
Abstract
Objective
To evaluate [11C]choline positron emission tomography/computed tomography ([11C]choline PET/CT) for the detection of a biochemical recurrence of prostate cancer after radical prostatectomy.
Methods
Retrospective analysis of [11C]choline PET/CT performed in 41 consecutive prostate cancer patients with a rising PSA. The mean time to biochemical relapse was 24 months. PSA levels were determined at time of examination, and patients received either a targeted biopsy or surgery. Histopathology reports served as reference for the evaluation of the [11C]choline PET/CT findings.
Results
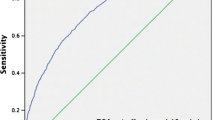
Mean PSA in [11C]choline PET/CT positive patients was 3.1 ng/ml (median 2.2 ng/ml, range 0.5–11.6 ng/ml) and 0.86 ng/ml in [11C]choline PET/CT negative patients (median 0.83 ng/ml, range 0.41–1.40 ng/ml). Six of 12 patients with PSA < 1.5 ng/ml [11C]choline PET/CT revealed a pathological uptake. Histopathology was positive in 6/12 patients in this group. At PSA levels ranging from 1.5 to 2.5 ng/ml all [11C]choline PET/CT were positive (n = 16), a positive histology was found in 12/16 patients (75%) and at PSA 2.5–5 ng/ml [11C]choline PET/CT was positive in 8/8 patients, confirmed by histology in 7/8 patients. Finally, at PSA higher than 5 ng/ml [11C]choline PET/CT identified 5/5 patients positive all confirmed by histology. The sensitivity of [11C]choline PET/CT for the detection of recurrence at PSA < 2.5 ng/ml was 89% with a positive predictive value of 72%.
Conclusion
[11C]choline PET/CT is useful for re-staging of prostate cancer in patients with rising PSA even at levels below 1.5 ng/ml. Our study confirms results from other published studies on [11C]choline PET/CT in prostate cancer relapse.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
A major clinical problem and thereby also diagnostic challenge is the detection of the site of recurrence indicated by a rising serum value of prostate specific antigen (PSA) after definitive treatment of prostate cancer. This is especially important in patients with PSA levels that do not exceed 20 ng/ml. Several imaging techniques are available (TRUS, CT, MRI, [111In]-capromab pendetide), however, they all have limitations and often fail to produce reliable results [1]. Transrectal ultrasonography (TRUS)-guided biopsies have a limited sensitivity of 25–54%, particularly when the PSA is ≤1.0 ng/ml [2]. Perianastomotic biopsies are questionable, since a positive result does not exclude metastatic disease and a negative result does not rule out local recurrence [3]. Contrast enhanced CT is not sufficiently sensitive in detecting local recurrence unless PSA velocity is >20 ng/ml per year [4]. Due to the intrinsic resolution of bone scintigraphy (small lesions are missed) it rarely demonstrates skeletal metastases below a PSA of approximately 30 ng/ml [3, 4]. Encouraging results were reported for endorectal MRI and MRI spectroscopy in small retrospective series [5], promising new sequences could further increase the accuracy of MRI [6]. Despite these imaging modalities, the PSA velocity or the PSA doubling time seem to be the best clinical parameters to distinguish local recurrence from distant metastasis so far [7].
There have been up to now several studies evaluating the value of [11C]choline PET and PET/CT in prostate cancer patients with relapsing PSA [4, 8–13]. Only a few were able to correlate the imaging results with the definitive histopathology, however, these studies have underlined the positive predictive value of this approach [12, 13].
