
Abstract
The objective of the systematic review and meta-analysis was to evaluate whether the choice between two radiotracers, 11C-choline (11C-cho) and 18F-fluorocholine (18F-FCH) for PET/CT, and different acquisition protocols contributed to detect metastases for patients with biochemical recurrence of prostate cancer after radical prostatectomy or radiotherapy. We searched in January 2016 in Pubmed and Embase for articles that had used radiolabeled choline PET/CT in restaging. The meta-analysis evaluated technical and clinical aspects. Across 18 articles 1 219 of 2 213 patients (54.9 %) had a positive radiolabeled PET/CT image. Mean of the mean/median restaging PSA levels was 3.6 ± 2.7 ng/mL (range 0.5–10.7 ng/mL). Six articles with 11C-cho PET/CT had a radiation activity of 561 ± 122 MBq and it was 293 ± 47 MBq in 12 articles with 18F-FCH PET/CT. The difference was significant (P = 0.007, t test). Uptake time was 5 min in articles with 11C-cho PET/CT and it was 29 ± 24 min in articles with 18F-FCH PET/CT. The difference was significant (P = 0.02, t test). Thereby the detection rates of metastatic sites in articles with 11C-cho (30 ± 5 %) and 18F-FCH (39 ± 5 %) did not differ significantly (P = 0.26, t test). In linear regression analyses of the articles, the radiation activity of 11C-cho and 18F-FCH was not significantly associated with the detection rate of metastatic sites (P = 0.75 and P = 0.60). Restaging with radiolabeled choline PET/CT detected metastatic sites for patients with biochemical recurrence and PSA levels of 1–10 ng/mL at clinically relevant level. The choice between the two choline radiotracers and different acquisition protocols had no significant impact on detection.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Prostate cancer is the most frequent cancer for old men in Western societies. For men, the mortality with prostate cancer is second to that with lung cancer. Patients with localized disease are mainly treated with radical prostatectomy (RP) and radiotherapy (RT) but up to a third of the patients develop a recurrence. The first clinical phase of recurrence is biochemical recurrence with rising serum PSA levels despite normal findings with conventional imaging. The Society of Nuclear Medicine gave an indication for 18F-fluorodeoxyglucose (18F-FDG) PET/CT to patients with biochemical recurrence if the restaging PSA levels were >10 ng/mL.
For patients with biochemical recurrence, 11C-choline (11C-cho) and 18F-fluorocholine (18F-FCH) PET/CT detected more sites of recurrence than 18F-FDG PET/CT [1]. 11C-cho has a half-life of 20 min and 18F-FCH has a half-life of 110 min. Only 18F-FCH has renal excretion. A review suggested that detection of prostate cancer might increase if the radiation activity of 11C-cho was increased up to 1000 megabequerel (MBq) and the uptake time for 11C-cho was increased up to 10 min [2]. The Food and Drug Administration (FDA) has approved 11C-cho PET/CT for restaging. 18F-FCH is either 18F-fluoromethylcholine or 18F-fluoroethylcholine. As for 18F-FCH PET/CT, some specialists in nuclear medicine prefer to combine an early stationary image of the pelvic region and a late stationary whole body image [3–5]. A European multicenter study with restaging including 18F-FCH PET/CT of 1 000 patients found that patients with restaging PSA levels >2 ng/mL had a high detection rate [6]. Also patients with a high Gleason score >7 and a PSA level <1 ng/mL had a relevant detection rate. 18F-FCH has been approved as a radiopharmaceutical in fifteen countries in the European Union.
Salvage radiotherapy for the prostate bed (SRT) is used for patients with biochemical recurrence after RP. For up to half of the patients with biochemical recurrence, radiolabeled choline PET/CT changed the stage of biochemical recurrence and changed the treatment from SRT. Patients had most delay of a second biochemical recurrence after SRT if it was started while they had restaging PSA levels <0.5 ng/mL.
We aimed with a systematic review and meta-analysis to evaluate whether 11C-cho and 18F-FCH PET/CT had a relevant detection rate of metastatic sites for restaging of patient with PSA levels <10 ng/mL and to evaluate whether the choice between 11C-cho and 18F-FCH as radiotracers for PET/CT and the acquisition protocols might have a significant impact on detection of metastatic sites.
