
Abstract
Although coronary computed tomographic angiography (CCTA) has been a robust diagnostic tool to identify anatomical significance of coronary artery disease (CAD), the utility of CCTA to assess hemodynamic significance of CAD remains unclear. We investigated the diagnostic performance of transluminal attenuation gradient (TAG) and fractional flow reserve derived from CCTA (FFRCT) to predict lesion-specific ischemia by invasive FFR. We identified 103 patients with suspected or known CAD enrolled from the DISCOVER-FLOW and DeFACTO studies who underwent invasive coronary angiography with FFR and high quality ≥64-slice CCTA. Diagnostic performance for predicting abnormal invasive FFR (≤0.80) was assessed for TAG [≤−1.1 HU/mm by the area under the curve (AUC) by receiver-operating characteristic curve analysis (ROC)], FFRCT (≤0.80), and CCTA stenosis (≥50 %). On a per-vessel analysis (n = 146), 52 vessels (35.6 %) had ischemia by invasive FFR. The sensitivity, specificity, positive predictive value and negative predictive value were 53.8, 45.7, 35.4, 64.2 % for TAG, 82.7, 74.5, 64.2, 88.6 % for FFRCT, 84.6, 39.4, 43.6, 82.2 % for CCTA stenosis, respectively. The AUC by ROC curve analysis for FFRCT (0.79) demonstrated greater discrimination of hemodynamic ischemia compared to TAG (0.50, p < 0.0001 vs. FFRCT), CCTA stenosis (0.62, p = 0.0004 vs. FFRCT) and the combination of the two (0.63, p = 0.004 vs. FFRCT). These results remained consistent regardless of the number of CCTA slices. FFRCT allows identification of lesion-specific ischemia using invasive FFR as a reference standard with greater diagnostic accuracy than TAG, CCTA stenosis, or the combination of the two.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Assessment of the hemodynamic significance of coronary stenosis has become the basis for guiding the management of patients with stable coronary artery disease (CAD). The recent DEFER and FAME trials demonstrated that functional assessment by invasive fractional flow reserve (FFR) was superior to anatomic assessment of coronary stenosis by invasive coronary angiography (ICA) in identifying patients who would benefit from coronary revascularization [1–3]. Therefore, the AHA/ACC guideline for percutaneous coronary intervention has recommended using FFR for guiding revascularization decisions as class IIa in patients with stable ischemia heart disease [4]. However, invasive assessment by ICA and invasive FFR may incur higher medical costs and expose patients to greater risks when compared to non-invasive assessments [5].
Coronary computed tomographic angiography (CCTA) has been widely used as a robust non-invasive diagnostic tool to identify anatomic CAD and to correlate highly with stenoses on ICA [6, 7]; however, coronary stenoses observed on CTA has not correlated as highly with noninvasive methods of functional assessment of ischemia or FFR [8]. Recently, techniques for the non-invasive assessment of lesion-specific ischemia by CCTA have been developed. For example, transluminal attenuation gradient (TAG) [9, 10] and FFR derived from CCTA (FFRCT) [11–13] are both methods that require only a single image without any additional image acquisition, contrast, or radiation exposure. However, the comparative utility of TAG and FFRCT for hemodynamic assessment of coronary stenosis has not been well examined. Thus, we investigated the diagnostic performance of TAG and FFRCT to predict lesion-specific ischemia by invasive FFR.
Materials and methods
Study population
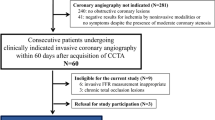
We studied patients with suspected or known CAD enrolled from the DISCOVER-FLOW [11] and DeFACTO studies [12], who underwent ICA with FFR and ≥64 slice coronary CCTA. Out of 355 patients from the DISCOVER-FLOW and DeFACTO studies, we randomly reviewed 199 patients (93 from DISCOVER-FLOW and 106 from DeFACTO) for recalculating FFRCT using the latest-generation of computational fluid dynamic techniques (FFRCT version 1.4; HeartFlow, Inc. Redwood City, California, USA) for comparable results in the current study, since the original FFRCT measures were performed using the previous versions for DISCOVER-FLOW (version 1.1) and DeFACTO (version 1.2). Of those, the following patients were sequentially excluded from this study: insufficient image quality and/or no given nitroglycerin before CCTA for the latest software for modeling FFRCT (n = 89) and for the TAG measurements (n = 7). One hundred three patients (n = 64 from DISCOVER-FLOW and 39 from DeFACTO) were enrolled in the current study. Patients with bypass grafts, stents, and chronic total occlusions were excluded. This study was approved by the Institutional Review Board at each site.
