, 1996; Dempsey et al., 2009; Kumpulainen et al., 1998; Landoll et al., 2015; Neary & Joseph, 1994; Slee, 1995; van der Wal, 2003; Williams et al., 1996; Yuchang et al., 2019). Moreover, there is some evidence to suggest that victimization is more strongly linked to symptoms of depression than anxiety symptoms (Drazdowski et al., 2019; Fite et al., 2023; Forbes et al., 2019; Sinclair et al., 2012; Storch & Ledley, 2005; Troop-Gordon et al., 2015); associations between victimization and anxiety range from modest to moderate (Forbes et al., 2019; Grills & Ollendick, 2002; Siegel et al., 2009; Storch et al., 2005), while associations between victimization and depression range from modest to large (Crick & Gotpeter; Dempsey et al., 2009; Forbes et al., 2019; Hawker & Boulton, 2000; Slee, 1995; Yuchang et al., 2019). As such, it is important to consider the unique influence of the various forms of peer victimization on distinct symptoms of depression and anxiety.
Unfortunately, this prior research does not inform our understanding of the unique and interactive effects of peer victimization and belonging on internalizing symptoms. Only one known study to date has examined belonging as moderator of the associations between peer victimization and internalizing symptoms. Wright and Wachs (2019) found that low levels of school belonging exacerbated the link between cyber-victimization and both depression and anxiety symptoms among middle school students. More specifically, low levels of school belongingness in seventh grade strengthened positive associations between cyber-victimization in seventh grade and depression and anxiety symptoms in eighth grade. Thus, consistent with a stress-buffering hypothesis, there is some evidence to suggest that experiencing low levels of belonging in tandem with being victimized can result in elevated internalizing symptoms. However, more research understanding the distinct and interactive effects of various sources of belonging and forms of peer victimization is warranted.
Current Study
Middle school is an especially sensitive developmental period characterized by rapid changes in brain and behavior (Paus et al., 2008). Because of structural and functional brain changes, increased social demands, and psychological stress, adolescence is a peak age of onset for anxiety and depression (Paus et al., 2008; Rudolph et al., 2001), though anxiety symptoms tend to appear earlier than depressive symptoms (Chaplin et al., 2009). Specifically, more than 5.8 million children experience anxiety and 2.7 million experience depression, with prevalence rates increasing across adolescence (CDC, 2022). Thus, understanding contributing factors for anxiety and depression in this rapidly developing age group is essential for early prevention and intervention (Allison et al., 2014).
Although there is evidence suggesting that low levels of belonging are associated with internalizing symptoms (e.g., Rejaan et al., 2022), more research is needed to understand which sources of belonging (peers, family, or school) are most strongly associated with various types of internalizing symptoms (i.e., symptoms of depression vs. anxiety). Further, it is not known how belonging is related to internalizing symptoms relative to experiencing various forms of peer victimization (relational, overt, and cyber), with peer victimization strongly and robustly linked to internalizing symptoms (e.g., Lucas-Molina, 2022; van der Wal, 2003; Hawker & Boulton, 2000). Moreover, the mitigating or exacerbating impacts of various sources of belonging on the links between peer victimization and internalizing symptoms warrant further investigation, as only one known study to date has examined the potential moderating effects of belonging (Wright & Wachs, 2019).
As such, the goals of the current study were to: (1) examine how peer, family, and school belonging are differentially associated with symptoms of depression and anxiety among middle school-age students, (2) evaluate whether these effects hold when also considering the effect of forms of peer victimization on symptoms of depression and anxiety, and (3) determine whether these various sources of belonging moderate the links between various forms of peer victimization and internalizing symptoms in middle school-age youth. The present study extends the extant literature (e.g., Rejaan et al., 2022) by further examining links between various sources of belonging and symptoms of depression and anxiety separately among middle school students while also considering forms of peer victimization. Further, the current study evaluates whether belonging contributes to the links between forms of peer victimization and symptoms of depression and anxiety.
All three sources of belonging were expected to be negatively associated with internalizing symptoms, but based on prior research (e.g., Rejaan et al., 2022), peer belonging was expected to be the most influential. However, given limitations in prior research (e.g., looking at internalizing symptoms broadly and/or not examining multiple sources of belonging in the same study), no hypotheses regarding magnitude of effects between specific sources of belonging and symptoms of depression versus anxiety were posited. Further note that the effects of belonging on internalizing symptoms were expected to be maintained even considering the effects of peer victimization. Relational and cyber-victimization were expected to be more strongly linked to both internalizing symptom clusters than overt victimization (Crick & Grotpeter, 1996; Kumpulainen et al., 1998; Landoll et al., 2015; Neary & Joseph, 1994; Slee, 1995; van der Wal, 2003; Williams et al., 1996), and these effects may be most robust with symptoms of depression than symptoms of anxiety (Drazdowski et al., 2019; Fite et al., 2023; Forbes et al., 2019; Sinclair et al., 2012; Storch & Ledley, 2005; Troop-Gordon et al., 2015). Finally, based on limited prior research (Wright & Wachs, 2019) and consistent with the stress-buffering hypothesis (Cohen & McKay, 1984; Cohen & Wills, 1985), low levels of belonging were expected to exacerbate the effects of peer victimization on internalizing symptoms. Specifically, peer and school belonging were expected to be more influential on the links between peer victimization and internalizing symptoms than family given that these sources of belonging are tied to peer relationships.
Methods
Participants
Participants were 256 students (52% male), ages 11–14 (M = 12.23 years). All students were enrolled in a public middle school in a rural community in the Midwestern US. Students were in sixth (32.8%), seventh (35.2%), and eighth (32.0%) grades at the time of data collection. The National Center for Education Statistics (2024) indicated that in Fall 2022, the racial/ethnic breakdown of students in the school was: 85% White (non-Hispanic), 1% Black, 6.5% Hispanic, and 7.5% two or more races/ethnicities. Note that eight youth responded as “other” when asked to identify their sex, and four youth chose not to respond to this question. Unfortunately, given the small sample size, those who chose “other” or did not respond regarding their sex were excluded from analyses.