The biochemical background for the usefulness of labeled choline in cancer imaging is the fact that the rate limiting enzyme choline kinase as well as the specific choline transporter are up regulated to support the necessities of the increased cell proliferation and the concomitant membrane forming with major components being various phospholipids [14]. In one of the first larger population studied with [11C]choline PET it was concluded that [11C]choline PET is not able to visualize prostate cancer in restaging below a PSA level of 4.5 ng/ml [9]. Recently, Heinisch et al. [15] reported about a [18F]fluorocholine- ET/CT phase III study for restaging of prostate cancer in a group of 34 patients (radical prostatectomy n = 31, external beam radiation n = 3) and they recommended this technique at PSA values <5 ng/ml. In this study the results of [18F]fluorocholine were compared with other imaging methods (CT and/or MRI), and only in a few cases local tumor progression was proven by biopsy and histology as well as the course of disease. They found in seven of eight [18F]fluorocholine PET/CT cases with PSA < 5 ng/ml malignancy. Other recent studies using integrated [11C]choline PET/CT demonstrated acceptable detection rates of local relapse and distant metastases in prostate cancer patients also for PSA levels lower than 5 ng/ml [11–13]. However, the patient populations were rather heterogenic (i.e. different primary therapies) and also the current treatment at time of the [11C]choline PET/CT (some patients with androgen deprivation therapy mixed with medication naïve patients) was variable [10]. Furthermore most of the studies did not use histopathology (i.e. targeted biopsies or salvage surgery) as golden standard. In recent reviews on detecting recurrent prostate cancer this technique has been described as a promising tool [4, 16]. Also other tracers for the detection of prostate cancer have been presented, among which [11C]acetate taken up due to the increased lipid synthesis (key enzyme acetyl-CoA) has been studied the most, a direct comparison showed similar results with respect to [11C]choline [17].
In this study a homogenous single center collective of patients with comparable initial therapeutic management was studied. Additionally, we were able to relate our findings with histopathological results in all patients, giving us the possibility to make a substantiated statement about the value of this approach even in patients with very low (<1 ng/ml) PSA levels.
Materials and methods
Patients
Retrospectively, a total of 41 consecutive patients without evidence of distant lymph node or bone metastasis with a mean age of 64.9 years (median age of 66 years, range 52–76) with prostate cancer and rising PSA referred for whole [11C]choline PET/CT for clinical restaging after radical prostatectomy (RPE) were evaluated. Nine patients had received adjuvant external beam radiation after RPE. The retrospective evaluation of data was done after a positive vote of the local ethics committee that did not require a specific personal signature of the patients themselves. The indication for [11C]choline PET/CT was a suspicion of local relapse or distant metastases due to rising PSA. Patients with biochemical evidence of disease after radical prostatectomy were identified by a postoperative serum PSA ≥ 0.2 ng/ml. Patients with biochemical evidence of disease after adjuvant external beam radiation (n = 9) were identified by three consecutive rises of serum PSA after nadir according to the American Society for Therapeutic Radiology and Oncology criteria (ASTRO 1996) [18, 19]. Mean PSA in all patients before primary therapy (i.e. radical prostatectomy) in this study was 25.7 ng/ml (range 3.8–176, median 14.3 ng/ml, Hybritech Assay). In all patients PSA was measured on the day of the [11C]choline PET/CT scan. The mean PSA value was 2.8 ng/ml (median PSA 2.1 ng/ml, range 0.41–11.6). Patients treated with external beam radiotherapy and interstitial brachytherapy before PET/CT or with prostatectomy in the previous 3 months were excluded from the study. PSA bouncing effect was also excluded. Four patients were under hormonal deprivation at the time of examination. Beside the [11C]choline PET/CT and the further histopathological confirmation all patients received also conventional diagnostic imaging procedures and a clinical examination including a digital rectal examination (DRE).