Materials and methods
Search strategy
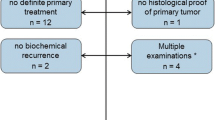
In January 2016, one of the authors (FEvE) undertook a literature search in the bibliographic database Pubmed. The search used Medical Subject Heading terms and text words (“prostatic neoplasms” OR “prostate cancer”) AND (“prostate specific antigen”) AND (“biochemical failure” OR “biochemical recurrence”OR “biochemical relapse” OR “PSA failure” OR “PSA recurrence” OR “PSA relapse”) AND (“positron emission tomography” OR “PET”). The search and a search in Embase gave 200 records. A search for relevant articles in reference lists added 20 records (Fig. 1). We searched for ongoing studies at http://www.ClinicalTrials.gov. The author contacted some principal investigators for complementary information.

Flow diagram for selection of articles
Our search included original full length research articles of biochemical recurrence after RP and RT. Included articles used 11C-cho and 18F-FCH PET/CT as index test to detect sites of recurrence. Of duplicate articles from an institution, we selected the article that reported most patients. Articles published before 2006 were excluded because the International Society of Urologic Pathology had changed the classification of the Gleason score in 2005 [7]. Further, our review excluded articles that undertook radiolabeled choline PET/CT for less than twenty patients and articles that did not allow for 2 × 2 tables on patient basis. Our review also excluded PET/CT articles that combined the initial RP and RT before the biochemical recurrence or combined staging and restaging. The review also excluded some records for administrative reasons.
Data extraction
An author extracted information from the articles to a database. Clinical items were year of publication, name of first author, institution, number of patients, median/mean age of the patients, initial treatment, and median/mean restaging PSA levels. As a finding with the index test, we evaluated the detection rate of a metastatic site. Technical items were type of CT scans, 11C-cho or 18F-FCH radiotracer, radiation activity of the radiotracers, uptake time, field size for PET/CT imaging, acquisition time for each bed position (PET field of view), and criteria for a positive site.
Definitions of items
Biochemical recurrence after RP was defined as a rise from unmeasurable PSA to levels >0.2 ng/mL for patients who had no clinical signs of cancer lesions and negative findings with conventional imaging [8]. Two further PSA measurements showing persisting or rising PSA levels confirmed the rise. Biochemical recurrence after initial RT was defined as a rise of PSA to levels >2.0 ng/mL above the nadir PSA level after RT [9]. Some articles reported the radiation activity of the radiotracer as MBq per kg body weight. For these articles, our meta-analysis evaluated the radiation activity calculated for a patient with a body weight of 80 kg. Uptake time was defined as the time interval from intravenous injection of the radiotracer to start of the imaging. For articles reporting a range of uptake times, our meta-analysis evaluated the longest uptake time. Torso field was defined as a field from base of the skull/top of the neck to the bottom of the pelvis/mid-thigh. The review evaluated the threshold used for diagnosing a site of recurrence. Our review calculated the rate of metastatic sites detected with radiolabeled choline PET/CT as the ratio of patients with a metastatic site detected with PET/CT in relation to the total number of examined patients.
Reference standard for diagnosis of a prostate cancer sites in the articles was positive if a biopsy of the site was positive (mainly loco-regional sites) or if a treatment of the site reduced PSA levels at least 50 % for at least 1 month. Reference standard was negative if a targeted biopsy was negative or if treatment of the site did not reduce PSA levels.
Assessment of quality and strength of evidence
The study quality of articles was assessed by the revised system of Quality Assessment of Diagnostic Accuracy Studies, QUADAS-2, as shown in Table 1 [10, 11]. Studies were interpreted as in a systematic review by Wu et al. [12]. Our evaluations were categorized in three groups. Our meta-analysis assessed evidence and strength of a recommendation for management of the sites of recurrence by the system of Grading of Recommendations, Assessment, Development, and Evaluation (GRADE).
