
Abstract
The World Health Organization estimates that by the year 2040, neurodegenerative diseases will be the second leading cause of death in developed countries, overtaking cancer-related deaths and exceeded only by cardiovascular disease–related death. The search for interventions has therefore become paramount to alleviate some of this burden. Based on pathways affected in neurodegenerative diseases, hyperbaric oxygen treatment (HBOT) could be a good candidate. This therapy has been used for the past 50 years for conditions such as decompression sickness and wound healing and has been shown to have promising effects in conditions associated with neurodegeneration and functional impairments. The goal of this review was to explore the history of hyperbaric oxygen therapy, its uses, and benefits, and to evaluate its effectiveness as an intervention in treating neurodegenerative diseases. Additionally, we examined common mechanisms underlying the effects of HBOT in different neurodegenerative diseases, with a special emphasis on epigenetics.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Neurodegenerative diseases (NDD) can be characterized by a continuous or progressive loss of a specific vulnerable neuronal population in the brain or spinal cord [1]. The classification of NDD can be based on the anatomical spread of neurodegeneration (e.g., extrapyramidal disorders, frontotemporal degenerations, or spinocerebellar degenerations), the primary molecular abnormality (e.g., amyloid-β, prion protein, tau, α-synuclein), or the main clinical features (e.g., parkinsonism, motor neuron disorder, or dementia) [1, 2]. Despite these differential classifications and symptoms presentations, NDDs, including disorders such as Parkinson’s disease (PD), amyotrophic lateral sclerosis (ALS), and Alzheimer’s disease (AD), share certain processes that lead to the dysfunction and eventual death of neurons. Some of the major common factors involved in NDDs are oxidative stress, programmed cell death, neuroinflammation, mitochondrial dysfunction, epigenetic modifications, proteotoxic stress, and impairment of its associated ubiquitin/proteasomal and autophagosomal systems [2]. Because of these commonalities, it is not surprising to observe an overlap of symptomology in these diseases [1].
Millions of individuals are affected by NDDs worldwide, so much so that by 2040, the World Health Organization estimates that NDDs will be the second leading cause of death in developed countries [3]. Treatments are available to relieve and manage symptoms of particular diseases [4]; however, effective therapies to slow down the progress or cure these diseases are still lacking. Recent studies show a paradigm shift from just symptomatic management to prevention of further deterioration mainly by cytoprotective mechanisms. Substantial evidence points to oxidative stress and inflammation playing a fundamental role in neurodegeneration. Thus, these mechanisms have become targets for cytoprotection [4]. Hyperbaric oxygen therapy (HBOT) has been used over the past 50 years for a variety of conditions such as decompression sickness, wound healing, and in conditions where oxygen levels are compromised [5]. HBOT reduces neuroinflammation in severe brain dysfunctions and has the capacity to down-regulate proinflammatory cytokines (IL-1β, IL-12, TNFα, and IFNγ) while upregulating an anti-inflammatory cytokine (IL-10) making it potentially cytoprotective [6]. Recently, basic and clinical research has shown the potential of HBOT to treat neurodegenerative diseases [7,8,9]. The goal of this narrative review is to provide a historical context on the use of HBOT, to consider its efficacy in treating NDDs in preclinical and clinical settings, and to highlight the mechanisms underlying its beneficial effects with a fresh perspective on the role of epigenetics.
Search
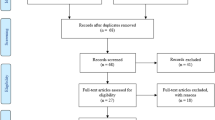
The literature search was conducted using PubMed from 1968 to 2022, using the following keywords: “Hyperbaric oxygen therapy,” “Hyperbaric oxygen,” “neurodegenerative disease,” “Alzheimer’s disease,” “Parkinson’s Disease,” and “Amyotrophic lateral sclerosis.” Articles written in English that were full text were included in the review. Articles that had a direct relation with hyperbaric oxygen and neurodegenerative diseases were reviewed. As the articles were evaluated, some of the references made were further explored and added to this review.
Hyperbaric oxygen therapy (HBOT)
Normoxic conditions (20.8% oxygen) are necessary to maintain effective metabolism, and any slight deviation from this concentration can lead to major physiological alterations [10]. Hypoxic conditions are sensed by chemoreceptors leading to altered cellular response. Generally, mitochondria signal the onset of hypoxia by generating reactive oxygen species via the electron transport chain. The reactive oxygen species, once released into the intermembrane space of the mitochondria, activate enzymes, transcription factors, and post‐translational responses [11]. The focus of this review is on hyperbaric oxygen, which relates to exposure to 100% oxygen while in a pressurized chamber. The pressure needs to be higher than 1 atmosphere absolute (ATA) which is considered sea level [12]. Hyperbaric oxygen treatment usually entails increasing the pressure to 2.0–2.5 ATA for a duration of 90–120 min, with a number of therapeutic sessions depending on the conditions being treated [13]. The air pressure increase leads to improve oxygen cellular delivery [10]. Oxygen increases and in turn stimulates stem-cell proliferation and certain growth factors that mediate the healing process [10]. However, an increase in oxygen may lead to excess oxidative stress which could lead to damages of macromolecules like deoxyribonucleic acid, proteins, and lipids [14], which was the main reason for prior reluctance in using HBOT as a therapeutic tool.