Invasive coronary angiography image acquisition with fractional flow reserve
ICA was performed in accordance with the American College of Cardiology Guidelines for Coronary Angiography [14], and subsequently, FFR was performed using a pressure-monitoring guidewire (PressureWire Certus, St. Jude Medical Systems, Uppsala, Sweden; ComboWire, Volcano Corporation, San Diego, California) after administration of nitroglycerin in vessels with <99 % stenosis as clinically indicated. Hyperemia was induced by administration of intravenous (140 µg/kg/min) or intracoronary (50 µg) adenosine. A threshold of ≤0.80 was considered as an abnormality by FFR [2].
CT image acquisition protocol
All patients underwent ≥64-slice CCTA (Lightspeed VCT, GE Healthcare, Milwaukee, WI; Somatom Sensation and Definition CT, Siemens, Forchheim, Germany; Brilliance 256 and 64, Philips, Surrey, United Kingdom; Aquilion One and 64, Toshiba, Otawara, Japan), including 32 patients (31.1 %) for 64 slice, 51 patients (49.5 %) for 128 slice, 14 patients (13.6 %) for 256 slice, and 6 patients (5.8 %) for 320 slice. Patients received oral and/or intervenous beta-blockades to achieve the target heart rate, as well as sublingual nitroglycerin for coronary artery dilatation. In accordance with Society of Cardiovascular Computed Tomography guideline [15], scan parameters were obtained as follows: tube voltage 100 or 120 kVp, ≤0.75 mm slice thickness and 512 × 512 matrix size. Helical or axial scan was obtained with prospective or retrospective electrocardiogram triggering.
Out of 103 patients, 52 patients underwent non-contrast CT for coronary artery calcium (CAC) before CCTA scanning. Scan parameters were obtained as follows: prospective electrocardiogram-triggering, 512 × 512 matrix size, and peak tube voltage of 120 kVp. Acquired images were transferred to a remote Philips workstation for analysis. All coronary calcium score measurements were performed by a CT core laboratory (Harbor UCLA Medical Center) on a Philips workstation (Intelispace Portal 6.0.1, Philips) to quantify coronary artery calcification using the Agatston method [16].
CCTA image analysis for stenosis severity
CCTAs were assessed using an 18-segment American Heart Association coronary tree model in accordance with Society of Cardiovascular Computed Tomography guidelines [15] by CT core laboratories (CVCTA, San Francisco, California, USA, or Harbor UCLA Medical Center, Torrance, California, USA) in a blinded manner. Coronary plaque was identified as any hyper- or hypodense structure distinct from the lumen and >1 mm2 in size. CAD stenosis severity was visually classified into 0–49, 50–69, and ≥70 % luminal stenosis groups. Obstructive CCTA stenosis was defined as ≥50 % stenosis.
CTA image analysis for TAG
TAG was measured in a blinded fashion by a CT core laboratory at Harbor UCLA Medical Center (Torrance, California, USA). TAG was calculated as the slope of the linear regression on the lumen intensities in the coronary vessel from the ostium to the most distal location with ≥1.5 mm vessel diameter. The lumen intensities were measured at 0.5 mm intervals and defined as the average intensity inside semi-automatically defined lumen boundaries obtained using quantitative CT software (QAngio CT Research Edition 2.0.5, Medis medical imaging systems b.v., the Netherlands).
CTA image analysis for FFRCT
FFRCT was calculated from CCTA data using the latest-generation of computational fluid dynamic techniques (FFRCT v1.4) at HeartFlow, Inc. (Redwood City, California, USA), with blinding to the previous FFRCT measurements. The anatomy, physiology and fluid dynamics were analyzed for the calculation of FFRCT. Anatomic information was derived from CCTA datasets to build 3D models of the epicardial coronary arteries and myocardium. Coronary physiology was calculated with factors including cardiac output, aortic pressure and microcirculatory resistance. These anatomical and physiological models were used to compute FFRCT with computational fluid dynamics [17, 18].
All analyses of these CT variables incorporating CCTA stenosis severity, TAG and FFRCT were performed independently and with blinding to the invasive FFR measurements.
