
Abstract
This work presents a new mathematical model that investigates the impact of diagnosis and treatment of both latent tuberculosis infections and active cases on the transmission dynamics of the disease in a population. Mathematical analysis reveal that the model undergoes the phenomenon of backward bifurcation where a stable disease-free equilibrium co-exist with a stable endemic (positive) equilibrium when the associated reproduction number is less than unity. It is shown that this phenomenon does not exist in the absence of exogenous re-infection. In the absence of exogenous re-infection, the disease-free solution of the model is shown to be globally asymptotically stable when the associated reproduction number is less than unity. It is further shown that a special case of the model has a unique endemic equilibrium point, which is globally asymptotically stable when the associated reproduction number exceeds unity. Uncertainty and sensitivity analysis is carried out to identify key parameters that have the greatest influence on the transmission dynamics of TB in the population using the reproduction number of the model, incidence of the disease and the total number of infected individuals in the various infective classes as output responses. The analysis shows that the top three parameters of the model that have the most influence on the reproduction number of the model are the transmission rate, the fraction of fast disease progression and the rate of detection of active TB cases, with other key parameters influencing the outcomes of the other output responses. Numerical simulations of the model show that the treatment rates for latent and active TB cases significantly determines the impact of the fraction of new latent TB cases diagnosed (and the fraction of active TB cases that promptly receives treatment) on the burden of the disease in a population. The simulations suggest that, with availability of treatment for both latent and active TB cases, increasing the fraction of latent TB cases that are diagnosed and treated (even with a small fraction of active TB cases promptly receiving treatment) will result in a reduction in the TB burden in the population.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
1 Introduction
Tuberculosis (TB) is a chronic bacterial infectious disease caused by Mycobacterium tuberculosis which pose a major health, social and economic burden globally, especially in low and middle income countries [17]. It is the second deadliest disease due to a single infectious agent only after HIV/AIDS [22, 64]. The surge in HIV-TB co-infection and growing emergence of multidrug-resistant TB (MDR-TB) and extensively drug resistant TB (XDR-TB) strains has further fuelled TB epidemic [62, 64]. TB usually affects the lungs (pulmonary TB) but it can also affect other sites as well (extra-pulmonary TB). Tuberculosis is transmitted by tiny airborne droplets which are expelled into the air when a person with active pulmonary TB coughs or talks [26].
Estimate show that TB has infected one-third of the world’s population with the most infections occurring in Africa and Asia [64]. In 2015, there were an estimated 10.4 million new TB cases (incidence) in worldwide, as well as an estimated 1.4 million TB-induced deaths, and an additional 0.4 million deaths resulting from TB disease among persons living with HIV [64]. Furthermore, over 95% of these deaths occurred in low- and middle-income countries where the cost of diagnosis and treatment is high, and not readily accessible [64].
Diagnosis of latent TB infections (LTBI) and prompt treatment of active cases remains an important component of effective TB control [5, 14, 30, 32, 39]. On the other hand, undetected TB infection and delay in the treatment of active TB cases leads to more severe disease conditions in the infected person which could result in wider disease spread in the community [2, 31, 51, 55, 63]. Such delays also contribute to increased infectivity in the community [5], whereby, the infected individuals unknowingly continue to serve as a reservoir for the pathogen (M. tuberculosis). Hence, this could lead to increased risk of disease transmission in the community. In fact, the effects of diagnosis of LTBI and delay in the treatment of active TB cases on the incidence and prevalence of TB were issues considered by some presenters at the 45th World Conference on Lung Health held in 2014 [25].
Health literacy, i.e., knowledge and education related to tuberculosis, as well as socio-cultural factors such as gender roles and status in the family has been identified as having considerable influence on undetected latent TB infection and delay in the treatment of active cases [31, 33, 65]. TB knowledge includes the ability to identify causes and understand the transmission path of the disease, recognize disease symptoms, and be aware of available treatment regimens such as directly observed treatment short course (DOTS); which is the TB treatment strategy recommended by the World Health Organization (WHO) [9, 20, 27, 44]. On the other hand, ignorance on the part of infected individuals about TB usually leads to postponement in seeking appropriate medical attention, and in some cases such persons will rather adopt alternative approaches, such as seeking traditional healers, before consulting DOTS facility, thereby delaying diagnosis and treatment of TB [36, 58].
A recent study in China identified financial difficulty as well as ignoring early TB symptoms or not understanding the meaning of such symptoms on the part of actively-infected persons as being responsible for delay in seeking appropriate medical attention [31]. Besides, some infected individuals are scared of undergoing TB diagnosis because of fear of having to pay for a prolong TB treatment regimen (6–8 months), which ultimately could increase the possibility of developing multidrug-resistant TB strains [10].
In some developing countries, the distance and additional transportation cost to and from a DOTS facility could also discourage actively-infected persons from seeking appropriate medical attention as soon as possible [7]. In the same vain, the life style and habit of some infected individuals have been identified as being also responsible for undetected latent TB infection and delay in the treatment of active TB cases. For example, a person who smokes cigarette may continue to trivialize early TB symptoms such as cough, thereby delaying prompt diagnosis and treatment of the disease [6].
Stigmatization and discrimination towards individuals infected with TB is another factor that could deter persons from seeking prompt TB diagnosis and treatment since it fosters social exclusion and saddens the infected person and members of their family [44, 47]. And because of the social rejection and stigmatization, some patients would rather postpone seeking appropriate medical attention due to the fear of getting to find out about their positive TB status [13].
Health system delay (HSD) in the diagnosis and treatment of LTBI as well as active TB case is usually connected with an infected patient’s visit to an health care center, but without receiving accurate diagnosis. HSD is often caused by unavailability of up-to-date diagnostic laboratory equipments, not adhering to the diagnostic procedures based on DOTS strategy recommended by the WHO [27], and difficulties in identifying TB symptoms in an infected person especially if such symptoms coexist with other chronic lung diseases and/or severe cough [3, 49, 61]. Infected individuals can also experience diagnostic delays as a result of low clinical suspicion of tuberculosis on the part of health-care practitioners. A possible explanation for such wrong or delayed diagnosis on the part of health-care provider is that pulmonary TB can manifest itself with symptoms that are very similar to other diseases such as community-acquired pneumonia (CAP), which is often treated with antibiotics like fluoroquinolones [60]. It has been shown that FQs also have antimicrobial activity against M. tuberculosis [60]. This results in a seeming improvement in the TB symptoms of the infected individual which may ultimately delay the positive diagnosis of the disease [53].
Several mathematical models have been developed and used to study the transmission dynamics of TB in a population [4, 12, 23, 40, 41, 43, 45, 52]. For example, Okuonghae [40] presented a deterministic TB model with genetic heterogeneity in susceptibility and disease progression. Zhang and Feng [67] formulated and globally analyzed a dynamical model to investigate the spread of TB in a community with isolation and incomplete treatment. Trauera et al. [54] presented a deterministic model to describe TB spread in highly endemic regions in Asia-Pacific regions. The model incorporates features such as partial and temporary vaccine efficacy, likelihood of re-infection during the latent state and after treatment, decreasing risk of acute disease after infection. Mishra and Srivastava [37] proposed a mathematical model to study the transmission of TB in human population for both sensitive and drug-resistant subjects.
The purpose of this article is to formulate and rigorously analyze a new model for the transmission dynamics of TB which provides insights into the effects of diagnosis of latent and active TB infection, as well as delay in the treatment of some active cases, on the disease burden in a population. The paper is organized as follows. In Sect. 2, the treatment model is formulated and its basic properties explored. In Sect. 3, the local asymptotic stability of the disease-free equilibrium of the model is examined. The existence of endemic equilibrium point (EEP) for a special case is investigated in Sect. 4. Backward bifurcation analysis is presented in Sect. 5. The existence and global asymptotic stability of EEP for a special case is shown in Sect. 6. Uncertainty and sensitivity analysis and numerical simulation of the model are presented in Sect. 7. Finally, a discussion of the findings from this work is presented in Sect. 8.
