
Abstract
Products used in daily life can contain chemicals such as parabens, benzophenones, triclosan, and triclocarban that have potential endocrine-disrupting effects. Little is known about the temporal trends of exposure levels to some of these chemicals in Japan. Our study assessed the intake and risk associated with exposure to commonly used chemicals. We measured the concentrations of five parabens, four benzophenones, and triclosan and triclocarban in 133 single spot urine samples. The urine samples were collected in 1993, 2000, 2003, 2009, 2011, and 2016 from healthy female residents in Kyoto, Japan. With the exception of methylparaben, ethylparaben, and butylparaben, there were no significant fluctuations in the concentrations of target chemicals over the study period; however, methylparaben, ethylparaben, and butylparaben showed temporal changes in concentrations. Methylparaben concentrations peaked in 2003 with a median value of 309 μg/g creatinine, ethylparaben concentrations peaked in 1993 with a median value of 17.3 μg/g creatinine, and butylparaben showed a decline, with the median values becoming non-detectable in 2009 and 2016. We calculated estimated daily intakes and hazard quotients for each chemical. In the analysis of total samples, 2.3% (3 samples) for butylparaben and 0.8% (1 sample) for propylparaben were found to surpass a hazard quotient of 1. Overall, 3% (n = 4) of the study participants exceeded a hazard index of 1. The potential health risks associated with exposure to butylparaben and propylparaben emphasize the need for further monitoring and research.
Graphical Abstract

Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Industrialization has advanced rapidly in recent decades, leading to increased exposure to industrial chemicals and by-products from the environment in daily life (Ambade et al. 2020, 2023; Patidar et al. 2023; Sankar et al. 2023; Sethi, et al. 2023). Parabens as preservatives, benzophenones as UV filters, and triclosan and triclocarban as antimicrobial agents are all chemicals that have been widely utilized in everyday products for an extended period. Consequently, people can easily come into contact with these substances through the use of such products. It has been suggested that these chemicals may have endocrine-disrupting effects (Wei et al. 2021; Mao et al. 2022; Gavrila et al. 2023; Milanović et al. 2023). Exogenous chemicals with endocrine-acting properties may mimic, block, or interfere with hormone action and exposure to them can cause hazards to human health (Yilmaz et al. 2020). These chemicals are ubiquitously present in both environmental settings and biological samples due to their extensive use as additives. They have been identified in various matrices, including environmental samples like indoor dust and surface water, as well as in human fluids such as urine, placenta, and breast milk (Wei et al. 2021; Gavrila et al. 2023; Milanović et al. 2023). Given the widespread occurrence of these potential endocrine-disrupting chemicals, it is crucial to conduct surveillance measures, including monitoring exposure levels and performing risk assessments, to prevent the potential hazards that may arise from exposure.
Parabens are used as preservatives and antiseptics in personal care products, pharmaceuticals, and food products since the 1920s (Soni et al. 2005; Hong et al. 2021). Their broad application has let to environmental detection and human exposure through dermal and oral routes (Wei et al. 2021). Increased use of lotions, sunscreens, and cosmetics correlates with higher urinary paraben levels (Dodson et al. 2020). Past studies have reported that some parabens exhibit estrogenic and antiandrogenic effects, potentially impacting sperm quality and testosterone levels in animal models (Fisher et al. 1999; Oishi 2001; Oishi 2002; Guerra et al. 2017; Pollock et al. 2017; Nowak et al. 2018). Epidemiological studies linked paraben exposure to metabolic diseases (Li et al. 2018; Kim and Chevrier 2020; Wei et al. 2021). In 2014, the European Union limited the use of propylparaben (PrP) and butylparaben (BuP) in cosmetics to 0.14% (EC 2014a). It also banned iso-PrP, iso-BuP, pentylparaben, and benzylparaben (BzP) in cosmetics (EC 2014b).
Benzophenones are a group of organic compounds, used as a UV filter in sunscreens and cosmetics. They can strongly absorb UV radiation, especially UV-A (320–400 nm) and UV-B (290–320 nm) radiation (Song et al. 2020; Mao et al. 2022). They are also used to coat the surface of plastic products to prevent photodegradation of polymers, such as food packaging materials. The primary route of exposure to benzophenones is by sunscreens and other consumer products on the skin. Among benzophenones, present studies indicate that benzophenone-1 (BP-1) and benzophenone-3 (BP-3) are the most likely to be detected in human biological samples (Mao et al. 2022). BP-1 is also the major metabolite of BP-3 in humans (Wang and Kannan 2013; Kim and Choi 2014). Some benzophenones have been found to have potential estrogenic and antiandrogenic effects in vitro and in vivo (Wang et al. 2016; Mao et al. 2022; Yao et al. 2024). Moreover, epidemiological studies correlated higher BP-3 exposure to lower thyroid hormone levels (Mustieles, et al. 2023). Currently in Japan, the use of benzophenone in products is regulated by the Ministry of Health, Labour, and Welfare of Japan, which allows up to 5% BP-3 for cosmetic use (Ministry of Health of Japan 2000). The U.S. Food and Drug Administration (FDA) allows up to 6% BP-3 in commercial sunscreen products (FDA 2017).
Triclosan and triclocarban have been used in soaps and detergents as antimicrobial agents. Triclosan and triclocarban have also recently been called into question for their endocrine-disrupting effects (Yueh and Tukey 2016; Zhang and Lu 2023). For instance, triclosan and triclocarban has been reported to be estrogenic, and can cause decrease in thyroid hormones in vitro and in vivo (Dodson et al. 2020; Iacopetta et al. 2021). Epidemiological studies also linked triclosan and triclocarban with various adverse outcomes in human, such as reproductive and developmental defects (Weatherly and Gosse 2017; Zhang and Lu 2023). In 2016, the FDA announced that selling antibacterial soaps containing triclosan and triclocarban must stop within a year, on the grounds that their effectiveness and safety were not guaranteed (FDA 2016). In Japan, the Ministry of Health, Labour and Welfare and a coalition of companies promoted a switch to products that do not contain these ingredients (Ministry of Health, Labour and Welfare of Japan 2016).
