
Abstract
Objectives
We assessed how shared plans of care (SPoC), a care coordination tool, impact healthcare utilization of a cohort of children with special healthcare needs (CSHCN) and mental health conditions.
Methods
Data, including emergency department (ED) visits, hospitalizations, and primary care visits, were collected through chart review of CSHCN. A Poisson generalized linear mixed model was used to analyze healthcare utilization data for CSHCN.
Results
Our results showed a decrease in primary care visits, hospitalizations, and ED visits for CSHCN after SPoC implementation, though only primary care visits reached significance. Mental health care visits were specifically found to decrease by 39% following employment of SPoC.
Conclusions for Practice
The use of SPoCs in CSHCN had a positive impact on healthcare utilization suggesting widespread use of this tool improved care coordination in this population.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Significance
What is already known on this subject? Healthcare utilization by children with special health care needs (CSHCN) can be influenced by care coordination activities. Shared plans of care (SPoC), comprehensive care coordination documents that focus on patient and family goal setting, can improve parental satisfaction and decrease in hospitalizations and emergency department visits for CSHCN. What this study adds? This study provided an assessment of a SPoC in CSHCN with behavioral and mental health conditions and demonstrated a positive impact on healthcare utilization indicating the value of a standardized care coordination tool.
Introduction
Children with special healthcare needs (CSHCN) are those who are at risk for chronic physical, developmental, and behavioral conditions that utilize healthcare services beyond those of children in general (Merle McPherson et al. 1998). For CSHCN, care coordination implemented though a medical home is associated with fewer out of pocket expenses for families, fewer school absences, decreased time spent coordinating care by parents (Turchi et al. 2009), fewer emergency department visits and hospitalizations (Cooley et al. 2009; Gordon et al. 2007; Raphael et al. 2009), increased parental satisfaction, (Farmer et al. 2011) and prevention of more costly levels of service use (Antonelli and Antonelli 2004; Gordon et al. 2007; Turchi et al. 2009). In Iowa there are over 130,000 CSHCN, yet only 52% receive care that meets medical home criteria (Data Resource Center for Child and Adolescent Health supported by Cooperative Agreement U59MC27866 from the U.S. Department of Health and Human Services, n.d.). While access to care is an important target for improvement, maximizing the efficacy of care coordination in current medical homes is imperative.
Studies to date have evaluated care coordination programs as a whole but few have evaluated specific tools used in the model. One instrument utilized in a medical home for care coordination is a shared plan of care (SPoC). SPoCs have been developed using an accessible, secure platform on which healthcare information for CSHCN is stored and where it can be accessed by providers as well as families (Adams et al. 2013). The ideal SPoC focuses on the comprehensive compiling of medical information and family centered goals that are needed to support coordination of care for the patient as an individual (Wirth and Kuznetsov 2016).
Children with behavioral and mental health conditions represent a unique subset of CSHCN who would benefit from care coordination in a medical home, yet there have been limited studies into the efficacy of care coordination activities for such children (Keller and Sarvet 2013). One study found that nearly half of CSHCN had unmet mental health needs, even though 40% of patients had used mental health care in the past year (Parasuraman et al. 2018). In addition, more parents of CSHCN with mental health problems reported financial problems and reduction of work hours due to their child’s mental health condition when compared to CSHCN without mental health concerns (Dey et al. 2015). The mental healthcare needs of CSHCN is an ever increasing problem (An 2016) that is primed to be tackled by care coordination in a medical home (McAllister et al. 2018).
To our knowledge, specific care coordination tools, such as a SPoC, have not been objectively assessed in the important subset of CSHCN with behavioral and mental health conditions. The purpose of this study was to determine, in a population of CSHCN with behavioral and mental health conditions, whether healthcare utilization as measured by the number of inpatient hospitalizations, emergency department visits, and primary care and outpatient psychiatry visits would be influenced by SPoC implementation.
Methods
Participant Selection and Description
SPoCs were offered to families of children seen in the Division of Child and Community Health’s Regional Centers in 2016. Children less than 18 years of age were eligible for the study if they: (1) had a diagnosis of serious emotional disturbance (SED) as verified by a psychiatrist, psychologist or mental health professional within the past twelve months; or (2) were determined by Iowa Medicaid Enterprise (IME) Medical Services to need a psychiatric hospitalization. “Serious emotional disturbance” was defined as a diagnosable mental, behavioral, or emotional disorder that: (1) was of sufficient duration to meet diagnostic criteria for the disorder specified by the current version of the Diagnostic and Statistical Manual of Mental Disorders (DSM 5) published by the American Psychiatric Association (American Psychiatric Association 2013); and (2) resulted in a functional impairment that substantially interfered with or limited a patient’s role or functioning in family, school, or community activities. This excluded neurodevelopmental disorders, substance-use related disorders, or conditions or problems classified in the current version of the DSM 5 as “other conditions that may be a focus of clinical attention” unless these conditions co-occurred with another diagnosable serious emotional disturbance.
