
Abstract
Purpose
To highlight a new imaging acquisition protocol during 18F-fluorocholine PET/CT in patients with biochemical recurrence after RP.
Methods
A total of 146 patients with PSA levels between 0.2 and 1 ng/ml with negative conventional imaging who did not receive salvage treatment were prospectively enrolled. Imaging acquisition protocol included an early dynamic phase (1–8 min), a conventional whole body (10–20 min), and a late phase (30–40 min). Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were measured. Univariable and multivariable analyses were performed to identify independent predictors of positive PET/CT.
Results
The median trigger PSA was 0.6 ng/ml (IQR 0.43–0.76). Median PSA doubling time (PSA DT) was 7.91 months (IQR 4.42–11.3); median PSA velocity (PSAV) was 0.02 ng/ml per month (IQR 0.02–0.04). Overall, 18F-fluorocholine PET/CT was positive in 111 of 146 patients (76 %). Out of 111 positive examinations, 80 (72.1 %) were positive only in the early dynamic phase. Sensitivity, specificity, PPV, NPV, and accuracy were 78.9, 76.9, 97.2, 26.3, and 78.7 %, respectively. At multivariable logistic regression, trigger PSA ≥ 0.6 ng/ml [odds ratio (OR) 3.13; p = 0.001] and PSAV ≥ 0.04 ng/ml per month (OR 4.95; p = 0.004) were independent predictors of positive PET/CT. The low NPV remains the main limitation of PET/CT in this setting of patients.
Conclusions
The increased sensitivity, thanks to the early imaging acquisition protocol, makes 18F-fluorocholine PET/CT an attractive tool to detect prostate cancer recurrences in patients with a PSA level <1 ng/ml.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Radical prostatectomy (RP) is an established treatment option for patients with clinically localised prostate cancer (PCa) [1].
In a large series of 11,521 patients, RP provided durable cancer control with a 15-year cancer-specific survival of 93 % [2]. More recently, Mullins et al. [3] reported long-term oncologic outcomes of a single centre, single surgeon series of RP with a 25-year cancer-specific survival rate of 86 % and confirmed RP as the gold standard in the surgical management of clinically localised PCa. However, despite the standardisation of surgical steps, the incidence of biochemical recurrence after RP ranges from 30 to 50 %, and up to 35 % of patients receive a second-line treatment within the first 10 year [4, 5].
Prostate-specific antigen (PSA) is the most sensitive and commonly used tool for assessing disease recurrence after RP. Biochemical recurrence has been defined as serum PSA values >0.2 ng/ml confirmed by two consecutive measurements [6]. However, PSA levels do not assess the site of recurrence [7], and bone scintigraphy or conventional computed tomography has low sensitivity. Both provide reliable results only with PSA levels >20 ng/ml [6].
Digital rectal examination (DRE), transrectal ultrasound (TRUS), magnetic resonance imaging (MRI), and biopsies of urethrovesical anastomosis or of prostatic fossa have shown limited sensitivity, especially with low PSA values [6, 8, 9]. The European Association of Urology guidelines recommend treating recurrences after RP at PSA levels <0.5 ng/ml to achieve better cancer control [6].
Consequently, the goal of imaging techniques should be the early diagnosis of local recurrences at PSA values <1 ng/ml when recurrence volume is low and the efficacy of salvage radiotherapy (SRT) is greater [6]. Several studies recently reported on the successful use of choline positron emission tomography/computed tomography (PET/CT) that allows a simultaneous assessment of both local and systemic recurrences [9].
However, according to available evidence, its role in patients with PSA values <1 ng/ml remains controversial [9].
The aim of this study was to investigate prospectively the role of 18F-fluorocholine PET/CT in the early restaging (PSA < 1 ng/ml) of patients with biochemical failure after RP who never received any SRT and with a 1-year minimum androgen deprivation treatment (ADT)-free interval at PET/CT.
Methods
From March 2009 to December 2012, 568 patients were referred to 18F-fluorocholine PET/CT for the restaging of disease after RP. The institutional review board approved this prospective study in March 2009. We obtained written informed consent for 18F-fluorocholine PET/CT from all patients.
A total of 146 patients met the inclusion criteria: biochemical failure (defined as two PSA measurements >0.2 ng/ml), PSA levels <1 ng/ml, negative DRE, and conventional imaging, having not received any radiotherapy and having ≥1 year ADT-free interval at the time of the scan.