Measures
Peer and Family Belonging
Youth reported their feelings of social (i.e., family and peer) belonging using the 6-item Milwaukee Youth Belongingness Scale—Revised Version (MYBS; Slaten et al., 2019). Family belongingness was captured by three items (e.g., “My family members like to spend time with me”), and peer belongingness was captured by three items (e.g., “I get along well with people my age”). Youth responded to items using a 4-point scale (1 = disagree; 5 = agree), and mean scores were used for both peer and family belongingness. This scale has established validity and reliability for the full measure and its subscales within Midwest middle school samples (Slaten et al., 2019). In the current study, internal consistency was modest (α = 0.65) for family belonging and was good (α = 0.85) for peer belonging.
School Belonging
Participants self-reported their feelings of school attachment/belonging using three items from the National Longitudinal Study of Adolescent Mood and Health (Moody & Bearman, 1998, as cited in Libbey, 2004). Youth responded to items (e.g., “I feel close to people at this school”) using a 5-point scale (1 = strongly disagree; 5 = strongly agree). A mean score was used. Prior studies have determined good internal consistency among middle and high school students in both rural and suburban schools (McNeely et al., 2010), and internal consistency for this measure was good (α = 0.82) for the current study.
Overt and Relational Victimization
Children self-reported victimization using the 9-item Victimization of Self Scale from the Peer Experiences Questionnaire (Dill et al., 2004). Overt victimization items captured physical acts of aggression that the child experienced (e.g., “a kid hit, kicked, or pushed me in a mean way”). Relational victimization items captured bullying behaviors that target the child’s peer relationships (e.g., “a kid told likes about me so other kids wouldn’t like me”). Youth responded to items using a 5-point scale (0 = never; 4 = few times a week). Mean scores for overt and relational victimization were used. Prior research has identified good internal consistency (Dill et al., 2004), and in the current study, internal consistency for overt victimization was acceptable (α = 0.74), and internal consistency for relational victimization was good (α = 0.87).
Cyber-Victimization
Participants self-reported cyber-victimization using six items from the 12-item European Cyberbullying Intervention Project Questionnaire (Del Rey et al., 2015). Items captured victimization experienced online or over text (e.g., “someone threatened me through texts or online messages”) in the past two months. Youth responded using a 5-point scale (0 = never; 4 = few times a week). Mean scores for cyber-victimization were used. Prior research has identified good internal consistency for the measure (Del Rey et al., 2015), and internal consistency for the current study was good (α = 0.89).
Depression Symptoms
Youth self-reported symptoms of depression using the 13-item Short Mood and Feelings Questionnaire (Sharp et al., 2006). This measure was developed as a self-report screening measure to assess depressive symptoms in both rural and urban community samples of children (Sharp et al., 2006). Items captured depressive symptoms (e.g., “I felt miserable or unhappy”) experienced in the past two weeks. Children responded using a 3-point scale (0 = not true; 2 = true). Mean scores for depressive symptoms were used. The scale has established validity and reliability among elementary and middle school students (Sharp et al., 2006; Thabrew et al., 2018), and internal consistency was good for the current study (α = 0.94).
Anxiety Symptoms
Youth self-reported anxiety symptoms using the 8-item Patient-Reported Outcomes Measurement Information System (PROMIS) Pediatric form for anxiety. This measure was developed to advance the application of youth-reported outcomes through item banks and computerized adaptive tests for clinical research (Irwin et al., 2010). Youth responded to questions about anxiety (e.g., “I felt like something awful might happen”) using a 5-point scale (0 = never; 4 = always). Mean scores for anxiety symptoms were used. This scale has established validity (Liu et al., 2016) and reliability (Irwin et al., 2010) among elementary, middle, and high school students. Internal consistency was good (α = 0.93) for the current sample.
Procedures
This study was approved by the researchers’ Institutional Review Board and school administrators. Guardian consent was obtained in the Fall of 2022 through online back-to-school enrollment packets, and youth assented at the beginning of the data collection session. Overall, 71.97% (n = 285) of caregivers consented for their child to participate, and 63.61% (N = 256) of the study body completed the survey. Through Qualtrics, a secure online platform, students completed a 30-min survey on their individual laptops, while survey items were read aloud by an audio recording. Trained research staff answered questions and assisted the youth when needed. Teachers and youth not taking the survey were not present in the classrooms in order to increase confidentiality and increase the accuracy of responses.
Data Analysis Plan
There was minimal missing data for the dataset (< 10%), and as such listwise deletion was used to accommodate missing data (Newman, 2014). This approach resulted in sample sizes between 236 and 256 for various analyses. Correlations among study variables were first estimated to determine bivariate associations. Specifically, point-biserial coefficients are reported for associations between one dichotomous and one continuous variable (i.e., any correlation with gender), and Pearson coefficients are reported for associations between two continuous variables (i.e., all association that do not include gender; Cohen et al., 2003).
A series of multiple regression models were then conducted for both symptoms of depression and anxiety. Note that skewness and kurtosis of the outcomes were less than 2 (depression symptoms: skewness = 1.43, kurtosis = 1.51; anxiety symptoms: skewness = 1.08, kurtosis = 0.77), suggesting non-normality was not a concern (George & Mallery, 2010; Hair et al., 2010). Prior to creating interaction terms and conducting regression analyses, all variables were standardized to aid in the interpretation of interaction effects (Aiken & West, 1991). First, symptoms of depression (or anxiety) were regressed on the three sources of belonging (peers, family, and school) while also considering age and gender as covariates, as age and gender differences in depression and anxiety are frequently evident in the literature (e.g., Chaplin et al., 2009). The three forms of peer victimization were then added to the initial model to determine whether the effects of belonging on internalizing symptoms remained when also considering the effect of peer victimization. Finally, the moderating effects of each of the sources of belonging were evaluated one at time by adding the multiplicative terms between the source of belonging and each form of peer victimization (e.g., family belonging X overt victimization, family belonging X relational victimization, and family belonging X cyber-victimization) to the model. Statistically significant interactions were then probed at high (+ 1 SD) and low levels (– 1 SD) of the source of belonging to determine the nature of the moderating effect (Aiken & West, 1991).
