
Abstract
Objectives To examine the association between having a patient-centered medical home (PCMH) and healthcare expenditures and quality of care for children with special health care needs (CSHCN). Methods We conducted a cross-sectional analysis of 8802 CSHCN using the 2008–2012 Medical Expenditure Panel Survey. A PCMH indicator was constructed from survey responses. Inverse probability treatment weighting was applied to balance the cohort. CSHCN’s annual health care expenditures and quality were analyzed using two-part and logistic models, respectively. Results Covariate-adjusted annual total expenditures were similar between CSHCN with and without a PCMH ($4267 vs. $3957, p = 0.285). CSHCN with a PCMH had higher odds of incurring expenditure (OR 1.66, 95% CI 1.22–2.25)—in particular, office-based services and prescriptions (OR 1.46 and 1.36, 95% CI 1.24–1.72 and 1.17–1.58, respectively)—compared to those without a PCMH, without shifting expenditures. When examined in detail, PCMH was associated with lower odds of accessing office-based mental health services (OR 0.80, 95% CI 0.66–0.96), leading to lower expenditures ($106 vs. $137; p = 0.046). PCMH was associated with higher odds of post-operation and immunization visits (OR 1.23 and 1.22, 95% CI 1.05–1.45 and 1.004–1.48, respectively) without changing expenditures. Parents of CSHCN with a PCMH were more likely to report having the best health care quality (OR 2.33, p < 0.001). Conclusions CSHCN who had a PCMH experienced better health care quality and were more likely to access preventive services, with unchanged expenditures. However, they were less likely to use mental health services in office-based settings. As the effects of PCMH varied across services for CSHCN, more research is warranted.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Significance
Patient-centered medical home (PCMH) was associated with better health care quality and improved access to prescriptions and post-operation office-based services and immunization visits without shifting health care expenditures for children with special health care needs (CSHCN). However, PCMH was also associated with a decreased use of mental health services in office-based setting, suggesting either unmet mental health service needs, or that mental health care needs had been addressed by improved primary care. The effects of PCMH varied across types of health services for CSHCN so more efforts are warranted to investigate the changes, especially for mental health services.
Introduction
Children with special health care needs (CSHCN) have been defined as “children who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition, and who also require health and related services of a type or amount beyond that required by children generally” (McPherson et al. 1998). In the United States, 15.1% of all children (approximately 11.2 million) were identified as CSHCN.Footnote 1 These children were estimated to incur medical expenses three times higher than healthy children and account for 42% of health care expenditures among all US children (Newacheck and Kim 2005).
The concept of the patient-centered medical home (PCMH) has gained popularity as a desirable primary care model since the publication of the Joint Principles of PCMH in 2007 (American Academy of Family Physicians 2008). An ideal PCMH is accessible, family-centered, continuous, comprehensive, coordinated, compassionate, and culturally effective (The Medical Home 2002). Approximately 43% of CSHCN reported receiving care at clinics with medical home features.1 CSHCN who received care from a PCMH had an increased probability of having medical needs met, enjoyed improved health outcomes, and had an increased probability of using preventive care than CSHCN without a PCMH (Cooley et al. 2009; Garcia-Huidobro et al. 2016; Homer et al. 2008; Miller et al. 2013; Strickland et al. 2011).
For health care expenditures, Romaire et al. is one of the key studies that examined the effect of PCMHs for CSHCN using the 2003–2008 Medical Expenditure Panel Survey (MEPS) data (Romaire et al. 2012). They found CSHCN with a PCMH had an increased probability of accessing hospital outpatient and office-based visits, and prescriptions, without significant changes in overall expenditures (Romaire et al. 2012). Han et al. investigated the annual health care expenditure and quality among all children, rather than CSHCN, and a longer time horizon (2004–2012) (Han et al. 2017). For all children, no significant effects of PCMH on health care expenditures were found, but a significant increase in parent-reported health care quality resulted from the presence of a PCMH (Han et al. 2017).