Data collection
At 18F-fluorocholine PET/CT, collected variables included age, pathologic T and N stages, pathologic Gleason score, trigger PSA, PSA velocity (PSAV), and PSA doubling time (PSA DT). Following PET/CT, collected data included histology findings when available (urethrovesical anastomosis biopsy or histology of removed lymph nodes), PSA levels at 3-month intervals, PSAV, and PSA DT. At the treating physician’s discretion, conventional imaging or PET/CT was performed during follow-up.
PET/CT protocol and imaging acquisition
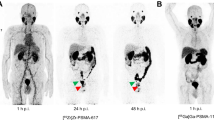
The studies were performed using a high-resolution PET/CT scanner (Biograph Hi-Rez 16; Siemens, Munich, Germany). The acquisition protocol included an early dynamic study of the pelvis starting immediately after the intravenous injection of 4 MBq/kg of 18F-fluoromethyl-dimethyl-2-hydroxyethyl-ammonium (fluorocholine) and a standard whole-body study starting 10–20 min after the injection (3 min on the bed per position). Late images of the pelvis were repeated 30 min following the injection.
The early dynamic phase was an 8-min study of the pelvis with the bladder filled with non-radioactive urine (60 s per frame collected in list mode). Time-activity curves were obtained on the dynamic study by regions of interest on vessels, ureters, bladder, prostate site, and pelvic nodes to discriminate different tracer kinetics. CT data were used for attenuation correction and anatomic localisation. The criteria of PET/CT image interpretation were focal 18F-fluorocholine uptake in the prostatic bed observed on the dynamic study and confirmed by time-increasing kinetics, as shown by the time-activity curve, considered a marker for local recurrence. Focal uptake on pelvic nodes evidenced on the dynamic study and confirmed on the whole body was considered a marker of pelvic node metastasis; any non-physiological uptake on skeleton was considered to be a bone metastasis.
Work-up
TRUS biopsy and salvage lymph-node dissection were performed in the case of urethrovesical or nodal tracer uptake, respectively. Patients with prostate fossa fluorocholine uptake did not undergo biopsy and received SRT. Bone recurrences were confirmed with histology and treated with ADT.
All patients with negative PET/CT findings underwent SRT, except those with a trigger PSA < 0.5 ng/ml and PSAV < 0.1 ng/ml per month.
Interpretation of findings
Positive findings were considered true positives when one of the following criteria was met: (1) positive histology of vesicourethral anastomosis biopsy, (2) positive nodes at salvage lymph-node dissection, (3) disease progression confirmed by increasing PSA values and imaging, and (4) a nadir PSA value <0.1 ng/ml after SRT without ADT. Negative findings were considered false-negatives in all cases but those with PSAV ≤ 0.01 ng/ml per month at 1-year follow-up.
Statistical analysis
A preliminary univariable analysis was performed for each variable to assess the optimal cutoff point by maximising the likelihood ratio. Univariable and multivariable logistic regressions were performed to identify variables independently predictive of positive 18F-choline PET/CT. The odd ratios (ORs) computed by logistic regression, together with their 95 % confidence intervals (CIs), were reported.
All tests were two-sided, and statistical significance was set at p < 0.05. Statistical analysis was performed using SPSS v.19.0 (IBM Corp., Armonk, NY, USA).
Results
Table 1 reports the patient characteristics.
18F-fluorocholine PET/CT was positive in 111 of 146 patients (76 %). A pathologic uptake was observed at the surgical bed site (Fig. 1), at pelvic nodes (Fig. 2), and in the skeleton only (Fig. 3) in 99 patients (89.2 %), 5 patients (4.5 %), and 1 patient (0.9 %), respectively. Multiple-site uptake was observed in five patients at the surgical bed and pelvic nodes (4.5 %) and in one patient (0.9 %) at the pelvic nodes and bone, respectively (Table 2). True positive findings were confirmed in 108/111 patients. Among the 35 negative PET/CT scans, true negativity was confirmed in seven cases.

Axial, sagittal, and coronal views of a pathologic choline uptake suggesting a local recurrence

Axial, sagittal, and coronal views of a pathologic choline uptake at left hypogastric area, suggesting a nodal recurrence

Axial and coronal views of a pathologic choline uptake at left pubic bone suggesting a bone metastasis
Out of 111 positive examinations, 83 (74.8 %) were positive only in the early dynamic phase (Table 3).
Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of PET/CT were 78.9, 76.9, 97.2, 26.3, and 78.7 %, respectively; a phase-specific analysis of findings demonstrated the key role of the early dynamic phase in providing a dramatic increase in diagnostic accuracy (Table 4).