Results
Descriptive Statistics
Descriptive statistics and correlations among study variables are reported in Table 1. All sources of belonging were negatively associated with both symptoms of depression and anxiety (rs = − 0.22 to − 0.44, ps < 0.001), and all forms of peer victimization were positively associated with both symptoms of depression and anxiety (rs = 0.34–0.54, ps < 0.001). All forms of peer victimization were negatively associated with all sources of belonging (rs = − 0.18 to − 0.40, ps < 0.010). Older youth reported higher levels of family belonging (r = 0.16, p = 0.015) and school belonging (r = 0.14, p = 0.028) than younger youth, while younger youth reported higher levels of anxiety (r = − 0.15, p = 0.022) than older youth. Females reported higher levels of cyber- (r = 0.15, p = 0.025) and relational victimization (r = 0.13, p = 0.045) as well as symptoms of anxiety (r = 0.20, p = 0.002) than males. In contrast, males reported higher levels of overt victimization (r = − 0.13, p = 0.045) than females.
Multiple Regression Analyses
Symptoms of Depression
As seen in Table 2, females reported more symptoms of depression than males (β = 0.13, p = 0.020). All three sources of belonging were negatively associated with symptoms of depression (βs = − 0.16 to − 0.33, ps < 0.050). However, when forms of peer victimization were also considered, only family belonging remained statistically negatively associated with symptoms of depression (β = − 0.29, p < 0.001) with both relational and cyber-victimization, both positively associated with symptoms of depression (βs = 0.23 and 0.26, ps < 0.001). Further note that adjusted R2 increased when victimization was added to the model, suggesting that peer victimization is contributing to a substantial portion of the variance (see Table 2).
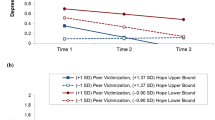
The moderating effects of each source of belonging were added to the model one at a time. No moderating effects of peer (βs = − 0.04 to 0.10, p > 0.150) or family belonging (βs = − 0.05 to 0.09, p > 0.190) were evident. School belonging, however, moderated the association between overt victimization and depression symptoms (β = 0.14, p = 0.013), but not cyber- or relational victimization (βs = − 0.05 to − 0.002, p > 0.210). At high levels of school belonging, overt victimization was positively associated with symptoms of depression (β = 0.28, p = 0.007). At low levels of school belonging, overt victimization was unrelated to symptoms of depression (β = − 0.004, p = 0.961). As seen in Fig. 1, at low levels of school belonging, symptoms of depression were slightly above the mean regardless of levels of overt victimization. In contrast, the lowest levels of depression were evident at high levels of school belonging and low levels of overt victimization. However, as overt victimization increased, so did symptoms of depression when levels of school belonging were high.

Association between overt victimization and depression symptoms at high and low levels of school belonging
Symptoms of Anxiety
As seen in Table 3, females reported higher levels of symptoms of anxiety than males. The only source of belonging associated with symptoms of anxiety was school belonging (β = − 0.24, p = 0.003), and this effect remained when considering peer victimization (β = − 0.15, p = 0.037). Cyber- and relational victimization were positively associated with symptoms of anxiety (βs = 0.16 and 0.36, ps < 0.015). Further note that adjusted R2 increased when victimization was added to the model, suggesting that peer victimization is contributing to a substantial portion of the variance (see Table 3).
The moderating effects of each source of belonging were added to the model one at a time. However, no moderating effects were evident for school belonging (βs = − 0.006 to 0.06, ps > 0.306), family belonging (βs = 0.05 to 0.09, ps > 0.207), or peer belonging (βs = 0.00 to 0.09, ps > 0.157).Footnote 1
Discussion
The current study adopted an ecological systems framework to extend the extant belonging literature by examining distinct associations between various sources of belonging (family, peers, and school) and symptoms of depression and anxiety while also considering the effects of various forms of peer victimization (i.e., relational, cyber, and overt). Further, sources of belonging were examined as potential moderators of the links between the forms of victimization and symptoms of depression and anxiety. Overall, findings suggest that belonging is robustly associated with symptoms of depression and anxiety over and above peer victimization. However, the robustness of findings depends on the source of belonging and symptoms of depression versus anxiety. Specific associations are discussed in turn.
Both correlation and regression analyses supported the links between higher levels of all three sources of belonging and lower levels of depression symptoms. However, only family belonging was associated with depression symptoms when also considering peer victimization. Findings are consistent with the prior literature linking family belonging to low levels of depression symptoms (Jacobson & Rowe, 1999; King et al., 2018). The prior literature also links peer (McGraw et al., 2008; Rejaän et al., 2022) and school (Baskin et al., 2010) belonging to internalizing symptoms; however, the current study is one of the first to examine distinct associations between sources of belonging and symptoms of depression specifically. It may be that family belonging is more strongly tied to symptoms of depression given that family belonging is established over a longer period of time. It may also be that peer victimization, being a negative peer influence, overpowers the positive aspects of social influence (belonging) within the school environment and among peer relationships.