2 Model formulation
The total population at time t, denoted by N(t), is subdivided into eight mutually-disjoint compartments of susceptible (S(t)), new latently-infected \((E_1(t))\), diagnosed latently-infected \((E_2(t))\), undiagnosed latently-infected \((E_3(t))\), undiagnosed actively-infected (I(t)), diagnosed actively-infected with prompt treatment \((J_1(t))\), diagnosed actively-infected with delay in treatment \((J_2(t))\), and treated individuals (T(t)). Let \(\Lambda \) be the recruitment rate of individuals into the susceptible class (S). We assume that \(\mu \) is the per capita natural death rate in all epidemiological classes; hence \(1/\mu \) is the average life span of individuals in the population. Let \(\delta _i, i=1,2,3\) be the TB-induced death rates, with \(\delta _1\) being the rate for undiagnosed actively-infected persons (I), \(\delta _2\) being the rate for diagnosed actively-infected persons with prompt treatment \((J_1)\), and \(\delta _3\) being the rate for diagnosed actively-infected persons with delay treatment \((J_2)\); hence, it is reasonable to assume that \(\delta _1 \ge \delta _3 \ge \delta _2\). Susceptible individuals make contact with actively-infected persons and become infected at the rate \(\lambda \) (called the force of infection), with \(\beta \) being the transmission rate, \(\eta _1\) and \(\eta _2\) are modification parameters that accounts for the reduced likelihood of disease transmission by individuals who are diagnosed with active TB and promptly treated (\(J_1\)) and those who delay in receiving treatment (\(J_2\)), respectively, in comparison to actively-infected individuals who were not diagnosed (I); hence we assume that \(0< \eta _1 \le \eta _2 < 1\) [66].
We assume that \(p ~ (0< p < 1)\) is the fraction of individuals with new infections who develop TB fast per unit of time [48]. Hence a fraction, \((1-p)\), of the newly infected individuals (\(\lambda S\)), and previously effectively treated individuals (\(b_3\lambda T\)) who become re-infected are assumed to slowly progress in their disease condition and are moved to the latent class, \(E_1\), with \(b_3 ~ (b_3 > 1)\) being a modification parameter which accounts for the increased likelihood of infection by the previously treated individuals in comparison to wholly-susceptible individuals [59]. The assumption that \(b_3 > 1\) makes biological sense since Verver et al. [59] showed that the rate of tuberculosis reinfection after successful treatment is higher than the rate of a new TB infection.
New latently-infected individuals \((E_1)\) are either diagnosed or remain undetected, at the rate \(\sigma \), in a given unit of time [1, 5]. Hence \({1}/({\sigma + \mu })\) will be the time spent in the “newly” infected state, which is determined by how often screening is done in order to detect new infections. A fraction, \(n ~ (0< n <1)\), of new latently-infected individuals are diagnosed \((E_2)\) and placed on TB treatment at a rate \(r_0\), while the remaining fraction, \(1 - n\), remain undiagnosed \((E_3)\). Undiagnosed latently-infected persons are individually diagnosed at a rate \(\alpha \). Diagnosed latently-infected and undiagnosed latently-infected individuals are both exogenously re-infected at the rates \(b_1~ (0< b_1 <1)\) and \(b_2~ (0< b_2 <1)\), respectively. Individuals with undiagnosed latent TB infections progress to active TB at a rate k. Individuals with undiagnosed active TB cases (I) are detected at a rate \(\kappa \), with a fraction, \(q ~ (0< q < 1)\), of these detected active cases being promptly treated at a rate \(r_1\), while the remaining fraction, \(1 - q\), experiencing some delay before the commencing treatment at a rate \(r_2\); hence it is makes biological sense to assume that \(r_1 \ge r_2\).
Based on the assumptions above, our formulated TB model is given by the following system of nonlinear ordinary differential equations in (2.1), and a flow diagram of the model is given in Fig. 1. The associated variables and parameters used for the formulation are defined in Table 1, while the values and ranges of the parameters used for carrying out numerical simulation of the treatment model (2.1) are listed in Table 2
where the force of infection \(\lambda \) is given by

Since the model (2.1) monitors human population, it is important that all its state variables and associated parameters are non-negative for all time, t. Hence, the following non-negativity result holds for the state variables in the model (2.1).
Theorem 2.1
Let the initial data for the TB model (2.1) be \(S(0)>0, E_1(0)>0, E_2(0)>0, E_3(0)>0, I(0)>0, J_1(0)>0, J_2(0)>0~\) and \(~T(0)>0~\). Then the solutions \((S(t), E_1(t), E_2(t), E_3(t), I(t), J_1(t), J_2(t), T(t))\) of the model (2.1), with positive initial data, will remain positive for all time \(t>0.\)
Proof
Let \(t_1 = \sup \{t>0 : S(0)>0, E_1(0)>0, E_2(0)>0, E_3(0)>0, I(0)>0, J_1(0)>0, J_2(0)>0, T(0)>0\}.\)
From the first equation of model (2.1), it follows that
which can be rewritten as
Thus,
So that,
Similarly, it can be shown that \(E_1(t)>0, E_2(t)>0, E_3(t)>0, I(t)>0, J_1(t)>0, J_2(t) > 0\) and \(T(t) > 0\) for all time \(t>0.\) Thus, all solutions of the system (2.1) remain positive for all non-negative initial conditions. \(\square \)
Lemma 2.2
The closed set
is positively-invariant and attracts all positive solutions of the treatment model (2.1).
Proof
Adding all the equations of model (2.1) gives
Since \(\frac{dN}{dt} \le \lambda - \mu N,\) it follows that \(\frac{dN}{dt} \le 0\) if \(N(t) \ge \frac{\Lambda }{\mu } \). Hence, a standard comparison theorem [28] can be used to show that \(N(t) \le N(0) e^{-\mu t}+\frac{\Lambda }{\mu }(1-e^{-\mu t}).\) In particular, if \(N(0) \le \frac{\Lambda }{\mu }\), then \(N(t) \le \frac{\Lambda }{\mu }\) for all \(t>0.\) Hence, the domain \(\mathcal {D}\) is positively invariant. Furthermore, if \(N(0)>\frac{\Lambda }{\mu },\) then either the solution enters the domain \(\mathcal {D}\) in finite time or N(t) approaches \(\frac{\Lambda }{\mu }\) asymptotically as \(t \rightarrow \infty .\) Hence, the domain \(\mathcal {D}\) attracts all solutions in \(\mathbb {R}^8_+.\)\(\square \)
Since the domain \(\mathcal {D}\) is positively-invariant, it is enough to investigate the dynamics of the flow generated by the model (2.1) in \(\mathcal {D}\). Hence the model (2.1) is both mathematically and epidemiologically well posed.
3 Local asymptotic stability of disease-free equilibrium
The disease-free equilibrium (DFE) of the model (2.1) is given by
The local asymptotic stability (LAS) of the DFE is shown using the next generation operator method [18, 57]. Following similar procedure as in [57], the computed effective reproduction number associated with the model (2.1) is given by
where \( a_{11}=(\sigma +\mu )\), \(a_{22}=(r_0+\mu )\), \(a_{33}=(\alpha +k+\mu )\), \(a_{44}=(\kappa +\delta _1+\mu )\), \(a_{55}=(r_1+\delta _2+\mu )\), and \(a_{66}=(r_2+\delta _3+\mu )\).