[11C]choline PET/CT
[11C]choline was synthesized according to the loop methylation method [20]. [11C]choline PET/CT was performed after 5–8 h fasting with an integrated PET/CT scanner (GE Discovery LS) following intravenous injection of 1056 ± 143 MBq [11C]choline. PET images with a 3 min acquisition time per bed position (FOV 14.6 cm, 35 planes) were acquired in 2D-mode 5 min post-injection starting from mid-thigh to the base of the skull [21]. Contrast enhanced CT (140 kV, 160 mAs, pitch 1.5) was acquired with 120 ml non-ionic contrast given intravenously as bolus (Ultravist, Schering) immediately before the PET acquisition. PET images were reconstructed with the iterative reconstruction ordered-subset expectation maximum likelihood algorithm (OSEM) of the manufacturer after attenuation correction based on the CT data set PET images were reconstructed using CT attenuation correction (28 subsets, 2 iterations, loop filter with a full-width at half-maximum (FWHM) of 3.91 mm, post filter with an FWHM of 6.5 mm, 128 × 128 image matrix, pixel-size 4.29 mm). Consecutive transverse PET/CT slices of 4.25 mm thickness with an in plane resolution of 4.29 × 4.29 mm were generated.
Image analysis
The visual assessment was done in consent of a radiologist and a nuclear medicine physician blinded to clinical data and results of previous imaging studies. Criteria for diagnosing recurrent PCa was an increased uptake of [11C]choline retrovesically and prerectally that had to be at least twofold higher than [11C]choline uptake in perirectal soft or fat tissue as determined by the standard uptake value (SUV). Any increased uptake in pelvic or paraaortal lymph nodes was determined as a local or distant lymph node metastases irrespective of the size of the lymph nodes. [11C]choline uptake in inguinal, mediastinal or hilar lymph node was defined as unspecific uptake. Bone metastases were suspected in patients with typical sclerotic lesions and or increased focal uptake of [11C]choline.
Transrectal ultrasound (TRUS)
TRUS was done in all patients using a commercially available 3D 7.5-MHz-probe (Combison 530 D, type number ultrasound scanner A 00595, type number of transducer 14843, GENERAL ELECTRIC, Milwaukee, WI, USA). In order to improve the image quality we routinely used pre-procedure cleansing enemas. The procedure was performed by using local analgesia agents and analgetics (Instillagel®: FARCO-PHARMA, Cologne, Germany, Tramal®: GRUENENTHAL GmbH, Aachen, Germany). The ultrasound probe armed with an 18 G biopsy gun (in side firing technique) was placed in the rectum 10–15 cm from the anal verge in a technique which allowed visualisation of the suspected local relapse in PET/CT. In all patients biopsy was successfully taken. At least 3 biopsies were taken in each patient from the visualizised lesion.
Histological examination
Histology was performed on the biopsy specimens and on operation specimens after pelvic, iliac or paraaortal lymphadenectomy (LA, n = 13), TUR-bladder (TUR-B, n = 1) as well as TRUS-guided biopsy (TGB, n = 27). The operation specimens were processed according to standard methods. Primary histological diagnosis was made upon H/E stained sections with additional immunohistochemical staining of PSA and prostate specific acid phosphatase (PSAP) in all cases.
PSA determination
PSA in the serum was determined at the central chemical laboratory of the University of Ulm using a HYBRITECH ASSAY (analytical sensitivity <0.01 ng/ml).
Statistics
To get an overall impression of the diagnostic value of [11C]choline PET/CT its sensitivity, specificity and accuracy including the 95% confidence intervals were calculated based on the entire sample size. Additionally, we examined these characteristics for the different subgroups of patients established by the PSA value at the time of [11C]choline PET/CT.