As the PCMH model becomes more prevalent and matures, it is important to update this body of literature. This study aimed to use more recent data to examine the relationship between having a PCMH on annual health care expenditures and health care quality for CSHCN, the population for whom the model was originally designed. We investigated the association between having a PCMH and annual health care expenditures and quality of care. In addition, we add to the understanding of how having a PCMH affects office-based care.
Methods
Data Source
We used the Agency for Healthcare Research and Quality MEPS Household Component 2008–2012 full-year and event data, an in-person interview survey of US non-institutionalized families and individuals.Footnote 2 These public-use files include data on individual demographics, health conditions, healthcare expenditures and utilization, insurance coverage, and health status. MEPS also collected information surrounding individuals’ perception of health care quality using Consumer Assessment of Healthcare Providers and Systems (CAHPS), a survey instrument measuring consumer-perceived healthcare quality during the past year (MEPS HC-155: 2012 Full Year Consolidated Data File 2014). Using weights accounting for survey design, we were able to obtain national estimates from a representative non-institutionalized population using MEPS (see footnote 2). The Institutional Review Board of the University of Southern California determined this study was exempt from review.
Study Population
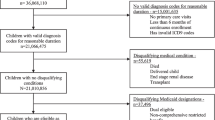
The study sample includes children under 18 years of age in 2008–2012 and identified as CSHCN by the responses to the CSHCN Screener (n = 8802), representing 14.6 million CSHCN in the US. The screener is a non-condition-specific, health consequence-based tool for CSHCN identification in several national surveys, including MEPS (The Children with Special Health Care Needs (CSHCN) Screener 1998). The screener consists of five items that assesses: (1) need or use of prescription medicine; (2) need or use of more medical care, mental health care, or educational services than children of the same age; (3) being limited or unable to do the things most children of the same age can do; (4) need or receipt of physical, occupational, or speech therapy; and (5) have emotional, developmental, or behavioral problems that need or use treatment or counseling (The Children with Special Health Care Needs (CSHCN) Screener 1998). Even though the screener is the gold standard for operationalizing the Maternal and Child Health Bureau CSHCN definition, its focus on health services means it may not comprehensively identify the at risk population.
We excluded infants younger than 30 days old, a population unlikely to have immediate exposure to a medical home and whose healthcare expenditures were unrelated to medical home (Romaire et al. 2012). Since the health maintenance organizations (HMOs) were linked to primary care provider based care management and referral, we conducted sensitivity analyses using CSHCN not covered by HMO plans to examine independent impacts of PCMH.
Exposure/Independent Variable
We followed the MEPS-based algorithm described and validated in Romaire and Bell (2010) to construct a parent-reported binary PCMH indicator. The algorithm maps 22 survey items to five medical home domains: usual source of care, accessibility, family centeredness, comprehensiveness, and compassionate care. A child must have a usual source of care and a minimum score in each domain to be considered as having a medical home (Romaire et al. 2012).
Outcome Measures/Dependent Variables
Our outcomes of interest were health care expenditures and quality of care indicators. The MEPS expenditure algorithm incorporates information on payments from the respondents and medical providers with an imputation for missing expenditures using payments for similar services. Expenditures in MEPS represent costs from all sources, including out-of-pocket payments, Medicare, Medicaid, and private insurance (MEPS HC-155: 2012 Full Year Consolidated Data File 2014). Payments for services reported by respondents were totalled as the annual total expenditure including payments to hospitals, physicians, other health care providers, and pharmacies (MEPS HC-155: 2012 Full Year Consolidated Data File 2014). Our study examined annual expenditures in total and by type of service.