Using Theorem 2 in [57] we have the following result:
Lemma 3.1
The DFE (\(\mathcal {E}_0\)) of the model (2.1), given by (3.1), is locally asymptomatically stable (LAS) if \(\mathcal {R}_T < 1\) and unstable if \(\mathcal {R}_T > 1.\)
The threshold quantity, \(\mathcal {R}_T,\) measures the average number of new TB infections generated by a single actively-infected individual in a wholly susceptible populations where there exist control measures such as treatment. The epidemiological implication of Lemma 3.1 is that TB can be eliminated from the community when the effective reproduction numnber is less than unity (\(\mathcal {R}_T < 1\)) if the initial sizes of the subpopulations of the model (2.1) are in the basin of attraction of the DFE (\(\mathcal {E}_0\)). That is, a small influx of TB-infected persons into the community will not generate a large TB outbreak in the community, and the disease will eventually die out in time.
3.1 Analysis of reproduction number (\(\mathcal {R}_T\))
Using the threshold quantity, \(\mathcal {R}_T,\) in (3.2), we wish to investigate the effect of diagnosis of latently-infected individuals and delay in the treatment of active TB cases on the dynamics of the disease in a population, and thus glean effective control strategies involving parameters that characterize these effects.
It can be seen from (3.2), that
The limit in (3.3) implies that a TB control programme that focuses on correct diagnosis of a large fraction of new latent TB infections (\(n \rightarrow 1\)) at a high rate (\(\sigma \rightarrow \infty \)) can lead to effective TB control provided it results in making the right-hand sides of (3.3) less than unity.
From (3.2), it can also be seen that
The limit in (3.4) implies that a TB programme that combines prompt treatment of a large fraction of detected active TB cases (\(q \rightarrow 1\)) at a high rate (\(\kappa \rightarrow \infty \)) can lead to effective TB control provided it results in making the right-hand sides of (3.4) less than unity.
In the same vein, we can see that
The limit in (3.5) implies that a TB control programme that focuses on correct diagnosis of a large fraction of new latent TB cases (\(n \rightarrow 1\)) and prompt treatment of a large fraction of detected active TB cases (\(q \rightarrow 1\)) can lead to effective TB control provided it results in making the right-hand sides of (3.5) less than unity.
Furthermore, we see that
The result in (3.6) implies that a TB control programme that focuses on high rate of diagnosis of latent TB cases and high rate of detection of active TB cases (\(\kappa \rightarrow \infty \)) can lead to effective TB control provided it results in making the right-hand sides of (3.6) less than unity.
Finally, using (3.2), it can be seen that
The limit in (3.7) implies that a TB control programme that focuses on effective combination of diagnosis of a large fraction of new latent TB infections, detection of a large fraction of active TB cases with prompt treatment, high rate of diagnosis of latent TB infections, and high rate of detection of active TB cases (i.e., \(n \rightarrow 1, q \rightarrow 1, \sigma \rightarrow \infty , \kappa \rightarrow \infty \)) can lead to effective TB control if it results in making the right-hand side of (3.7) less than unity. Hence, control strategies that results in any of the limiting expressions in (3.3) to (3.7) to be less than unity will lead to a reduction in the TB burden in the population.
Further sensitivity analysis on some key parameters associated with diagnosis and treatment of latent TB infections and active TB cases (i.e., \(n, q, \kappa , r_1,\) and \( r_2\)) in the model (2.1) are carried out by computing the partial derivatives of \(\mathcal {R}_T\) with respect to these parameters.
The partial derivative of \(\mathcal {R}_T\) with respect to the fraction of new latent TB infections who got diagnosed (n) yields
Clearly, it follows that \(\frac{\mathcal {R}_T}{\partial n} < 0\) unconditionally. Hence, increasing the fraction of new latent TB who got diagnosed, will have a positive impact in reducing TB burden in a population, regardless of the values of other parameters in the expression for \(\mathcal {R}_T\).
Considering the rate of change of (3.2) with respect the fraction of detected and promptly treated active TB cases (q), we have
It follows from (3.9) that \(\frac{\mathcal {R}_T}{\partial q} < 0\) if
Equation (3.10) implies that the detection (and prompt treatment) of a fraction of active TB cases will have a positive impact in reducing TB burden in the community only if \(\eta _1 < \triangle _1\) (or \(\eta _2 > \triangle _2\)). Such control strategy will fail to reduce TB burden in the community if \(\eta _1 = \triangle _1\) (or \(\eta _2 = \triangle _2\)), and will have a detrimental impact in the community if \(\eta _1 > \triangle _1\) (or \(\eta _2 < \triangle _2\)), since this will lead to an increase in the reproduction number \( \mathcal {R}_T\). This results are summarized below:
Lemma 3.2
The detection (and prompt treatment) of a fraction of actively-infected TB cases will have a positive impact in reducing TB burden in the community only if \(\eta _1 < \triangle _1\) (or \(\eta _2 > \triangle _2\)), no impact if \(\eta _1 = \triangle _1\) (or \(\eta _2 = \triangle _2\)), and a detrimental impact if \(\eta _1 > \triangle _1\) (or \(\eta _2 < \triangle _2\)).
Considering the rate of change of (3.2) with respect to the rate of detection of active TB cases (\(\kappa \)), it follows that
where \(a_{11}, a_{22}, a_{33}, a_{44}, a_{55}\), and \(a_{66}\) are as defined in (3.2). From (3.11) it can be seen that \(\frac{\mathcal {R}_T}{\partial \kappa } < 0\) if
The expression in \(\triangle _{3_1}\) is the product of the fraction of detected active TB cases who receive prompt treatment (q) together with the modification parameter \((\eta _1)\) that accounts for the reduced likelihood of disease transmission by individuals who are diagnosed with active TB and promptly treated (\(J_1\)) in comparison to actively-infected individuals who were not detected (I), and the average time spent in the \(J_1\) class. The expression in \(\triangle _{3_2}\) is the product of the fraction of detected active TB cases with delay in commencing treatment \((1-q)\), the modification parameter \((\eta _2)\) that accounts for the reduced likelihood of disease transmission by individuals who are diagnosed with active TB but delay in commencing treatment (\(J_2\)) in comparison to actively-infected individuals who were not detected (I), and the average time spent in the \(J_2\) class. The expression in (3.12) implies that detection of active TB cases will have a positive impact in reducing TB burden if \(\frac{1}{(\delta _1 + \mu )} > \triangle _3\). Such a strategy will have no effect in reducing TB burden if \(\frac{1}{(\delta _1 + \mu )} = \triangle _3\), and will have a detrimental impact in the community if \(\frac{1}{(\delta _1 + \mu )} < \triangle _3\). This result is summed up in the lemma below:
Lemma 3.3
The detection of active TB cases will have a positive impact in reducing TB burden in the community only if \(\frac{1}{(\delta _1 + \mu )} > \triangle _3\), no impact if \(\frac{1}{(\delta _1 + \mu )}= \triangle _3\) and a negative impact if \(\frac{1}{(\delta _1 + \mu )} < \triangle _3\).
Note that \(\frac{1}{\delta _1 + \mu }\) is the average time spent in the class of undetected active TB cases when there is no diagnosis of active TB in the population. If this time spent is greater than the expression in the right hand side of (3.12), then detection (and diagnosis) of active TB cases will have a positive effect on TB population level control.
If we consider the rate of change of \(\mathcal {R}_T\) with respect to the rate at which active TB cases are promptly treated (\(r_1\)), we have
Obviously, it follows that the partial derivative in (3.13) is unconditionally less than zero, i.e., \(\frac{\mathcal {R}_T}{\partial r_1} < 0\). Hence prompt treatment of active TB cases will go a long way in reducing the TB burden in the population, regardless of the values of other parameters in the expression for \(\mathcal {R}_T\).