Results
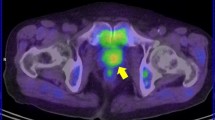
Patients’ characteristics are shown in Table 1 and an overview on the results of PET/CT and histology is shown in a flow chart (Fig. 1). The mean PSA value was 2.8 ng/ml (median PSA 2.1 ng/ml, range 0.41–11.6) at the time of [11C]choline PET/CT. In patients with pathological [11C]choline uptake PSA was 3.1 ng/ml (median PSA 2.2 ng/ml, range 0.5–11.6), in [11C]choline PET/CT negative patients PSA was 0.86 ng/ml (median 0.83 ng/ml, range 0.41–1.40). In 6 of 12 patients (50%) with PSA < 1.5 ng/ml [11C]choline PET/CT showed a pathological uptake, a positive histology was found in 6/12 patients (50%). Three of them were margin positive in the postoperative pathology report (R1 resection). In Fig. 2 a patient (pT3a pN0 cM0 GII Gl.7 R1, adjuvant radiation of the prostate bed) with a histologically confirmed lymph node metastases in a right iliaca externa lymph node is shown (PSA 1.13 ng/ml). In patients with PSA levels ranging from 1.5 to 2.5 ng/ml [11C]choline PET/CT displayed a pathologic pattern in 16/16 patients (100%), a positive histology was found in 12/16 patients (75%) and in patients with PSA 2.5–5 ng/ml [11C]choline PET/CT was pathological in 8/8 patients, the histology at these PSA values was positive in 7/8 patients (88%). Finally, at PSA higher than 5 ng/ml [11C]choline PET/CT identified 5/5 patients with pathological uptake, all lesions were histologically confirmed (100%). The overall sensitivity as well as the positive predictive value (PPV) of [11C]choline PET/CT concerning detection of recurrence was 93% (95% CI 0.78; 0.99) and 80% (0.63; 0.92) with an overall accuracy of 78% (95 CI 0.62; 0.89). The sensitivity at PSA < 2.5 ng/ml—this group included a total of 28 patients—was 89% (95 CI 0.65; 0.99] and the specificity 40% (95 CI 0.12; 0.74], respectively. Table 2 gives detailed information about sensitivity, specificity, positive predictive value and negative predictive value in each PSA subcategory. Five patients showed no pathological [11C]choline uptake, in two of them ultrasound-guided transrectal biopsy (TGB) revealed local recurrence. 6/27 patients which showed a positive uptake in the prostate bed had an unsuspicious transrectal ultrasound (TRUS). In 21 of 27 patients visualization of the lesion by TRUS was possible. Apart from the PET/CT results 26 patients had suspicious TRUS results of which 20 were histological positive. While other 11 patients had a negative TRUS, 8 of them had yet a positive histology report. The mean PSA value of TGB negative patients was 2.8 ng/ml (1.1–2.8), the mean PSA value of TGB positive was 3.1 ng/ml (0.5–3.1).

Flow-chart of patients (n = 41)

a Contrast enhanced 4-row-helical CT scan (tranxaxial slice) of small pelvis after radical prostatectomy (pT3a pN0 cM0 GII Gl. 7 R1, adjuvant radiation of the prostate bed). Thick red arrow shows a lymph node ventral A. iliac externa right, this structure was suspected of a lymph node metastasis. b [11C]choline PET image (tranxaxial slice): focal [11C]choline uptake in a pelvis lymph node without precise localization (thick red arrow). Physiological [11C]choline uptake in urine and rectum (dotted line arrow). c Fused PET/CT image: thick red arrow shows a suspected lymph node ventral A. iliac externa right, dotted line arrow shows physiological [11C]choline uptake in urine and rectum. The salvage lymphadenectomy confirmed histologically lymph node metastases. The subsequent therapy was androgen deprivation
Discussion
In this study we could demonstrate a positive relation between the measured PSA value and the detection rate of [11C]choline PET/CT. Even at levels below 1.5 ng/ml fifty percent of the patients revealed a pathological choline uptake either determined as local recurrence or lymph node metastases, however, the sensitivity is still directly correlated to the PSA level at the time of study. This study adds to the body of evidence that [11C]choline PET/CT is a valuable diagnostic tool in the setting of relapsing PSA and confirms results from other published studies in this field. The important point being here that in all patients a histological evaluation of the tumor relapse was available. In another study of our group we have focused only on patients with suspected local relapse that were candidates for local salvage radiotherapy [11]. In this study the standard uptake value of the local relapse seen on [11C]choline PET/CT in approximately 73% of the patients performed inferior with respect to visual analysis. Also in this study in most patients a histological confirmation was sought [11]. We focused in the current analysis on the visual assessment and could demonstrate comparable descriptive statistics like in the earlier study [11]. In the current retrospective study we included also patients with lymph node metastases and were able to underline the high positive predictive value of [11C]choline PET/CT in occult relapse.