Univariable binomial logistic regression was performed to identify independent predictors of 18F-fluorocholine PET/CT positivity (Table 5) . At multivariable logistic regression, trigger PSA ≥ 0.6 ng/ml and PSAV ≥ 0.04 ng/ml per month were independent predictors of 18F-fluorocholine PET/CT positivity (OR 3.13; 95 % CI, 1.55–6.31; p = 0.001 and OR 4.95; 95 % CI, 1.65–14.83; p = 0.004, respectively) (Table 6).
Once patients were stratified into three groups according to these two variables (PSA ≥ 0.6 ng/ml and PSAV ≥ 0.04 ng/ml per month), in patients with both PSA ≥ 0.6 and PSAV ≥ 0.04, in those with one of these two variables over the cutoff point, and in those with both variables under the cutoff point, the positive detection rates were 93.3, 78.4, and 64.1 %, respectively (Chi square, p = 0.014).
Discussion
Persistently elevated or increasing PSA levels following RP can be due to a local relapse as well as to a metastatic spread to nodes, bone, or viscera. CT scan, MRI, and bone scan are not recommended to follow-up patients after RP at PSA levels <20 ng/ml; TRUS biopsy of vesicourethral anastomosis is only indicated when affecting the treatment plan; measurement of PSA levels remains the cornerstone in the follow-up of patients who underwent RP [6].
In the absence of effective imaging techniques, a rapidly increasing PSA level (high PSAV, short PSA DT) suggests distant metastases, whereas later and slowly increasing PSA levels most likely indicate local recurrence [6]. However, biochemical failure usually precedes clinically evident disease by 6–48 months [10]. Over the years, promising data have been published on the diagnostic efficacy of PET/CT following RP [9, 11, 12]. PET/CT also provides metabolic and anatomic information about recurrences with the advantage of distinguishing among local, regional, or distant relapses to target the treatment accordingly [6].
Several authors have investigated the role of PET/CT with either 11C-choline or 18F-fluorocholine PET/CT in restaging patients with biochemical failure following RP and highlighted a correlation between trigger PSA values and imaging accuracy. As expected, PET/CT sensitivity increased linearly with trigger PSA values, from 19 to 36 % with PSA < 1 ng/ml to 63–83 % when PSA levels are >3 ng/ml [13–17].
In a series of 63 consecutive patients with a mean PSA value of 5.9 ng/ml, Krause et al. reported a 56 % overall 11C-choline PET/CT detection rate. In patients with a PSA < 1 ng/ml, in those with PSA values between 1 and 2 ng/ml, between 2 and 3 ng/ml, and ≥3 ng/ml, the detection rates were 36, 43, 62, and 73 %, respectively [14].
Castellucci et al. [17] investigated the role of 11C-choline PET/CT in 190 patients with PSA relapse (mean 4.2; median 2.1; range 0.2–25.4 ng/ml) following RP. The PET/CT detection rate was 19 % in patients with PSA < 1 ng/ml, 25 % with PSA between 1 and 2 ng/ml, 41 % with PSA between 2 and 5 ng/ml, and 67 % in patients with PSA > 5 ng/ml. Because the trigger PSA value was significantly different (p = 0.0001) between PET-positive (median PSA 4.0 ng/ml) and PET-negative patients (median PSA 1.4 ng/ml), the authors set the optimal trigger PSA cutoff point at 2.43 ng/ml [17].
The low sensitivity rates of PET/CT raised a question about its role in patients with PSA levels <1 ng/ml following RP. As claimed in a 2011 review by Picchio et al. [9], given that the trigger PSA values predictive of PET/CT positivity are significantly higher than 1 ng/ml, no final evidence is available on the role of this imaging modality, so its routine use cannot be commonly recommended in patients with PSA levels <1 ng/ml. However, because the sensitivity of PET/CT increases linearly with a trigger PSA value, including patients with PSA values >5 ng/ml provided a cutoff point significantly higher than 1 ng/ml [17].
In a recent paper [18], the authors compared the diagnostic accuracy of the combined techniques of proton magnetic resonance spectroscopic imaging and dynamic contrast-enhanced MRI on a 3-T magnet with 18F-fluorocholine PET/CT performed in other “undefined” centres in men with biochemical failure following RP. The MRI technique showed 94 % accuracy with 100 % PPV in a subgroup of 56 patients with mean PSA values of 1.9 ng/ml and a biopsy-proven recurrence in 93 % of cases. Despite the interestingly high accuracy of MRI in detecting local recurrences, MRI does not provide a whole-body staging and in this study failed to play a role in patients with PSA levels <1 ng/ml. The key point of this debate is the need for a relatively early treatment of local relapses following RP, which makes PET/CT a less attractive diagnostic tool due to its low sensitivity rate in patients with PSA levels <1 ng/ml.