Similarly, if we consider the rate of change of \(\mathcal {R}_T\), (3.2) with respect to the rate at which active TB cases with delayed treatment (\(r_2\)), we have
Although the partial derivative in (3.14) is also unconditionally less than zero, i.e., \(\frac{\mathcal {R}_T}{\partial r_2} < 0\) with respect to the treatment of active TB cases with delay in treatment, however delay in treatment of active TB cases should be discouraged since this could lead to increase TB incidence in the population [31, 51, 55]. Hence, treatment of active TB (even if there is a delay) will always have a positive population-level impact on TB control, albeit, at a different rate compared to active cases promptly treated.
To further investigate the impact of diagnosis and treatment of both latent and active cases in TB control [7], contour plots of the reproduction number (\(\mathcal {R}_T\)), as a function of the fraction of new latent TB cases that got diagnosed (n) and the fraction of detected active TB cases that received prompt treatment (q), at different treatment levels, are given in Figs. 2 and 3. The parameter values used in producing the contour plots are the baseline values given in Table 2.
Figure 2 shows that at low treatment level (i.e., \(r_0 = 1.5, r_1 = 2.5, r_2 = 1.5\)), it is not possible to eradicate TB from the population since any control strategy based on such low treatment level cannot bring the reproduction number to a value less than unity.

A 2D contour plot of \(\mathcal {R}_T\) as a function of n and q at low treatment level: \(r_0 = 1.5, r_1 = 2.5, r_2 = 1.5\), and \(\beta = 15.557\)
As depicted in Fig. 3, we observe that at treatment levels that are 10 times the low treatment values above (i.e., \(r_0 = 15, r_1 = 25, r_2 = 15\)), eradicating tuberculosis from the population is achievable. For example, if almost \(100\%\) of latently-infected individuals are diagnosed (and treated) along with about \(60\%\) of active TB cases, then it is possible to eliminate TB from the population. However, this strategy will be very difficult to implement in developing countries since a TB control programme that requires diagnosis of a large percentage of latent TB will not be easy to implement in such countries with limited resources.

A 2D contour plot of \(\mathcal {R}_T\) as a function of n and q at moderate treatment level: \(r_0 = 15, r_1 = 25, r_2 = 15\), and \(\beta = 15.557\)
4 Existence of endemic equilibrium point: special case
The existence of endemic equilibria of the treatment model (2.1) is now investigated for a special case when the disease-induced death rates are assumed to be negligible (i.e., \(\delta _1 = \delta _2 = \delta _3 = 0\)). This can fits setting such as most countries in Western Europe, Canada, the United States, Australia and New Zealand where the average number of TB-induced deaths is less than 1 per 100,000 population [64].
Adding up all equations in the model (2.1), and setting the disease-induced death rates to zero yields the following equation for the rate of change of the total population,
Hence, \(N(t) \rightarrow \frac{\Lambda }{\mu } \) as \(t \rightarrow \infty \). Using the limiting value \(N(t) = \frac{\Lambda }{\mu }\) and substitution \(\delta _1 = \delta _2 = \delta _3 = 0\) in the model (2.1), we have the following system of equations:
where \(~\tilde{\lambda } = \frac{\beta \mu }{\Lambda } (I+\eta _1J_1 + \eta _2J_2 \big ) \) is the force of infection.
Let
denote an EEP of the model (4.2). The equations in (4.2) are solved in terms of the force of infection (\(\tilde{\lambda }^{**}\)), at steady-state, given by
It follows that the associated reproduction number corresponding to the model (4.2), denoted by \(\mathcal {R}_{T1}\), is:
where \( a_{11}=(\sigma +\mu )\), \(a_{22}=(r_0+\mu )\), \(a_{33}=(\alpha + k+\mu )\), \(\tilde{a}_{44}=(\kappa +\mu )\), \(\tilde{a}_{55}=(r_1+\mu )\), and \(\tilde{a}_{66}=(r_2+\mu )\).
Setting the right-hand sides of the equations in (4.2) to zero and solving for the state variables, in terms of the force of infection at steady state, yields:
where
The remaining coefficients \(M_2, \ldots , M_6\) and \(N_1, \ldots , N_5\) are quite large, and have been omitted for convenience sake.
By substituting the expressions for the EEP in (4.5) [and noting (4.6)] into the force of infection at the steady state given in (4.3), it follows (after several algebraic manipulations) that the endemic equilibria of the model (4.2) satisfies the following polynomial (in terms of \( \tilde{\lambda }^{**} \)),
where
The components of the EEP are then obtained by solving for \(\tilde{\lambda }^{**}\) from the polynomial (4.7), and substituting the positive values of \(\tilde{\lambda }^{**}\) into the expressions in (4.5) [noting (4.6)]. Furthermore, it follows from (4.8) that the coefficient \(F_6\), is always positive and \(F_0\) is positive (negative) if \(\mathcal {R}_{T1}\) is less (greater) than unity. The following results can be deduced.
Theorem 4.1
The TB model (4.2) with \(\delta _1 = \delta _2 = \delta _3 = 0\) has:
-
(i)
six or four endemic equilibria if \(F_5< 0, F_4> 0, F_3< 0, F_2 > 0, F_1 < 0\) and \(\mathcal {R}_{T1} < 1\),
-
(ii)
four or two endemic equilibria if \(F_5> 0, F_4< 0, F_3> 0, F_2 < 0, F_1 > 0\) and \(\mathcal {R}_{T1} < 1\),
-
(iii)
two endemic equilibria if \(F_5> 0, F_4> 0, F_3< 0, F_2 < 0, F_1 > 0\) and \(\mathcal {R}_{T1} < 1\),
-
(iv)
no endemic equilibrium otherwise, when \(\mathcal {R}_{T1} < 1\).
Items (i)–(iii) of Theorem 4.1 suggests the possibility of backward bifurcation in the treatment model (4.2) with negligible TB-induced deaths (i.e., \(\delta _1 =\delta _2 = \delta _3 = 0\)) when \(\mathcal {R}_{T1} < 1\). The phenomenon of backward bifurcation is characterised by the co-existence of a stable DFE and a stable EEP when the associated reproduction number of the model is less than unity. The epidemiological implication of backward bifurcation is that the classical requirement of having the the reproduction number less than unity, while necessary, is no longer sufficient for effective TB control. Such control measures will now be dependent on the initial sizes of the sub-population of the model [24].
5 Bifurcation analysis
In this section, we characterize the type of bifurcation exhibited by the models (4.2). We claim the following result:
Theorem 5.1
The model (4.2) with \(\delta _1 = \delta _2 = \delta _3 = 0~\) exhibit backward bifurcation at \(\mathcal {R}_{T1}=1\) whenever a bifurcation coefficient, denoted by a [given by (5.9)], is positive.
Proof
Let
represent an arbitrary endemic equilibrium point of the complete model system in (2.1). The existence of backward bifurcation is investigated using the Center Manifold Theory [11, 12, 19, 57]. Before applying this theory, it is convenient to carry out the following change of variables.
Let \(S = x_1\), \(E_1 = x_2\), \(E_2 = x_3\), \(E_3 = x_4\), \(I = x_5\), \(J_1 = x_6\), \(J_2 = x_7\), and \(T = x_8\), so that the total population \(N = \sum ^8_{i=1} x_i\).