In contrast, while correlation analyses supported a negative link between all sources of belonging and anxiety symptoms, regression analyses indicated that school belonging was the only source of belonging distinctly associated with anxiety symptoms. Further note that this effect remained when also considering peer victimization. Prior research has found a strong link between school connectedness (Pikulski et al., 2020; Schochet et al., 2006) or belonging (Baskin et al., 2010; McMahon et al., 2008) and internalizing symptoms. Interestingly, however, Rejaän et al. (2022) found that school belonging was not associated with a broad measure of internalizing symptoms among adolescents (10–19 years of age). It may be that these differences are due to not uniquely examining anxiety symptoms or that school-specific anxiety was not examined (e.g., Pikulski et al., 2020). Alternatively, it may be something specific about anxiety symptoms during middle school that was not captured in the Rejaän et al. (2022) study. School belonging may be particularly important to anxiety symptoms, over and above peer and family belonging, given the academic pressures that can contribute to various forms of anxiety. More research further delineating these associations is needed, however, before firm conclusions can be drawn.
Cyber- and relational victimization were robustly positively associated with both depression and anxiety symptoms. However, although correlated, overt victimization was not related to either symptom cluster when also considering the variance associated with other forms of victimization. Findings are consistent with prior research (Crick & Grotpeter, 1996; Kumpulainen et al., 1998; Landoll et al., 2015; Neary & Joseph, 1994; Slee, 1995; van der Wal, 2003; Williams et al., 1996), which indicates that relational and cyber-victimization are more strongly linked to internalizing symptoms than overt victimization. However, findings are not consistent with prior research suggesting that peer victimization may be more strongly linked to symptoms of depression than anxiety (Drazdowski et al., 2019; Fite et al., 2023; Forbes et al., 2019; Sinclair et al., 2012; Storch & Ledley, 2005; Troop-Gordon et al., 2015). The majority of this prior research was with elementary school-age youth, and it may be that the effects on anxiety become stronger during middle school. Nonetheless, the robust nature of effects for cyber- and relational victimization on both symptoms of depression and anxiety while also considering various sources of belonging further highlights the seriousness of peer victimization on maladjustment among middle school-age youth.
Finally, with one exception, it appears that the links between belonging and peer victimization and internalizing symptoms are largely independent of one another. However, school belonging was found to impact the link between overt victimization and symptoms of depression. Findings suggest that low levels of school belonging are associated with above average symptoms of depression regardless of levels of overt victimization, with the effects of overt victimization on depression symptoms only evident when levels of school belonging are high. This finding suggests that low levels of school belonging are associated with elevated symptoms of depression. Further, overt aggression is linked to symptoms of depression if it is happening in the context in which youth feel connected to their school. This finding may suggest that youth who feel a part of their school but are overtly victimized are feeling somewhat conflicted, that they like their school but that it does not feel safe, contributing to symptoms of depression. This finding may support a “reverse stress-buffering effect” (Rueger et al., 2022) in which social belonging is less protective in the context of negative peer interactions. This reduced effectiveness of school belonging under these stressful conditions may also be referred to as stress-dampening effects on social support. This finding is also consistent with the “health context paradox” reported in the bullying literature. This research has reported that bullied individuals in healthy contexts (i.e., schools where there is low victimization at the classroom level) demonstrate an enhanced association between bullying and internalizing problems and have more severe adaptation challenges (Huang et al., 2023). Note, however, that this finding is in contrast to prior research, which found that low levels of school belonging exacerbated the influence of cyber-victimization on symptoms of depression and anxiety (Wright & Wachs, 2019). It may be differences in cyber- versus overt victimization, with overt victimization being physically experienced. Further research examining these associations and the potential health context paradox theory is warranted to fully understand these interactive effects.
There are several limitations of the current study that inform its findings and implications. Firstly, the current study is cross-sectional, and as such conclusions about timing or causation cannot be inferred. Future research may benefit from measuring these constructs across middle school. Middle school is a developmentally sensitive period (Paus et al., 2008; Rudolph et al., 2001), making the age of the current study’s sample a strength. However, implications from the current study are limited to this age range, and relations between belonging, victimization, and internalizing symptoms likely differ for younger and older children. Future research should aim to examine these associations in elementary school- and high school-age youth. Participating youth were sampled from a predominantly White community, limiting the generalizability of findings. Prior research suggests racial/ethnic differences in prevalence rates for anxiety and depression (McLaughlin et al., 2007) as well as experiences of victimization (Turner et al., 2006). School and peer belonging may also differ for youth of color depending on racial or ethnic congruence (Georgiades et al., 2013). Finally, the internal consistency of the current family belonging measure was modest, likely due to the small number of items. Future work utilizing a more internally consistent measure would be beneficial.
Despite these limitations, the current study indicates that sources of belonging are differentially linked to depression versus anxiety symptoms, with family belonging being most important to symptoms of depression and school belonging being most important to symptoms of anxiety. Further, low levels of school belonging are consistently associated with above average symptoms of depression regardless of levels of overt victimization, while high levels of school belonging exacerbate the link between overt victimization and symptoms of depression. As such, belonging may be an important target of prevention and intervention, with findings indicating different intervention targets for symptoms of depression and anxiety. Examples of potential interventions include treatment plans that promote family belongingness and increasing family rituals (Malaquias et al., 2015) and positive parent–child relationships (King et al., 2018), and school programs that provide cognitive behavioral approaches including coping strategies and alternative actions, psychoeducation, and role-playing that are specific to relational and cyber-victimization (as opposed to general victimization; Polanin et al., 2022). Further, overt victimization must be addressed directly, and it needs to be understood that school belonging does not help mitigate the potential deleterious outcomes of experiencing such acts. Future research examining the distinct and interactive effects of belonging and peer victimization on symptoms of depression and anxiety is needed to fully understand these associations. Further, while exploratory analyses did not find gender differences in associations, future research examining potential gender differences, along with other potential influential factors (e.g., age) with larger sample sizes is warranted to fully understand these links. Additionally, the current study focused on symptoms of depression and anxiety. Future research may want to also understand how belonging and peer victimization contribute to stress and other negative emotions.
Notes
Additional exploratory gender interactions were examined. However, no two-way interactions between gender and the sources of belonging (βs = − 0.11 to 0.01, p ≥ .074) or three-way interactions between gender, sources of belonging, and peer victimization (βs = − 0.11 to 0.13, p ≥ .067) were evident.