Since office-based care is a common setting for primary care, we studied utilization and expenditures for in-person, office-based visits in greater detail. Respondents assigned each of their office-based visits to one of following mutually exclusive categories: general checkup, well-child exam, diagnosis or treatment, psychotherapy/mental health counseling, follow-up/post-operation visit, immunizations/shots, and others (MEPS HC-152G: 2012 Office-Based Medical Provider Visits 2014). Following the literature (Abdus and Selden 2013), we combined visits for general checkups and well-child exams into a “well-child care” category. We did not include emergency, vision exam, and pregnancy-related visits because they were uncommon and not providing additional policy implication for the study. We included the same types of visits in hospital outpatient settings as a sensitivity analysis to allow comparison with previous work (Romaire et al. 2012). All expenditures were converted into 2012 US dollars using the Personal Health Care Expenditures Price index.Footnote 3
Timely well-child visits represent high-quality health care as they provide children with preventive services, developmental evaluations, and ensure timely immunizations (Olson et al. 2008). Thus, our study followed the specification in the MEPS statistical brief to apply receipt of one or more well-child visits annually as the quality of care measure (Caldwell 2013). Abdus and Seldon (2013) found that occurrence of one or more visits is strongly correlated with receiving the age-specific recommended number of visits. We also conducted sensitivity analyses applying a broader definition of well-child visit that included visits for immunization or shots, as used in the literature (Abdus and Selden 2013; Caldwell 2013). Finally, we use parent-reported rating of health care quality from the CAHPS as second quality of care measure (Han et al. 2017). This survey item asked parents to rate the health care that their children received from 0 (the worst possible) to 10 (the best possible) (MEPS HC-155: 2012 Full Year Consolidated Data File 2014). Because responses were heavily skewed toward higher values, we defined perception of high-quality health care as a rating of 10, using lower cut-offs of 8 or 9 in sensitivity testing.
Covariates
We controlled for a range of covariates that were likely to affect outcomes. Following previous research for PCMH and children (Diedhiou et al. 2010; Han et al. 2017), we adopted Andersen’s behavioral model (Andersen 1995) of health services use as a framework to categorize our predictors and covariates into: (1) predisposing factors, including age range, sex, and race/ethnicity; (2) enabling factors, including poverty level, maternal educational level, insurance coverage, geographic region, whether the child resided in a metropolitan area, number of family members, and language spoken at home; and (3) needs factors, including whether the child had functional and/or sensory limitations, and parent-reported children’s health status. Dummy variables were included to adjust for systemic differences between cohort years. These variables are summarized in Table 1. We applied mode imputation for missing predictors, including age groups (1.6%), language (0.1%), region (0.1%), number of family members (2.7%), and mother’s education level (13.6%). Missingness in mother’s education level was elevated in part because we recoded “other degree” (7.0%) as missing. Excluding children with missing covariates from our analysis yielded directionally similar effects of slightly larger size (Online Resource eTable 3 and 4), consistent with the attenuation bias expected from the mode imputation (Ambler et al. 2007). We reported the more conservative findings from mode imputations here.
Statistical Analysis
This study is a cross-sectional analysis of observational, self-reported survey data. Survey design weights in MEPS were applied in order to generate national representative estimates. We first summarized statistics for independent (Table 1) and dependent variables (Table 2) by PCMH. These tables show statistically significant differences between the populations using bivariate \({\chi ^2}~\) tests for categorical variables and t-tests for continuous variables. To balance observed characteristics that were significantly different between the PCMH groups, propensity score weighting, also called inverse probability treatment weighting (IPTW), was applied (Austin 2011). Specifically, to adjust complex survey design with the IPTW following DuGoff et al.’s recommendation (2014), we first calculated the propensity score of having a PCMH using a logistic regression model as a function of the observable patient characteristics and the survey weights. The final weights in the survey-based IPTW were the products of the survey weights and the inverse propensity score (DuGoff et al. 2014), allowing us to improve balance in our sample without dropping any observations.