Historical perspective
The history of HBOT is closely related to that of diving medicine, with origins dating back to the 1500 s when Leonardo Da Vinci made drawings of diving appliances [15]. It was not until 1662, however, that hyperbaric therapy was first documented when Henshaw, a British physician, built an airtight chamber called a “Domicilium” that could simulate various climate and pressure conditions [15]. In 1834, Junrod treated pulmonary problems with a hyperbaric chamber in France [15]. Over time, hyperbaric chambers became more present and were available in most cities of Europe. However, the challenge was that there was no scientific rationale for the use of HBOT and no standardized prescription across physicians [16]. In 1775, the discovery of oxygen led to its use in lieu of compressed gases, yet it was short-lived as Lavoisier and Seguin reported the harmful effects of concentrated oxygen in 1789 [16]. Subsequently, Bert suggested the use of normobaric instead of hyperbaric oxygen for decompression sickness [16]. Behnke and Shaw were the first to utilize HBOT for decompression sickness treatment in 1937 based on the model devised by Drager, who first explored the possibility of treating this condition with oxygen under pressure [16].
Hyperbaric oxygen therapy indications and caveats
The initial uses of HBOT were based on the pressure-dependent effervescent reducing action (Boyle-Marriott law) and the hyperoxygenation of tissues [17]. Pathologies with known benefits from the hyperoxic state created by HBOT are necrotizing tissues, radiation injury, wounds and burns, compartment syndromes, and gas gangrene [18], and several others as listed by the Undersea and Hyperbaric Medical Society [19]. The other mechanism (bubble-reducing effect) has been associated with another set of indications that benefits from HBOT such as decompression sickness and air/gas embolism [19]. In fact, HBOT remains the only treatment available for decompression sickness, a result of nitrogen forming gas bubbles in tissues and blood due to a partial increase in nitrogen’s pressure from divers rising too quickly to the water surface [20]. Another major issue that HBOT is used for as a life-saving treatment is carbon monoxide poison. Typically, carbon monoxide has an affinity for hemoglobin 240 times higher than that of oxygen. Hence, the ability of the blood to carry oxygen is decreased in the presence of carbon monoxide. Hyperbaric oxygen supplies the tissue with oxygen by enhancing its dissolution in the plasma, and by freeing hemoglobin from carbon monoxide [20]. Noteworthy, for certain conditions, HBOT is used as an adjunctive treatment and has demonstrated improvements in a variety of inflammatory or infectious disease models such as colitis, sepsis, and others [17]. Based on the anti-inflammatory and oxygenation mechanisms of HBOT, there is some potential for it to be a therapy used in neurodegenerative diseases, which we will discuss further below.
It is important to note that the use of hyperbaric oxygen therapy must not exceed a pressure of 3 ATA and not be administered for more than 2 h at a time, as this typically results in toxicity [17]. The side effects of HBOT are usually dependent on pressure and time exposure [12]. Generally, side effects, such as headache, claustrophobia, and reversible myopia, are tolerable and easily reversed when the therapy is halted [21]. Interestingly, HBOT has been used as a tool to induce oxidative stress in screening potential antioxidants, using high pressure for long periods of time (above 4 ATA and for a period exceeding 3 h) [12, 17].
Hyperbaric oxygen and neurodegenerative diseases
Rationale for the use of HBOT in neurodegenerative diseases
Diseases associated with a reduced loss of oxygen supply predispose the individual to neurodegeneration [22] suggesting a major role of hypoxia in NDDs. Hypoxia-inducible factor-1 (HIF-1), a transcriptional factor fundamental to cellular and tissue adaption to low oxygen tension, has been implicated in a host of NDDs including Alzheimer’s (AD), Parkinson’s (PD), Huntington’s diseases (HD), and amyotrophic lateral sclerosis (ALS) and has become a potential medicinal target [21, 23]. The incidence of AD, for instance, is greatly increased following conditions associated with hypoxia such as stroke and cerebral ischemia [24, 25]. Furthermore, cerebral hypoperfusion which gives rise to cerebral hypoxia has been observed in the early stages of AD, with strong correlations to both worsening of function and structural components implicated in AD [26,27,28]. Hypoxia is known to drive hyperphosphorylation of tau, dysfunction of the blood–brain barrier, accumulation of β-amyloid (Aβ), and degeneration of neurons [29]. In the case of Parkinson’s disease (PD), hypoxic brain injury enhances α-synuclein (α-syn) expression and aggregation which is a pathological hallmark of PD [22]. It has been postulated that hypoxia through HIF-1α in dopaminergic cells upregulates ATP13A2 (PARK9), a transcription factor with mutations that have been found in postmortem PD [22]. Occupations that could cause hypoxic conditions, like being a firefighter, double the risk to develop amyotrophic lateral sclerosis (ALS). In fact, hypoxia is not only one of the causing factors of ALS but also drives the progression of it [22]. Neurotoxicity and cell death induced by hypoxia involve a complex plethora of factors that tend to be interrelated. They include mitochondrial dysregulation, oxidative stress, inflammation, metal homeostasis, apoptosis, synaptic transmission, and autophagy, all contributing to neuronal death [22]. Another factor affecting the development of dementia and age-related cognitive declines is the cerebromicrovasculature, as impaired microcirculation has been associated with vascular cognitive impairments [30]. Since the fundamental problem in the above-described conditions is a dearth of oxygen, the theoretical approach to address this problem is to augment oxygen in the system; therefore, HBOT may be a viable tool in their management [30, 31].