Statistical analysis
Continuous variables are expressed as the mean ± SD. Receiver-operating characteristics (ROC) curve analysis was used to assess the diagnostic performance of CTA stenosis, TAG, the combination of the two, FFRCT, and the combined FFRCT and CTA stenosis in predicting lesion-specific ischemia by invasive FFR (≤0.80). The area under the ROC curves (AUC) was compared between these variables by regression models. From the ROC analysis of our population, −1.1 HU/mm was identified as the optimal cutoff for the prediction of abnormal invasive FFR. In addition, two other thresholds of TAG for abnormality (≤−15.1 HU/10 mm or ≤−0.654 HU/mm) from previous studies [9, 10] were used to assess it's diagnostic performance. In a sub-analysis, we also examined the ROC curve of the comparative diagnostic performance of vessels scanned by a >64 slice CT scanner. The agreement between two observers or the comparison between manual and semi-automated techniques in TAG measurements was assessed by an intraclass correlation coefficient. All statistical calculations were performed using SAS (Version 9.3, SAS Inc., Cary, NC) for Windows.
Inter-observer variability and the comparison between semi-automated versus manual techniques
We randomly selected 20 cases (29 vessels) for inter-observer variability and the comparison between manual and semi-automated assessments. The experienced readers blindly measured TAG using semi-automated quantitative CT software. On per vessel analysis, high correlation was observed between TAG values independently performed by two observers (Correlation coefficient 0.995, 95 % CI 0.94–0.99).
For the assessment of TAG using semi-automated measurements versus manual techniques, we also blindly and manually measured the luminal contrast attenuations across a coronary vessel ≥1.5 mm from the ostium to a distal point at 2.5 mm intervals using a Philips workstation (Intelispace Portal 6.0.1, Philips). TAG was derived from the linear regression model calculated by these contrast attenuations between different intervals of 2.5, 5.0 and 10 mm. TAG measured using semi-automated measurements showed high correlation with that measured by manual techniques at 2.5 mm (Correlation coefficient 0.960, 95 % CI 0.92–0.98), 5.0 mm (Correlation coefficient 0.957, 95 % CI 0.91–0.98) or 10 mm intervals (Correlation coefficient 0.943, 95 % CI 0.88–0.97).
Results
Baseline characteristics of this study are listed in Table 1. Among 103 subjects, 68 % were men, and the mean age was 62 years. A majority of patients had hypertension (62 %) or dyslipidemia (68 %) (Table 1). Median and 75th percentile of CAC was 243 and 562 among 52 patients who underwent CAC scanning (Fig. 1).

Study patient with lesion-specific ischemia by invasive FFR. Invasive FFR demonstrated lesion-specific ischemia with a value of 0.76 in left anterior descending artery (a). FFRCT was highly correlated with invasive FFR (FFRCT = 0.72) (b). With respect to TAG, a value showed −1.0/mm, indicating no ischemia when using −1.1/mm as a cut-off (c) and CCTA also showed non-obstructive coronary artery disease with <50 % stenosis in left anterior descending artery (d). FFR fractional flow reserve, TAG transluminal attenuation gradient, CCTA coronary computed tomographic anigiography
One hundred forty six vessels (left anterior descending artery; n = 91, left circumflex artery; n = 26, and right coronary artery; n = 29) were evaluated in this current study, and maximal stenosis severities with 0–49, 50–69 and 70–99 % observed on CCTA were 45 (31 %), 54 (37 %) and 47 vessels (32 %), respectively. Among the 146 vessels, overall, 52 vessels (35.6 %) met physiological criteria of invasive FFR ≤ 0.80. Figure 2 shows frequencies of CCTA stenosis <50 % or ≥50 % and normal or abnormal TAGs and FFRCT stratified by FFR ≤ 0.8 or FFR > 0.8 in the 146 vessels. The frequencies of false negatives in the vessels assessed by TAGs were approximately threefold higher compared to those in the vessels assessed by FFRCT or CCTA stenosis. In addition, the incidence of false positives was less frequent in the vessels assessed by FFRCT, compared to those by CCTA stenosis or TAGs (Fig. 2).

