
Abstract
Purpose
To assess the utility of transluminal attenuation gradient (TAG) in combination with coronary computed tomography angiography (CTA) for detecting obstructive coronary artery stenosis.
Materials and methods
We retrospectively evaluated coronary CTA data in 35 consecutive patients who underwent invasive coronary angiography (ICA). We compared the diagnostic performance of TAG with that of quantitative coronary angiography, which we used as the reference standard. For the combination of TAG and coronary CTA, we designed a logical conjunction model (CCTA&&TAG) as well as a logical disjunction model (CCTA||TAG), and evaluated their diagnostic accuracies.
Results
Among 130 vessels of 35 patients, 30 lesions (23%) showed significant stenosis on ICA. TAG predicted significant coronary artery stenosis with a sensitivity of 75%, specificity of 63%, positive predictive value of 40%, negative predictive value of 89%, and accuracy of 66%, and had a cutoff value of − 15.4 HU/10 mm. The respective values for CCTA&&TAG were 73, 98, 88, 90, and 90%; those for CCTA||TAG were 94, 61, 56, 94, and 72%. CCTA&&TAG improved the diagnostic accuracy significantly more than CCTA||TAG.
Conclusion
TAG in conjunction with coronary CTA improves the diagnostic accuracy of coronary CTA.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Coronary computed tomography angiography (CTA) is a non-invasive alternative to coronary angiography for diagnosing coronary arterial disease. Recent multicenter trials proved the efficacy of coronary CTA as a diagnostic and prognostic tool [1,2,3]. However, coronary CTA has limited predictive ability for identifying borderline morphologically significant stenosis because of its lower spatial resolution compared to invasive coronary angiography (ICA).
To improve the diagnostic accuracy of coronary CTA, some trials have reported the use of a combination of coronary CTA and myocardial perfusion CT [4] or fractional flow reserve assessment by computed tomography (FFR-CT) [5, 6]. Despite of the high diagnostic accuracies brought by these techniques, their processes are very complex or time-consuming.
The transluminal attenuation gradient (TAG), defined as the gradient of intraluminal attenuation, reflects the hemodynamics of the coronary artery and is an index for lesion severity. It is calculated as a numerical value and represents the decrease in contrast attenuation in the lumen at the proximal and distal coronary arteries. Recent studies have described the utility of TAG for assessing the significance of obstructive coronary stenosis [7, 8]. In the present study, we focused on the ability of TAG for improving the diagnostic accuracies of morphologically significant stenosis by coronary CTA in comparison with quantitative coronary angiography (QCA). So far, there is no consensus on how to interpret contradictory TAG and coronary CTA findings. Therefore, the aim of the present study was to evaluate the diagnostic accuracy of TAG compared with that of coronary artery angiography (CAG), and the improvement in diagnostic accuracy when TAG was combined with coronary CTA, especially in cases with discrepant TAG and coronary CTA results. This article describes the patterns of combined coronary CTA and TAG.
Materials and methods
Patients
This retrospective study was approved by our institutional review board. A total of 35 consecutive patients who underwent both coronary CTA and ICA between May and October 2015 were included. Exclusion criteria in our study were as follows: coronary artery occlusion, multiple significant stenoses (> 50% diameter stenosis) in a single coronary artery branch on coronary CTA or ICA, small vessel (lumen cross-sectional area less than 2 mm2), history of percutaneous coronary intervention or bypass grafting, motion artifacts on CT (due to poor breath-holding or severe arrhythmia), heart rate > 65 beats/min (despite β-blocker use), no prospective electrocardiographic gating covering 70–80% of the R–R interval, and coronary artery calcification score > 1500 [9]. We obtained TAG measurements of the left coronary artery (left anterior descending artery and left circumflex artery) and right coronary artery (American Heart Association segment #4PD and #4AV). Among 140 coronary vessels of 35 patients, 10 coronary vessels were excluded (9 were small vessels and 1 had motion artifacts). Thus, the final study population comprised 35 patients (30 men, 5 women; mean age 64 ± 10.8 years; range 41–85 years) and a total of 130 coronary vessels.