Annual health care expenditures were also compared by PCMH status using a multivariate two-part model (Deb et al. 2006). In order to produce robust results, all multivariate analyses used IPTW to balance the observable characteristics of study population and included relevant covariates to control for their effects. The two-part model was designed to address patients with zero expenditures (Deb et al. 2006). Part 1 modeled the likelihood of incurring expenditures using a logistic regression; the finding can be interpreted as the probability of the child using care. Part 2 estimated the association between the PCMH and health care expenditures, conditional on accessing care. The general linear model in Part 2 accounts for the right-skewed distribution of the expenditure data by using a log-link with gamma distribution. Both parts are modeled simultaneously to account for the correlation in the error terms. The mean differences by PCMH status were estimated combining both parts in the two-part model, and the 95% confidence intervals (CI) were estimated from 1000 bootstrapped samples (Belotti et al. 2015). For the parent-reported health care quality rating, we estimated the probability parents reported high-quality health care using a multivariate logistic regression model. Statistical significance was judged at a two-sided α = 0.05 level. Data preparation and analyses were performed using STATA MP version 14.0 (StataCorp).
Results
Characteristics of CSHCN
Table 1 summarizes the observable characteristics of the CSHCN. Before implementing IPTW, 48.5% of CSHCN reported receiving care from a PCMH. They were more likely to be male, have private insurance, to be in higher income categories, speak English at home, report better health statuses, reside in metropolitan areas, and have higher maternal education, while being less likely to have functional and/or sensory limitations. Geographic differences were found between PCMH groups. Most CSHCN characteristics were balanced after IPTW, but the age distribution was significantly different between PCMH groups. An alternate test, standardized differences, is not sensitive to sample size and measures adequate balance in age distribution (Austin 2011).
Health Care Expenditures
During the study period, the majority of CSHCN had incurred healthcare expenditures (Table 2). In descriptive statistics with IPTW, CSHCN with a PCMH were more likely to use office-based services and prescriptions. No significant differences were found in health care expenditures conditional on accessing care.
Consistent with the summary statistics in Table 2, Part 1 of the multivariate two-part model (Table 3) showed that having a PCMH was associated with significantly higher odds of accessing healthcare (odds ratio [OR] 1.66, 95% CI 1.22–2.25). CSHCN with a PCMH had higher odds of using office-based services and prescriptions after adjusting for covariates (OR 1.46 and 1.36, 95% CI 1.24–1.72 and 1.17–1.58, respectively). Part 2 of the model estimated the percent change in dollars, conditional on accessing care. Conditional expenditures for office-based services were significantly lower for CSHCN with a PCMH (− 11.2% change, 95% CI − 20.7 to − 0.6%). When both parts were combined, annual expenditures for CSHCN with a PCMH were estimated at $4267, while those without a PCMH were estimated at $3957, a statistically insignificant difference. No significant differences in annual expenditures were found for any type of services when both parts of the model were combined. In other words, an increase in accessing care was not associated with significantly greater expenditures for CSHCN with a PCMH.
We then examined office-based services by type of visit to identify the source of the increase in accessing office-based care and the decrease in office-based conditional expenditures (Table 4). In Part 1, we found an increase in accessing a follow-up/post-operation visit (OR 1.23, 95% CI 1.05–1.45) and an immunizations/shots visit (OR 1.22, 95% CI 1.004–1.48) for CSHCN with a PCMH. Having a PCMH was also associated with a 20% decrease in odds of using psychotherapy/mental health counseling (OR 0.80, 95% CI 0.66–0.96). In Part 2, follow-up/post-operation visits demonstrated a decreased conditional expenditure (− 25.8% change, 95% CI − 39.1 to − 9.6%). Collectively, the follow-up/post-operation visits did not show a significant increase in expenditures because the increase in accessing the services was offset by the decrease in conditional expenditure. We found that a PCMH was associated with lower annual expenditures in psychotherapy/mental health counseling visits (− $31, 95% CI − 61 to − 1), driven by changes in the likelihood of accessing the services. The findings of the sensitivity analyses for excluding CSHCN on HMO plans were directionally identical but lost statistical power due to exclusion of 47% CSHCN (Online Resource eTables 1 and 2).