Despite that research has provided evidence on the potential toxicity, safety data on long-term exposure to some of these chemicals regarding human health remain limited (Zhang and Lu 2023; Yao et al. 2024). Consequently, continuous biomonitoring and health risk assessment on the exposure level to these chemicals is necessary. Several studies have observed long-term temporal changes in the exposure level to parabens, BP-3, and triclosan over the last decades in Europe, the United States and Canada (Han et al. 2016; Moos et al. 2017; Jiang et al. 2023). However, those targeting the East Asian region are rare.
This study aimed to assess trends in the intake of the abovementioned chemicals, parabens, benzophenone, triclosan and triclocarban, and the risks associated with exposure to them, using urine samples collected between 1993 and 2016.
Materials and methods
Study subjects
A study protocol was reviewed and approved by the Kyoto University Graduate School and Faculty of Medicine, Ethics Committee (approval number R1478, last approved date: May 31, 2022). Informed consents were given either verbally (before 2000) or in writing before participation of the participants.
The samples analyzed were collected from healthy female study participants living in and around Kyoto City, Japan. They were recruited during their participation in a cross-sectional healthcare checkup program in the years 1993, 2000, 2003, 2009, 2011, and 2016. The sampling years corresponded to the specific years the program was implemented. Due to the availability of participants, the individuals in the study were not the same across each sampling year, and the sample exclusively included women. Each participant was required to collect their first morning urine sample in a paper cup, then transfer a sample to a polypropylene tube and store in a home refrigerator until the sample was transported to the health checkup facilities. The samples were kept at − 30 °C in the Kyoto University Human Specimen Bank (Koizumi et al. 2009).
Determination of target analytes in urine samples
A total of 11 compounds were assessed in the study, including methylparaben (MeP), ethylparaben (EtP), BuP, PrP, benzylparaben (BzP), BP-1, benzophenone-2, -4 and -8 (BP-2, BP-4, and BP-8), triclosan, and triclocarban. These compounds were acquired from the Cambridge Isotope Laboratory in Andover, MA, U.S..
The method used for measuring the target analytes is briefly summarized in the supplementary material. Detailed procedures have been previously described (Mok et al. 2021; Lyu et al. 2023). The LODs and results of method validation are shown in Table S2.
Calculation of daily intake
In analyzing the data, the urinary concentrations of target analytes were corrected with urinary creatinine concentrations to account for the urine dilution effect of single spot samples. The estimated value of creatinine excretion per day (PRCr) was calculated by the following equation (Tanaka et al. 2002):
Since the values of body weight and height were unknown for the subjects in 2000 and 2003, the average values of women from the same age group in the national nutrition survey of the same year were used in the calculations (Ministry of Health, Labour and Welfare of Japan 2001, 2005).
The daily excretion of each compound was calculated by the following equation:
The creatinine ratio (CR) of a target analyte was determined by dividing the urinary concentration (μg/L) by the urinary creatinine concentration (g/L).
The daily intake (DI) of each compound was estimated based on the calculated daily excretion using the following equation (EPA 1986):
Fue is the urinary excretion factor. The Fue for each compound and the references are presented in Table S3.
Risk assessment
The hazard quotient (HQ) was calculated by dividing DI by a dose of no concern [e.g., the reference dose (RfD) or acceptable daily intake (ADI)]. Hazard index (HI) is defined as the sum of HQs (Moos et al. 2017). HIs were calculated for benzophenones (BP-1 and BP-2), parabens (MeP, EtP, PrP, and BuP), and the sum of triclosan and triclocarban. HQ or HI values greater than 1 indicates that the exposure exceeds an acceptable amount. Reference values of no concern used for determining HQ are presented in Table S3.
Data analysis
For urinary concentration, the non-detected values were set to 1/2 of the LODs. The urinary concentrations were adjusted using creatinine concentrations to reduce the effects of variation of analyte concentrations in single spot urine samples. Data were log-transformed in the analysis. JMP Pro 16 was used for statistical analyses. One-way analysis of variance (ANOVA) and Tukey’s honest significant differences test were used to investigate the differences in means of concentrations between each sampling year. Partial correlation coefficients were calculated to examine the changes in urinary concentrations of the chemicals across the years, in which age was set as a control variable. Pearson correlation coefficients were calculated between the chemicals. Two-tailed p-values less than 0.05 were considered statistically significant. A principal component analysis (PCA) was employed to identify potential variances in target compounds through a correlation matrix approach. For the analysis, eigenvectors were utilized when eigenvalues exceeded 1. Additionally, varimax rotation was applied to these eigenvectors to enhance interpretability.
Results and discussion
This study used a total of 133 urine samples collected from different participants each year: n = 10 in 1993; n = 25 in 2000 and 2003; n = 26 in 2009; n = 22 in 2011; and n = 25 in 2016. Table 1 shows demographic data for the subjects. The number of subjects in each year and participants characteristics are presented in Table 1.
Only MeP had a detection frequency of 100%; the detection frequencies of BP-4, BP-8, and BzP were extremely low (< 10% in each year). Tables S4 and S5 summarize the urinary concentrations of chemicals examined and the creatinine-corrected values. Table S4 also shows the detection frequency of each chemical substance for each year. BP-4, BP-8, and BzP were excluded from the following data analysis because of the low detection frequencies.