CT protocol
A previously described CT scanning protocol was utilized [8]. Patients were scanned using a 320-multidetector row CT scanner (Aquilion ONE VISION Edition; Toshiba Medical Systems, Otawara, Japan). The detailed scanning parameters were as follows: tube voltage, 120 kV; tube current, 100–450 mA (targeting image noise of 28 HU); collimation, 0.5 mm × 320 row; and gantry rotation time, 0.275 s/rotation. Prospective electrocardiographic gating was used, covering 70–80% of the R–R interval [7, 8]. Patients with heart rates > 65 beats/min were intravenously administered 0.125-mg/kg landiolol (Corebeta; Ono Pharmaceutical, Tokyo, Japan). Scan data were acquired during the injection of contrast medium containing 370 mg/ml of iodine (Iopamiron 370; Bayer Japan, Osaka, Japan) or 350 mg/ml of (Omnipaque 350; Daiichi Sankyo Co., Tokyo, Japan) at a rate of 0.07 ml/kg/s for 10 s followed by a 35-ml saline flush. The threshold of bolus tracking was 150 Hounsfield units (HU), with the region of interest set in the ascending aorta. Subsequent to the triggering, image acquisition began automatically at 6 s.
An experienced cardiovascular CT technician determined the optimal stationary cardiac phase from the available scanning data. All axial CT data were reconstructed with the half-scan reconstruction using a kernel of FC44 with the hybrid iterative reconstruction (IR) technique (Adaptive Iterative Dose Reduction 3D enhanced; AIDRe 3D, Toshiba Medical Systems) at a thickness of 0.5 mm with 0.5-mm increments in the axial plane.
ICA
ICA was performed as a diagnostic or pre-procedural imaging technique in conjunction with percutaneous transluminal coronary intervention using the Allura Xper FD20/10 or Allura Xper FD10/10 system (Philips Electronics Japan Ltd., Tokyo, Japan). A 4-Fr or 5-Fr diagnostic catheter (Judkins or Amplatz) was placed via the transfemoral or transbrachial approach. High-concentration contrast medium (iohexol 350 mg/ml) was administered using ACIST (DVx Co, Ltd, Tokyo, Japan). The injection volume and rate of contrast medium was 6.2 ml and 3 ml/s for the left coronary artery, and 5.4 ml and 2.5 ml/s for the right coronary artery, respectively. The extent of stenosis in each major coronary artery was evaluated using QCA (QAngio XA 7.1; Medis Medical Imaging Systems bv, Leiden, the Netherlands). Significant stenosis was defined as ≥ 50% diameter stenosis on QCA.
TAG
TAG was defined as the linear regression coefficient between the intraluminal radiological attenuation (in HU) and the distance from the coronary ostium (in mm), and was determined as the change in HU per 10 mm of length (i.e., HU/10 mm) [7, 8]. We measured TAG using a commercially available workstation (Vitrea version 7.3; Toshiba Medical Systems, Otawara, Japan). Cross-sectional images perpendicular to the vessel centerline were automatically reconstructed for each major coronary vessel, and CT values (HU) were measured at 5-mm intervals from the proximal to the distal level where the vessel cross-sectional area fell below 2.0 mm2. Representative examples are shown in Fig. 1.

Representative case of transluminal attenuation gradient (TAG) measurements of the left anterior descending artery. The white dots represent 5-mm intervals at which intraluminal attenuation [Hounsfield units (HU)] was measured. TAG is shown as an approximate straight line with the least-squares method. a Without significant stenosis, TAG has a moderate negative value (− 0.812 HU/10 mm). b With significant stenosis, TAG has a severe negative value (− 45.35 HU/10 mm)
Coronary CTA combined with TAG
Significant stenosis was defined as ≥ 50% diameter stenosis measured on coronary CTA using a caliper method. For reclassification of the significant stenosis, two models were designed for coronary CTA in conjunction with TAG: (1) the diagnosis was deemed negative when both coronary CTA and TAG results were negative (logical disjunction: CCTA||TAG); or (2) the diagnosis was deemed negative when either the coronary CTA or the TAG result was negative (logical conjunction: CCTA&&TAG). The results determined by coronary CTA, TAG alone, and coronary CTA combined with TAG (CCTA||TAG and CCTA&&TAG) were compared with the result of QCA, and their diagnostic accuracies were evaluated.