Frequencies of FFRCT ≤ 0.8 or FFR > 0.8, CCTA stenosis <50 % or ≥50 %, and normal or abnormal TAGs were stratified by FFR ≤ 0.8 or FFR > 0.8 in 146 vessels. A false or true negative was defined if the vessel with FFRCT >0.80, CCTA stenosis <50 %, TAG > −1.1/mm, TAG > −0.6254/mm or TAG > −15.1/10 mm had evidence of invasive FFR ≤0.80 or >0.8. A false or true positive was defined when the vessel with FFRCT ≤ 0.80, CCTA stenosis ≥50 %, TAG ≤ −1.1/mm, TAG ≤ −0.6254/mm or TAG ≤ −15.1/10 mm showed invasive FFR >0.80 or ≤0.80. FFR fractional flow reserve, TAG transluminal attenuation gradient, CCTA coronary computed tomographic anigiography
Diagnostic accuracy of CCTA stenosis, TAGs and FFRCT compared to invasive FFR
Figure 3a illustrates per-patient diagnostic accuracy by different CCTA variables. The diagnostic accuracy of FFRCT (76.7 %) demonstrated the highest performance compared to those of CCTA stenosis and TAG by three thresholds with high specificity (67.9 %). On a per-vessel analysis of 146 vessels, similar results were observed. FFRCT also demonstrated higher per-vessel diagnostic performance compared to that of CCTA stenosis or TAG (Fig. 3b).

a Per patient analysis for diagnostic accuracy of CCTA stenosis, TAG using three thresholds, and FFRCT in 103 patients. b Per-vessel analysis for diagnostic accuracy of CCTA stenosis, TAG using three thresholds, and FFRCT in the 146 vessels. FFR fractional flow reserve, TAG transluminal attenuation gradient, CCTA coronary computed tomographic anigiography
Receiver-operating characteristic curve analysis in predicting lesion-specific ischemia
On a per-patient basis, the AUC by ROC curve analysis for FFRCT (0.7696) demonstrated greater performance for prediction of hemodynamic ischemia compared to that of obstructive stenosis (0.5532, p < 0.0001 vs. FFRCT), TAG with ≤−1.1/mm (0.5208, p = 0.0001 vs. FFRCT), TAG with ≤−0.654/mm (0.5557, p = 0.0006 vs. FFRCT), TAG with ≤−15.1/10 mm (0.5408, p < 0.0001 vs. FFRCT), and the combinations of each TAG and CCTA stenosis. The diagnostic performance for identifying ischemia did not differ between CCTA stenosis and TAG with ≤−1.1/mm (p = 0.59), TAG with ≤−0.654/mm (p = 0.96) or TAG with ≤−15.1/10 mm (p = 0.71). When compared to CCTA stenosis alone (AUC: 0.5532), any TAG values did not add incremental diagnostic yield to CCTA stenosis (AUC: 0.5679 for ≤−1.1/mm, p = 0.68; AUC: 0.5879 for ≤−0.654/mm, p = 0.62, AUC: 0.5796 for ≤−15.1/10 mm, p = 0.90). Of note, CCTA stenosis plus FFRCT did not demonstrate incremental diagnostic value compared to FFRCT alone (0.7762 vs. 0.7696, p = 0.66) (Fig. 4a).

a AUCs by receiver-operating characteristic curve analysis to predict lesion-specific ischemia by invasive FFR in 103 patients. b AUCs by receiver-operating characteristic curve analysis to predict lesion-specific ischemia by invasive FFR in the 146 vessels. AUC area under the curve, ROC receiver-operating characteristic curve, FFR fractional flow reserve, CCTA coronary computed tomographic anigiography, TAG transluminal attenuation gradient
The AUC by ROC curve analysis in predicting lesion-specific ischemia by per vessel assessment is displayed in Fig. 4b. Similarly, the AUC for FFRCT demonstrated significantly greater performance compared to that of other CCTA variables including CCTA stenosis, TAG or a combination of the two. Compared to CCTA stenosis alone (AUC: 0.6199), the combination of TAG and CCTA stenosis did not provide a greater diagnostic value (AUC: 0.6281 for ≤−1.1/mm, p = 0.76; AUC: 0.6402 for ≤−0.654/mm, p = 0.43, AUC: 0.6428 for ≤−15.1/10 mm, p = 0.36). AUCs were not different between FFRCT and the combination of FFRCT and CCTA stenosis (0.7858 vs. 0.8117, p = 0.09) (Fig. 4b).