It follows, that the model (2.1) can be re-written as
with
Consider the case with \(\beta = \beta ^*\), a bifurcation parameter. Solving for \(\beta = \beta ^*\) from \(\mathcal {R}_T = 1\) yields
where \( a_{11}= (\sigma +\mu ), a_{22}= (r_0+\mu ), a_{33}= ( \alpha + k + \mu ), \tilde{a}_{44} = (\kappa +\mu ), \tilde{a}_{55} = ( r_1 + \mu )\), and \(\tilde{a}_{66} = ( r_2 + \mu )\).
The Jacobian of the transformed system (5.2), evaluated at the DFE (\(\mathcal {E}_0\)) with \(\beta = \beta ^*\), is given by
The matrix \(J^*\) has a simple zero eigenvalue (a center) and all other eigenvalues having negative real part (thus, the Center Manifold Theory can be applied [11, 12, 19, 57]. Moreover, \(J^*\) has a right eigenvector given by \(\mathbf {w} = (w_1, w_2, \ldots , w_8)^T\), where
Similarly \(J^*\) has a left eigenvector \(\mathbf {v} = (v_1, v_2, \ldots , v_8)\), satisfying \(\mathbf {v.w}=1\), with
It follows from Theorem 4.1 in [12], by computing the the associated non-zero partial derivatives of f(x) (evaluated at the DFE (\(\mathcal {E}_0\)) with \(\beta = \beta ^*\)) that the associated bifurcation coefficients, a and b, are given by
which leads to
and
with
Clearly, \(b > 0\) for all biologically feasible parameters. Hence, the direction of the bifurcation at \(\beta = \beta ^*\) (i.e., \(\mathcal {R}_T = 1\)) depends only on the sign of a. Looking at (5.11), we have that \(Q_{22}\) and \(Q_{22}\) are clearly positive. It can easily be shown that \(Q_{33}\) is also positive.
Hence, we have that the existence of of backward bifurcation occurs if and only if the rates of exogenous reinfection, \(b_1\) and \(b_2\), are large enough such that the positive part of (5.9) dominates the negative part. Thus backward bifurcation occurs if and only if:
\(\square \)
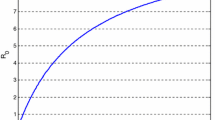
The backward bifurcation exhibited by the model (4.2) is shown in Fig. 4.

Backward bifurcation diagram for the TB model (4.2), showing the force of infection against the effective reproduction number (\(\mathcal {R}_{T1}\))
5.1 Non-existence of backward bifurcation
Consider the special case of the model (4.2) with \(b_1 = b_2 = 0\) (i.e., negligible exogenous re-infection). It can be shown that, in this case, the backward bifurcation coefficient, a, given by (5.9) (and noting that \(\beta ^*>0\) and that all parameters in the model (2.1) are positive) reduces to:
where
and \(w_i, i=1,\ldots ,8\) are given above in Sect. 5.
Hence, it follows from Theorem 4.1 in [12] that the model (4.2), does not undergo a backward bifurcation if \(b_1 = b_2 = 0\) (i.e., in the absence of exogenous re-infection). Hence, this study has confirmed that the presence of exogenous re-infection induces backward bifurcation in the transmission dynamics of TB. This corroborate results from other TB models, that exogenous re-infection can cause the backward bifurcation phenomenon [12, 23, 41, 45].
6 Global asymptotic stability of EEP: special case
Consider the special case of the model (2.1) with \(\alpha = p = b_1 = b_2 = b_3= \delta _1 = \delta _2 = \delta _3 = 0\), given by
where \(\lambda = \frac{\beta (I+\eta _1J_1 + \eta _2J_2 )}{N}\) is the force of infection. It follows that the associated reproduction number corresponding to the model (6.1), denoted by \(\mathcal {R}_{T2}\), is given by
Let
denote an EEP of the model (6.1).
Since \( \delta _1 = \delta _2 = \delta _3 = 0,\) then the total population N(t) in model (6.1) at any time t tends to a limiting value \(\frac{\Lambda }{\mu }\), i.e., \(N(t) \rightarrow \frac{\Lambda }{\mu }\) as \(t \rightarrow \infty \). Let \(\tilde{\beta } = \frac{\mu \beta }{\Lambda }\) so that
is the force of infection for the model (6.1). The system of equations in (6.1) are solved in terms of the force of infection (4.3) to obtain
where \( a_{11}= (\sigma +\mu ) \), \(a_{22}= (r_0+\mu ) \), \(a_{33}= ( k + \mu ) \), \(\tilde{a}_{44}= (\kappa +\mu ) \), \(\tilde{a}_{55}= (r_1 + \mu ) \), \(\tilde{a}_{66}= ( r_2 + \mu ) \), and \(\tilde{\lambda }^{**} = \frac{\tilde{\beta } \big (I^{**} + \eta _1J_1^{**} + \eta _2J_2^{**} \big )}{N}\) is the force of infection at the EEP. Substituting the expressions in (6.5) into the force of infection at the EEP yields a unique value for \(\tilde{\lambda }^{**}\), which is:
Hence, the following result has been established.
Lemma 6.1
The model (6.1), with \(\alpha = p = b_1 = b_2 = b_3= \delta _1 = \delta _2 = \delta _3 = 0\), has a unique EEP, given by \(\mathcal {E}_3\), whenever \(\mathcal {R}_{T2} > 1\).
Furthermore, let [the stable manifold of the DFE of the model (6.1)] be
We claim the following result.
Theorem 6.2
The unique EEP, \(\mathcal {E}_3\), of the reduced model (6.1), with \(\alpha = p = b_1 = b_2 = b_3= \delta _1 = \delta _2 = \delta _3 = 0\), is GAS in \(\mathcal {D} {\setminus } \mathcal {D}_0\) whenever \(\mathcal {R}_{T2} > 1\).
Proof
Consider the model (6.1) with (6.4). Further, let \( \mathcal {R}_{T2} > 1\) (so that the endemic equilibrium \(\mathcal {E}_4\) exists, in line with Lemma 6.1). Consider the following non-linear Lyapunov function
where
and with Lyapunov derivative,
It can be shown from the model (6.1) and (6.4), at steady state, that
Substituting the right hand sides of the first to seventh equations of (6.1) into (6.10), and using (6.11) (after several algebraic calculations) gives
Finally, since the arithmetic mean exceeds the geometric mean, the following inequalities hold:
Thus, \(\mathcal {\dot{Z}} \le 0\) for \(\mathcal {R}_{T2} > 1\). Since the relevant variables in the equations for T are at the endemic steady state, it follows that these can be substituted into the equation for T in (6.1), so that
Hence, \(\mathcal {Z}\) is a Lyapunov function in \(\mathcal {D} {\setminus } \mathcal {D}_0\) [29]. \(\square \)
7 Simulation
In this section, we carry out uncertainty and sensitivity analysis of all the parameters in the treatment model (2.1) using the six infected classes, the reproduction number \((\mathcal {R}_T)\), and TB incidence as response functions. Numerical simulation results of the model (2.1) are also presented.
7.1 Uncertainty and sensitivity analysis
There are 21 parameters in the treatment model (2.1), and uncertainties are expected to arise in estimates of the values used in the numerical simulations. In order to access the effect of these uncertainties and to determine the parameter(s) that have the greatest impact on the transmission dynamics of tuberculosis, we perform uncertainty and sensitivity analysis [8, 34, 35]. Following [8, 39], we perform Latin Hypercube Sampling (LHS) and Partial Rank Correlation Coefficients (PRCC) on the treatment model (2.1). The analysis carried out in this section is based on demographic data relevant to Nigeria [16, 64]. The range and baseline values of the parameters tabulated in Table 2 are used in the analysis.