Temporal trends of exposure of target analytes in this study
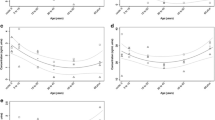
The distributions of urinary concentrations of all analytes are shown in Tables S4 and S5. Except for MeP, EtP, and BuP, there were no significant differences in the concentration of target chemicals from year to year (Table S5). Figure 1 shows the temporal trends in creatinine-adjusted urinary concentrations of MeP, EtP, and BuP. The exposure levels of MeP and EtP both demonstrated a minimal descending trend over the study period, with correlation coefficients of r = -0.235 and -0.225 and p-values of 0.007 and 0.009, respectively (Table S5). The urinary concentrations of MeP were highest in 2003 (median 309 µg/g), while median levels ranged from 73.2 to 189 µg/g in other years. The median MeP concentration declined 3.7-fold between 2003 and 2016, resulting in the overall downward trend observed (p = 0.040, Table S6). For EtP, the exposure levels showed a fluctuation during the study period. The urinary concentrations were lowest in 2009 (median 2.76 µg/g) and highest in 1993 (median 17.3 µg/g), with a significant difference observed between these two years (p = 0.023, Table S6). Median EtP levels in other years remained relatively consistent, ranging from 6.06 to 11.3 µg/g. BuP concentrations were lowest in 2016, with significant differences noted when compared to 1993, 2000, 2003, and 2011 (p = 0.001, 0.008, 0.003, and 0.009, respectively, Table S6). Median BuP concentrations ranged from 3.49 to 8.93 µg/g during 1993–2003 and were measured at 2.52 µg/g in 2011. However, the medians were “not detectable” in 2009 and 2016, indicating a slight decrease in BuP exposure levels over the study period (r = -0.395, p < 0.001, Table S5). Exposure levels of the three parabens all fluctuated during the study period. Given that parabens’ short biological half-lives, exposure level fluctuations could stem from factors such as variations in participants' product use status around the time of sampling.

Urinary concentrations of methylparaben (A), ethylparaben (B), and butylparaben (C) (μg/g creatinine). Values are log10-transformed. The boxes and whiskers indicate the median and interquartile ranges, and the 5th and 95th percentiles, respectively. The smoothing splines (blue curves) are fitted (lambda = 0.1) with 95% confidence intervals
Temporal trends of exposure reported in other countries
Previous studies have investigated temporal changes in these chemicals worldwide, yielding varied results.
For parabens, a German study by Moos et al. (2015) examined 24 h urine samples (total 660) over a period of 17 years (1995–2012). They found that mean urinary paraben concentrations remained unchanged except for MeP, whose median concentration in 2012 was 80.1 μg/g creatinine, more than twice the median of 34.0 μg/g creatinine in 1995. In Boston, MA, U.S., Jiang et al. (2023) investigated 1815 participants, and observed an overall decreasing trend in urinary concentrations of MeP, BuP, and PrP during 2000–2017 (percent change per year − 5.37%, − 14.2%, and − 10.2% for MeP, BuP, and PrP, respectively), with increases during 2000–2007 followed by declines from 2007 to 2017. Additionally, urinary concentrations of EtP showed an 11.8% decrease per year during 2010–2017 in their study. Similarly, in a high-familial risk autism spectrum disorder cohort in California, U.S., the least squares geometric means (LSGMs) decreased during 2007–2014 (percent change per year − 13.0%, − 5.5%, and − 13.3% for MeP, EtP, and PrP, respectively) among pregnant women (Kim et al. 2021). However, given the specific study population, the researchers speculated that this decrease may be attributed to intentional changes in consumer product choices. Similarly, based on biomonitoring data from the Canadian Health Measures Survey, Pollock et al. (2021) observed significant decreasing trends for a 32% decline for MeP and a 36% decline for PrP between the 2012 − 2013 research cycle and the 2016–2017 research cycle.
For triclosan and triclocarban, consistent with our study results, the study by Kim et al. (2021), mentioned above, did not observe any temporal trends in the urinary concentrations of triclosan and triclocarban among cohort participants during 2007–2014 in California. However, other studies presented different results.
Han et al. (2016) studied 10,232 participants from the U.S. National Health and Nutritional Examination Survey (NHANES) during 2003–2012, and observed a decreasing trend of the LSGM of urinary triclosan concentrations since the 2005–2006 research cycle (Han et al. 2016). In particular, the authors noticed a significant decrease in urinary triclosan levels in males in 2011–2012 compared with 2003–2004, while in females, a significant increase in triclosan levels was found in 2005–2010 compared with 2003–2004, with no significant change in 2011–2012. Nevertheless, they found no statistically significant changes in the concentration of urinary triclosan over the entire study period. In contrast, Li et al. (2023) found a reduction in HQ values for triclosan over the 2005–2016 period in U.S. children and adolescents aged 6–19 years participating in NHANES, with an annual percent change in LSGM HQ for triclosan of − 9.2% (Li et al. 2023). Similarly, Jiang et al. (2023) reported triclosan showing a large decreasing trend with a –18.8% change per year during 2010–2017 in Boston, MA, U.S.; Pollock et al. (2021) found a 31% decline for triclosan between the 2009–2011 cycle and the 2014–2015 cycle according to biomonitoring data in Canada.