Patients were provided SPoCs on a rolling basis. Patient data, including name, date of birth, and date of SPoC implementation, were gathered from patients’ electronic medical records (EMR). A list of patient diagnoses was obtained from SPoC documentation, and the number and date of hospitalizations, ED visits, and primary care visits were recorded for each patient. Study data were collected and managed using REDCap electronic data capture tools (Harris et al. 2019, 2009). REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies that provided: (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources. This investigation was approved by the Institutional Review Board and all participants provided consent and assent to participate in the study.
SPoCs
Initial versions of the SPoCs were developed according to an implementation guide authored by McAllister et al. (2014). Families met with care coordinators and other stakeholders (school representatives, primary care doctors, DHS/social workers) to create goals, make emergency plans, and emphasize individual patients’ strengths. Many of the initial SPoC documents were recorded on a pre-formatted paper and scanned into the EMR. Later versions of SPoCs were entered into a customizable and editable app that was more directly assessable to parents and other care providers.
Healthcare Utilization
Emergency department (ED) visits, number of occurrences of inpatient hospitalization, and primary care visits were used as proxies for healthcare utilization. All data were collected through chart review. Emergency department visits included quick care visits, while primary care visits included mental health visits and general pediatric visits. Supplemental data for measures of healthcare utilization included: reason for ED visit, reason for inpatient hospitalization, and type of primary care visit (mental health versus general pediatric). All visits were included in the period from 3 years prior to the date of each patient’s SPoC implementation (to serve as baseline) as well as through 3 years after the SPoC date.
Statistics
A Poisson generalized linear mixed model (GLMM) was used to assess the effect of SPoCs on the rates of hospitalization, ED visits, and primary care visits for children with behavioral and mental health conditions (measures of healthcare utilization described above). The Poisson GLMM allowed for modeling of non-normal data collected over a fixed time interval (3 years before and after SPoC implementation). The models were fit separately to the count data for hospitalizations, ED visits, and primary care visits. A separate model was fit with the primary care data, which had been categorized into mental healthcare visits and general pediatrics visits. In addition to a predictor variable indicating if the counts were observed before or after implementation of the SPoC, the number of diagnoses was also included in the model. A patient-specific random effect was included to account for subject-level variation in the rates, with an exposure of 3 years both before and after SPOC implementation, which reflected the periods of health care utilization that were abstracted from the EMR. The Poisson GLMM method of analysis was chosen to determine if the implementation of a SPoC had a significant positive or negative effect on the rate of hospitalizations, primary care visits, and ED visits expected per year. A p-value less than 0.05 was considered significant.
Results
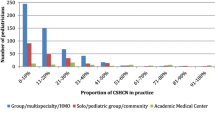
A total of 15 subjects were included in the analysis. Of these, 6.7% of the subjects were female and 93.3% were male. The average age at time of SPoC was 12.2 years old. As patients aged, there was a rise in the mean number of diagnoses by 2.8% (Confidence Interval (CI): (− 5.0, 11.2), p = 0.4949]. The most common diagnoses were Oppositional Defiant Disorder and Generalized Anxiety Disorder (Fig. 1). The average number of diagnoses per patient was 4.5 (min = 1, max = 8). During the observational period, 47% of patients in the study had at least 1 hospitalization. 75% of the hospitalizations were for psychiatric complaints including aggression, Oppositional Defiant Disorder, and suicidal ideation. The mean number of days for hospitalization for each patient was 8.1 days. 19.7% of ED visits were for psychiatric complains including aggression, suicidal ideation, and depression. The majority of other ED visit reasons included, but were not limited to, abdominal pain, pharyngitis, fever, musculoskeletal complaints, and ear/eye problems. Of the primary care visits, 52% were for mental healthcare visits and the remaining were general pediatric visits.