Statistical analysis
A variable was mainly given as the mean ± standard deviation. Our systematic review used parametric statistics. Missing technical information in the reporting of the PET acquisition protocols was not substituted. Our meta-analysis compared groups of articles using t tests. We used linear regression analyses as we evaluated whether radiation activity of the tracer and uptake time was significantly associated with detection rate of metastatic sites. Our meta-analysis used a P value of <0.05 to indicate statistical significance. We used Stata 14.0 as statistical software (StataCorp, College station, TX, USA).
Results
Characteristics of articles
Records with non-choline tracers and duplicate reports were excluded from the 220 records in our search, as shown in Fig. 1. All articles reported cohort studies. We found no randomized trial that compared the diagnostic accuracy with 11C-cho and 18F-FCH PET/CT. Our systematic review included 18 articles with 2219 patients [3, 13–29]. Mean of the median/mean age was 68 ± 4 years. Mean of the median/mean restaging PSA levels was 3.5 ± 2.7 ng/mL (range 0.5–10.7 ng/mL). Table 1 shows how we evaluated the quality in the articles. Our evaluations were summarized in three categories and are shown in Fig. 2.

Evaluation of the quality in 18 articles. Regarding bias: green shows low risk of bias, yellow unclear risk of bias, and red high risk of bias. Regarding applicability: green indicates high applicability, yellow unclear applicability, and red low applicability
Acquisition protocols for radiolabelled choline PET/CT
An acquisition protocols for radiolabeled choline PET/CT was reported in all articles. CT scans were mainly performed with a low dose technique without contrast. The articles used CT scans to localize the PET site and to correct attenuation of the imaging. Radiation activity of the radiotracer was 561 ± 122 MBq in articles with 11C-cho as shown in Table 2, and 293 ± 47 MBq in articles with 18F-FCH as shown in Table 3. The radiation activity with the two radiotracers differed significantly (P = 0.007, t test). Most PET/CT imaging used a torso field.
Uptake time was 5 min in articles with 11C-cho PET/CT as shown in Table 2. In contrast, uptake time varied in articles with 18F-FCH PET/CT as shown in Table 3. Five articles included an early imaging after 1–5 min [19, 23, 25, 26], four articles included only a late imaging after 15–60 min [13, 18, 20, 27], and three articles included an early and a late imaging [3, 21, 29]. Uptake time was 29 ± 24 min in the articles with 18F-FCH PET/CT. The uptake time with the two radiotracers differed significantly (P = 0.02, t test). Acquisition times for each bed position were grossly similar with the two radiotracers.
A site of recurrence was diagnosed with the PET/CT if the site had an increased uptake compared with that of the background or with that of a volume of normal tissue. Fifteen articles reported qualitatively the ratios of uptake and three articles reported the ratios semi-quantitatively using a standardized uptake value.
11C-cho and 18F-FCH PET/CT and detection of metastatic sites
Overall, 1219 patients (54.9 %) had positive sites with radiolabeled choline PET/CT. Six articles reported detection rates with 11C-cho PET/CT as shown in Table 2 and 12 articles reported detection rates with 18F-FCH PET/CT as shown in Table 3. Detection rates of metastatic sites were 30 ± 5 % in articles with 11C-cho and 39 ± 5 % in articles with 18F-FCH. Summarizing the articles, detection rates of metastatic sites did not differ significantly between the two choline radiotracers (P = 0.26, t test). Figure 3 shows the detection rates of metastatic sites with the two radiotracers. In linear regression analysis of articles with 11C-cho PET/CT, radiation activities of the radiotracer was not significantly associated with detection rates of metastatic sites (P = 0.75). Neither did the article with 18F-FCH PET/CT show a significant association (P = 0.60). Linear regression analysis showed no significant association between uptake time for the two choline radiotracers and rate of metastatic sites (P = 0.50).

Detection rates of metastatic sites summarizing six articles with 11C-cho PET/CT (11C-cho) and 12 articles with 18F-FCH PET/CT (18F-FCH). The boxes show the 25, 50, and 75 percentiles, and the whiskers show the full range
Ongoing studies
Table 4 points out ongoing studies with radiolabeled choline PET. Some centers combined PET and MRI [24, 27]. One study compares 11C-cho PET/CT and 11C-cho PET/MRI. Another study compares 11C-cho PET/CT and 18F-FCH PET/CT. Other studies continue to evaluate 18F-FDG PET/CT [30]. Further studies evaluate a promising new radiotracer, 68Ga-prostate specific membrane antigen (PSMA)-HBED-CC, also called 68Ga-PSMA [31].