Correlations of target analytes
Pearson correlations among the analytes in urine samples are shown in Table S7. The values of BP-1 and BP-2 were positively correlated (r = 0.20, p = 0.022). The urinary concentrations of triclosan and triclocarban have a slight positive correlation (r = 0.32, p < 0.001). The paraben concentrations were positively correlated with each other. Among them MeP and PrP were most significantly associated (r = 0.54, p < 0.001). Chemicals from each group were not associated with those from other groups. A PCA was applied to more thoroughly investigate the different sources of exposure. The results revealed three significant factors that contributed 27.8%, 16.5%, and 13.4% to the total variance, respectively, each with an eigenvalue greater than 1.0 (Table S8). These factors corresponded primarily to the three groups of target compounds: parabens, triclosan and triclocarban, and benzophenones, except for EtP (Fig. 2). This result suggested that the exposure of the population to triclosan and triclocarban originated from different sources or through distinct exposure pathways from parabens and benzophenones. However, given that parabens and benzophenones are both used in cosmetics and other personal care products (Wei et al. 2021; Mao et al. 2022), there may be some overlap in the exposure sources or pathways.

Principal component analysis among target compounds through a correlation matrix approach. Dara was based on log-transformed urinary concentrations of each analyte. Eigenvectors were utilized when eigenvalues exceeded 1. Varimax rotation was applied to these eigenvectors
Similarly to our results, numerous studies found strong correlations between parabens (Ma et al. 2013; Asimakopoulos et al. 2014; Moos et al. 2015; Zhang et al. 2020; Wang et al. 2021; Wei et al. 2022). Associations between MeP and PrP concentrations have been detected in personal care products (Guo et al. 2014) and indoor dust (Wang et al. 2021), suggesting a possible co-exposure to both of these chemicals. Furthermore, several studies have found significant correlations among other parabens, such as between MeP and EtP (Shirai et al. 2013; Kang et al. 2016; Wei et al. 2022).
Estimated daily intakes and associated risks
The estimated DIs of each target chemical are shown in Table S9. The prior research, which presented estimated Daily Intakes (DIs) based on urinary concentrations, was summarized in the supplementary tables by each group of target chemicals (Tables S10, S11, and S12). However, these estimates are challenging to compare directly because of the variability in urinary excretion factors, as well as other parameters employed in calculations across different studies. The current study has presented the urinary excretion factors used in previous studies, selecting factors that we believe have the most significant impact on the estimated results (Tables S10, S11 and S12).
The calculated HQs and cumulative HIs for BPs, parabens, and the sum of triclosan and triclocarban are depicted in Table S13. The HQs for BPs, the sum of triclosan and triclocarban, and the sum of MeP and EtP were considerably below 1 in all sampling years. The maximum HQ for the sum of MeP and EtP was 0.031 in 2003. However, unlike the MeP and EtP HQ values, the calculated HQ values for BuP exceeded 1 in 2.3% of the total samples. The highest HQ value for BuP was 7.8 from one sample in 2011. For PrP, only one sample, collected in 2003, had an HQ value higher than 1 among all years.
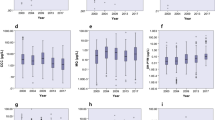
The HIs for BPs, parabens, and the sum of triclosan and triclocarban in each sampling year are presented in Fig. 3. For the HI, BPs had a median value of 0.002 and maximum of 0.09, and the sum of triclosan and triclocarban had a median of 0.004 and maximum of 0.18. The HI of parabens was a median value of 0.06 and 90th percentile of 0.64, but the maximum value was 7.8 from one participant in 2011, who generated the highest HQ value for BuP. Overall, 3% (n = 4) of the 133 samples from participants in our study exceeded the HI of 1. The percentages of HQs and HIs that exceeded 1 for parabens are shown in Table 2.

Boxplots of hazard index (after log10-transformation, log HI) of benzophenones (BPs), parabens, and the sum of triclocarban and triclosan (TCB + TCS). The boxes depict the interquartile ranges and whiskers depict the 5th and 95th percentiles
Several studies have also calculated HQ and HI for the abovementioned chemicals. Yu et al. (2019) reported 15 workers (2.7%, n = 562) with an HQ greater than 1 for PrP between 2013 and 2015 in South China, using the same RfD [0.1 mg/kg body weight (bw)/day] as our study (Yu et al. 2019). Moos et al. (2017) found that 5.2% of study participants (n = 660) had HQs for n-PrP greater than 1 during the period 1995–2012, based on a lower RfD of 0.02 mg/kg bw/day (Moos et al. 2017). It is noteworthy that this dose is five times lower than the RfD of 0.1 mg/kg bw/day used in the current study. Varghese et al. (2022) reported a margin of exposure of PrP less than 10000 (based on 6.5 mg/kg bw/day as the no-observed-adverse-effect level value) in Indian pregnant women (n = 28), suggesting potential health risks (Varghese et al. 2022). None of the abovementioned studies reported HQ values for the sum of MeP and EtP greater than 1 (ADI was 10 mg/kg bw/day) (EFSA 2004).
Contrary to our findings, Moos et al. (2017) did not find any participants with an HQ greater than 1 for BuP (Moos et al. 2017). Certain studies reported that HQ and HI values of parabens (Li et al. 2021; Wei et al. 2022; Xu et al. 2022), triclosan (Li et al. 2021; Wei et al. 2022; Xu et al. 2022), and BPs (Wei et al. 2022; Xu et al. 2022) did not exceed 1 among Chinese general populations in 2018 and 2020, even though two of these three studies (Li et al. 2021; Xu et al. 2022) used RfDs similar to the present study.
Regarding triclosan alone, Jin et al. (2020) reported HQ values lower than 1 among pregnant women in China in 2010 and 2013, using an RfD of 0.047 mg/kg bw/day (Jin et al. 2020). Li et al. (2023) calculated HQs lower than 1 for triclosan in US children and adolescents from 2005–2016 using a tolerable DI of 50 mg/kg bw/day as an RfD. They also noted a descending trend in the LGSM HQ values, as we have discussed in the previous section regarding temporal trends (Li et al. 2023).