Number of diagnoses for CSHCN with SPoC. Diagnoses of CSHCN that received SPoCs. ADHD attention deficit hyperactivity disorder, ODD oppositional defiant disorder, AD anxiety disorder, MDD major depressive disorder, ASD autism spectrum disorder, PTSD post-traumatic stress disorder; conduct disorder and related disorders includes adjustment disorder with disturbance of conduct; communication disorder/ASD includes mixed receptive-expressive language disorder; endocrine disorders includes premature adrenarche and advanced bone age; Neurologic disorders includes seizure disorder and Tourette’s disorder; OCD includes mixed obsessional thoughts and acts, ODD and related disorders includes adjustment disorder with disturbance of conduct; ophthalmological disorders include exophoria and myopia; urological disorders include testicular pain and communicating hydrocele; other mood disorders includes bipolar disorder and disruptive mood disorder
A Poisson GLMM was fitted to each response variable, with SPoC implementation with number of diagnoses considered as fixed effects and patient ID treated as a random effect. The length of the observational window (i.e., 3 years) was considered as an offset, and inference was focused on the effects of SPoC and number of diagnoses on the rate of hospitalization, primary care visits, and ED visits.
After SPoC implementation, the was considerable variability in the number of hospitalizations and ED visits per year. Though SPoC implementation decreased hospitalization by approximately 22% and ED visits by 15%, neither change reached significance (Hospitalization mean ratio: 0.78, 95% C.I. (0.35, 1.74), p-value: 0.54; ED Visits mean ratio: 0.85, 95% C.I. (0.58, 1.25), p-value: 0.42). However, the estimated number of primary care visits per year decreased significantly by 32% (mean ratio: 0.68, 95% C.I. (0.51, 0.90), p-value: 0.007). Thus, though a decrease was found in all measures of healthcare utilization following SPoC implementation, only the 32% reduction in primary care visits was significant.
Following SPoC implementation, the estimated number of mental health visits per year decreased significantly by 39% (mean ratio: 0.61, 95% C.I. (0.42, 0.91), p-value: 0.02). While the estimated number of general pediatric health visits per year decreased after SPoC implementation by 25%, the decline did not reach statistical significance (mean ratio: 0.75, 95% C.I. (0.52, 1.09), p-value: 0.13).
Though it is difficult to define the severity of mental health illness in a population, number of diagnoses was included in the model as an estimate of mental health disease burden (Zimmerman et al. 2018). The data suggested that as the number of diagnoses per patient increased by one, regardless of implementing a SPoC, the rate of ED visits by 27% (mean ratio: 0.73, 95% C.I. (0.54, 0.98), p-value: 0.04). The effect of the number of diagnoses on the rate of hospitalization and primary care visits was unchanged (Hospitalization mean ratio: 0.59, 95% C.I. (0.19, 1.83), p-value: 0.36; Primary Care Visit mean ratio: 0.90, 95% C.I. (0.75, 1.10), p-value: 0.28).
Discussion
The hypothesis of this study was that, in the population CSHCN with behavioral and mental health conditions, healthcare utilization would be impacted by SPoC implementation and would shift utilization from higher cost interventions, such as inpatient hospitalizations and ED visits, to lower cost incremental care, such as primary care and outpatient psychiatry visits. The evaluation did show that CSHCN had fewer instances of high cost care, such as ED visits and hospitalizations, after a SPoC was implemented. While the costlier types of care did not reach statistical significance, it was interesting that SPoC implementation was associated with a statistically significant decrease, rather than increase, in primary care visits. In addition, this decrease was found to be statistically significant for the category of mental health visits within the defined primary care visits.
In 2018, Lin and colleagues found that patients within a medical home had a higher likelihood of incurring primary care office-based costs including access to prescriptions, follow up/post op, and immunizations (Lin et al. 2018). However, they observed a decrease in accessing psychotherapy/mental health care suggesting that the improvement in accessing care may not be consistent across all types of primary care visits. The significant decrease in number of primary care visits in the current study, would support this conclusion. Further, the reduction in primary care visits following implementation of a SPoC may provide a strategy for primary care providers (PCPs) to effectively support the increasing number of CSHCN with mental and behavioral conditions within their medical home. This study supported the value of the growing number of care coordination tools that patients and families can access, which can be a factor in decreasing the need for primary care visits.
Several care coordination programs have been described that enlist PCPs in the community as more direct partners in the patients’ care coordination, which resulted in a subsequent decrease in hospitalizations and increase in outpatient services (Gordon et al. 2007). While our program enlisted PCP involvement in SPoC creation, anecdotally, there was little PCP buy-in and, objectively, a majority of the care coordination efforts within the program was done by social workers and family-to-family support staff who acted as care coordinators.