Using the population of new latently-infected individuals \((E_1)\) as response function, it is shown in Table 3 that the top three PRCC-ranked parameters of the treatment model are: the rate of diagnosis of latent TB \((\sigma )\), fraction of fast TB progression (p), and the rate of detection of active TB \((\kappa )\). Similarly, using the population of diagnosed latently-infected and undiagnosed latently-infected individuals \((E_2\) and \(E_3)\) as response functions, the top three PRCC-ranked parameters are the fraction of fast TB progression (p), rate of detection of active TB \(( \kappa )\) and the treatment rate for diagnosed latently-infected individuals \((r_0)\), and rate of diagnosis of previously undiagnosed latently-infected persons \((\alpha )\), fraction of fast TB progression (p) and fraction of new latent TB infection who got diagnosed (n), respectively. Also, using the population of undiagnosed actively-infected individuals (I) as response function, the top three PRCC-ranked parameters are: the fraction of fast TB progression (p), the rate of detection of active TB \((\kappa )\), and the transmission rate \((\beta )\)). Furthermore, using the population of diagnosed actively-infected with prompt treatment and actively-infected with delay treatment \((J_1\) and \(J_2)\) a response functions, the top three PRCC-ranked parameters are the fraction of fast TB progression (p), the transmission rate \((\beta )\), and the fraction of detected active TB cases with prompt treatment (q). Finally, using the reproduction number \((\mathcal {R}_T)\) as response function, the top three PRCC-ranked parameters are: the fraction of fast TB progression (p), rate of detection of active TB cases \((\kappa )\), and the transmission rate \((\beta )\). In summary, this study identifies nine parameters that have the most significant influence on the transmission dynamics of the treatment model, albeit, depending on the output response of interest, namely: the transmission rate \((\beta )\), fraction of fast TB progression (p), fraction new latent TB who got diagnosed (n), rate of diagnosis of latent TB \((\sigma )\), fraction of detected active TB cases with prompt treatment (q), rate of detection of active TB cases \((\kappa )\), treatment rate for diagnosed latently-infected individuals \((r_0)\), treatment rate for diagnosed actively-infected individuals with delay treatment \((r_2)\), and the rate at which latently-infected individuals become diagnosed individually \((\alpha )\).
The incidence of a disease is the rate of occurrence of new cases of the disease at a given time (or a period of time). In order to investigate significant parameters that greatly influence the occurrence of new cases of tuberculosis (i.e., TB incidence), we use the TB incidence as a response function. It follows from Table 4 that the top three PRCC-ranked parameters are the transmission rate \(( \beta )\), fraction of fast TB progression (p), and rate of detection of active TB cases \(( \kappa )\).
It is worth noting that the fraction of fast TB progression (p) is common to all output responses as one of the significant parameters that has an influence on the transmission dynamics in the population. Hence, an increase in the value of p will result in corresponding increases in the values of the output responses considered herein.
7.2 Numerical simulations
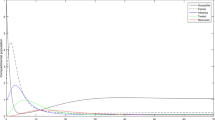
The TB model (2.1) is numerically simulated to illustrate the effect of varying some key parameters related to diagnosis of latent and active TB cases. The parameter values listed in Table 2 are used for the simulations, otherwise specific parameter values (especially the transmission rate, \(\beta \)) used for the simulations are stated in the caption of the each figure. For the simulation in this section, demographic parameters relevant to Nigeria were chosen. Since the total population of Nigeria in 2015 is estimated to be 184,635,279 [16], it follows that, at the disease free equilibrium, \(\Lambda /\mu =184{,}635{,}279\). Moreover, the average mortality rate in Nigeria is \(\mu = 0.02041\) per year [56] so that the average recruitment rate is \(\Lambda = 3{,}768{,}400\) per year, and the total TB incidence in Nigeria was estimated to be 600,000 in 2015 [64].

Cumulative number of new TB cases with \(\beta = 9\), and varied n
Considering Fig. 5, we have the cumulative number of new TB cases as we vary the fraction of new latent TB infection who got diagnosed (n) between 0 and 1. The simulation shows that the cumulative number of new TB cases significantly drops as more latent TB are diagnosed (i.e., as \(n \rightarrow 1\)). This suggest that increasing the fraction of latent TB cases who are diagnosed have a positive effect in reducing the number of new TB cases over time.

Cumulative number of new TB cases with \(\beta = 9,\) and varied q
Looking at Fig. 6, we have the cumulative number of new TB cases as we vary the fraction of detected active TB cases (q) between 0 and 1. The simulation shows that as we increase the fraction of detected active TB cases who are promptly treated, the cumulative incidence of TB reduces.

Cumulative number of new TB cases with \(\beta = 9\), and varied \(\sigma \)
The plot in Fig. 7 shows the cumulative number of new TB cases as we vary the rate of diagnosis of latent TB \((\sigma )\) between 0.2 and 3. The simulation shows that as more latent TB infections are diagnosed, the cumulative number of new TB cases also decreases.

Cumulative number of new TB cases for with \(\beta = 4\), and varied \(\kappa \)
Figure 8 depicts the cumulative number of new TB cases as we vary the rate of detection of active TB cases \((\kappa )\) between 0.2 and 4. Just like the case in Fig. 6, a reduction in the cumulative number of new TB cases can only be achieved with very high detection rate for active cases.
8 Discussion
A new deterministic model for investigating the effect of diagnosis and treatment of latent TB infections and active cases on the transmission dynamics of the disease in a population is formulated and analyzed. We summarize the major theoretical and epidemiological findings as follows:
-
(i)
The model has a disease-free equilibrium (DFE), which is locally asymptotically stable whenever the associated reproduction number is less than unity. In the absence of exogenous re-infection, the treatment model has a globally asymptotically stable DFE whenever the associated reproduction number is less than unity. For a special case, the treatment model is shown to have a unique endemic equilibrium which is shown to be globally-asymptotically stable.
-
(ii)
The model exhibits the backward bifurcation phenomenon when the reproduction number \((\mathcal {R}_{T1})\) is less than unity due to the presence of exogenous re-infection.
-
(iii)
Analysis of the effective reproduction number of the model (2.1) show that the fraction of detected active TB cases that are promptly treated as well as the detection rate for active TB can have a population-level impact on the transmission dynamics of TB under certain conditions. Moreover, the impact of the fraction of new latent TB infections (together with the fraction of active TB cases detected and promptly treated) on the disease burden on the population is largely dependent on the treatment rates for TB infected individuals.
Uncertainty and sensitivity analysis of the treatment model (2.1) show the following:
-
(a)
Using the population of new latently-infected individuals \((E_1)\) as response function, it is shown that the top three PRCC-ranked parameters are the rate of diagnosis of latent TB \((\sigma )\), fraction of fast TB progression (p), and the rate of detection of active TB \((\kappa )\). In the same vein, using the population of diagnosed latently-infected and undiagnosed latently-infected individuals \((E_2\) and \(E_3)\) as response functions, the top three PRCC-ranked parameters are the fraction of fast TB progression (p), rate of detection of active TB \(( \kappa )\) and the treatment rate for diagnosed latently-infected individuals \((r_0)\), and rate of diagnosis of previously undiagnosed latently-infected persons \((\alpha )\), fraction of fast TB progression (p) and fraction of new latent TB infection who got diagnosed (n), respectively.
-
(b)
Furthermore, when the population of undiagnosed actively-infected individuals (I) is used as response function, the top three PRCC-ranked parameters are the fraction of fast TB progression (p), the rate of detection of active TB \((\kappa )\), and the transmission rate \((\beta )\)). Similarly, using the population of diagnosed actively-infected with prompt treatment and actively-infected with delay treatment \((J_1\) and \(J_2)\) a response functions, the top three PRCC-ranked parameters are: the fraction of fast TB progression (p), the transmission rate \((\beta )\), and the fraction of detected active TB cases with prompt treatment (q). It is worth noting that this result also holds when the reproduction number \((\mathcal {R}_T)\) is used as a response function.