Quality Outcomes
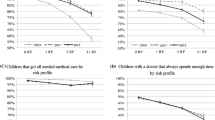
We evaluated quality of care based on parental rating of health care quality and as receipt of well-child care. For parent-reported high-quality health care, CSHCN who received care from a PCMH were more likely to report having best possible health care quality after adjusting for covariates (OR 2.33, p < 0.001; Fig. 1). When we lowered cutoffs in sensitivity testing, these odds ratios increased (i.e., for rating ≥ 8, OR 3.74, p < 0.001).

Multivariate-adjusted parent-reported health care quality rating for CSHCN. Health care quality rating range = 0 (worst) to 10 (best); survey designs and the inverse probability treatment weighting were applied. CSHCN children with special health care needs, PCMH patient centered-medical home, SE standard error
Receipt of well-child care corresponds to Part 1 of the two-part model. As shown in Table 4, having a PCMH was not associated with improved access to well-child care. However, when the immunizations/shots category was included for the broader definition of a well-child visit, PCMH became significantly associated with improved access to well-child visit (OR 1.16, 95% CI 1.03–1.31, p = 0.014). The addition of visits in the hospital outpatient setting showed similar results. This suggested that having a PCMH was associated with improvement in accessing preventive services.
Discussion
We found receiving care from a PCMH had no association with overall health care expenditures, but was significantly associated with better parent-reported health care quality in a nationally representative sample of CSHCN in 2008–2012. Our study advanced evidence surrounding the impact of PCMH on different types of office-based services, where most primary care services are delivered, and applied a model that distinguished the mechanisms of the changes. On one hand, CSHCN with a PCMH were more likely to access prescriptions and office-based services for follow-up/post-operation and immunizations. On the other hand, we observed a decrease in accessing psychotherapy/mental health counseling in office-based visits, resulting in a reduction in expenditures for this type of service for CSHCN with a PCMH. These findings suggested the effects of PCMH varied across types of visits in the office-based setting.
Our findings confirm the prior literature describing the impact of PCMHs on children with an updated focus on CSHCN using recent data (Han et al. 2017; Romaire et al. 2012). We advance the literature by examining hospital outpatient and office-based services separately, finding that PCMH affected them differently. For office-based services, the significance in both parts of the two-part model suggested an offset between the increase in accessing the care and a reduction in expenditures when using office-based services. These findings suggest that the PCMH addressed some access issues (Miller et al. 2013) and potentially lowered the expenditures for individual CSHCN. However, a decrease in mental health services use was found for CSHCN with a PCMH, suggesting that the improvement in accessing care may not be consistent across types of primary care visits. This finding may represent potential forgone mental health services for CSHCN with a PCMH. Alternatively, the findings may suggest that these needs are more often met through the primary care system in a PCMH, and not separately identified. More research is needed to understand how the PCMH model affects individuals’ access to mental health services, and whether there is a rise in unmet mental health care needs and potentially forgone mental health services among CSHCN (An 2016; Sannicandro et al. 2016) within a PCMH.
Consistent with findings in the overall pediatric population (Han et al. 2017), a PCMH was significantly associated with better health care quality for CSHCN without increase in expenditures. When applying the broader definition of well-child visits, having a PCMH was associated with increased access to preventative care for CSHCN, a finding consistent with the literature (Garcia-Huidobro et al. 2016; Strickland et al. 2011). In particular, our findings pinpoint seeking immunizations/shots as an important driver of increased well-child visits.
This study had several limitations. First, the PCMH indicator was constructed by parent-reported survey information. This distinguished our study from facility-based PCMH assignment, which identified whether a person received care from a qualified PCMH practice. Since family-centered care is a key element in the PCMH model and the care burden for CSHCN was likely to fall on family members’ shoulders, parent/familial perceptions of the PCMH have been viewed as relevant when evaluating for CSHCN (“The medical home,” 2002). Second, expenditures and types of office-based visits were subject to recall biases and to misreporting of health care use in the survey setting. However, because the rates of underreporting were similar across all socioeconomic groups, it is unlikely that this misreporting bias would affect the comparison of CSHCN with and without a PCMH (Zuvekas and Olin 2009). Moreover, we only included a functional and/or sensory limitation indicator as a covariate to stratify CSHCN. As the effects of PCMH may differ between health conditions, more research is needed to confirm that resources are allocated to CSHCN who benefit the most from the model. Also, we were unable to investigate whether increased prescription use without changing expenditure (Online Resource eTable 5) related to generic drugs use for CSHCN with a PCMH due to data availability. Lastly, due to the cross-sectional nature of this observational study, we cannot establish causal inference because of the potential existence of unobserved factors that affect having a PCMH and the expenditures. Applying IPTW, which relied on observed CSHCN characteristics, may not fully balance unobserved confounders.