References
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing and interpreting interactions. Sage Publication.
Allen, K. A., Berger, E., Reupert, A., Grove, C., May, F., Patlamazoglou, L., Gamble, N., Wurf, G., & Warton, W. (2023). Student-identified practices for improving belonging in Australian secondary schools: Moving beyond COVID-19. School Mental Health, 15(3), 927–39. https://doi.org/10.1007/s12310-023-09596-9
Allen, K. A., & Bowles, T. (2012). Belonging as a guiding principle in the education of Adolescents. Australian Journal of Educational & Developmental Psychology, 12, 108–119.
Allen, K.-A., Vella-Brodrick, D., & Waters, L. (2016). Fostering School Belonging in Secondary Schools Using a Socio-Ecological Framework. The Educational and Developmental Psychologist, 33(1), 97–121. https://doi.org/10.1017/edp.2016.5
Allen, K. A., Vella-Brodrick, D., & Waters, L. (2018). Rethinking school belonging: A socio-ecological framework. Pathways to Belonging (pp. 191–218). Brill.
Allison, V. L., Nativio, D. G., Mitchell, A. M., Ren, D., & Yuhasz, J. (2014). Identifying symptoms of depression and anxiety in students in the school setting. The Journal of School Nursing, 30(3), 165–172. https://doi.org/10.1177/1059840513500076
Ang, R. P., & Goh, D. H. (2010). Cyberbullying among adolescents: The role of effective and cognitive empathy, and gender. Child Psychiatry and Human Development, 41, 387–397. https://doi.org/10.1007/s10578-010-0176-3
Armitage, J. M., Wang, R. A. H., Davis, O. S. P., Bowes, L., & Haworth, C. M. A. (2021). Peer victimization during adolescence and its impact on wellbeing in adulthood: A prospective cohort study. BMC Public Health, 21(1), 148. https://doi.org/10.1186/s12889-021-10198-w
Baskin, T. W., Wampold, B. E., Quintana, S. M., & Enright, R. D. (2010). Belongingness as a protective factor against loneliness and potential depression in a multicultural middle school. The Counseling Psychologist, 38(5), 626–651. https://doi.org/10.1177/0011000009358459
Baumeister, R. F., & Leary, M. R. (1995). The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychological Bulletin, 117(3), 497–529. https://doi.org/10.1037/0033-2909.117.3.497
Borowsky, I. W., Ireland, M., & Resnick, M. D. (2001). Adolescent suicide attempts: Risks and protectors. Pediatrics, 107(3), 485–493. https://doi.org/10.1542/peds.107.3.485
Bowles, T., & Scull, J. (2019). The centrality of connectedness: A conceptual synthesis of attending, belonging, egaging and flowing. Journal of Psychologists and Counsellors in Schools, 29(1), 3–21. https://doi.org/10.1017/jgc.2018.13
Bronfenbrenner, U. (1994). Ecological models of human development. In Gauvain, M., & Cole, M. (Eds.), International Encyclopedia of Education (2nd ed., Vol. 3) Oxford: Elsevier. Reprinted in: Readings on the development of children, 2nd ed. (1993, pp. 37–43). NY: Freeman.
Casper, D. M., & Card, N. A. (2017). Overt and relational victimization: A meta-analytic review of their overlap and associations with social-psychological adjustment. Child Development, 88(2), 466–483. https://doi.org/10.1111/cdev.12621
CDC. (2022, June 3). Data and statistics on children’s mental health | CDC. Centers for disease control and prevention. https://www.cdc.gov/childrensmentalhealth/data.html
Chaplin, T. M., Gillham, J. E., & Seligman, M. E. P. (2009). Gender, Anxiety, and depressive symptoms: A longitudinal study of early adolescents. Journal of Early Adolescents, 29(2), 307–327. https://doi.org/10.1177/0272431608320125
Cohen, J., Cohen, P., West, S. G., & Aiken, L. S. (2003). Applied multiple regression/correlation analysis for the behavioral sciences (3rd ed.). Lawrence Erlbaum.
Cohen, S., & McKay, G. (1984). Social support, stress and the buffering hypothesis: A theoretical analysis. In Baum, A., Taylor, S. E., & Singer J. E. (Eds.), Handbook of psychology and health (pp. 253–267). Hillsdale, NJ: Erlbaum.
Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310. https://doi.org/10.1037/0033-2909.98.2.310
Crick, N. R., & Bigbee, M. A. (1998). Relational and overt forms of peer victimization: A multi- informant approach. Journal of Clinical and Consulting Psychology, 66, 337.
Crick, N. R., Casas, J. F., & Ku, H. C. (1999). Relational and physical forms of peer victimization in preschool. Developmental Psychology, 33, 579–588.