Diagnostic accuracy of CCTA stenosis, TAG and FFRCT compared to invasive FFR by higher slice (>64 slice) CTs
Figure 5 show the diagnostic accuracy of CCTA variables on higher slice (>64 slice) CT scanners (n = 105 vessels). FFRCT had a higher diagnostic accuracy than CCTA stenosis or TAG.

Diagnostic accuracy of CTA stenosis, TAG using three thresholds, and FFRCT by >64 slice CT in the 105 vessels. FFR fractional flow reserve, TAG transluminal attenuation gradient, CCTA coronary computed tomographic anigiography
Discussions
TAG is a novel method developed to assess the hemodynamic significance of CAD and is calculated using a linear regression model of luminal contrast attenuations in a coronary vessel obtained by manual or semi-automated techniques [9, 10, 19–22]. To date, several studies have examined the relation of TAG to invasive FFR and have shown a variety in the diagnostic accuracy of TAG in predicting lesion-specific ischemia by invasive FFR <0.80. Yoon et al. investigated the diagnostic accuracy of TAG and FFRCT for identifying lesion-specific ischemia among 53 patients who underwent 64 slice CCTA [9]. In a per-vessel analysis, TAG showed a low sensitivity but a high specificity of 38 and 88 %, respectively. In addition, the diagnostic performance of TAG was lower but not statistically different from that of CCTA stenosis alone (AUC: 0.63 vs. 0.73, p = 0.217) [9]. Choi also demonstrated similar results showing lower diagnostic performance of TAG than that of CCTA stenosis (AUC: 0.696 vs. 0.726) among 63 patients undergoing 64-slice CCTA [22]. These findings are in line with our results demonstrating only a modest diagnostic performance of TAG.
In contrast with these studies, another study of 54 patients undergoing 320 slice CCTA by Wong et al. [10] demonstrated acceptable diagnostic accuracy for the determination of abnormal invasive FFR in addition to CCTA stenosis (AUC: 0.88, p < 0.001). The discordance of the study by Wong et al. and the results of our study as well as Yoon and Choi’s study may be explained by variations in contrast along vessels using scanners that require sequential heart cycles for image acquisition, which does not occur with the 320 slice CT scanner that covers the whole heart within one heartbeat. For solving the issue in assessing TAG by limited CT slices, Stuijfzand et al. [20] prospectively examined the comparative utility of TAG and TAG with corrected coronary opacification (CCO) (TAG-CCO), which potentially corrects the temporal contrast variations in a coronary artery between scans, among 85 patients undergoing 256 slice CCTA [23]. However, the diagnostic performance of TAG-CCO did not differ from that of CCTA stenosis alone (AUC: 0.88 vs. 0.85). Another potential issue may be that an optimal cut-off of TAG has not yet been established and the range of thresholds of TAG to predict lesion-specific ischemia has varied widely, ranging from −0.654 HU/mm (64 slice) to −15.1 HU/10 mm (320 slice) [9, 10, 20]. Although optimal thresholds for TAG were derived from ROC curve analysis among their limited cohort in these previous studies, the cut-off of TAG including various CT slices derived from ROC curve analysis was −1.1 HU/mm in our study, which is in line between these ranges. Even when using the two thresholds for abnormality from previous studies [9, 10], our study demonstrated that the diagnostic performance of TAG was similarly modest.
With respect to FFRCT, our findings recalculated by the latest-generation software are similar to those previously reported in the main DISCOVER-FLOW and DeFACTO studies [11, 12]. The current generation used in the current study allows more time-saving for each case to create 3-D coronary modeling and computed FFRCT while maintaining high diagnostic accuracy for the determination of functional significant CAD compared to previous versions, allowing the use of FFRCT to fit into more clinical settings. The diagnostic accuracy of FFRCT was superior to that of TAG or CCTA stenosis, which is concordant with the aforementioned study by Yoon et al. [9]. FFRCT is derived from CCTA data at rest using computational fluid dynamic techniques and is not affected by the number of cardiac cycles needed for acquisition. The optimal cut-off value of FFRCT has generally been more consistent and reliable compared to TAG, as it is similar to that of invasive FFR. Since Yoon et al. examined their study among patients undergoing only 64 slices CT, our study is the first study to explore the comparative feasibility and utility of TAG and FFRCT using multi detector CT platforms with broad Z axis coverage among a much larger population. Our current study expanded the patient cohort and the scanner technology with large detector CT scanners to reflect real world use. By our sub-analysis among patients with higher CT slices, the diagnostic performance of FFRCT was always superior to that of TAG. Another potential explanation for the greater diagnostic accuracy of FFRCT compared to that of TAG and the modest diagnostic performance of TAG may be that FFRCT computation considers numerous variables observed on CCTA, estimating coronary blood flow, and pressure at maximum hyperemia [17, 18]. Meanwhile, TAG assesses only a drop in contrast across a stenotic lesion in the coronary vessel in the rest condition and does not take into account the complex array of variables that are used by FFRCT to model flow reserve from the rest CCTA. Therefore, abnormality by TAG is likely to be associated with severe anatomic stenosis [24] as well as limited coronary flow [23], and TAG may fail to detect stenosis that limits flow as assessed by invasive FFR during pharmacologic stress but does not reduce resting coronary flow. This underlying mechanism may also explain why the combination of TAG and CCTA stenosis did not provide a greater diagnostic performance over CCTA stenosis alone in the current study and the aforementioned study [20].