As age is a major risk factor for the development of several neurodegenerative diseases [32], it is important to discuss the effect of HBOT on the neurobiology of aging. HBOT improved age-related cognitive deficits in healthy elderly subjects [33]. In that study, male patients with a mean age of 68 years exhibiting clinical manifestations of intellectual deterioration were assessed after 30 intermittent exposures to 100% oxygen at 2.5 ATA. Psychological tests of cognitive functioning showed highly significant gains in treated subjects as compared to control levels [33]. In a recent randomized control clinical trial, healthy adults aged above 64 years were either exposed to HBOT or no treatment for 3 months. HBOT induced cognitive improvement in these healthy aging adults through mechanisms involving regional changes in cerebral blood flow (CBF) measured by perfusion magnetic resonance imaging [34]. Also, elderly patients who had significant memory loss exhibited improved cognition and increased cerebral blood flow after exposure to HBOT [35]. In a pre-clinical model of aging (D-gal-induced aging) in rats [36] and mice [37, 38] as well as in a model of aging and obesity [36], HBOT prevented cognitive impairments and hippocampal-dependent pathologies via augmentation of cholinergic pathways, anti-apoptotic effects [37], and reduction in oxidative damage and inflammatory responses [36, 37].
Clinical studies of HBOT in neurodegenerative diseases
Several clinical studies have been conducted to evaluate the influence of HBOT on neurodegenerative diseases, and of other neurological conditions like stroke and traumatic brain injury which predisposes patients to developing neurodegenerative diseases like AD (Table 1). In a randomized prospective crossover control trial of mild traumatic brain injury (mTBI), 56 patients were enrolled and the treated group was exposed to 40 HBOT sessions (60 min a day at a pressure of 1.5 ATA) [39]. The Mindstreams battery test for evaluating cognition, EQ-5D for quality of life, and SPECT imaging for assessing brain activity were carried out. Treatment with hyperbaric oxygen improved cognitive function and quality of life significantly and treated patients also exhibited increased brain activity [39]. In another study, the same research group using the same HBOT protocol determined that the treatment led to a reduction in memory impairment in post-stroke patients [40]. In a case study, a 58-year-old woman, diagnosed with rapid progression AD, was exposed to HBOT for 8 weeks at 1.15 atmosphere absolute with 50-min total treatment time, once per day, 5 days per week [41]. The patient became more energetic and her capacity to carry out tasks like drawing of clock and daily living was improved after the 21st day of HBOT. PET imaging showed a corresponding regional and global increase in brain metabolism [41]. In a larger clinical study including control AD patients, AD patients, and amnestic mild cognitive impairment (aMCI), psychiatric assessments including Montreal cognitive assessment (MoCA), mini-mental state examination (MMSE), and activities of daily living (ADL) scale before and at different months after treatment were carried out. Treatment involved exposing AD and aMCI patients to 40 min of oxygen at a pressure of 0.12 Megapascal (MPa) (equivalent of 1.18 ATA) separated by 20-min intervals. HBOT improved cognitive function significantly assessed by MMSE and MoCA in AD patients after a month follow-up. MMSE score was also improved by treatment at 3 months while MoCA score saw improvement at both 1- and 3-month follow-ups in aMCI patients [42]. Another case study reported that HBOT treatment given to Parkinson’s disease patient over a period of 30 days improved non-motor symptoms of severe depression and anxiety [43]. Phase I clinical trial involving 5 ALS patients treated with hyperbaric oxygen at 2 atmospheres pressure for 60 min daily for 5 days a week for 4 weeks resulted in decreased fatigue and increased muscle strength [44].