Crick, N. R., & Grotpeter, J. K. (1996). Children’s treatment by peers: Victims of relational and overt aggression. Developmental Psychopathology, 8(2), 367–380. https://doi.org/10.1017/S0954579400007148
Del Rey, R., Casas, J. A., Ortega-Ruiz, R., Schultze-Krumbholz, A., Scheithauer, H., Smith, P., Thompson, F., Barkoukis, V., Tsorbatzoudis, H., Brighi, A., Guarini, A., Pyżalski, J., & Plichta, P. (2015). Structural validation and cross-cultural robustness of the European Cyberbullying Intervention Project Questionnaire. Computers in Human Behavior, 50, 141–147. https://doi.org/10.1016/j.chb.2015.03.065
Dempsey, A. G., Sulkowski, M. L., Nichols, R., & Storch, E. A. (2009). Differences between peer victimization in cyber and physical settings and associated psychosocial adjustment in early adolescence. Psychology in the Schools, 46(10), 962–972. https://doi.org/10.1002/pits.20437
DeWall, C. N., Deckman, T., Pond, R. S., & Bonser, I. (2011). Belongingness as a core personality trait: How social exclusion influences social functioning and personality expression. Journal of Personality, 79(6), 979–1314. https://doi.org/10.1111/j.1467-6494.2010.00695.x
Dill, E. J., Vernberg, E. M., Fonagy, P., Twemlow, S. W., & Gamm, B. K. (2004). Negative Affect in victimized children: The roles of social withdrawal, peer rejection, and attitudes toward bullying. Journal of Abnormal Child Psychology, 32(2), 159–173. https://doi.org/10.1023/B:JACP.0000019768.31348.81
Drazdowski, T. K., Kliewer, W. L., Farrell, A., Sullivan, T., Roberson-Nay, R., & Jäggi, L. (2019). A longitudinal study of the bidirectional relations between anxiety symptoms and peer victimization in urban adolescents. Journal of Interpersonal Violence, 36, 13–14. https://doi.org/10.1177/0886260518824647
Fite, P. J., Cooley, J. L., Diaz, K., Singh, M., & Zax, A. (2023). Impact of sibling victimization on child internalizing symptoms. Child Psychiatry and Human Development, 54, 750–757. https://doi.org/10.1007/s10578-021-01287-3
Forbes, M. K., Fitzpatrick, S., Magson, N. R., & Rapee, R. M. (2019). Depression, anxiety, and peer victimization: Bidirectional relationships and associated outcomes transitioning from childhood to adolescence. Journal of Youth and Adolescence, 48(4), 692–702. https://doi.org/10.1007/s10964-018-0922-6
Foster, H., & Brooks-Gunn, J. (2013). Neighborhood, family and individual influences on school physical victimization. Journal of Youth and Adolescence, 42(10), 1596–1610. https://doi.org/10.1007/s10964-012-9890-4
George, D., & Mallery, M. (2010). SPSS for Windows Step by Step: A Simple Guide and Reference (10a ed.). Pearson.
Georgiades, K., Boyle, M. H., & Fife, K. A. (2013). Emotional and behavioral problems among adolescent students: The role of immigrant, racial/ethnic congruence and belongingness in schools. Journal of Youth and Adolescence, 42(9), 1473–1492. https://doi.org/10.1007/s10964-012-9868-2
Grigg, D. W. (2010). Cyber-aggression: Definition and concept of cyberbullying. Journal of Psychologists and Counselors in School, 20, 143–156. https://doi.org/10.1375/ajgc.20.2.143
Grills, A. E., & Ollendick, T. H. (2002). Peer victimization, global self-worth, and anxiety in middle school children. Journal of Clinical Child and Adolescent Psychology, 31(1), 59–68. https://doi.org/10.1207/S15374424JCCP3101_08
Hair, J., Black, W. C., Babin, B. J., & Anderson, R. E. (2010). Multivariate data analysis (7th ed.). Pearson Educational International.
Hawker, D. S., & Boulton, M. J. (2000). Twenty years’ research on peer victimization and psychosocial maladjustment: A meta-analytic review of cross-sectional studies. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 41(4), 441–455.
Huang, Y., Gan, X., Jin, X., Wei, Z., Cao, Y., & Ke, H. (2023). The healthy context paradox of bullying victimization and academic adjustment among Chinese adolescents: A moderated mediation model. PLoS ONE, 18(8), e0290452. https://doi.org/10.1371/journal.pone.0290452
Irwin, D. E., Stucky, B., Langer, M. M., Thissen, D., DeWitt, E. M., Lai, J.-S., Varni, J. W., Yeatts, K., & DeWalt, D. A. (2010). An item response analysis of the pediatric PROMIS anxiety and depressive symptoms scales. Quality of Life Research, 19(4), 595–607. https://doi.org/10.1007/s11136-010-9619-3
Jacobson, K. C., & Rowe, D. C. (1999). Genetic and environmental influences on the relationships between family connectedness, school connectedness, and adolescent depressed mood: Sex differences. Developmental Psychology, 35(4), 926–939. https://doi.org/10.1037/0012-1649.35.4.926
King, V., Boyd, L. M., & Pragg, B. (2018). Parent-adolescent closeness, family belonging, and adolescent well-being across family structures. Journal of Family Issues, 39(7), 2007–2036. https://doi.org/10.1177/0192513X17739048
Kowalski, R. M., Giumetti, G. W., Schroeder, A. N., & Lattanner, M. R. (2014). Bullying in the digital age: A critical review and meta-analysis of cyberbullying research among youth. Psychological Bulletin, 140(4), 1073–1137. https://doi.org/10.1037/a0035618
Kumpulainen, K., Räsänen, E., Henttonen, I., Almqvist, F., Kresanov, K., Linna, S. L., Moilanen, I., Piha, J., Puura, K., & Tamminen, T. (1998). Bullying and psychiatric symptoms among elementary school-age children. Child Abuse and Neglect, 22(7), 705–717. https://doi.org/10.1016/s0145-2134(98)00049-0
Landoll, R. R., La Greca, A. M., Lai, B. S., Chan, S. F., & Herge, W. M. (2015). Cyber victimization by peers: Prospective associations with adolescent social anxiety and depression symptoms. Journal of Adolescence, 42, 77–86. https://doi.org/10.1016/j.adolescence.2015.04.002
Leary, M. R., & Cox, C. B. (2008). Belongingness motivation: A mainspring of social action. In J. Y. Shah & W. L. Gardner (Eds.), Handbook of motivation science (pp. 27–40). The Guilford Press.