Limitations
This study had several limitations. First, the study population consisted exclusively of women living in the same geographic area until 2016, with a maximum of 26 participants in each sampling year. The sample size was particularly limited in 1993, attributable to participant availability and challenges associated with long-term sample storage. Due to the restricted study location, the findings cannot be generalized to other locations. Second, the current study used single spot urine samples for chemical analysis, and the concentration of target chemicals may include large variabilities. Additionally, although both BP-1 and BP-3 were reported to be the most ubiquitous benzophenones in human biological samples (Mao et al. 2022), we only investigated urinary concentrations of BP-1, BP-2, BP-4, and BP-8.
Conclusion
Our research investigated urinary concentrations of multiple endocrine-disrupting chemicals among a female population in Japan from 1993 to 2016. Our findings indicated that exposure to these chemicals within this population remained relatively steady over this two-decade span. The HQs for PrP and BuP, as well as the HI values for parabens, suggest potential health risks associated with paraben exposure among Japanese women. As far as we know, this study is the first in Japan to investigate prolonged temporal variations in exposure to multiple groups of endocrine-disrupting chemicals, along with associated risk assessments. Therefore, continued monitoring and further evaluations are needed, particularly focusing on parabens, due to their potential health implications.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request under the ethical guidelines for medical and biological research involving human subjects in Japan..
References
Ambade B, Sankar TK, Kumar A, Sethi SS (2020) Characterization of PAHs and n-Alkanes in Atmospheric Aerosol of Jamshedpur City, India. J Hazard Toxic Radioact Waste 24:04020003. https://doi.org/10.1061/(ASCE)HZ.2153-5515.0000490
Ambade B, Sethi SS, Chintalacheruvu MR (2023) Distribution, risk assessment, and source apportionment of polycyclic aromatic hydrocarbons (PAHs) using positive matrix factorization (PMF) in urban soils of East India. Environ Geochem Health 45:491–505. https://doi.org/10.1007/s10653-022-01223-x
Asimakopoulos AG, Thomaidis NS, Kannan K (2014) Widespread occurrence of bisphenol A diglycidyl ethers, p-hydroxybenzoic acid esters (parabens), benzophenone type-UV filters, triclosan, and triclocarban in human urine from Athens, Greece. Sci Total Environ 470–471:1243–1249. https://doi.org/10.1016/j.scitotenv.2013.10.089
Dodson RE, Boronow KE, Susmann H, Udesky JO, Rodgers KM, Weller D, Woudneh M, Brody JG, Rudel RA (2020) Consumer behavior and exposure to parabens, bisphenols, triclosan, dichlorophenols, and benzophenone-3: Results from a crowdsourced biomonitoring study. Int J Hyg Environ Health 230:113624. https://doi.org/10.1016/j.ijheh.2020.113624
EC (2014a) Commission Regulation (EU) No 358/2014 amending Annexes II and V to Regulation (EC) No 1223/2009 of the European Parliament and of the Council of 30 November 2009 on cosmetic products. https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=OJ:JOL_2014_107_R_0002&from=EN. Accessed 3 July 2023
EC (2014b) Commission Regulation (EU) No 1004/2014 of 18 September 2014 Amending Annex V to Regulation (EC) No 1223/2009 of the European Parliament and of the Council on Cosmetic Products. http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32014R1004&from=EN. Accessed 3 July 2023
EFSA (2004) Opinion of the scientific panel on food additives, flavourings, processing aids and materials in contact with food on a request from the commission related to parahydroxybenzoates (E214-219). Question number EFAS-Q-2004-063, adopted on 13 July 2004. EFSA J 83:1–26. https://doi.org/10.2903/j.efsa.2004.83
EPA (1986) Guidelines for the health risk assessment of chemical mixtures (Final Report, 1986). Federal Register 51(185):34014–34025. https://www.epa.gov/risk/guidelines-health-risk-assessment-chemical-mixtures. Accessed 3 July 2023
FDA (2016) Safety and Effectiveness of Consumer Antiseptics; Topical Antimicrobial Drug Products for Over-the-Counter Human Use. 21CFR310 https://www.federalregister.gov/documents/2016/09/06/2016-21337/safety-and-effectiveness-of-consumer-antiseptics-topical-antimicrobial-drug-products-for. Accessed 3 July 2023
FDA (2017) Sunscreen Drug Products for Over-the-Counter Human Use. 21CFR352. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/cfrsearch.cfm?cfrpart=352&showfr=1. Accessed 3 July 2023
Fisher JS, Turner KJ, Brown D, Sharpe RM (1999) Effect of neonatal exposure to estrogenic compounds on development of the excurrent ducts of the rat testis through puberty to adulthood. Environ Health Perspect 107:397–405. https://doi.org/10.1289/ehp.99107397
Gavrila AA, Dasteridis IS, Tzimas AA, Chatzimitakos TG, Stalikas CD (2023) Benzophenones in the Environment: Occurrence, Fate and Sample Preparation in the Analysis. Molecules 28:1229. https://doi.org/10.3390/molecules28031229
Guerra MT, Sanabria M, Leite GA, Borges CS, Cucielo MS, Anselmo-Franci JA, Foster WG, Kempinas WG (2017) Maternal exposure to butyl paraben impairs testicular structure and sperm quality on male rats. Environ Toxicol 32:1273–1289. https://doi.org/10.1002/tox.22323