Pre-clinical studies of HBOT in neurodegenerative diseases
There are several pre-clinical studies also suggesting a beneficial role of HBOT in a variety of animal models (Table 2). In a mouse model of AD (3 × Tg), HBOT improved cognition while reducing inflammation, plaque burden, and Tau phosphorylation [9]. In that study, male 3 × Tg mice aged 17 months were used with 14-month-old C57BL/6 male mice as controls. The treatment with HBO consisted of 2 ATA for an hour daily for 14 consecutive days and resulted in diminished neuroinflammatory processes by reducing microgliosis, astrogliosis, and the secretion of pro-inflammatory cytokines while improving cognition in the process [9]. In another study, HBOT improved cognition in a mouse model of AD (5 × FAD) and improved cerebral blood flow [35]. A combination of HBOT and Ginkgo biloba extract has also been found to ameliorate cognitive and memory impairment in an AD model of rat induced by injecting Aβ 25–35 [45], through inhibiting oxidative stress by blocking mitochondria-mediated apoptosis signaling [46], activation of NF-κB[45] and enhancing of superoxide dismutase, an antioxidative enzyme, in rat hippocampal tissue [47]. Pre-treatment of HBOT has also been shown to lower the rate of hippocampal p38 mitogen-activated protein kinase phosphorylation with a reduction of hippocampal damage [48]. In a Parkinson’s disease rodent model (6-hydroxydopamine model), the combinatory effect of HBOT and Madopar (levodopa-used for management of Parkinson’s disease) therapy was evaluated. Both HBOT and the combination therapy reduced apomorphine-induced turning in PD rats and offered neuroprotective effect on substantia nigra’s dopaminergic neurons [49]. In another model of PD, the 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) mice, protective mechanisms of HBOT on neurons and motor function were evaluated. The locomotor activity and grip strength of the mice were increased alongside increased mitochondria biogenesis signaling (SIRT-1, PGC-1α, and TFAM) [50]. Furthermore, mild hyperbaric oxygen inhibited the decrease of dopaminergic neurons in the substantia nigra [51]. The improvement of motor deficits in Parkinson’s disease has also partly been attributed to the increase in norepinephrine after HBOT exposure [52]. HBOT has also been shown to improve function in a model of human motor neuron disease (Wobbler mouse). HBOT was administered at 2 ATA for 1 h daily for 30 days. The treatment significantly delayed the onset of the disease as measured by both paw condition and walking; from 36 ± 4.3 days to 59 ± 8.2 days (walking) and from 40 ± 5.7 days to 63 ± 7.6 days (paw condition) [53].
Mechanisms of HBOT
HBOT affects diverse cellular and molecular pathways that are important for cellular and neuronal recovery such as oxidative stress, mitochondrial functions, inflammation, apoptosis, microcirculation, and epigenetics via interconnected pathway [30, 31] (Table 3). As aforementioned, these processes and pathways are fundamental and common in most NDDs.
Effect of HBOT on inflammation, oxidative stress, and mitochondrial functions
HBOT reduces neuroinflammation in severe brain dysfunctions. HBOT has the capacity to downregulate proinflammatory cytokines (IL-1β, IL-12, TNFα, and IFNγ) and upregulate an anti-inflammatory cytokine (IL-10) as shown in an atherosclerosis rodent model [6]. More so, it is reported to inactivate cyclooxygenase, the same target enzyme for non-steroidal anti-inflammatory disease [54]. Evidence suggests that even though HBOT increases the level of lipid peroxidation and/or protein oxidation in blood and tissues of HBOT-exposed organisms under certain conditions [12, 14], however, HBOT has also been associated with a significant elevation in antioxidants defenses such as superoxide dismutase, catalase, and glutathione peroxidase [17]. What is even more fascinating is that some researchers argue that ROS generated by HBOT mediates and signals some of the beneficial effects of HBOT [14, 17, 55]. Thus, aside from the pressure-dependent effervescence-reducing action and the hyperoxygenation saturation of tissues, the beneficial effect of HBOT has been argued to be in part, dependent on the physiological roles of the reactive oxygen species generated [56, 57]. Superoxide radicals along with hydrogen peroxide are known to be the major fraction of ROS produced via HBOT [58]. Through a series of steps, they activate transcription factors, nuclear factor erythroid 2-related factor 2 (Nrf2), and hypoxia-inducible factor-1 alpha (HIF-1α) along with their main target protein, heme oxygenase-1 (HO-1), also called heat shock protein (HSP)32, which provides robustness to the organism against oxidative damage and plays a vital role in the regulation of cell proliferation, differentiation, oxidant/antioxidant systems, and apoptosis [59]. HIF-1α is induced in response to hypoxia. Ironically, in HBOT where hyperoxia instead of hypoxia is produced, HIF-1α is also induced because of the rapid fall of tissue oxygen levels after the hyperoxic state, i.e., mimicking hypoxia. While chronic hypoxia stimulates only HIF-1α, intermittent hypoxia induces both HIF-1α and Nrf2 [60]. HIF-1α normally downregulates HO-1 induction, but in Nrf2 over-expression, the inhibitory effect of HIF-1α is reversed, contributing to [the HO-1-mediated action [61]. In accordance, the cycling of hyperoxia-normoxia-hyperoxia between HBOT sessions can be placed in the context of normoxia-hypoxia-normoxia loops, therefore simulating intermittent hypoxia. As a result, HBOT stimulates both HIF-1α and Nrf2 [17]. This explains in part the convergence of intermittent hypoxia and HBOT. Mitochondria act as an oxygen sensor by generating ROS signals through the electron transport chain in hypoxic conditions [62]. Following HBOT treatment, humanin expression (a neuroprotective mitochondrion-derived peptide in humans) was increased in vascular dementia patients [63]. Recent studies have also suggested that the increased resiliency of neurons exposed to HBOT is a result of the transfer of mitochondria from astrocytes to neurons [64].