Lee, R. M., & Robbins, S. B. (1995). Measuring belongingness: The Social Connectedness and the Social Assurance scales. Journal of Counseling Psychology, 42(2), 232–241. https://doi.org/10.1037/0022-0167.42.2.232
Libbey, H. P. (2004). Measuring student relationships to school: Attachment, bonding, connectedness, and engagement. Journal of School Health, 74, 274–283. https://doi.org/10.1111/j.1746-1561.2004.tb08284.x
Liu, Y., Yuan, C., Wang, J., Brown, J. G., Zhou, F., Zhao, X., Shen, M., & Hinds, P. S. (2016). Comparability of the patient-reported outcomes measurement information system Pediatric short form symptom measures across culture: Examination between Chinese and American children with cancer. Quality of Life Research, 25, 2523–2533. https://doi.org/10.1007/s11136-016-1312-8
Lucas-Molina, B., Pérez-Albéniz, A., Solbes-Canales, I., Ortuño-Sierra, J., & Fonseca-Pedrero, E. (2022). Bullying, cyberbullying and mental health: The role of student connectedness as a school protective factor. Psychosocial Intervention., 31(1), 33. https://doi.org/10.5093/pi2022a1
Malaquias, S., Crespo, C., & Francisco, R. (2015). How do Adolescents benefit from family rituals? Links to social connectedness, depression and anxiety. Journal of Child and Family Studies, 24(10), 3009–3017. https://doi.org/10.1007/s10826-014-0104-4
Malone, G. P., Pillow, D. R., & Osman, A. (2012). The general belongingness scale (GBS): Assessing achieved belongingness. Personality and Individual Differences, 52(3), 311–316. https://doi.org/10.1016/j.paid.2011.10.027
McGraw, K., Moore, S., Fuller, A., & Bates, G. (2008). Family, peer and school connectedness in final year secondary school students. Australian Psychologist, 43(1), 27–37. https://doi.org/10.1080/00050060701668637
McLaughlin, K. A., Hilt, L. M., & Nolen-Hoeksema, S. (2007). Racial/Ethnic differences in internalizing and externalizing symptoms in adolescents. Journal of Abnormal Child Psychology, 35(5), 801–816. https://doi.org/10.1007/s10802-007-9128-1
McMahon, S. D., Parnes, A. L., Keys, C. B., & Viola, J. J. (2008). School belonging among low-income urban youth with disabilities: Testing a theoretical model. Psychology in the Schools, 45(5), 387–401. https://doi.org/10.1002/pits.20304
McNeely, C. A., Nonnemaker, J. M., & Blum, R. W. (2002). Promoting school connectedness: Evidence from the national longitudinal study of adolescent health. Journal of School Health, 72(4), 138–46. https://doi.org/10.1111/j.1746-1561.2002.tb06533.x
Molero, M. M., Martos, Á., Barragán, A. B., Pérez-Fuentes, M. C., & Gázquez, J. J. (2022). Anxiety and depression from cybervictimization in adolescents: A metaanalysis and meta-regression study. The European Journal of Psychology Applied to Legal Context, 14(1), 42–50. https://doi.org/10.5093/ejpalc2022a5
Moody, J., & Bearman, P. S. (1998). Shaping school climate: School context, adolescent social networks, and attachment to school. Unpublished manuscript.
National Center for Education Statistics (2024). Enrollment Characteristics [Table]. Common Core of Data. Retrieved from https://nces.ed.gov/ccd/schoolsearch/
Neary, A., & Joseph, S. (1994). Peer victimization and its relationship to self-concept and depression among schoolgirls. Personality and Individual Differences, 16(1), 183–186. https://doi.org/10.1016/0191-8869(94)90122-8
Newman, D. A. (2014). Missing data: Five practical guidelines. Organizational Research Methods, 17, 372–411. https://doi.org/10.1177/1094428114548590
Patchin, J. W., & Hinduja, S. (2006). Bullies move beyond the schoolyard: A preliminary look at cyberbullying. Youth Violence and Juvenile Justice, 4, 148–169. https://doi.org/10.1177/1541204006286288
Paus, T., Keshavan, M., & Giedd, J. N. (2008). Why do many psychiatric disorders emerge during adolescence? Nature Reviews Neuroscience, 9(12), 947–957. https://doi.org/10.1038/nrn2513
Pikulski, P. J., Pella, J. E., Casline, E. P., Hale, A. E., Drake, K., & Ginsburg, G. S. (2020). School connectedness and child anxiety. Journal of Psychologists and Counsellors in Schools, 30(1), 13–24. https://doi.org/10.1017/jgc.2020.3
Polanin, J. R., Espelage, D. L., Grotpeter, J. K., Ingram, K., Michaelson, L., Spinney, E., Valido, A., Sheikh, A. E., Torgal, C., & Robinson, L. (2022). A Systematic Review and Meta-analysis of Interventions to Decrease Cyberbullying Perpetration and Victimization. Prevention Science : Society for Prevention Research, 23(3), 439–454. https://doi.org/10.1007/s11121-021-01259-y
Rejaän, Z., van der Valk, I. E., & Branje, S. (2022). The Role of Sense of Belonging and Family Structure in Adolescent Adjustment. Journal of Research on Adolescence, 32(4), 1354–1368. https://doi.org/10.1111/jora.12694
Roeser, R. W., Eccles, J. S., & Sameroff, A. J. (1998). Academic and emotional functioning in early adolescence: Longitudinal relations, patterns, and prediction by experience in middle school. Development and Psychopathology, 10(2), 321–352. https://doi.org/10.1017/S0954579498001631
Rudolph, K. D., Lambert, S. F., Clark, A. G., & Kurlakowsky, K. D. (2001). Negotiating the transition to middle school: The role of self-regulatory processes. Child Development, 72(3), 929–946. https://doi.org/10.1111/1467-8624.00325
Rudolph, K. D., Troop-Gordon, W., Monti, J. D., & Miernicki, M. E. (2014). Moving against and away from the world: The adolescent legacy of peer victimization. Development and Psychopathology, 26, 721–732. https://doi.org/10.1017/S0954579414000340