Statistical analyses
Data following a parametric distribution (Shapiro–Wilk test, p > 0.05) are described using the mean ± standard deviation (SD). Nonparametric data are described using the median and ranges. Numbers and percentages were used to describe categorical variables. Two independent and blinded observers evaluated coronary CTA. We classified interobserver agreement based on the κ value as follows: κ < 0.4, poor; 0.4 ≤ κ < 0.6, moderate; 0.6 ≤ κ < 0.8, good; and κ ≥ 0.8, excellent. Receiver-operating characteristic (ROC) analysis was used to assess the performance of TAG for detecting ischemia-causing stenosis. The area under the ROC curve (AUC) was calculated for TAG. The optimal cutoff value was derived from the ROC analysis and was defined as the value at maximum sensitivity + (1 − specificity). The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for TAG, coronary CTA, and coronary CTA combined with TAG were calculated on a per-vessel basis and are expressed with the corresponding 95% confidence interval (CI). Differences in the diagnostic abilities of coronary CTA and coronary CTA combined with TAG were evaluated using McNemar’s test.
A p value of less than 0.05 was defined to indicate statistical significance. All statistical analyses were performed using SPSS version 22 software (IBM Co., Armonk, NY, USA).
Results
The clinical characteristics of the study population are summarized in Table 1. Most of the patients were male [30/35 (85.7%)], and the mean coronary calcium score was 252. Twenty of 35 (57.1%) patients and 30 of 130 (23.0%) vessels had obstructive coronary artery disease (CAD) on QCA. The prevalence of CAD in patients and in vessels was 57.1 and 23.0%, respectively. The coronary CTA results were interpreted by two radiologists (κ value 0.83).
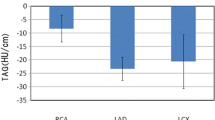
The ROC analysis for TAG in all patients yielded an AUC of 0.745 (95% CI 0.653–0.835), with an optimal cutoff value of − 15.4 HU/10 mm. The AUCs of the TAG in the left anterior descending artery, left circumflex artery, and right coronary artery were 0.710 (95% CI 0.537–0.883), 0.706 (95% CI 0.501–0.912), and 0.761 (95% CI 0.612–0.910), respectively (Fig. 2). The resulting bootstrapped sensitivity, specificity, PPV, NPV, and accuracy of TAG were 75% (95% CI 60–86), 63% (95% CI 59–67), 40% (95% CI 32–46), 89% (95% CI 82–94), and 66% (95% CI 59–72), respectively (Table 2). The diagnostic values of coronary CTA in terms of sensitivity, specificity, PPV, NPV, and accuracy were 75% (95% CI 63–85), 86% (95% CI 80–90), 71% (95% CI 59–80), 89% (95% CI 83–93), and 83% (95% CI 75–89), respectively. The diagnostic values of CCTA||TAG in terms of sensitivity, specificity, PPV, NPV, and accuracy were 94% (95% CI 84–98), 61% (95% CI 55–63), 56% (95% CI 50–59), 94% (95% CI 86–99), and 72% (95% CI 65–75), respectively; the diagnostic values of CCTA&&TAG in terms of sensitivity, specificity, PPV, NPV, and accuracy were 73% (95% CI 63–75), 98% (95% CI 94–99), 88% (95% CI 83–99), 90% (95% CI 85–90), and 90% (95% CI 65–92), respectively (Table 2). The specificity and accuracy of CCTA||TAG were significantly worse compared to those of coronary CT angiography. In contrast, those of CCTA&&TAG were significantly improved without a reduction in sensitivity, PPV, and NPV (Table 3).

The areas under the receiver-operating characteristics curve for transluminal attenuation gradient (TAG). The receiver-operating characteristics (ROC) curve indicates the optimal cutoff value of TAG assessment is − 15.4 HU/10 mm. RCA right coronary artery, LAD left anterior descending artery, LCX left circumflex artery
Discussion
TAG may be useful as a diagnostic tool for significant coronary stenosis. In some cases in our study, TAG was more useful than coronary CTA for diagnosing significant coronary stenosis (Fig. 3). In the present study, we demonstrated that TAG in combination with coronary CTA improves the diagnostic accuracy of morphologically significant stenosis. The cutoff value of TAG is an objective criterion that can be used to determine significant coronary stenosis. In a study that compared TAG between multi- and single-beat scanning using 128-slice dual source CT [10], the cutoff value of single-beat scans was − 14.3 HU/10 mm, which was significantly higher than that of multi-beat scans (− 13.3 HU/10 mm). The cutoff values of TAG using helical or multi-beat scanning have also been shown to vary widely [11,12,13,14]. TAG data produced by different types of scanners can be biased. Because a contrast gradient is used in front of and behind the lesion, data acquisition in a single phase of the same cardiac cycle is ideal. We used 320-row CT, with which whole-heart data acquisition is achieved in one heartbeat. Therefore, there is no time lag among the slices. The cutoff value of TAG from our data was − 15.4 HU/10 mm, which is similar to that reported previously in a study using 320-row CT (− 15.1 HU/10 mm) [7].