Effect of HBOT on apoptosis and neuroprotection
HBOT has been found to reduce hippocampal p38 mitogen-activated protein kinase (MAPK) phosphorylation which led to improvement in cognition and reduction in hippocampal damage [48]. Individually and in combination with Gingko Biloba extract, HBOT reduced Bax expression and the activity of caspase-9/3 leading to a reduction in apoptotic rate in Aβ25-35-induced toxicity in rats [46]. In another study, HBOT pre-conditioning induced tolerance to cerebral ischemia mediated via an increase in SIRT1 with an associated increase in B-cell lymphoma 2 Bcl-2) expression and reduction in cleaved caspase 3 [65]. These corroborate the neuroprotection and anti-apoptotic effects of HBOT.
Effect of HBOT on microcirculation and neurogenesis
HBOT exposure has been observed to have a plethora of effects on the cerebrovasculature of the brain [30], including improvement of blood–brain barrier permeability [66], angiogenesis [31], and edema reduction [30]. HBOT, in addition to providing increased access of oxygen to tissues, enhances the formation of blood vessels via activation of transcription factors such as vascular endothelial growth factor as well as neuronal stem cell proliferation [67].
Effect of HBOT on epigenetics
It has been found that, after exposure of human microvascular endothelial cells (HMEC-1) to HBOT or 24 h later, 8101 genes are significantly regulated [68]. This includes both up- and downregulation of gene expression with increased expression observed in antioxidant response pathways. Hachmo et al. also reported that exposure to HBOT led to a lengthening of telomeres and a reduction in cellular senescence [69]. Shortening of telomeres and increased cellular senescence are two major hallmarks of the aging process at the cellular level [69]. What these data suggest is the capacity of HBOT to exert some influence at the genetic level, probably through epigenetic modifications. Recent evidence suggests dysregulation of epigenetic mechanisms such as DNA methylation, and histone post-translational modifications are implicated in NDDs [70]. Rats exposed to long-term-intermittent hypoxia exhibited increased DNA methylation and suppression of several antioxidant enzymes [71]. Also, histone demethylases (chromatin regulators), such as KDM6A and KDM5A, are oxygen sensors that are inactivated by chronic hypoxia [72, 73]. Based on these studies and the fact that the removal of methyl from lysine and DNA requires oxygen, we anticipate that one of the major roles of HBOT will be through epigenetic modification. In fact, the pain-relieving effect of HBOT in neuropathic pain is believed to be mediated in part through down-regulation of DNA methyltransferase 3a (DNMT3a) mRNA and protein expression which is an enzyme that plays a significant role in epigenetic modification [74]. This area still remains an unchartered territory and further exploration could hold the key to neurodegenerative diseases while answering the questions between the genetic predisposition of individuals to NDDs and the interaction of environmental influences.
Conclusions
The use of HBOT has come a long way. Its availability, reliability, and safety have stood the test of time [12, 17]. While the therapy has been used as off label treatment for NDDs and has been somewhat studied, there is a need for rigorous studies to standardize the practice of HBOT for NDDs. More studies are needed to determine how often a patient should receive treatment, and how long-lasting are the beneficial effects to provide better recommendations on HBO therapy. The strength of HBOT as a therapy relies on the multiple pathways it seems to affect leading to functional improvements. The studies of the crucial mechanisms that lead to the beneficial effects of HBOT need to be done to identify therapeutics in case chambers are not available, or simply because the treatment itself is rather inconvenient. Interestingly, there have been some reported sex differences in using HBOT as an intervention [75, 76]. This coupled with the prevalence or vulnerability of one sex in relation to another in neurodegenerative diseases [77, 78] should warrant the expansion of future studies to include sex and possibly race to determine how these factors may impact the effect of HBOT and if epigenetics plays a major role. Simply said, more work on the potential of HBOT as a therapy for NDDs needs to be funded and completed.