Beside the mentioned study [11] several studies or case-series on [11C]choline PET and PET/CT for restaging prostate cancer have been published. Yoshida et al. [22] reported on eight patients using [11C] choline PET for restaging of prostate cancer after radical prostatectomy (n = 5) and radiotherapy (n = 3). The mean PSA value was 5.3 ng/ml (range 2.3–11). Positive results were found in 75% of the patients. Other imaging techniques (such us ultrasound and MRI) were used as reference. In one of the first studies employing [11C]choline PET [9] no pathological choline uptake was found in the re-staging of patients with PSA levels <5 ng/ml. Picchio et al. [8] compared [11C]choline PET and FDG PET for restaging of prostate cancer in a group of 100 patients. Only in few cases a histological confirmation was obtained, the reference methods were beside PSA follow up, conventional imaging studies at the time of PET imaging and 1 year later. They report about pathological [11C]choline uptake in 3 patients even at PSA levels of 1.2 ng/ml, however, without providing patient specific data. In the current study in 50% of the patients with a PSA < 1.5 ng/ml [11C]choline PET/CT revealed a pathological uptake. A positive histology at this PSA range was seen in 6/12 patients (50%). In 6 patients either a positive histology or a positive PET/CT was lacking, despite elevated PSA and therefore otherwise not detectable prostate cancer relapse has to be assumed. Expanding the group to all patients with PSA values <2.5 ng/ml, the sensitivity of [11C]choline PET/CT and the positive predictive value were high (89 and 72%, respectively ), whereas the specificity and the negative predictive value were relatively low with 40 and 67%, respectively. Similar values were obtained for the total sample size. Thus [11C]choline PET/CT seems to be good in detecting a clinically recurrence, but fails to identify several occult recurrences. This explains why the overall accuracy is only 78%.
In the studies stating that [11C]choline PET is not reasonable at PSA values below 5 ng/ml no integrated PET/CT systems were used [8, 9, 22]. On the one hand this had a higher potential to increase the rate of false-positive results due to the lack of anatomical information and on the other hand small lesions can easily be missed. Recent studies have used also integrated PET/CT cameras, that allow an improved sensitivity and specificity since focal uptake of choline can be more easily assigned to anatomical structures [10–12]. Our data for PSA values below 1 ng/ml are comparable with the results of Krause and coworkers that showed a detection rate of 36% in this group of patients [10]. In another study of our group on a different patient collective with variable initial treatments we experienced also comparable detection rates at the low-PSA levels [12]. A further study concentrated on patients with suspected local relapse after prostatectomy and could demonstrate that focal [11C]choline uptake in the prostate bed is a reliable predictor of an otherwise occult local relapse [11]. We found no correlation between the five negative [11C]choline PET/CT’s and the Gleason-score, the mean PSA before PET/CT examination was 0.86 ng/ml (median 0.83 ng/ml, range 0.41–1.4). Two of the five negative [11C]choline PET/CT results had a positive histology after targeted surgery/biopsy. The reason for false negative cases is most likely due to the small size of the metastases On the other hand one might speculate that a possible intrinsic blockage of choline uptake either by food intake (competitive uptake inhibition or saturation with choline) or hormonal interference with the expression of the choline transporter and the rate limiting enzyme choline kinase could be an explanation, however, scientific evidence is up to now scarce.
Since the results of the [11C]choline PET/CT were included in the further oncological management only a comparison with a historical collective would enable us to disentangle the direct impact of this imaging method on the outcome of patients. Furthermore given the fact that this is a retrospective evaluation this cannot be discussed as real results and certainly is asking for a prospective trial comparing conventional diagnostic approaches with new techniques, possibly including new MRI sequences, MRI spectroscopy and contrast agents, e.g. [23]. Such an approach would give the option to perform a comparison to other imaging techniques and would certainly give an idea on the survival benefit for the patients based on improved diagnostic approaches and possibly earlier detection of the recurrent tumor.