A case with borderline stenosis on coronary computed tomography angiography (CTA) judged as negative in logical conjunction of coronary CTA and transluminal attenuation gradient (TAG). a In coronary CTA, the stenosis of the left anterior descending (LAD) artery was measured as 60% stenosis. b TAG value along the lesion was − 14.72 HU and we judged negative on TAG evaluation. In logical conjunction of coronary CTA and TAG (CCTA&&TAG), the lesion was defined as no significant stenosis. c On CAG in left anterior oblique cranial view, the final judgment of the lesion on LAD was not significant
Different scanners might also influence the diagnostic accuracy of TAG. There are many pros and cons to the utility of TAG [7, 8, 10,11,12,13,14,15]. Because of the differences between CT scanners, reproducibility of TAG may be limited. However, with the prospective scanning of the entire heart in one cardiac cycle using 320-row CT, the reproducibility of TAG might improve, because each vascular lumen can be evaluated in the same cardiac phase.
A prior study that compared diagnostic accuracies between FFR-CT and TAG versus invasive fractional flow reserve measurement showed that FFR-CT had the best results [15]. However, the diagnostic value of TAG was still better than that of coronary CT angiography only. Moreover, TAG analysis is less time-consuming (less than 5 min) than FFR-CT analysis, which is convenient in clinical settings.
TAG used in combination with CTA showed improved diagnostic value. In this study, only the logical conjunction (CCTA&&TAG) of coronary CTA and TAG was assessed. With logical disjunction of coronary CTA and TAG (CCTA||TAG), the sensitivity and NPV of diagnosis of obstructive CAD were improved, but specificity and PPV were decreased. On the other hand, with logical conjunction of coronary CTA and TAG (CCTA&&TAG), the specificity, PPV, and NPV were improved with preserved sensitivity. The most reliable point of coronary CTA is its high NPV; however, false positives should be minimized when using a clinical diagnostic tool. The CCTA&&TAG method was more accurate than the CCTA||TAG method in the reclassification of significant coronary artery stenosis. There was a significant difference between the specificity, PPV, NPV, and accuracy of CCTA&&TAG and those of coronary CTA. Statistically, CCTA&&TAG significantly improved specificity; therefore, CCTA&&TAG is considered clinically superior to CCTA||TAG. Thus, when the TAG result is different from the positive finding by coronary CTA, interpreting the final result as negative is optimal.
The present study has several limitations. First, this study included a relatively small number of patients. Second, TAG was not analyzed in patients with a high coronary calcium score (> 1500). In the present study, the maximum calcium score was 1381. Therefore, the efficacy of this method is uncertain in patients with severe coronary artery calcification. Moreover, we excluded patients with various conditions, which may affect the generalizability of the results. In addition, the TAG cutoff value from our study may not be generalizable to studies that use different CT scanners and/or scanning protocols. Third, the lack of correlation with fractional flow reserve might also be a major limitation. In our study group, only a few fractional flow reserve measurements were undertaken. Therefore, we could not analyze the correlation of TAG with fractional flow reserve.
In conclusion, TAG combined with coronary CTA had improved specificity, PPV, NPV, and accuracy compared to coronary CTA alone. The logical conjunction of coronary CTA and TAG improved the diagnostic accuracy of coronary CTA.
References
Doris M, Newby DE. Coronary CT angiography as a diagnostic and prognostic tool: perspectives from the SCOT-HEART trial. Curr Cardiol Rep. 2016;18:18.
Budoff MJ, Dowe D, Jollis JG, Gitter M, Sutherland J, Halamert E, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (assessment by coronary computed tomographic angiography of individuals undergoing invasive coronary angiography) trial. J Am Coll Cardiol. 2008;52:1724–32.