References
Kovacs GG. Molecular pathology of neurodegenerative diseases: principles and practice. J Clin Pathol. 2019;72(11):725–35.
Dugger BN, Dickson DW. Pathology of neurodegenerative diseases. Cold Spring Harb Perspect Biol. 2017;9(7):a028035.
Gammon K. Neurodegenerative disease: brain windfall. Nature. 2014;515(7526):299–300.
Miller E, et al. Potential of redox therapies in neurodegenerative disorders. Frontiers in Bioscience-Elite. 2017;9(2):214–34.
Shah J. Hyperbaric oxygen therapy. J Am Col Certif Wound Spec. 2010;2(1):9–13.
Kudchodkar B, et al. Hyperbaric oxygen treatment attenuates the pro-inflammatory and immune responses in apolipoprotein E knockout mice. Clin Immunol. 2008;128(3):435–41.
Huang L, Obenaus A. Hyperbaric oxygen therapy for traumatic brain injury. Med Gas Res. 2011;1(1):21.
Huang L, et al. Neuroprotective effect of hyperbaric oxygen therapy in a juvenile rat model of repetitive mild traumatic brain injury. Med Gas Res. 2016;6(4):187–93.
Shapira R, et al. Hyperbaric oxygen therapy ameliorates pathophysiology of 3xTg-AD mouse model by attenuating neuroinflammation. Neurobiol Aging. 2018;62:105–19.
Hadanny A, Efrati S. The hyperoxic-hypoxic paradox. Biomolecules. 2020;10(6):958.
Waypa GB, Smith KA, Schumacker PT. O2 sensing, mitochondria and ROS signaling: the fog is lifting. Mol Aspects Med. 2016;47:76–89.
Simsek K, et al. Evaluation of the oxidative effect of long-term repetitive hyperbaric oxygen exposures on different brain regions of rats. Sci World J. 2012;2012:849183.
Hajhosseini B, et al. Hyperbaric oxygen therapy: descriptive review of the technology and current application in chronic wounds. Plast Reconstr Surg Glob Open. 2020;8(9):e3136.
Thom SR. Oxidative stress is fundamental to hyperbaric oxygen therapy. J Appl Physiol. 2009;106(3):988–95.
Jain, K.K., The history of hyperbaric medicine. Textbook of hyperbaric medicine, 2017: 3–9
Edwards ML. Hyperbaric oxygen therapy. Part 1: history and principles. J Vet Emerg Crit Care (San Antonio). 2010;20(3):284–8.
Simsek K, Sadir S, Oter S. The relation of hyperbaric oxygen with oxidative stress-reactive molecules in action. Oxid Antioxid Med Sci. 2015;4(1):17–22.
Cannellotto M, et al. Hyperbaric oxygen as an adjuvant treatment for patients with COVID-19 severe hypoxaemia: a randomised controlled trial. Emerg Med J. 2022;39(2):88–93.
Levina O, et al. The safety of hyperbaric oxygen therapy in the treatment of COVID-19. Russ Sklifosovsky “J Emerg Med Care.” 2020;9(3):314–20.
Leach RM, Rees PJ, Wilmshurst P. Hyperbaric oxygen therapy. BMJ. 1998;317(7166):1140–3.
Somaa F. A review of the application of hyperbaric oxygen therapy in Alzheimer’s Disease. J Alzheimers Dis. 2021;81(4):1361–7.
Bhatia D, et al. Hypoxia and its emerging therapeutics in neurodegenerative, inflammatory and renal diseases. Hypoxia Hum Dis. 2017;21:404–43.
Zhang Z, et al. Hypoxia inducible factor-1 as a target for neurodegenerative diseases. Curr Med Chem. 2011;18(28):4335–43.
Altieri M, et al. Delayed poststroke dementia: a 4-year follow-up study. Neurol. 2004;62(12):2193–7.
Honig LS, Kukull W, Mayeux R. Atherosclerosis and AD: analysis of data from the US National Alzheimer’s Coordinating Center. Neurol. 2005;64(3):494–500.
Chao LL, et al. ASL perfusion MRI predicts cognitive decline and conversion from MCI to dementia. Alzheimer Dis Assoc Disord. 2010;24(1):19–27.
Chen JJ, Rosas HD, Salat DH. Age-associated reductions in cerebral blood flow are independent from regional atrophy. Neuroimage. 2011;55(2):468–78.
Roher AE, et al. Cerebral blood flow in Alzheimer’s disease. Vasc Health Risk Manag. 2012;8:599–611.
Zhang X, Le W. Pathological role of hypoxia in Alzheimer’s disease. Exp Neurol. 2010;223(2):299–303.
Balasubramanian P, et al. Integrative role of hyperbaric oxygen therapy on healthspan, age-related vascular cognitive impairment, and dementia. Front Aging. 2021;2:678543.