Rueger, S. Y., Pyun, Y., Coyle, S., Wimmer, J., & Stone, L. B. (2022). Youth depression and perceived social support from parents: A meta-analysis of gender and stress-related differences. Psychological Bulletin, 148(9–10), 710–740. https://doi.org/10.1037/bul0000378
Sabatelli, R. M., & Anderson, S. A. (1991). Family system dynamics, peer relationships, and adolescents’ psychological adjustment. Family Relations, 40(4), 363–369. https://doi.org/10.2307/584891
Schacter, H. L., & Juvonen, J. (2015). The effects of school-level victimization on self-blame: Evidence for contextualized social cognitions. Developmental Psychology, 51, 841–847. https://doi.org/10.1037/dev0000016
Schuler, M. S., Tucker, J. S., Pedersen, E. R., & D’Amico, E. J. (2019). Relative influence of perceived peer and family substance use on adolescent alcohol, cigarette, and marijuana use across middle and high school. Addictive Behaviors, 88, 99–105. https://doi.org/10.1016/j.addbeh.2018.08.025
Sharp, C., Goodyer, I. M., & Croudace, T. J. (2006). The Short Mood and Feelings Questionnaire (SMFQ): A unidimensional item response theory and categorical data factor analysis of self-report ratings from a community sample of 7-through 11-year-old children. Journal of Abnormal Child Psychology, 34(3), 379–391. https://doi.org/10.1007/s10802-006-9027-x
Shochet, I. M., Dadds, M. R., Ham, D., & Montague, R. (2006). School connectedness is an underemphasized parameter in adolescent mental health: Results of a community prediction study. Journal of Clinical Child & Adolescent Psychology, 35(2), 170–179. https://doi.org/10.1207/s15374424jccp3502_1
Siegel, R. S., La Greca, A. M., & Harrison, H. M. (2009). Peer victimization and social anxiety in adolescents: Prospective and reciprocal relationships. Journal of Youth and Adolescence, 38, 1096–1109. https://doi.org/10.1007/s10964-009-9392-1
Sinclair, K. R., Cole, D. A., Dukewich, T., Felton, J., Weitlauf, A. S., Maxwell, M. A., Tilghman-Osborne, C., & Jacky, A. (2012). Impact of physical and relational peer victimization on depressive cognitions in children and adolescents. Journal of Clinical Child & Adolescent Psychology, 41(5), 570–583. https://doi.org/10.1080/15374416.2012.704841
Slaten, C. D., Rose, C. A., Bonifay, W., & Ferguson, J. K. (2019). The Milwaukee Youth Belongingness Scale (MYBS): Development and validation of the scale utilizing item response theory. School Psychology, 34(3), 296–306. https://doi.org/10.1037/spq0000299
Slee, P. T. (1995). Peer victimization and its relationship to depression among Australian primary school students. Personality and Individual Differences, 18(1), 57–62. https://doi.org/10.1016/0191-8869(94)00114-8
Stillman, T. F., & Baumeister, R. F. (2009). Uncertainty, belongingness, and four needs for meaning. Psychological Inquiry, 20(4), 249–251. https://doi.org/10.1080/10478400903333544
Storch, E. A., & Ledley, D. R. (2005). Peer victimization and psychosocial adjustment in children: Current knowledge and future directions. Clinical Pediatrics, 44(1), 29–38. https://doi.org/10.1177/000992280504400103
Storch, E. A., Masia-Warner, C., Crisp, H., & Klein, R. G. (2005). Peer victimization and social anxiety in adolescence: A prospective study Aggressive Behavior. Official Journal of the International Society for Research on Aggression, 31(5), 437–452. https://doi.org/10.1002/ab.20093
Thabrew, H., Stasiak, K., Bavin, L. M., Frampton, C., & Merry, S. (2018). Validation of the mood and feelings questionnaire (MFQ) and short mood and feelings questionnaire (SMFQ) in New Zealand help-seeking adolescents. International journal of methods in psychiatric research, 27(3), e1610. https://doi.org/10.1002/mpr.1610
Troop-Gordon, W., Rudolph, K. D., Sugimura, N., & Little, T. D. (2015). Peer victimization in middle childhood impedes adaptive responses to stress: A pathway to depressive symptoms. Journal of Clinical Child & Adolescent Psychology, 44(3), 432–445. https://doi.org/10.1080/15374416.2014.891225
Turner, H. A., Finkelhor, D., & Ormrod, R. (2006). The effect of lifetime victimization on the mental health of children and adolescents. Social Science & Medicine, 62(1), 13–27. https://doi.org/10.1016/j.socscimed.2005.05.030
van der Wal, M. F., de Wit, C. A., & Hirasing, R. A. (2003). Psychosocial health among young victims and offenders of direct and indirect bullying. Pediatrics, 111(6 Pt 1), 1312–1317. https://doi.org/10.1542/peds.111.6.1312
Williams, K., Chambers, M., Logan, S., & Robinson, D. (1996). Association of common health symptoms with bullying in primary school children. British Medical Journal, 313(7048), 17–19. https://doi.org/10.1136/bmj.313.7048.17
Wright, M. F., & Wachs, S. (2019). Adolescents’ psychological consequences and cyber victimization: The moderation of school-belongingness and ethnicity. International Journal of Environmental Research and Public Health, 16(14), 2493. https://doi.org/10.3390/ijerph16142493
Yuchang, J., Junyi, L., Junxiu, A., Jing, W., & Mingcheng, H. (2019). The differential victimization associated with depression and anxiety in cross-cultural perspective: A meta-analysis. Trauma, Violence, & Abuse, 20(4), 560–573. https://doi.org/10.1177/1524838017726426
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no financial interests related to this work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Fite, P.J., Hesse, D. & Hichborn, E. Associations Between Belonging and Peer Victimization and Internalizing Symptoms Among Middle School-Age Youth. School Mental Health (2024). https://doi.org/10.1007/s12310-024-09702-5
Accepted:
Published:
DOI: https://doi.org/10.1007/s12310-024-09702-5