Miller JM, Rochitte CE, Dewey M, Arbab-Zadeh A, Niinuma H, Gottlieb I, et al. Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med. 2008;359:2324–36.
Rochitte CE, George RT, Chen MY, Arbab-Zadeh A, Dewey M, Miller JM, et al. Computed tomography angiography and perfusion to assess coronary artery stenosis causing perfusion defects by single photon emission computed tomography: the CORE320 study. Eur Heart J. 2014;35:1120–30.
Norgaard BL, Leipsic J, Gaur S, Seneviratne S, Ko BS, Ito H, et al. Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in suspected coronary artery disease: the NXT trial (analysis of coronary blood flow using CT angiography: next steps). J Am Coll Cardiol. 2014;63:1145–55.
Min JK, Leipsic J, Pencina MJ, Berman DS, Koo BK, van Mieghem C, et al. Diagnostic accuracy of fractional flow reserve from anatomic CT angiography. JAMA. 2012;308:1237–45.
Wong DT, Ko BS, Cameron JD, Nerlekar N, Leung MC, Malaiapan Y, et al. Transluminal attenuation gradient in coronary computed tomography angiography is a novel noninvasive approach to the identification of functionally significant coronary artery stenosis: a comparison with fractional flow reserve. J Am Coll Cardiol. 2013;61:1271–9.
Choi JH, Min JK, Labounty TM, Lin FY, Mendoza DD, Shin DH, et al. Intracoronary transluminal attenuation gradient in coronary CT angiography for determining coronary artery stenosis. JACC Cardiovasc Imaging. 2011;4:1149–57.
Mitsutake R, Niimura H, Miura S, Zhang B, Iwata A, Nishikawa H, et al. Clinical significance of the coronary calcification score by multidetector row computed tomography for the evaluation of coronary stenosis in Japanese patients. Circ J. 2006;70:1122–7.
Kim HJ, Kim SM, Choi JH, Choe YH. Influence of scan technique on intracoronary transluminal attenuation gradient in coronary CT angiography using 128-slice dual source CT: multi-beat versus one-beat scan. Int J Cardiovasc Imaging. 2017;33:937–46.
Nakanishi R, Matsumoto S, Alani A, Li D, Kitslaar PH, Broersen A, et al. Diagnostic performance of transluminal attenuation gradient and fractional flow reserve by coronary computed tomographic angiography (FFR(CT)) compared to invasive FFR: a sub-group analysis from the DISCOVER-FLOW and DeFACTO studies. Int J Cardiovasc Imaging. 2015;31:1251–9.
Yoon YE, Choi JH, Kim JH, Park KW, Doh JH, Kim YJ, et al. Noninvasive diagnosis of ischemia-causing coronary stenosis using CT angiography: diagnostic value of transluminal attenuation gradient and fractional flow reserve computed from coronary CT angiography compared to invasively measured fractional flow reserve. JACC Cardiovasc Imaging. 2012;5:1088–96.
Choi JH, Koo BK, Yoon YE, Min JK, Song YB, Hahn JY, et al. Diagnostic performance of intracoronary gradient-based methods by coronary computed tomography angiography for the evaluation of physiologically significant coronary artery stenoses: a validation study with fractional flow reserve. Eur Heart J Cardiovasc Imaging. 2012;13:1001–7.
Stuijfzand WJ, Danad I, Raijmakers PG, Marcu CB, Heymans MW, van Kuijk CC, et al. Additional value of transluminal attenuation gradient in CT angiography to predict hemodynamic significance of coronary artery stenosis. JACC Cardiovasc Imaging. 2014;7:374–86.
Ko BS, Wong DT, Norgaard BL, Leong DP, Cameron JD, Gaur S, et al. Diagnostic performance of transluminal attenuation gradient and noninvasive fractional flow reserve derived from 320-detector row CT angiography to diagnose hemodynamically significant coronary stenosis: an NXT substudy. Radiology. 2016;279:75–83.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Nagata, K., Tanaka, R., Takagi, H. et al. Improved diagnostic performance of transluminal attenuation gradient in combination with morphological evaluation of coronary artery stenosis using 320-row computed tomography. Jpn J Radiol 36, 51–58 (2018). https://doi.org/10.1007/s11604-017-0699-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11604-017-0699-7