-
(c)
When the TB incidence is used as the response function, it is shown that the top three PRCC-ranked parameters that influences the incidence of TB in the population are the transmission rate \(( \beta )\), fraction of fast TB progression (p), and rate of detection of active TB cases \(( \kappa )\).
-
(d)
The common parameter that significantly influences all output responses is the fraction of fast TB progression (p).
Numerical simulations of the TB model (2.1), using relevant demographic data from Nigeria, show that the cumulative number of new cases is significantly reduced as we increase the fraction of diagnosed new latent TB infections (LTBI) (n), and the rate of diagnosis of latent TB \((\sigma )\). Furthermore, the cumulative number of new cases can be reduced when a very large fraction of detected active TB cases are promptly treated (q), and the rate of detection of active TB cases \((\kappa )\) is high.
This study has shown that, with a relatively high fraction of diagnosed (and treated) latent TB infections (even with a small fraction of detected active TB cases promptly receiving treatment), it is possible to reduce the TB burden in the population, in agreement with some of reports, such as [30] and other reference therein. However, the impact of these diagnosis will be positively felt if there are robust treatment policies that will allow for high treatment rates for most TB infections diagnosed.
References
Adewale, S.O., Podder, C.N., Gumel, A.B.: Mathematical analysis of a TB transmission model with DOTS. Can. Appl. Math. Quat. 17(1), 1–36 (2009)
Al-Darraji, H.A.A., Altice, F.L., Kamarulzaman, A.: Undiagnosed pulmonary tuberculosis among prisoners in Malaysia: an overlooked risk for tuberculosis in the community. Tropical Medicine and International Health (2016). https://doi.org/10.1111/tmi.12726
Andrews, J.R., Noubary, F., Walensky, R.P., et al.: Risk of progression to active tuberculosis following reinfection with Mycobacterium tuberculosis. Clin. Infect. Dis. 54(6), 784–791 (2012)
Aparicio, J.P., Castillo-Chavez, C.: Mathematical modelling of tuberculosis epidemics. Math. Biosci. Eng. 6(2), 209–37 (2009)
Asefa, A., Teshome, W.: Total delay in treatment among smear positive pulmonary tuberculosis patients in five primary health centers, southern Ethiopia: a cross sectional study. PLoS ONE 9(7), e102884 (2014). https://doi.org/10.1371/journal.pone.0102884
Bam, T.S., Enarson, D.A., Hinderaker, S.G., et al.: Longer delay in accessing treatment among current smokers with new sputum smear-positive tuberculosis in Nepal. Union: Int. J. Tuberc. Lung Dis. 16(6), 822–827 (2012)
Belay, M., Bjune, G., Ameni, G., et al.: Diagnostic and treatment delay among Tuberculosis patients in Afar Region, Ethiopia: a cross-sectional study. BMC Public Health 12, 369 (2012)
Blower, S.M., Dowlatabadi, H.: Sensitivity and uncertainty analysis of complex models of disease transmission: an HIV model, as an example. Int. Stat. Rev./Rev. Int. Stat. 62(2), 229–243 (1994)
Borgdorff, M.W.: New measurable indicator for tuberculosis case detection. Emerg. Infect. Dis. 10(9), 1523–1528 (2004)
Cain, K.P., Marano, N., Kamene, M., et al.: The movement of multidrug-resistant tuberculosis across borders in East Africa needs a regional and global solution. PLoS Med. (2015). https://doi.org/10.1371/journal.pmed.1001791
Carr, J.: Applications of Center Manifold Theory. Springer, New York (1981)
Castillo-Chavez, C., Song, B.: Dynamical models of tuberculosis and their applications. Math. Biosci. Eng. 1(2), 361–404 (2004)
Cattamanchi, A., Miller, C.R., Tapley, A., et al.: Health worker perspectives on barriers to delivery of routine tuberculosis diagnostic evaluation services in Uganda: a qualitative study to guide clinic-based interventions. BMC Health Serv. Res. 15, 10 (2015)
Centers for Disease Control and Prevention (CDC): Testing for TB infection (2016). http://www.cdc.gov/tb/topic/testing/. Accessed on 23 Sept 2016
Cohen, T., Colijn, C., Finklea, B., et al.: Exogenous re-infection and the dynamics of tuberculosis epidemics: local effects in a network model of transmission. J. R. Soc. Interface 4(14), 523–531 (2007)
Countrymeter Population of Nigeria: Retrieved on 8th December, 2016 from (2015). http://countrymeters.info/en/Nigeria
Delogu, G., Sali, M., Fadda, G.: The biology of mycobacterium tuberculosis infection. Mediterr. J. Hematol. Infect. Dis. (2013). https://doi.org/10.4084/MJHID.2013.070
Diekmann, O., Heesterbeek, J.A.P., Metz, J.A.J.: On the definition and the computation of the basic reproduction ratio \(R_o\) in models for infectious diseases in heterogeneous populations. J. Math. Biol. 28, 365–382 (1990)
Dushoff, J., Huang, W., Castillo-Chavez, C.: Backward bifurcations and catastrophe in simple models of fata diseases. J. Math. Anal. Appl. 36, 227–248 (1998)
Dye, C., Garnett, G.P., Sleeman, K., et al.: Prospects for worldwide tuberculosis control under the WHO DOTS strategy. Directly observed short-course therapy. Lancet 352(9144), 1886–91 (1998)
Esmail, H., Barry, C.E., Young, D.B., et al.: The ongoing challenge of latent tuberculosis. Philos. Trans. R. Soc. B: Biol. Sci. 369(1645), 20130437 (2014). https://doi.org/10.1098/rstb.2013.0437
Fatima, N., Shameem, M., Khan, F., et al.: Tuberculosis: laboratory diagnosis and dots strategy outcome in an urban setting: a retrospective study. J. Tubercul. Res. 2, 106–110 (2014)
Feng, Z., Castillo-Chavez, C., Capurro, A.F.: A model for tuberculosis with exogenous reinfection. Theor. Popul. Biol. 57(3), 235–47 (2000)
Gumel, A.B.: Causes of backward bifurcation in some epidemiological models. J. Math. Anal. Appl. 395(1), 355–365 (2012)
International Union Against Tuberculosis and Lung Disease (The Union): 45th World Union Conference on Lung Health, Barcelona (2014). http://barcelona.worldlunghealth.org/
Issarowa, C.M., Muldera, N., Wood, R.: Modelling the risk of airborne infectious disease using exhaled air. J. Theor. Biol. 372, 100–106 (2015)
Kuznetsov, V.N., Grjibovski, A.M., Mariandyshev, A.O., et al.: Two vicious circles contributing to a diagnostic delay for tuberculosis patients in Arkhangelsk. Emerg. Health Threats J. (2014). https://doi.org/10.3402/ehtj.v7.24909
Lakshmikantham, V., Leela, S., Martynyuk, A.A.: Stability analysis of nonlinear systems. SIAM Rev. 33(1), 152–154 (1991)
LaSalle, J.P., Lefschetz, S.: The Stability of Dynamical Systems. SIAM, Philadelphia (1976)
Lee, S.H.: Diagnosis and treatment of latent tuberculosis infection. Tubercul. Respir. Dis. 78, 56–63 (2015)
Lin, Y., Enarson, D.A., Chiang, C.Y., et al.: Patient delay in the diagnosis and treatment of tuberculosis in China: findings of case detection projects. Union: Public Health Action 5(1), 65–69 (2015)