Recently, Wong et al. explored the diagnostic utility of the hybrid assessment by CCTA stenosis ≥50 %, TAG, and computed tomography stress myocardial perfusion imaging in identifying lesion-specific ischemia [21]. This combined assessment by CCTA may have a potential role in more accurately identifying patients who would benefit from ICA and revascularization, while maintaining a higher sensitivity and specificity compared to CCTA stenosis alone. Of importance, our study demonstrated the diagnostic performance of the combined FFRCT and CCTA stenosis ≥50 % was similar compared to that of FFRCT alone. This is certainly true because FFRCT is computed from the complex array of numerous CCTA variables including anatomical models or fluid dynamic models and does not require additional CCTA information. Therefore, FFRCT can be used as a substitute for invasive FFR and can be a novel method in guiding patient care.
Limitation
There are several limitations in this current study. Given a small sample size including only six patients undergoing 320 slice CT; we could not separately analyze the comparative diagnostic accuracy between TAG and FFRCT among this cohort. In addition, since a semi-automated CT software only calculated TAG in coronary arteries and does not provide TAG-CCO for correcting temporal contrast attenuations, we did not assess the diagnostic utility of TAG-CCO among patients with <320 slice CTs. Recent paper has reported quantitative CCTA stenosis improves the identification of functional significant CAD compared to visual CCTA stenosis [25]. However, we do not have the data regarding quantitative CCTA stenosis in the current study.
Conclusion
The innovative technique of FFRCT based on computational fluid dynamics allows for better predictions of lesion-specific ischemia by invasive FFR. In addition, its diagnostic accuracy is greater than TAG, CCTA obstructive stenosis or these two in combination. The diagnostic performance of TAG is modest and limited in assessing hemodynamic ischemia.
Abbreviations
- CCTA:
-
Coronary computed tomographic angiography
- CAD:
-
Coronary artery disease
- FFR:
-
Fractional flow reserve
- TAG:
-
Transluminal attenuation gradient
References
Pijls NH, van Schaardenburgh P, Manoharan G, Boersma E, Bech JW, van’t Veer M, Bar F, Hoorntje J, Koolen J, Wijns W, de Bruyne B (2007) Percutaneous coronary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER Study. J Am Coll Cardiol 49:2105–2111
Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, van’t Veer M, Klauss V, Manoharan G, Engstrøm T, Oldroyd KG, Ver Lee PN, MacCarthy PA, Fearon WF, FAME Study Investigators (2009) Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med 360:213–224
Pijls NH, Fearon WF, Tonino PA, Siebert U, Ikeno F, Bornschein B, van’t Veer M, Klauss V, Manoharan G, Engstrom T, Oldroyd KG, Ver Lee PN, MacCarthy PA, De Bruyne B, FAME Study Investigators (2010) Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease: 2-year follow-up of the FAME (fractional flow reserve versus angiography for multivessel evaluation) study. J Am Coll Cardiol 56:177–184
Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, Khot UN, Lange RA, Mauri L, Mehran R, Moussa ID, Mukherjee D, Nallamothu BK, Ting HH (2011) 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation 124:e574–e651
Hlatky MA, Saxena A, Koo BK, Erglis A, Zarins CK, Min JK (2013) Projected costs and consequences of computed tomography-determined fractional flow reserve. Clin Cardiol 36:743–748
Budoff MJ, Dowe D, Jollis JG, Gitter M, Sutherland J, Halamert E, Scherer M, Bellinger R, Martin A, Benton R, Delago A, Min JK (2008) Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (assessment by coronary computed tomographic angiography of individuals undergoing invasive coronary angiography) trial. J Am Coll Cardiol 52:1724–1732