In another study, including patients with PSA levels <1 ng/ml after RP, although 18F-fluorocholine and 11C-acetate PET/CT studies succeeded in detecting recurrent disease in about 50 % of cases (11 of 20), the authors did not recommend PET/CT as a standard diagnostic tool for early relapse or the suspicion of subclinical minimally persistent disease after surgery [19].
Giovacchini et al. [20] have investigated the role of 11C-choline PET/CT in 75 patients with biochemical recurrence following RP, restricting the cohort of patients to those with PSA levels <1.5 ng/ml who received neither ADT nor SRT. This setting of patients is the one that can really benefit from an early diagnosis and a tailored treatment in the case of positive findings. Patients with evidence of distant metastases and negative local pathologic tracer uptake would also benefit from avoiding unnecessary SRT.
Despite a PET/CT positivity of only 21 %, the authors highlighted that 11C-choline PET/CT may reduce by 50 % the number in whom salvage therapy is initiated empirically without knowing the disease location [20].
As demonstrated by Stephenson et al. in a cohort of 1,603 men with PSA progression after RP treated by SRT, the therapeutic benefit is more evident in the presence of minimal PSA serum levels. The 6-year PSA-free survival was 48 % in men with PSA < 0.5 ng/ml, whereas it was only 40, 28, and 18 % in men with PSA levels of 0.51–1, 1.01–1.5, and >1.5 ng/ml, respectively [21].
However, when recommending SRT in patients with PSA levels <0.5 ng/ml, the EAU guidelines highlight how men with slowly progressing disease, although at risk for progression, may not benefit from SRT because of a low risk for developing fatal PCa [6].
In this context, PET/CT could be a useful tool to select patients who could safely avoid receiving SRT.
In the present series of 146 patients with biochemical failure after RP and PSA values <1 ng/ml, 18F-fluorocholine PET/CT showed a recurrence in 111 of 146 patients (76.0 %), with a sensitivity of 79.4 %.
We first reported such a high sensitivity rate in a setting of patients with low PSA threshold (<1 ng/mL). However, the PET/CT positivity rate (17.8 %) in the conventional “whole-body” acquisition phase was comparable to that reported by Giovacchini et al. [20] (21 %).
If such a difference could be partially explained by physical differences in positron emitter radiotracers (i.e., longer mean range in tissue of 18F-fluorocholine vs. 11C-choline), our findings supported the early dynamic imaging acquisition provided by the PET/CT tomography used (Biograph Hi-Rez 16; Siemens) as the real cornerstone of the increased sensitivity in these “early” recurrences (small lesions with low PSA values).
In fact, the phase-specific findings reported in Table 4 demonstrate the dramatic increase in sensitivity rate provided by the early dynamic acquisition [from 18.4 % (whole-body phase) to 78.2 %].
Conversely, despite a high sensitivity, our findings highlighted a very low NPV of PET/CT (26.3 %) in this setting of patients. We find it reasonable to consider this result as a consequence of “low-volume” disease with low metabolic activity that does not turn in a detectable tracer uptake. However, we believe that our findings shed new light on the role of this imaging technique in a clinical setting where conventional imaging fails to support physicians.
Keeping in mind that the earlier the SRT the better the oncologic outcome, we identified two cutoff points (≥0.6 and ≥0.04 ng/ml per month) for trigger PSA levels and PSAV, respectively, that can be used to maximise PET/CT positivity in patients with PSA < 1 ng/ml from 64.1 % in patients with trigger PSA < 0.6 and PSAV < 0.04 to 93 % in patients with trigger PSA ≥ 0.6 and PSAV ≥ 0.04.
Limitations of this study include the need for larger cohorts and a further prospective validation of findings. The lack of histologic confirmation of positive PET/CT findings, in cases of pathologic uptake at prostatic fossa, should be considered an intrinsic limitation of all imaging techniques currently available in clinical practice. The main drawback of 18F-fluorocholine PET/CT in this setting of patients remains the low NPV.
The high accuracy (78.7 %) of 18F-fluorocholine PET/CT in patients with PSA levels <1 ng/ml supports this imaging technique as a valid option to overcome the definition of “biochemical recurrence,” to detect early recurrences after RP, and to perform imaging-guided salvage treatments. Trigger PSA ≥ 0.6 ng/ml and PSAV ≥ 0.04 ng/ml per month proved to be useful predictive tools of PET/CT-positive findings.