Guo Y, Wang L, Kannan K (2014) Phthalates and parabens in personal care products from China: concentrations and human exposure. Arch Environ Contam Toxicol 66:113–119. https://doi.org/10.1007/s00244-013-9937-x
Han C, Lim YH, Hong YC (2016) Ten-year trends in urinary concentrations of triclosan and benzophenone-3 in the general U.S. population from 2003 to 2012. Environ Pollut 208:803–810. https://doi.org/10.1016/j.envpol.2015.11.002
Hong S, Jeon HL, Lee J, Kim S, Lee C, Lee S, Cho YH, Choi K, Yoo J (2021) Urinary parabens and their potential sources of exposure among Korean children and adolescents: Korean National Environmental Health Survey 2015–2017. Int J Hyg Environ Health 236:113781. https://doi.org/10.1016/j.ijheh.2021.113781
Iacopetta D, Catalano A, Ceramella J, Saturnino C, Salvagno L, Ielo I, Drommi D, Scali E, Plutino MR, Rosace G, Sinicropi MS (2021) The Different Facets of Triclocarban: A Review. Molecules 26. https://doi.org/10.3390/molecules26092811
Jiang VS, Calafat AM, Williams PL, Chavarro JE, Ford JB, Souter I, Hauser R, Mínguez-Alarcón L (2023) Temporal trends in urinary concentrations of phenols, phthalate metabolites and phthalate replacements between 2000 and 2017 in Boston, MA. Sci Total Environ 898:165353. https://doi.org/10.1016/j.scitotenv.2023.165353
Jin C, Yao Q, Zhou Y, Shi R, Gao Y, Wang C, Tian Y (2020) Exposure to triclosan among pregnant women in northern China: urinary concentrations, sociodemographic predictors, and seasonal variability. Environ Sci Pollut Res Int 27:4840–4848. https://doi.org/10.1007/s11356-019-07294-1
Kang HS, Kyung MS, Ko A, Park JH, Hwang MS, Kwon JE, Suh JH, Lee HS, Moon GI, Hong JH, Hwang IG (2016) Urinary concentrations of parabens and their association with demographic factors: A population-based cross-sectional study. Environ Res 146:245–251. https://doi.org/10.1016/j.envres.2015.12.032
Kim J, Chevrier J (2020) Exposure to parabens and prevalence of obesity and metabolic syndrome: An analysis of the Canadian Health Measures Survey. Sci Total Environ 713:135116. https://doi.org/10.1016/j.scitotenv.2019.135116
Kim S, Choi K (2014) Occurrences, toxicities, and ecological risks of benzophenone-3, a common component of organic sunscreen products: a mini-review. Environ Int 70:143–157. https://doi.org/10.1016/j.envint.2014.05.015
Kim K, Shin HM, Busgang SA, Barr DB, Panuwet P, Schmidt RJ, Hertz-Picciotto I, Bennett DH (2021) Temporal Trends of Phenol, Paraben, and Triclocarban Exposure in California Pregnant Women during 2007–2014. Environ Sci Technol 55:11155–11165. https://doi.org/10.1021/acs.est.1c01564
Koizumi A, Harada KH, Inoue K, Hitomi T, Yang HR, Moon CS, Wang P, Hung NN, Watanabe T, Shimbo S, Ikeda M (2009) Past, present, and future of environmental specimen banks. Environ Health Prev Med 14:307–318. https://doi.org/10.1007/s12199-009-0101-1
Li AJ, Xue J, Lin S, Al-Malki AL, Al-Ghamdi MA, Kumosani TA, Kannan K (2018) Urinary concentrations of environmental phenols and their association with type 2 diabetes in a population in Jeddah, Saudi Arabia. Environ Res 166:544–552. https://doi.org/10.1016/j.envres.2018.06.040
Li X, Zhong Y, He W, Huang S, Li Q, Guo C, Ma S, Li G, Yu Y (2021) Co-exposure and health risks of parabens, bisphenols, triclosan, phthalate metabolites and hydroxyl polycyclic aromatic hydrocarbons based on simultaneous detection in urine samples from guangzhou, south China. Environ Pollut 272:115990. https://doi.org/10.1016/j.envpol.2020.115990
Li R, Zhan W, Ren J, Zhang F, Huang X, Ma Y (2023) Temporal trends in risk of bisphenol A, benzophenone-3 and triclosan exposure among U.S. children and adolescents aged 6–19 years: Findings from the National Health and Nutrition Examination Survey 2005–2016. Environ Res 216:114474. https://doi.org/10.1016/j.envres.2022.114474
Lyu Z, Harada KH, Kim S, Fujitani T, Hitomi T, Pan R, Park N, Fujii Y, Kho Y, Choi K (2023) Temporal trends in bisphenol exposures and associated health risk among Japanese women living in the Kyoto area from 1993 to 2016. Chemosphere 316:137867. https://doi.org/10.1016/j.chemosphere.2023.137867
Ma WL, Wang L, Guo Y, Liu LY, Qi H, Zhu NZ, Gao CJ, Li YF, Kannan K (2013) Urinary concentrations of parabens in Chinese young adults: implications for human exposure. Arch Environ Contam Toxicol 65:611–618. https://doi.org/10.1007/s00244-013-9924-2
Mao JF, Li W, Ong CN, He Y, Jong MC, Gin KY (2022) Assessment of human exposure to benzophenone-type UV filters: A review. Environ Int 167:107405. https://doi.org/10.1016/j.envint.2022.107405
Milanović M, Đurić L, Milošević N, Milić N (2023) Comprehensive insight into triclosan-from widespread occurrence to health outcomes. Environ Sci Pollut Res Int 30:25119–25140. https://doi.org/10.1007/s11356-021-17273-0
Ministry of Health of Japan (2000) Ministry of Health and Welfare Notification No.331 of 2000. Standards for Cosmetics. https://www.mhlw.go.jp/file/06-Seisakujouhou-11120000-Iyakushokuhinkyoku/0000032704.pdf. Accessed 3 July 2023
Ministry of Health, Labour and Welfare of Japan (2001) The 2000 National Health and Nutrition Survey. https://www.mhlw.go.jp/toukei/kouhyo/indexkk_14_7.html. Accessed 19 July 2023