The limitation of the presented study is the small sample size and thereby the relative low statistical power. A further methodological issue is the lack of a control group without signs of recurrence to evaluate the false-positive rate more thoroughly. Since choline PET/CT is not performed in other tumor entities or in non-malignant indications studying a control group is ethically difficult to argue (high-radiation exposure).
The results of our study showed that local recurrence or distant metastasis could be detected by [11C]choline PET/CT with an overall sensitivity of 93% and a PPV of 80%. Our study is in accordance to former reports [8–12, 11, 22]. [11C]choline PET/CT proves to be a valid and useful method for detection of recurrent prostate cancer.
Conclusion
[11C]choline PET/CT has a high sensitivity for the detection of local recurrence or distant metastases in prostate cancer and should be even recommended at PSA < 1.5 ng/ml. Once validated, this approach will have direct impact on clinical decision making, i.e. local versus systemic therapy.
References
Wilkinson S, Chodak G (2004) The role of 111indium-capromab pendetide imaging for assessing biochemical failure after radical prostatectomy. J Urol 172(1):133–136. doi:10.1097/01.ju.0000132138.02846.08
Scattoni V, Roscigno M, Raber M, Montorsi F, Da Pozzo L, Guazzoni G et al (2003) Multiple vesico-urethral biopsies following radical prostatectomy: the predictive roles of TRUS, DRE, PSA and the pathological stage. Eur Urol 44(4):407–414. doi:10.1016/S0302-2838(03)00320-8
Bott SR (2004) Management of recurrent disease after radical prostatectomy. Prostate Cancer Prostatic Dis 7(3):211–216. doi:10.1038/sj.pcan.4500732
Reske SN, Blumstein NM, Glatting G (2006) PET and PET/CT in relapsing prostate carcinoma. Urologe A 45(10):1240–1250. doi:10.1007/s00120-006-1212-6
Sella T, Schwartz LH, Swindle PW, Onyebuchi CN, Scardino PT, Scher HI et al (2004) Suspected local recurrence after radical prostatectomy: endorectal coil MR imaging. Radiology 231(2):379–385. doi:10.1148/radiol.2312030011
Pucar D, Sella T, Schoder H (2008) The role of imaging in the detection of prostate cancer local recurrence after radiation therapy and surgery. Curr Opin Urol 18(1):87–97
Okotie OT, Aronson WJ, Wieder JA, Liao Y, Dorey F, De KJ et al (2004) Predictors of metastatic disease in men with biochemical failure following radical prostatectomy. J Urol 171(6 Pt 1):2260–2264. doi:10.1097/01.ju.0000127734.01845.99
Picchio M, Messa C, Landoni C, Gianolli L, Sironi S, Brioschi M et al (2003) Value of [11C]choline-positron emission tomography for re-staging prostate cancer: a comparison with [18F]fluorodeoxyglucose-positron emission tomography. J Urol 169(4):1337–1340. doi:10.1097/01.ju.0000056901.95996.43
de Jong IJ, Pruim J, Elsinga PH, Vaalburg W, Mensink HJ (2003) 11C-choline positron emission tomography for the evaluation after treatment of localized prostate cancer. Eur Urol 44(1):32–38. doi:10.1016/S0302-2838(03)00207-0 discussion 38–9
Krause BJ, Souvatzoglou M, Tuncel M, Herrmann K, Buck AK, Praus C et al (2008) The detection rate of [(11)C]choline-PET/CT depends on the serum PSA-value in patients with biochemical recurrence of prostate cancer. Eur J Nucl Med Mol Imaging 35(1):18–23. doi:10.1007/s00259-007-0581-4
Reske SN, Blumstein NM, Glatting G (2008) [(11)C]choline PET/CT imaging in occult local relapse of prostate cancer after radical prostatectomy. Eur J Nucl Med Mol Imaging 35(1):9–17. doi:10.1007/s00259-007-0530-2