Conclusions
A PCMH was associated with increased access to prescriptions and office-based services in follow-up/post-operation visits and immunizations for CSHCN, without significantly shifting overall expenditures or lowering the quality of care. However, we did not observe that a PCMH enhance the use of mental health services in the primary care setting resulting in decreased expenditures for these services, suggesting the effects of PCMH varied across different types of office-based services. As gaps in mental health services are profound for CSHCN (An 2016; Sannicandro et al. 2016), the effects of PCMH should be further examined to understand whether there were forgone mental health services or the mental health needs were met through improved primary care. More research is warranted to capture the changes and causal relationships among health services, in various settings of PCMHs for CSHCN.
Notes
Nationwide Report from 2009/10 National Survey of Children with Special Health Care Needs. Retrieved from http://www.childhealthdata.org.
MEPS-HC Sample Design and Collection Process. Retrieved from http://www.meps.ahrq.gov/survey_comp/hc_data_collection.jsp.
Using Appropriate Price Indices for Analyses of Health Care Expenditures or income across multiple years. Retrieved from https://meps.ahrq.gov/about_meps/Price_Index.shtml.
References
Abdus, S., & Selden, T. M. (2013). Adherence with recommended well-child visits has grown, but large gaps persist among various socioeconomic groups. Health Affairs, 32(3), 508–515.
Ambler, G., Omar, R. Z., & Royston, P. (2007). A comparison of imputation techniques for handling missing predictor values in a risk model with a binary outcome. Statistical Methods in Medical Research, 16(3), 277–298.
American Academy of Family Physicians. (2008). Joint principles of the patient-centered medical home. Delaware Medical Journal, 80(1), 21.
An, R. (2016). Unmet Mental Health Care Needs in US Children with Medical Complexity, 2005–2010. Journal of Psychosomatic Research, 82, 1–3. https://doi.org/10.1016/j.jpsychores.2015.12.007.
Andersen, R. (1995). Revisiting the behavioral model and access to medical care: Does it matter? Journal of Health and Social Behavior, 36(1), 1–10.
Austin, P. C. (2011). An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behavioral Research, 46(3), 399–424.
Belotti, F., Deb, P., Manning, W. G., & Norton, E. C. (2015). twopm: Two-part models. Stata Journal, 15(1), 3–20.
Caldwell, J. B. T. (2013). Trends in well-child visits: United States, 2002–2009. Retrieved from http://meps.ahrq.gov/mepsweb/data_files/publications/st419/stat419.shtml.
Cooley, W. C., McAllister, J. W., Sherrieb, K., & Kuhlthau, K. (2009). Improved Outcomes associated with medical home implementation in pediatric primary care. Pediatrics, 124(1), 358–364. https://doi.org/10.1542/peds.2008-2600.
Deb, P., Manning, W., & Norton, E. (2006). Modeling health care costs and counts. Paper presented at the 8th World Congress on Health Economics.
Diedhiou, A., Probst, J. C., Hardin, J. W., Martin, A. B., & Xirasagar, S. (2010). Relationship Between presence of a reported medical home and emergency department use among children with asthma. Medical Care Research and Review, 67(4), 450–475. https://doi.org/10.1177/1077558710367735.
DuGoff, E. H., Schuler, M., & Stuart, E. A. (2014). Generalizing observational study results: Applying propensity score methods to complex surveys. Health Services Research, 49(1), 284–303.