Meijboom WB, Meijs MF, Schuijf JD, Cramer MJ, Mollet NR, van Mieghem CA, Nieman K, van Werkhoven JM, Pundziute G, Weustink AC, de Vos AM, Pugliese F, Rensing B, Jukema JW, Bax JJ, Prokop M, Doevendans PA, Hunink MG, Krestin GP, de Feyter PJ (2008) Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol 52:2135–2144
Meijboom WB, van Mieghem CA, van Pelt N, Weustink A, Pugliese F, Mollet NR, Boersma E, Regar E, van Geuns RJ, de Jaegere PJ, Serruys PW, Krestin GP, de Feyter PJ (2008) Comprehensive assessment of coronary artery stenoses: computed tomography coronary angiography versus conventional coronary angiography and correlation with fractional flow reserve in patients with stable angina. J Am Coll Cardiol 52:636–643
Yoon YE, Choi JH, Kim JH, Park KW, Doh JH, Kim YJ, Koo BK, Min JK, Erglis A, Gwon HC, Choe YH, Choi DJ, Kim HS, Oh BH, Park YB (2012) Noninvasive diagnosis of ischemia-causing coronary stenosis using CT angiography: diagnostic value of transluminal attenuation gradient and fractional flow reserve computed from coronary CT angiography compared to invasively measured fractional flow reserve. JACC Cardiovasc Imaging 5:1088–1096
Wong DT, Ko BS, Cameron JD, Nerlekar N, Leung MC, Malaiapan Y, Crossett M, Leong DP, Worthley SG, Troupis J, Meredith IT, Seneviratne SK (2013) Transluminal attenuation gradient in coronary computed tomography angiography is a novel noninvasive approach to the identification of functionally significant coronary artery stenosis: a comparison with fractional flow reserve. J Am Coll Cardiol 61:1271–1279
Koo BK, Erglis A, Doh JH, Daniels DV, Jegere S, Kim HS, Dunning A, DeFrance T, Lansky A, Leipsic J, Min JK (2011) Diagnosis of ischemia-causing coronary stenoses by noninvasive fractional flow reserve computed from coronary computed tomographic angiograms. Results from the prospective multicenter DISCOVER-FLOW (diagnosis of ischemia-causing stenoses obtained via noninvasive fractional flow reserve) study. J Am Coll Cardiol 58:1989–1997
Min JK, Leipsic J, Pencina MJ, Berman DS, Koo BK, van Mieghem C, Erglis A, Lin FY, Dunning AM, Apruzzese P, Budoff MJ, Cole JH, Jaffer FA, Leon MB, Malpeso J, Mancini GB, Park SJ, Schwartz RS, Shaw LJ, Mauri L (2012) Diagnostic accuracy of fractional flow reserve from anatomic CT angiography. JAMA 308:1237–1245
Nørgaard BL, Leipsic J, Gaur S, Seneviratne S, Ko BS, Ito H, Jensen JM, Mauri L, De Bruyne B, Bezerra H, Osawa K, Marwan M, Naber C, Erglis A, Park SJ, Christiansen EH, Kaltoft A, Lassen JF, Bøtker HE (2014) Achenbach S and group Nts. Diagnostic performance of non-invasive fractional flow reserve derived from coronary CT angiography in suspected coronary artery disease: the NXT trial. J Am Coll Cardiol 63(12):1145–1155
Scanlon PJ, Faxon DP, Audet AM, Carabello B, Dehmer GJ, Eagle KA, Legako RD, Leon DF, Murray JA, Nissen SE, Pepine CJ, Watson RM, Ritchie JL, Gibbons RJ, Cheitlin MD, Gardner TJ, Garson A Jr, Russell RO Jr, Ryan TJ, Smith SC Jr (1999) ACC/AHA guidelines for coronary angiography. A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Coronary Angiography). Developed in collaboration with the society for cardiac angiography and interventions. J Am Coll Cardiol 33:1756–1824
Leipsic J, Abbara S, Achenbach S, Cury R, Earls JP, Mancini GJ, Nieman K, Pontone G, Raff GL (2014) SCCT guidelines for the interpretation and reporting of coronary CT angiography: a report of the society of cardiovascular computed tomography guidelines committee. J Cardiovasc Comput Tomogr 8:342–358
Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M, Detrano R (1990) Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 15:827–832