Ministry of Health, Labour and Welfare of Japan (2005) The 2003 National Health and Nutrition Survey. https://www.mhlw.go.jp/bunya/kenkou/eiyou-chosa2-01/index.html. Accessed 19 July 2023
Ministry of Health, Labour and Welfare of Japan (2016) Encourages switching to medicated soaps containing triclosan, etc. https://www.mhlw.go.jp/stf/houdou/0000138223.html. Accessed 3 July 2023
Mok S, Jeong Y, Park M, Kim S, Lee I, Park J, Kim S, Choi K, Moon HB (2021) Exposure to phthalates and bisphenol analogues among childbearing-aged women in Korea: Influencing factors and potential health risks. Chemosphere 264:128425. https://doi.org/10.1016/j.chemosphere.2020.128425
Moos RK, Koch HM, Angerer J, Apel P, Schröter-Kermani C, Brüning T, Kolossa-Gehring M (2015) Parabens in 24 h urine samples of the German Environmental Specimen Bank from 1995 to 2012. Int J Hyg Environ Health 218:666–674. https://doi.org/10.1016/j.ijheh.2015.07.005
Moos RK, Apel P, Schröter-Kermani C, Kolossa-Gehring M, Brüning T, Koch HM (2017) Daily intake and hazard index of parabens based upon 24 h urine samples of the German Environmental Specimen Bank from 1995 to 2012. J Expo Sci Environ Epidemiol 27:591–600. https://doi.org/10.1038/jes.2016.65
Mustieles V, Balogh RK, Axelstad M, Montazeri P, Márquez S, Vrijheid M, Draskau MK, Taxvig C, Peinado FM, Berman T, Frederiksen H, Fernández MF, Marie Vinggaard A, Andersson AM (2023) Benzophenone-3: Comprehensive review of the toxicological and human evidence with meta-analysis of human biomonitoring studies. Environ Int 173:107739. https://doi.org/10.1016/j.envint.2023.107739
Nowak K, Ratajczak-Wrona W, Górska M, Jabłońska E (2018) Parabens and their effects on the endocrine system. Mol Cell Endocrinol 474:238–251. https://doi.org/10.1016/j.mce.2018.03.014
Oishi S (2001) Effects of butylparaben on the male reproductive system in rats. Toxicol Ind Health 17:31–39. https://doi.org/10.1191/0748233701th093oa
Oishi S (2002) Effects of propyl paraben on the male reproductive system. Food Chem Toxicol 40:1807–1813. https://doi.org/10.1016/s0278-6915(02)00204-1
Patidar K, Ambade B, Verma SK, Mohammad F (2023) Microplastic contamination in water and sediments of Mahanadi River, India: An assessment of ecological risk along rural-urban area. J Environ Manag 348:119363. https://doi.org/10.1016/j.jenvman.2023.119363
Pollock T, Weaver RE, Ghasemi R, deCatanzaro D (2017) Butyl paraben and propyl paraben modulate bisphenol A and estradiol concentrations in female and male mice. Toxicol Appl Pharmacol 325:18–24. https://doi.org/10.1016/j.taap.2017.04.001
Pollock T, Karthikeyan S, Walker M, Werry K, St-Amand A (2021) Trends in environmental chemical concentrations in the Canadian population: Biomonitoring data from the Canadian Health Measures Survey 2007–2017. Environ Int 155:106678. https://doi.org/10.1016/j.envint.2021.106678
Sankar TK, Kumar A, Mahto DK, Das KC, Narayan P, Fukate M, Awachat P, Padghan D, Mohammad F, Al-Lohedan HA, Soleiman AA, Ambade B (2023) The Health Risk and Source Assessment of Polycyclic Aromatic Hydrocarbons (PAHs) in the Soil of Industrial Cities in India. Toxics 11. https://doi.org/10.3390/toxics11060515
Sethi SS, Ambade B, Mohammad F, Al-Lohedan HA, Soleiman AA (2023) Accumulation and Toxicity of Polycyclic Aromatic Hydrocarbons in Long-Term Soil Irrigated with Treated Wastewater. Sustainability 15:13581. https://doi.org/10.3390/su151813581
Shirai S, Suzuki Y, Yoshinaga J, Shiraishi H, Mizumoto Y (2013) Urinary excretion of parabens in pregnant Japanese women. Reprod Toxicol 35:96–101. https://doi.org/10.1016/j.reprotox.2012.07.004
Song S, He Y, Huang Y, Huang X, Guo Y, Zhu H, Kannan K, Zhang T (2020) Occurrence and transfer of benzophenone-type ultraviolet filters from the pregnant women to fetuses. Sci Total Environ 726:138503. https://doi.org/10.1016/j.scitotenv.2020.138503
Soni MG, Carabin IG, Burdock GA (2005) Safety assessment of esters of p-hydroxybenzoic acid (parabens). Food Chem Toxicol 43:985–1015. https://doi.org/10.1016/j.fct.2005.01.020
Tanaka T, Okamura T, Miura K, Kadowaki T, Ueshima H, Nakagawa H, Hashimoto T (2002) A simple method to estimate populational 24-h urinary sodium and potassium excretion using a casual urine specimen. J Hum Hypertens 16:97–103. https://doi.org/10.1038/sj.jhh.1001307
Varghese B, Jala A, Das P, Borkar RM, Adela R (2022) Estimation of parabens and bisphenols in maternal products and urinary concentrations in Indian pregnant women: daily intake and health risk assessment. Environ Sci Pollut Res Int 29:21642–21655. https://doi.org/10.1007/s11356-021-17298-5
Wang L, Kannan K (2013) Characteristic profiles of benzonphenone-3 and its derivatives in urine of children and adults from the United States and China. Environ Sci Technol 47:12532–12538. https://doi.org/10.1021/es4032908
Wang Y, Li G, Zhu Q, Liao C (2021) Occurrence of parabens, triclosan and triclocarban in paired human urine and indoor dust from two typical cities in China and its implications for human exposure. Sci Total Environ 786:147485. https://doi.org/10.1016/j.scitotenv.2021.147485
Wang J, Pan L, Wu S, Lu L, Xu Y, Zhu Y, Guo M, Zhuang S (2016) Recent Advances on Endocrine Disrupting Effects of UV Filters. Int J Environ Res Public Health 13. https://doi.org/10.3390/ijerph13080782.