Garcia-Huidobro, D., Shippee, N., Joseph-DiCaprio, J., O’Brien, J. M., & Svetaz, M. V. (2016). Effect of patient-centered medical home on preventive services for adolescents and young adults. Pediatrics, 137, e20153813.
Han, B., Yu, H., & Friedberg, M. W. (2017). Evaluating the impact of parent-reported medical home status on children’s health care utilization, expenditures, and quality: A difference-in-differences analysis with causal inference methods. Health Services Research, 52(2), 786–806.
Homer, C. J., Klatka, K., Romm, D., Kuhlthau, K., Bloom, S., Newacheck, P., … Perrin, J. M. (2008). A review of the evidence for the medical home for children with special health care needs. Pediatrics, 122(4), e922–e937.
McPherson, M., Arango, P., Fox, H., Lauver, C., McManus, M., Newacheck, P. W., … Strickland, B. (1998). A new definition of children with special health care needs. Pediatrics, 102(1 Pt 1), 137–140.
MEPS HC-155: 2012 Full Year Consolidated Data File. (2014). Retrieved from https://meps.ahrq.gov/data_stats/download_data/pufs/h155/h155doc.shtml.
MEPS HC-152G: 2012 Office-Based Medical Provider Visits. (2014). Retrieved from https://meps.ahrq.gov/data_stats/download_data/pufs/h152g/h152gdoc.shtml.
Miller, J. E., Nugent, C. N., Gaboda, D., & Russell, L. B. (2013). Reasons for unmet need for child and family health services among children with special health care needs with and without medical homes. PLoS ONE, 8(12), e82570. https://doi.org/10.1371/journal.pone.0082570.
Newacheck, P. W., & Kim, S. E. (2005). A national profile of health care utilization and expenditures for children with special health care needs. Archives of Pediatrics and Adolescent Medicine, 159(1), 10–17.
Olson, L. M., Tanner, J. L., Stein, M. T., & Radecki, L. (2008). Well-child care: Looking back, looking forward. Pediatric Annals. https://doi.org/10.3928/00904481-20080301-08.
Romaire, M. A., & Bell, J. F. (2010). The medical home, preventive care screenings, and counseling for children: Evidence from the medical expenditure panel survey. Academic Pediatrics, 10(5), 338–345.
Romaire, M. A., Bell, J. F., & Grossman, D. C. (2012). Medical home access and health care use and expenditures among children with special health care needs. Archives of Pediatrics and Adolescent Medicine, 166(4), 323–330. https://doi.org/10.1001/archpediatrics.2011.1154.
Sannicandro, T., Parish, S. L., Son, E., & Powell, R. M. (2016). Health care changes for children with special health care needs, 2005–2011. Maternal and Child Health Journal, 21, 1–7.
Strickland, B. B., Jones, J. R., Ghandour, R. M., Kogan, M. D., & Newacheck, P. W. (2011). The medical home: Health care access and impact for children and youth in the United States. Pediatrics, 127(4), 604–611.
The Children with Special Health Care Needs (CSHCN) Screener. (1998). Retrieved from http://www.cahmi.org/wp-content/uploads/2014/06/CSHCNS-Survey-and-scoring.pdf.
The Medical Home. (2002). Pediatrics, 110(1 Pt 1), 184–186.
Zuvekas, S. H., & Olin, G. L. (2009). Validating household reports of health care use in the medical expenditure panel survey. Health Services Research, 44(5 Pt 1), 1679–1700. https://doi.org/10.1111/j.1475-6773.2009.00995.x.
Funding
Funding was provided by Leonard D. Schaeffer Center for Health Policy and Economics (US) and Medica Research Institute.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lin, CW., Romley, J.A. & Carlin, C. The Relationship Between the Patient-Centered Medical Homes, Healthcare Expenditures, and Quality of Care Among Children with Special Health Care Needs. Matern Child Health J 22, 1751–1760 (2018). https://doi.org/10.1007/s10995-018-2572-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-018-2572-4