Taylor CA, Fonte TA, Min JK (2013) Computational fluid dynamics applied to cardiac computed tomography for noninvasive quantification of fractional flow reserve: scientific basis. J Am Coll Cardiol 61:2233–2241
Zarins CK, Taylor CA, Min JK (2013) Computed fractional flow reserve (FFTCT) derived from coronary CT angiography. J Cardiovasc Transl Res 6:708–714
Steigner ML, Mitsouras D, Whitmore AG, Otero HJ, Wang C, Buckley O, Levit NA, Hussain AZ, Cai T, Mather RT, Smedby O, DiCarli MF, Rybicki FJ (2010) Iodinated contrast opacification gradients in normal coronary arteries imaged with prospectively ECG-gated single heart beat 320-detector row computed tomography. Circ Cardiovasc Imaging 3:179–186
Stuijfzand WJ, Danad I, Raijmakers PG, Marcu CB, Heymans MW, van Kuijk CC, van Rossum AC, Nieman K, Min JK, Leipsic J, van Royen N, Knaapen P (2014) Additional value of transluminal attenuation gradient in CT angiography to predict hemodynamic significance of coronary artery stenosis. JACC Cardiovasc Imaging 7:374–386
Wong DT, Ko BS, Cameron JD, Leong DP, Leung MC, Malaiapan Y, Nerlekar N, Crossett M, Troupis J, Meredith IT, Seneviratne SK (2014) Comparison of diagnostic accuracy of combined assessment using adenosine stress computed tomography + computed tomography angiography with transluminal attenuation gradient + computed tomography angiography against invasive fractional flow reserve. J Am Coll Cardiol 63:1904–1912
Choi JH, Koo BK, Yoon YE, Min JK, Song YB, Hahn JY, Choi SH, Gwon HC, Choe YH (2012) Diagnostic performance of intracoronary gradient-based methods by coronary computed tomography angiography for the evaluation of physiologically significant coronary artery stenoses: a validation study with fractional flow reserve. Eur Heart J Cardiovasc Imaging 13:1001–1007
Chow BJ, Kass M, Gagne O, Chen L, Yam Y, Dick A, Wells GA (2011) Can differences in corrected coronary opacification measured with computed tomography predict resting coronary artery flow? J Am Coll Cardiol 57:1280–1288
Choi JH, Min JK, Labounty TM, Lin FY, Mendoza DD, Shin DH, Ariaratnam NS, Koduru S, Granada JF, Gerber TC, Oh JK, Gwon HC, Choe YH (2011) Intracoronary transluminal attenuation gradient in coronary CT angiography for determining coronary artery stenosis. JACC Cardiovasc Imaging 4:1149–1157
Rossi A, Papadopoulou SL, Pugliese F, Russo B, Dharampal AS, Dedic A, Kitslaar PH, Broersen A, Meijboom WB, van Geuns RJ, Wragg A, Ligthart J, Schultz C, Petersen SE, Nieman K, Krestin GP, de Feyter PJ (2014) Quantitative computed tomographic coronary angiography: does it predict functionally significant coronary stenoses? Circ Cardiovasc Imaging 7:43–51
Acknowledgments
Dr. Matthew Budoff is a consultant for General Electric. Dr. James K. Min has served on the medical advisory boards of GE Healthcare, Arineta, Astra Zeneca, and Bristol-Myers Squibb; Speakers’ Bureau of GE Healthcare; and received research support from GE Healthcare, Vital Images, and Phillips Healthcare. Dr. Min serves as a consultant to Astra Zeneca and HeartFlow.; the other authors have no conflict of interest. This study is funded in part by HeartFlow Inc. The authors thank Vivek Bhatia, Souma Sengputa, Michael Fahmy, Jeby Abraham, Lucas Cespedes, and Christopher Dailing for contributions to this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Nakanishi, R., Matsumoto, S., Alani, A. et al. Diagnostic performance of transluminal attenuation gradient and fractional flow reserve by coronary computed tomographic angiography (FFRCT) compared to invasive FFR: a sub-group analysis from the DISCOVER-FLOW and DeFACTO studies. Int J Cardiovasc Imaging 31, 1251–1259 (2015). https://doi.org/10.1007/s10554-015-0666-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-015-0666-2