Discussion
PET/CT in our articles varied regarding the acquisition protocols. The articles gave 11C-cho with a significantly higher radiation activity than 18F-FCH. 18F-FCH PET/CT used a longer uptake time than 11C-Cho PET/CT. Thereby the articles with both radiotracers had a clinically relevant detection rate of metastatic sites at early restaging with median/mean restaging PSA levels of 1–10 ng/mL.
Regarding imaging, recent guidelines for prostate cancer have included radiolabeled choline PET/CT in restaging and it may expand in future. Radiolabeled choline PET/CT was often given with a radiation activity of 370–680 MBq for 11C-cho and a radiation activity of 270–320 MBq for 18F-FCH. Uptake time for 11C-cho PET/CT was 5 min. Massaro et al. [4] analyzed five different acquisition protocols for 18F-FCH PET/CT. The investigators preferred a combination of an early static imaging of the pelvic region and a late static imaging of the whole body. However, only three of 12 articles with 18F-FCH PET/CT (25 %) used the recommended dual-phase imaging. A review regarding staging with radiolabeled choline PET/CT suggested that detection of prostate cancer increased as radiation activity and uptake time for 11C-cho was increased [2]. In contrast, our meta-analysis of restaging with radiolabeled choline PET/CT did not find similar trends for detection of metastatic sites. Whereas FDA approved 11C-cho PET/CT for restaging of prostate cancer, the GRADE system clearly did not give preference of 11C-cho for 18F-FCH.
Further our findings have implications for treatment. Many patients with prostate cancer in the United States of America underwent PET/CT staging and restaging with only 18F-FDG PET/CT [30]. In contrast, our present meta-analysis added to our preference of radiolabeled choline PET/CT over 18F-FDG PET/CT to detect sites of recurrent prostate cancer [1]. All articles in our present meta-analysis undertook radiolabeled choline PET/CT in an early phase of biochemical recurrence with a median/mean restaging PSA level <10 ng/mL. This PSA level was the threshold to trigger restaging with 18F-FDG PET/CT. Hence compared with 18F-FDG PET/CT, radiolabeled choline PET/CT may detect sites of recurrence in an earlier phase of biochemical recurrence. A rationale for restaging with PET/CT is detection of sites outside the prostate bed because SRT is not a relevant treatment for these sites. Therefore, we evaluated the detection rate of metastatic sites by restaging with radiolabeled choline PET/CT. The articles detected metastatic sites for a third of the patients.
Our meta-analysis also has implications for future research. Ongoing studies may evaluate the external validity of our meta-analysis. Consensus may standardize execution and reporting of radiolabeled choline PET/CT. Radiation activity and uptake time of choline radiotracers did not seem to have a significant influence on detection of metastatic sites. Thus centers using 11C-cho PET/CT might be able to collaborate with centers using 18F-FCH PET/CT. Further studies may point to the best radiotracer and acquisition protocol for use of PET/CT in restaging of prostate cancer. 68Ga-PSMA PET/CT may detect sites of recurrence for half of the patients with biochemical recurrence after RP who have restaging PSA levels as low as 0.2–0.5 ng/mL. However, guidelines 2016 recommend that restaging PET/CT only use radiolabeled choline PET/CT.
Overall, our meta-analysis had strength. It showed that the acquisition protocols reflected and exploited the differences in metabolism of the two radiolabeled choline tracers. Our meta-analysis also had limitations. All articles had a median/mean restaging PSA level ≥0.5 ng/mL. The articles often relied on indirect evidence of prostate cancer and abstained from verifying histologically the metastatic sites found with the PET/CT imaging.
Conclusion
Restaging with radiolabelled choline PET/CT detected metastatic sites for patients with restaging PSA levels of 1–10 ng/mL at clinically relevant level. The choice between the two choline radiotracers and different acquisition protocols had no significant impact on detection.