Assessing severity of CSHCN with mental health conditions is difficult (Zimmerman et al. 2018). The results of this study found that patients with higher numbers of diagnoses had statistically significantly less ED visits regardless of a SPoC. This counterintuitive finding differs from studies that demonstrated that children with mental and social complexity have higher rates of non-urgent ED visits compared to children without mental and social complexity (Deavenport-Saman et al. 2016). It was possible that in the current study the number of diagnoses may not be an adequate representation of severity since some diagnoses were not mental or behavioral health related. For example, the severity of a patient with well treated depression, anxiety, premature adrenarche, and advanced bone age (total of 4 diagnoses) may have been less than another patient with poorly controlled conduct disorder and aggression (total of 2 diagnoses).
While this patient population is complex, with multiple diagnoses and a high level of patients utilizing inpatient care and ED visits, mental health conditions may have been impacted by a multitude of other factors including family stability and peer-to-peer interaction. This is unique to CSHCN with mental health conditions when compared to medically fragile CSHCN. Distilling the impact of these factors on healthcare utilization would be difficult in a retrospective chart review.
There are several limitations of this study that are important to note. Patient diagnoses and healthcare utilization were distilled from their electronic medical record that could have been incomplete or inaccurate, and the data were collected retrospectively. During the period of study, there was frequent turnover in coverage for Medicaid patients due to privatization of the state’s Medicaid system that occurred during the study period and the turnover of managed care organizations in the state. Loss of Medicaid managed care coverage with a designated payer may have caused a transition between care coordination programs that was difficult to measure. This could have altered the data to show decreased admissions and emergency department visits during the study period (Weier et al. 2017). The study was also limited by the small sample size, which may have limited the identification of significant changes or identified differences that may not have persisted in a larger patient population. In addition, a specific tool was studied in a care coordination framework that may not have fully encompassed all services that were provided to patients.
Overall, CSHCN with mental and behavioral health concerns had decreased utilization of healthcare after a SPoC was implemented. While the decline in hospitalizations and ED visits did not reach statistical significance, SPoC implementation was associated with a significant decrease, rather than hypothesized increase, in primary care visits. This was especially evident for mental health visits. It was also found that an increased number of diagnoses decreased the number of ED visits, a finding that could be complicated by the challenges of measuring the medical severity of specific diagnoses. Future studies should delve into stratification of CSHCN with mental health concerns as well as gathering additional data from Medicaid managed care databases, which has been shown to increase the reliability of results (Weier et al. 2017). While the findings regarding the usefulness of SPoCs in this population were not strong, future studies that include parental satisfaction surveys may further support the value of implementing SPoCs. The improved communication and care coordination provided by the systematic implementation of a SPoC tool can have an important impact on supports provided to CSHCN and their families.
References
Adams, S., Cohen, E., Mahant, S., Friedman, J. N., MacCulloch, R., & Nicholas, D. B. (2013). Exploring the usefulness of comprehensive care plans for children with medical complexity (CMC): A qualitative study. BMC Pediatrics. https://doi.org/10.1186/1471-2431-13-10.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
An, R. (2016). Unmet mental health care needs in U.S. children with medical complexity 2005–2010. Journal of Psychosomatic Research., 10, 12. https://doi.org/10.1016/j.jpsychores.2015.12.007.
Antonelli, R. C., & Antonelli, D. M. (2004). Providing a medical home: The cost of care coordination services in a community-based, general pediatric practice. Pediatrics, 113(5 Suppl), 1522–1528.
Cooley, W. C., McAllister, J. W., Sherrieb, K., & Kuhlthau, K. (2009). Improved outcomes associated with medical home implementation in pediatric primary care. Pediatrics. https://doi.org/10.1542/peds.2008-2600.
Data Resource Center for Child and Adolescent Health supported by Cooperative Agreement U59MC27866 from the U.S. Department of Health and Human Services, H. R. and S. A. M. and C. H. B. (HRSA M. (n.d.). 2016–2017 National Survey of Children’s Health (NSCH) data query.
Deavenport-Saman, A., Lu, Y., Smith, K., & Yin, L. (2016). Do children with autism overutilize the emergency department? Examining visit urgency and subsequent hospital admissions. Maternal and Child Health Journal. https://doi.org/10.1007/s10995-015-1830-y.
Dey, M., Wang, J., Jorm, A. F., & Mohler-Kuo, M. (2015). Children with mental versus physical health problems: Differences in perceived disease severity, health care service utilization and parental health literacy. Social Psychiatry and Psychiatric Epidemiology. https://doi.org/10.1007/s00127-014-0944-7.