Weatherly LM, Gosse JA (2017) Triclosan exposure, transformation, and human health effects. J Toxicol Environ Health-Part B-Crit Rev 20:447–469. https://doi.org/10.1080/10937404.2017.1399306
Wei F, Mortimer M, Cheng H, Sang N, Guo LH (2021) Parabens as chemicals of emerging concern in the environment and humans: A review. Sci Total Environ 778:146150. https://doi.org/10.1016/j.scitotenv.2021.146150
Wei X, Hu Y, Zhu Q, Gao J, Liao C, Jiang G (2022) Co-exposure and health risks of several typical endocrine disrupting chemicals in general population in eastern China. Environ Res 204:112366. https://doi.org/10.1016/j.envres.2021.112366
Xu L, Hu Y, Zhu Q, Liao C, Jiang G (2022) Several typical endocrine-disrupting chemicals in human urine from general population in China: Regional and demographic-related differences in exposure risk. J Hazard Mater 424:127489. https://doi.org/10.1016/j.jhazmat.2021.127489
Yao YN, Wang Y, Zhang H, Gao Y, Zhang T, Kannan K (2024) A review of sources, pathways, and toxic effects of human exposure to benzophenone ultraviolet light filters. Eco Environ Health 3:30–44. https://doi.org/10.1016/j.eehl.2023.10.001
Yilmaz B, Terekeci H, Sandal S, Kelestimur F (2020) Endocrine disrupting chemicals: exposure, effects on human health, mechanism of action, models for testing and strategies for prevention. Rev Endocr Metab Disord 21:127–147. https://doi.org/10.1007/s11154-019-09521-z
Yu Y, Li W, Lu S, Wu S, Wang F, Tse LA, Kang L, Ma S (2019) Urinary parabens in adults from South China: Implications for human exposure and health risks. Ecotoxicol Environ Saf 182:109419. https://doi.org/10.1016/j.ecoenv.2019.109419
Yueh MF, Tukey RH (2016) Triclosan: A Widespread Environmental Toxicant with Many Biological Effects. Annu Rev Pharmacol Toxicol 56:251–272. https://doi.org/10.1146/annurev-pharmtox-010715-103417
Zhang D, Lu S (2023) A holistic review on triclosan and triclocarban exposure: Epidemiological outcomes, antibiotic resistance, and health risk assessment. Sci Total Environ 872:162114. https://doi.org/10.1016/j.scitotenv.2023.162114
Zhang H, Quan Q, Li X, Sun W, Zhu K, Wang X, Sun X, Zhan M, Xu W, Lu L, Fan J, Gao Y (2020) Occurrence of parabens and their metabolites in the paired urine and blood samples from Chinese university students: Implications on human exposure. Environ Res 183:109288. https://doi.org/10.1016/j.envres.2020.109288
Acknowledgements
We thank Charles Allan, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Funding
This study was supported by Grants from the Japan Society for the Promotion of Science (Grant Nos. 23590739, 17H06281 and 120188819). Zhaoqing Lyu received a research fellowship supported by Japan Science and Technology Agency SPRING (Grant No. JPMJSP2110).
Author information
Authors and Affiliations
Contributions
Kouji H. Harada, Younglim Kho and Kyungho Choi contributed to the study conception and design and supervised the study. Material collection was performed by Zhaoqing Lyu, Toshiaki Hitomi, and Yukiko Fujii. Sample preparation and chemical analyses were performed by Sungmin Kim, Nayoun Park, and Younglim Kho. Statistical analysis was performed by Nao Yoshida, and Zhaoqing Lyu. The first draft of the manuscript was written by Nao Yoshida, and Zhaoqing Lyu. All authors reviewed and commented on the first draft. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
A study protocol was reviewed and approved by the Kyoto University Graduate School and Faculty of Medicine, Ethics Committee (approval number R1478, last approved date: May 31, 2022). Informed consents were given either verbally (before 2000) or in writing before participation of the participants.
Consent to publish
Not applicable to this study.
Consent to participate
Informed consents were given either verbally (before 2000) or in writing before participation of the participants.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Responsible Editor: Lotfi Aleya
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yoshida, N., Lyu, Z., Kim, S. et al. Temporal trends in exposure to parabens, benzophenones, triclosan, and triclocarban in adult females in Kyoto, Japan, from 1993 to 2016. Environ Sci Pollut Res 31, 37050–37059 (2024). https://doi.org/10.1007/s11356-024-33627-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-024-33627-w