References
von Eyben FE, Kairemo K. Meta-analysis of (11)C-choline and (18)F-choline PET/CT for management of patients with prostate cancer. Nucl Med Commun. 2014;35:221–30.
Chan J, Syndikus I, Mahmood S, Bell L, Vinjamuri S. Is choline PET useful for identifying intraprostatic tumour lesions? A literature review. Nucl Med Commun. 2015;36:871–80.
Simone G, Di Pierro GB, Papalia R, et al. Significant increase in detection of prostate cancer recurrence following radical prostatectomy with an early imaging acquisition protocol with (1)(8)F-fluorocholine positron emission tomography/computed tomography. World J Urol. 2015;33:1511–8.
Massaro A, Ferretti A, Secchiero C, et al. Optimising (18)F-choline PET/CT acquisition protocol in prostate cancer patients. N Am J Med Sci. 2012;4:416–20.
Chondrogiannis S, Marzola MC, Grassetto G, et al. Optimized protocol for (18)F-choline PET/CT in patients with biochemically relapsed prostate cancer: experiences on 250 consecutive cases. Clin Nucl Med. 2015;40:e308–12.
Cimitan M, Evangelista L, Hodolic M, et al. Gleason score at diagnosis predicts the rate of detection of 18F-choline PET/CT performed when biochemical evidence indicates recurrence of prostate cancer: experience with 1,000 patients. J Nucl Med. 2015;56:209–15.
Montironi R, Cheng L, Lopez-Beltran A, et al. Original Gleason system versus 2005 ISUP modified Gleason system: the importance of indicating which system is used in the patient’s pathology and clinical reports. Eur Urol. 2010;58:369–73.
Freedland SJ, Sutter ME, Dorey F, Aronson WJ. Defining the ideal cutpoint for determining PSA recurrence after radical prostatectomy. Prostate-specific antigen. Urology. 2003;61:365–9.
Roach M 3rd, Hanks G, Thames H Jr, et al. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys. 2006;65:965–74.
Whiting PF, Weswood ME, Rutjes AW, Reitsma JB, Bossuyt PN, Kleijnen J. Evaluation of QUADAS, a tool for the quality assessment of diagnostic accuracy studies. BMC Med Res Methodol. 2006;6:9.
Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155:529–36.
Wu LM, Xu JR, Gu HY, et al. Usefulness of diffusion-weighted magnetic resonance imaging in the diagnosis of prostate cancer. Acad Radiol. 2012;19:1215–24.
Pelosi E, Arena V, Skanjeti A, et al. Role of whole-body 18F-choline PET/CT in disease detection in patients with biochemical relapse after radical treatment for prostate cancer. Radiol Med. 2008;113:895–904.
Rinnab L, Simon J, Hautmann RE, et al. [(11)C]Choline PET/CT in prostate cancer patients with biochemical recurrence after radical prostatectomy. World J Urol. 2009;27:619–25.
Breeuwsma AJ, Pruim J, van den Bergh AC, et al. Detection of local, regional, and distant recurrence in patients with PSA relapse after external-beam radiotherapy using (11)C-choline positron emission tomography. Int J Radiat Oncol Biol Phys. 2010;77:160–4.
Giovacchini G, Picchio M, Coradeschi E, et al. Predictive factors of [(11)C]choline PET/CT in patients with biochemical failure after radical prostatectomy. Eur J Nucl Med Mol Imaging. 2010;37:301–9.
Souvatzoglou M, Weirich G, Schwarzenboeck S, et al. The sensitivity of [11C]choline PET/CT to localize prostate cancer depends on the tumor configuration. Clin Cancer Res. 2011;17:3751–9.
Graute V, Jansen N, Ubleis C, et al. Relationship between PSA kinetics and [18F]fluorocholine PET/CT detection rates of recurrence in patients with prostate cancer after total prostatectomy. Eur J Nucl Med Mol Imaging. 2012;39:271–82.
Henninger B, Vesco P, Putzer D, et al. [18F]choline positron emission tomography in prostate cancer patients with biochemical recurrence after radical prostatectomy: influence of antiandrogen therapy—a preliminary study. Nucl Med Commun. 2012;33:889–94.