Farmer, J. E., Clark, M. J., Drewel, E. H., Swenson, T. M., & Ge, B. (2011). Consultative care coordination through the medical home for CSHCN: A randomized controlled trial. Maternal and Child Health Journal. https://doi.org/10.1007/s10995-010-0658-8.
Gordon, J. B., Colby, H. H., Bartelt, T., Jablonski, D., Krauthoefer, M. L., & Havens, P. (2007). A tertiary care-primary care partnership model for medically complex and fragile children and youth with special health care needs. Archives of Pediatrics and Adolescent Medicine. https://doi.org/10.1001/archpedi.161.10.937.
Harris, P. A., Taylor, R., Minor, B. L., Elliott, V., Fernandez, M., O’Neal, L., & Duda, S. N. (2019). The REDCap consortium: Building an international community of software platform partners. Journal of Biomedical Informatics. https://doi.org/10.1016/j.jbi.2019.103208.
Harris, P. A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J. G. (2009). Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics. https://doi.org/10.1016/j.jbi.2008.08.010.
Keller, D., & Sarvet, B. (2013). Is there a psychiatrist in the house? Integrating child psychiatry into the pediatric medical home. Journal of the American Academy of Child and Adolescent Psychiatry. https://doi.org/10.1016/j.jaac.2012.10.010.
Lin, C. W., Romley, J. A., & Carlin, C. (2018). The relationship between the patient-centered medical homes, healthcare expenditures, and quality of care among children with special health care needs. Maternal and Child Health Journal. https://doi.org/10.1007/s10995-018-2572-4.
McAllister, J. W., Keehn, R. M., Rodgers, R., & Lock, T. (2014). Achieving a shared plan of care with children and youth with special health care needs. Journal of Pediatric Nursing. 1–58.
McAllister, J. W., Keehn, R. M. N., Rodgers, R., Mpofu, P. B., Monahan, P. O., & Lock, T. M. (2018). Effects of a care coordination intervention with children with neurodevelopmental disabilities and their families. Journal of Developmental and Behavioral Pediatrics. https://doi.org/10.1097/DBP.0000000000000576.
McPherson, M., Arango, P., Fox, H., Lauver, C., McManus, M., Newacheck, P. W., et al. (1998). A new definition of children with special health care needs. Pediatrics, 102(1), 137–140.
Parasuraman, S. R., Anglin, T. M., McLellan, S. E., Riley, C., & Mann, M. Y. (2018). Health care utilization and unmet need among youth with special health care needs. Journal of Adolescent Health. https://doi.org/10.1016/j.jadohealth.2018.03.020.
Raphael, J. L., Zhang, Y., Liu, H., Tapia, C. D., & Giardino, A. P. (2009). Association of medical home care and disparities in emergency care utilization among children with special health care needs. Academic Pediatrics. https://doi.org/10.1016/j.acap.2009.05.002.
Turchi, R. M., Berhane, Z., Bethell, C., Pomponio, A., Antonelli, R., & Minkovitz, C. S. (2009). Care coordination for CSHCN: Associations with family-provider relations and family/child outcomes. Pediatrics. https://doi.org/10.1542/peds.2009-1255O.
Weier, R. C., Gardner, W., Conkol, K., Pajer, K., & Kelleher, K. J. (2017). Partners for kids care coordination: Lessons from the field. Pediatrics. https://doi.org/10.1542/peds.2016-2786e.
Wirth, B., Kuznetsov, A. (2016). Shared plan of care: A tool to support child and youth with special health care needs and their families. Resource document. National Association of State Health Policy. Retrieved August 27, 2020, from https://medicalhomeinfo.aap.org/tools-resources/Documents/Shared%20Plan%20of%20Care2.pdf.
Zimmerman, M., Morgan, T. A., & Stanton, K. (2018). The severity of psychiatric disorders. World Psychiatry, 17(3), 258–275.
Acknowledgements
Thank you to Nathan Wikle, Jean Willard, Jennifer Cook, Martha Hanley, Sherri Murphy, and all of the staff in the Division of Child and Community Health. A special thank you to the families who agreed to be a part of this study. This study was supported in part by The University of Iowa Clinical and Translational Science Award—NIH (UL1TR002537).
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mann, E., Pyevich, M., Eyck, P.T. et al. Impact of Shared Plans of Care on Healthcare Utilization by Children with Special Healthcare Needs and Mental Health Diagnoses. Matern Child Health J 25, 584–589 (2021). https://doi.org/10.1007/s10995-020-03101-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-020-03101-3