Lin, S.Y., Hwang, S.C., Yang, Y.C., et al.: Early detection of Mycobacterium tuberculosis complex in BACTEC MGIT cultures using nucleic acid amplification. Eur. J. Clin. Microbiol. Infect. Dis. 35(6), 977–984 (2016)
Makwakwa, L., Sheu, M.I., Chiang, C.Y., et al.: Patient and health system delays in the diagnosis and treatment of new and retreatment pulmonary tuberculosis cases in Malawi. BMC Infect. Dis. 14, 132 (2014)
Marino, S., Hogue, I.B., Ray, C.J., et al.: A methodology for performing global uncertainty and sensitivity analysis in systems biology. J. Theor. Biol. 254(1), 178–96 (2008)
McLeod, R.G., Brewster, J.F., Gumel, A.B., et al.: Sensitivity and uncertainty analyses for a sars model with time-varying inputs and outputs. Math. Biosci. Eng. 3, 527–44 (2006)
Mesfin, M.M., Newell, J.N., Madeley, R.J., et al.: Cost implications of delays to tuberculosis diagnosis among pulmonary tuberculosis patients in Ethiopia. BMC Public Health 10, 173 (2010)
Mishra, B.K., Srivastava, J.: Mathematical model on pulmonary and multidrug-resistant tuberculosis patients with vaccination. J. Egypt. Math. Soc. 22(2), 311–316 (2014)
Moualeua, D.P., Weiserb, M., Ehriga, R., et al.: Optimal control for a tuberculosis model with undetected cases in Cameroon. Commun. Nonlinear Sci. Numer. Simul. 20, 986–1003 (2015)
Okuneye, K., Gumel, A.B.: Analysis of a temperature- and rainfall-dependent model for malaria transmission dynamic. Math. Biosci. (2016). https://doi.org/10.1016/j.mbs.2016.03.013
Okuonghae, D.: A mathematical model of tuberculosis transmission with heterogeneity in disease susceptibility and progression under a treatment regime for infectious cases. Appl. Math. Model. 37(10–11), 6786–6808 (2013)
Okuonghae, D., Aihie, V.: Case detection and direct observation therapy strategy (DOTS) in Nigeria: its effect on TB dynamics. J. Biol. Syst. 16(1), 1–31 (2008)
Okuonghae, D., Aihie, V.: Optimal control measures for tuberculosis mathematical models including immigration and isolation of infective. J. Biol. Syst. 18(1), 17–54 (2010)
Okuonghae, D., Ikhimwin, B.O.: Dynamics of a mathematical model for tuberculosis with variability in susceptibility and disease progressions due to difference in awareness level. Front. Microbiol. 6, 1530 (2016). https://doi.org/10.3389/fmicb.2015.01530
Okuonghae, D., Omosigho, S.: Determinants of TB case detection in Nigeria: a survey. Glob. J. Health Sci. 2(2), 123–128 (2010)
Okuonghae, D., Omosigho, S.: Analysis of a mathematical model for tuberculosis: what could be done to increase case detection. J. Theor. Biol. 269, 31–45 (2011)
Omar, T., Variava, E., Moroe, E., et al.: Undiagnosed TB in adults dying at home fromnatural causes in a high TB burden setting: a post-mortem study. Union: Int. J. Tuberc. Lung Dis. 19(11), 1320–1325 (2015)
Paul, S., Akter, R., Aftab, A., et al.: Knowledge and attitude of key community members towards tuberculosis: mixed method study from BRAC TB control areas in Bangladesh. BMC Public Health 15, 52 (2015)
Pullar, N.D., Steinum, H., Bruun, J.N., et al.: HIV patients with latent tuberculosis living in a low-endemic country do not develop active disease during a 2 year follow-up: a Norwegian prospective multicenter study. BMC Infect. Dis. 14, 667 (2014)
Saifodine, A., Gudo, P.S., Sidat, M., et al.: Patient and health system delay among patients with pulmonary tuberculosis in Beira city, Mozambique. BMC Public Health 13, 559 (2013)
Shea, K.M., Kammerer, J.S., Winston, C.A., et al.: Estimated rate of reactivation of latent tuberculosis infection in the United States, overall and by population subgroup. Am. J. Epidemiol. 179(2), 216–225 (2014)
Shero, K.C., Legesse, M., Medhin, G., et al.: Re-assessing tuberculin skin test (TST) for the diagnosis of tuberculosis (TB) among African migrants in western Europe and USA. J. Tubercul. Res. 4, 4–15 (2014)
Song, B., Castillo-Chavez, C., Aparicio, J.P.: Tuberculosis models with fast and slow dynamics: the role of close and casual contacts. Math. Biosci. 180, 187–205 (2002)
Storla, D.G., Yimer, S., Bjune, G.A.: A systematic review of delay in the diagnosis and treatment of tuberculosis. BMC Public Health 8, 15 (2008)
Trauera, J.M., Denholm, J.T., McBryde, E.S.: Construction of a mathematical model for tuberculosis transmission in highly endemic regions of the Asia-pacific. J. Theor. Biol. 358, 74–84 (2014)
Ukwaja, K.N., Alobu, I., Nweke, C.O., et al.: Healthcare-seeking behavior, treatment delays and its determinants among pulmonary tuberculosis patients in rural Nigeria: a cross-sectional study. BMC Health Serv. Res. 13, 25 (2013)
United Nations Programme on HIV/AIDS (UNAIDS): Communications and global advocacy fact sheet. UNAIDS (2014)
van den Driessche, P., Watmough, J.: Reproduction numbers and sub-threshold endemic equilibria for compartmental models of disease transmission. Math. Biosci. 180, 29–48 (2002)
Verhagen, L.M., Kapinga, R., van Rosmalen-Nooijens, K.A.W.L.: Factors underlying diagnostic delay in tuberculosis patients in a rural area in Tanzania: a qualitative approach. Clin. Epidemiol. Study: Infect. 38, 433–446 (2010)
Verver, S., Warren, R.M., Beyers, N., et al.: Rate of reinfection tuberculosis after successful treatment is higher than rate of new tuberculosis. Am. J. Respir. Crit. Care Med. 171(12), 1430–5 (2005)
Wang, M., FitzGerald, J.M., Richardson, K., et al.: Is the delay in diagnosis of pulmonary tuberculosis related to exposure to fluoroquinolones or any antibiotic? Union: Int. J. Tuberc. Lung Dis. 15(8), 1062–1068 (2011)
Wong, J., Lowenthal, P., Flood, J., et al.: Progression to active tuberculosis among immigrants and refugees with abnormal overseas chest radiographs—California, 1999–2012. Am. J. Respir. Crit. Care Med. 193, A7093 (2016)
World Health Organization (WHO): Global tuberculosis report. WHO report (2013)
World Health Organization (WHO): Guidelines on the management of latent tuberculosis infection (2014)
World Health Organization (WHO): Global tuberculosis report. WHO report (2016)
Yang, W.T., Gounder, C.R., Akande, T., et al.: Barriers and delays in tuberculosis diagnosis and treatment services: does gender matter? Tubercul. Res. Treat. (2014). https://doi.org/10.1155/2014/461935
Yuen, C.M., Amanullah, F., Dharmadhikari, A., et al.: Turning the tap: stopping tuberculosis transmission through active case-finding and prompt elective treatment. Lancet 386(10010), 2334–2343 (2015). https://doi.org/10.1016/S0140-6736(15)00322-0
Zhang, Z., Feng, G.: Global stability for a tuberculosis model with isolation and incomplete treatment. Comput. Appl. Math. (2014). https://doi.org/10.1007/s40314-014-0177-0
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Egonmwan, A.O., Okuonghae, D. Analysis of a mathematical model for tuberculosis with diagnosis. J. Appl. Math. Comput. 59, 129–162 (2019). https://doi.org/10.1007/s12190-018-1172-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12190-018-1172-1