Rinnab L, Mottaghy FM, Blumstein NM, Reske SN, Hautmann RE, Hohl K et al (2007) Evaluation of [11C]-choline positron-emission/computed tomography in patients with increasing prostate-specific antigen levels after primary treatment for prostate cancer. BJU Int 100(4):786–793. doi:10.1111/j.1464-410X.2007.07083.x
Scattoni V, Picchio M, Suardi N, Messa C, Freschi M, Roscigno M et al (2007) Detection of lymph-node metastases with integrated [11C]choline PET/CT in patients with PSA failure after radical retropubic prostatectomy: results confirmed by open pelvic-retroperitoneal lymphadenectomy. Eur Urol 52(2):423–429. doi:10.1016/j.eururo.2007.03.032
Zeisel SH (1981) Dietary choline: biochemistry, physiology, and pharmacology. Annu Rev Nutr 1:95–121. doi:10.1146/annurev.nu.01.070181.000523
Heinisch M, Dirisamer A, Loidl W, Stoiber F, Gruy B, Haim S et al (2006) Positron emission tomography/computed tomography with F-18-fluorocholine for restaging of prostate cancer patients: meaningful at PSA < 5 ng/ml? Mol Imaging Biol 8(1):43–48. doi:10.1007/s11307-005-0023-2
Machtens S, Serth J, Meyer A, Kleinhorst C, Ommer KJ, Herbst U et al (2007) Positron emission tomography (PET) in the urooncological evaluation of the small pelvis. World J Urol 25(4):341–349. doi:10.1007/s00345-007-0194-3
Kotzerke J, Volkmer BG, Glatting G, van den Hoff J, Gschwend JE, Messer P, Reske SN, Neumaier B (2003) Intraindividual comparison of [11C]acetate and [11C]choline PET for detection of metastases of prostate cancer. Nucl Med (Stuttg) 42(1):25–30
Fichtner J (2006) PSA recurrence following radical prostatectomy and radiotherapy. Urologe A
Roach M 3rd, Hanks G, Thames H Jr, Schellhammer P, Shipley WU, Sokol GH et al (2006) Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys 65(4):965–974. doi:10.1016/j.ijrobp.2006.04.029
Wilson AA, Garcia A, Jin L, Houle S (2000) Radiotracer synthesis from [(11)C]-iodomethane: a remarkably simple captive solvent method. Nucl Med Biol 27(6):529–532. doi:10.1016/S0969-8051(00)00132-3
Farsad M, Schiavina R, Castellucci P, Nanni C, Corti B, Martorana G et al (2005) Detection and localization of prostate cancer: correlation of (11)C-choline PET/CT with histopathologic step-section analysis. J Nucl Med 46(10):1642–1649
Yoshida S, Nakagomi K, Goto S, Futatsubashi M, Torizuka T (2005) 11C-choline positron emission tomography in prostate cancer: primary staging and recurrent site staging. Urol Int 74(3):214–220. doi:10.1159/000083551
Heijmink SW, Scheenen TW, Futterer JJ, Klomp DW, Heesakkers RA, Hulsbergen-van de Kaa CA et al (2007) Prostate and lymph node proton magnetic resonance (MR) spectroscopic imaging with external array coils at 3 T to detect recurrent prostate cancer after radiation therapy. Invest Radiol 42(6):420–427. doi:10.1097/01.rli.0000262759.46364.50
Conflict of interest statement
There is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
L. Rinnab and J. Simon contributed equally to this work.
Rights and permissions
About this article
Cite this article
Rinnab, L., Simon, J., Hautmann, R.E. et al. [11C]choline PET/CT in prostate cancer patients with biochemical recurrence after radical prostatectomy. World J Urol 27, 619–625 (2009). https://doi.org/10.1007/s00345-009-0371-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-009-0371-7