Gottfried I, Schottlender N, Ashery U. Hyperbaric oxygen treatment-from mechanisms to cognitive improvement. Biomolecules. 2021;11(10):1520.
Hou Y, et al. Ageing as a risk factor for neurodegenerative disease. Nat Rev Neurol. 2019;15(10):565–81.
Jacobs EA, et al. Hyperoxygenation effect on cognitive functioning in the aged. N Engl J Med. 1969;281(14):753–7.
Hadanny A, et al. Cognitive enhancement of healthy older adults using hyperbaric oxygen: a randomized controlled trial. Aging (Albany NY). 2020;12(13):13740–61.
Shapira R, et al. Hyperbaric oxygen therapy alleviates vascular dysfunction and amyloid burden in an Alzheimer’s disease mouse model and in elderly patients. Aging (Albany NY). 2021;13(17):20935–61.
Shwe T, et al. Hyperbaric oxygen therapy restores cognitive function and hippocampal pathologies in both aging and aging-obese rats. Mech Ageing Dev. 2021;195:111465.
Chen C, et al. Hyperbaric oxygen prevents cognitive impairments in mice induced by D-galactose by improving cholinergic and anti-apoptotic functions. Neurochem Res. 2017;42(4):1240–53.
Chen X, et al. Protective effect of hyperbaric oxygen on cognitive impairment induced by D-galactose in mice. Neurochem Res. 2016;41(11):3032–41.
Boussi-Gross R, et al. Hyperbaric oxygen therapy can improve post concussion syndrome years after mild traumatic brain injury-randomized prospective trial. PLoS ONE. 2013;8(11):e79995.
Boussi-Gross R, et al. Improvement of memory impairments in poststroke patients by hyperbaric oxygen therapy. Neuropsychol. 2015;29(4):610–21.
Harch PG, Fogarty EF. Hyperbaric oxygen therapy for Alzheimer’s dementia with positron emission tomography imaging: a case report. Med Gas Res. 2018;8(4):181.
Chen J, et al. Hyperbaric oxygen ameliorates cognitive impairment in patients with Alzheimer’s disease and amnestic mild cognitive impairment. Alzheimers Dement (N Y). 2020;6(1):e12030.
Xu JJ, et al. Hyperbaric oxygen treatment for Parkinson’s disease with severe depression and anxiety: a case report. Med (Baltimore). 2018;97(9):e0029.
Steele J, et al. A Phase I safety study of hyperbaric oxygen therapy for amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord. 2004;5(4):250–4.
Zhang LD, et al. Hyperbaric oxygen and ginkgo biloba extract ameliorate cognitive and memory impairment via nuclear factor kappa-B pathway in rat model of Alzheimer’s disease. Chin Med J (Engl). 2015;128(22):3088–93.
Tian X, et al. The protective effect of hyperbaric oxygen and Ginkgo biloba extract on Aβ25–35-induced oxidative stress and neuronal apoptosis in rats. Behav Brain Res. 2013;242:1–8.
Tian X, et al. Hyperbaric oxygen and Ginkgo Biloba extract inhibit Aβ25-35-induced toxicity and oxidative stress in vivo: a potential role in Alzheimer’s disease. Int J Neurosci. 2012;122(10):563–9.
Zhao B, et al. Hyperbaric oxygen pretreatment improves cognition and reduces hippocampal damage via p38 mitogen-activated protein kinase in a rat model. Yonsei Med J. 2017;58(1):131–8.
Pan X, et al. Neuroprotective effect of combined therapy with hyperbaric oxygen and madopar on 6-hydroxydopamine-induced Parkinson’s disease in rats. Neurosci Lett. 2015;600:220–5.
Hsu HT, et al. Hyperbaric oxygen therapy improves Parkinson’s disease by promoting mitochondrial biogenesis via the SIRT-1/PGC-1α pathway. Biomolecules. 2022;12(5):661.
Kusuda Y, et al. Mild hyperbaric oxygen inhibits the decrease of dopaminergic neurons in the substantia nigra of mice with MPTP-induced Parkinson’s disease. Neurosci Res. 2018;132:58–62.
Banou E. Hyperbaric oxygen therapy effect on “Kinesia Paradoxa” brain circuits. Adv Exp Med Biol. 2021;1339:139–46.
Dave K, et al. Hyperbaric oxygen therapy protects against mitochondrial dysfunction and delays onset of motor neuron disease in Wobbler mice. Neurosci. 2003;120(1):113–20.
Jukic I, et al. Mechanisms of HBO-induced vascular functional changes in diabetic animal models. In: Drenjančević I, editor., et al., Hyperbaric Oxygen Treatment in Research andClinical Practice. IntechOpen: Rijeka, Croatia; 2018. p. 87–108.
Thom SR. Hyperbaric oxygen–its mechanisms and efficacy. Plast Reconstr Surg. 2011;127(Suppl 1):131S.