References
Heidenreich A, Bellmunt J, Bolla M et al (2010) EAU guidelines on prostate cancer. Part 1: screening, diagnosis, and treatment of clinically localised disease. Eur Urol 59:61–71
Eggener SE, Scardino PT, Walsh PC et al (2011) Predicting 15-year prostate cancer specific mortality after radical prostatectomy. J Urol 185:869–875
Mullins JK, Feng Z, Trock BJ et al (2012) The impact of anatomical radical retropubic prostatectomy on cancer control: the 30-year anniversary. J Urol 188:2219–2224
Morgan WR, Bergstralh EJ, Zincke H (1993) Long-term evaluation of radical prostatectomy as treatment for clinical stage C (T3) prostate cancer. Urology 41:113–120
Bott SR (2004) Management of recurrent disease after radical prostatectomy. Prostate Cancer Prostatic Dis 7:211–216
Mottet N, Bellmunt J, Bolla M et al (2011) EAU guidelines on prostate cancer. Part II: treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur Urol 59:572–583
Scattoni V, Montorsi F, Picchio M et al (2004) Diagnosis of local recurrence after radical prostatectomy. BJU Int 93:680–688
Scattoni V, Roscigno M, Raber M et al (2003) Multiple vesicourethral biopsies following radical prostatectomy: the predictive roles of TRUS, DRE, PSA and the pathological stage. Eur Urol 44:407–414
Picchio M, Briganti A, Fanti S et al (2011) The role of choline positron emission tomography/computed tomography in the management of patients with prostate-specific antigen progression after radical treatment of prostate cancer. Eur Urol 59:51–60
Lange PH, Ercole CJ, Lightner DJ et al (1989) The value of serum prostate specific antigen determinations before and after radical prostatectomy. J Urol 141:873–879
Picchio M, Crivellaro C, Giovacchini G, Gianolli L, Messa C (2009) PET-CT for treatment planning in prostate cancer. Q J Nucl Med Mol Imaging 53:245–268
Pucar D, Sella T, Schoder H (2008) The role of imaging in the detection of prostate cancer local recurrence after radiation therapy and surgery. Curr Opin Urol 18:87–97
Rinnab L, Mottaghy FM, Simon J et al (2008) [11C]Choline PET/CT for targeted salvage lymph node dissection in patients with biochemical recurrence after primary curative therapy for prostate cancer. Preliminary results of a prospective study. Urol Int 81:191–197
Krause BJ, Souvatzoglou M, Tuncel M et al (2008) The detection rate of [11C]Choline-PET/CT depends on the serum PSA-value in patients with biochemical recurrence of prostate cancer. Eur J Nucl Med Mol Imaging 35:18–23
Husarik DB, Miralbell R, Dubs M et al (2008) Evaluation of [(18)F]-choline PET/CT for staging and restaging of prostate cancer. Eur J Nucl Med Mol Imaging 35:253–263
Pelosi E, Arena V, Skanjeti A et al (2008) Role of whole-body 18F-choline PET/CT in disease detection in patients with biochemical relapse after radical treatment for prostate cancer. Radiol Med 113:895–904
Castellucci P, Fuccio C, Nanni C et al (2009) Influence of trigger PSA and PSA kinetics on 11C-Choline PET/CT detection rate in patients with biochemical relapse after radical prostatectomy. J Nucl Med 50:1394–1400
Panebianco V, Sciarra A, Lisi D et al (2012) Prostate cancer: 1HMRS-DCEMR at 3 T versus [(18)F]choline PET/CT in the detection of local prostate cancer recurrence in men with biochemical progression after radical retropubic prostatectomy (RRP). Eur J Radiol 81:700–708
Vees H, Buchegger F, Albrecht S et al (2007) 18F-choline and/or 11C-acetate positron emission tomography: detection of residual or progressive subclinical disease at very low prostate-specific antigen values (<1 ng/mL) after radical prostatectomy. BJU Int 99:1415–1420
Giovacchini G, Picchio M, Garcia-Parra R et al (2013) [11C]Choline positron emission tomography/computerized tomography for early detection of prostate cancer recurrence in patients with low increasing prostate specific antigen. J Urol 189:105–110
Stephenson AJ, Scardino PT, Kattan MW et al (2007) Predicting outcome of salvage radiation therapy for recurrent prostate cancer after radical prostatectomy. J Clin Oncol 25:2035–2041
Conflict of interest
The authors declare that they have no conflict of interest.
Informed consent
The manuscript was approved by the institutional review board, and all patients gave written informed consent to treatment.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Simone, G., Di Pierro, G.B., Papalia, R. et al. Significant increase in detection of prostate cancer recurrence following radical prostatectomy with an early imaging acquisition protocol with 18F-fluorocholine positron emission tomography/computed tomography. World J Urol 33, 1511–1518 (2015). https://doi.org/10.1007/s00345-015-1481-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-015-1481-z