Schillaci O, Calabria F, Tavolozza M, et al. Influence of PSA, PSA velocity and PSA doubling time on contrast-enhanced 18F-choline PET/CT detection rate in patients with rising PSA after radical prostatectomy. Eur J Nucl Med Mol Imaging. 2012;39:589–96.
Marzola MC, Chondrogiannis S, Ferretti A, et al. Role of 18F-choline PET/CT in biochemically relapsed prostate cancer after radical prostatectomy: correlation with trigger PSA, PSA velocity, PSA doubling time, and metastatic distribution. Clin Nucl Med. 2013;38:e26–32.
Castellucci P, Ceci F, Graziani T, et al. Early biochemical relapse after radical prostatectomy: which prostate cancer patients may benefit from a restaging 11C-Choline PET/CT scan before salvage radiation therapy? J Nucl Med. 2014;55:1424–9.
D’Angelillo RM, Sciuto R, Ramella S, et al. (1)(8)F-Choline positron emission tomography/computed tomography-driven high-dose salvage radiation therapy in patients with biochemical progression after radical prostatectomy: feasibility study in 60 patients. Int J Radiat Oncol Biol Phys. 2014;90:296–302.
Kitajima K, Murphy RC, Nathan MA, et al. Detection of recurrent prostate cancer after radical prostatectomy: comparison of 11C-choline PET/CT with pelvic multiparametric MR imaging with endorectal coil. J Nucl Med. 2014;55:223–32.
Lepinoy A, Cochet A, Cueff A, et al. Pattern of occult nodal relapse diagnosed with (18)F-fluoro-choline PET/CT in prostate cancer patients with biochemical failure after prostate-only radiotherapy. Radiother Oncol. 2014;111:120–5.
Piccardo A, Paparo F, Picazzo R, et al. Value of fused 18F-Choline-PET/MRI to evaluate prostate cancer relapse in patients showing biochemical recurrence after EBRT: preliminary results. Biomed Res Int. 2014;2014:103718.
Di Biagio D, Chiaravalloti A, Tavolozza M, Abbatiello P, Schillaci O. Detection of local recurrence of prostate cancer after radical prostatectomy: is there a role for early (18)F-FCH PET/CT? Ann Nucl Med. 2015;29:861–9.
Kjolhede H, Ahlgren G, Almquist H, et al. (18)F-Choline PET/CT for early detection of metastases in biochemical recurrence following radical prostatectomy. World J Urol. 2015;33:1749–52.
Quero L, Vercellino L, de Kerviler E, et al. 18F-Choline PET/CT and prostate MRI for staging patients with biochemical relapse after irradiation for prostate cancer. Clin Nucl Med. 2015;40:e492–5.
Hillner BE, Siegel BA, Hanna L, et al. Impact of 18F-FDG PET used after initial treatment of cancer: comparison of the National Oncologic PET Registry 2006 and 2009 cohorts. J Nucl Med. 2012;53:831–7.
Afshar-Oromieh A, Zechmann CM, Malcher A, et al. Comparison of PET imaging with a (68)Ga-labelled PSMA ligand and (18)F-choline-based PET/CT for the diagnosis of recurrent prostate cancer. Eur J Nucl Med Mol Imaging. 2014;41:11–20.
Supiot S, Rio E, Pacteau V, Mauboussin MH, Campion L, Pein F. OLIGOPELVIS—GETUG P07: a multicentre phase II trial of combined salvage radiotherapy and hormone therapy in oligometastatic pelvic node relapses of prostate cancer. BMC Cancer. 2015;15:646.
Decaestecker K, De Meerleer G, Ameye F, et al. Surveillance or metastasis-directed therapy for oligometastatic prostate cancer recurrence (STOMP): study protocol for a randomized phase II trial. BMC Cancer. 2014;14:671.
Acknowledgments
No funding was received.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that this manuscript is free of conflict of interest.
Rights and permissions
About this article

Cite this article
von Eyben, F.E., Kairemo, K. Acquisition with 11C-choline and 18F-fluorocholine PET/CT for patients with biochemical recurrence of prostate cancer: a systematic review and meta-analysis. Ann Nucl Med 30, 385–392 (2016). https://doi.org/10.1007/s12149-016-1078-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-016-1078-7