Dröge W. Free radicals in the physiological control of cell function. Physiol Rev. 2002;82(1):47–95.
Forman HJ, Torres M. Reactive oxygen species and cell signaling: respiratory burst in macrophage signaling. Am J Respir Crit Care Med. 2002;166(1):S4–8.
Hink J, Jansen E. Are superoxide and/or hydrogen peroxide responsible for some of the beneficial effects of hyperbaric oxygen therapy? Med Hypotheses. 2001;57(6):764–9.
Grochot-Przeczek A, Dulak J, Jozkowicz A. Haem oxygenase-1: non-canonical roles in physiology and pathology. Clin Sci. 2012;122(3):93–103.
Malec V, et al. HIF-1α signaling is augmented during intermittent hypoxia by induction of the Nrf2 pathway in NOX1-expressing adenocarcinoma A549 cells. Free Radical Biol Med. 2010;48(12):1626–35.
Loboda A, et al. HIF-1 induction attenuates Nrf2-dependent IL-8 expression in human endothelial cells. Antioxid Redox Signal. 2009;11(7):1501–17.
Hadanny A, Efrati S. The hyperoxic-hypoxic paradox Biomolecules. 2020;10(6):958.
Xu Y, et al. Protective effect of hyperbaric oxygen therapy on cognitive function in patients with vascular dementia. Cell Transplant. 2019;28(8):1071–5.
Lippert T, Borlongan CV. Prophylactic treatment of hyperbaric oxygen treatment mitigates inflammatory response via mitochondria transfer. CNS Neurosci Ther. 2019;25(8):815–23.
Yan W, et al. SirT1 mediates hyperbaric oxygen preconditioning-induced ischemic tolerance in rat brain. J Cereb Blood Flow Metab. 2013;33(3):396–406.
Li HZ, et al. Effect of hyperbaric oxygen on the permeability of the blood-brain barrier in rats with global cerebral ischemia/reperfusion injury. Biomed Pharmacother. 2018;108:1725–30.
Yang YJ, et al. Hyperbaric oxygen induces endogenous neural stem cells to proliferate and differentiate in hypoxic-ischemic brain damage in neonatal rats. Undersea Hyperb Med. 2008;35(2):113–29.
Godman CA, et al. Hyperbaric oxygen induces a cytoprotective and angiogenic response in human microvascular endothelial cells. Cell Stress Chaperones. 2010;15(4):431–42.
Hachmo Y, et al. Hyperbaric oxygen therapy increases telomere length and decreases immunosenescence in isolated blood cells: a prospective trial. Aging (Albany NY). 2020;12(22):22445.
Hwang J-Y, Aromolaran KA, Zukin RS. The emerging field of epigenetics in neurodegeneration and neuroprotection. Nat Rev Neurosci. 2017;18(6):347–61.
Nanduri J, Semenza GL, Prabhakar NR. Epigenetic changes by DNA methylation in chronic and intermittent hypoxia. Am J Physiol-Lung Cell Mol Physiol. 2017;313(6):L1096–100.
Chakraborty AA, et al. Histone demethylase KDM6A directly senses oxygen to control chromatin and cell fate. Sci. 2019;363(6432):1217–22.
Batie M, et al. Hypoxia induces rapid changes to histone methylation and reprograms chromatin. Sci. 2019;363(6432):1222–6.
Liu K, Wu H, Gao R, Han G. DNA methylation may be involved in the analgesic effect of hyperbaric oxygen via regulating FUNDC1. Pain Res Manag. 2020;2020:1528362. https://doi.org/10.1155/2020/1528362
Brewer A, et al. (308) Investigation of the effect of sex on hyperbaric oxygen (HBO2)-induced antinociception in a rat model of neuropathic pain. J Pain. 2016;17(4):S53.
Huang C-C, et al. Effects of hyperbaric oxygen therapy on acute myocardial infarction following carbon monoxide poisoning. Cardiovasc Toxicol. 2020;20(3):291–300.
Pike CJ. Sex and the development of Alzheimer’s disease. J Neurosci Res. 2017;95(1–2):671–80.
Gillies GE, et al. Sex differences in Parkinson’s disease. Front Neuroendocrinol. 2014;35(3):370–84.
Funding
BvB Foundation Dallas; Lowdon Family Foundation; Office of Vice President for Research and Innovation, the Institute for Healthy Aging, and National Institutes of Health/National Institute on Aging (T32 AG020494); GSBS seed grant; Grant in Aid of Research from the National Academy of Sciences, administered by Sigma Xi, The Scientific Research Society.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Mensah-Kane, P., Sumien, N. The potential of hyperbaric oxygen as a therapy for neurodegenerative diseases. GeroScience 45, 747–756 (2023). https://doi.org/10.1007/s11357-022-00707-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11357-022-00707-z