
Abstract
In response to the high co-occurrence of anxiety symptoms in youth with autism spectrum disorder (ASD), several interventions have been developed for this population. In spite of promising findings, some youth with ASD respond only minimally to such interventions. To understand potential factors that may impact treatment response, the current study explores the role of parental anxiety in youth treatment outcome. Thirty-one youth with ASD, ages 7–18, and their parents participated in the study. Parents completed the State/Trait Anxiety Inventory pre- and post-treatment. Contrary to previous research, there was no correlation between parental anxiety and youth anxiety at baseline or post-treatment. However, parental trait anxiety significantly decreased from pre- to post-treatment for parents of treatment responders. The findings are consistent with previous research and suggest a youth-to-parent influence.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Anxiety disorders are among the most common psychiatric conditions in children and adolescents (Walkup et al. 2008). Not only are clinical anxiety symptoms prevalent in the general pediatric population, but recent research indicates that anxiety symptoms occur at higher rates in youth with autism spectrum disorder (ASD) (de Bruin et al. 2007; Leyfer et al. 2006; van Steensel et al. 2012a). Over the past 5 years, a number of randomized controlled trials examining the efficacy of modified cognitive behavior therapy (CBT) interventions for youth with ASD and anxiety have demonstrated significant reductions in anxiety symptoms following participation (e.g., Reaven et al. 2012a; Storch et al. 2013; White et al. 2013; Wood et al. 2009). Although these programs have demonstrated success in reducing anxiety symptoms, arguably, none of these interventions can claim complete success, since a portion of children demonstrate only modest improvements in anxiety symptoms or do not respond to treatment at all (Reaven et al. 2012a). Indeed, studies generally report that between 20 and 50 % of participants display modest to little positive response to anxiety interventions (White et al. 2013; Wood et al. 2009).
Given that there continues to be a subset of youth with ASD who do not demonstrate clinically meaningful reductions in anxiety symptoms following participation in modified CBT interventions, it is important to understand the factors that may influence treatment response. Parent variables, particularly parental anxiety, may be important to explore, given the extent to which parenting behaviors appear to play a role in the development and maintenance of anxiety symptoms in typically developing children (Creswell et al. 2005; Ginsburg and Schlossberg 2002; McClure et al. 2001; Rapee et al. 2009). Further, it has long been reported that anxious children are more likely to have anxious parents relative to their non-anxious peers; in fact, maternal lifetime history of anxiety may double the risk for anxiety in children (McClure et al. 2001).
Although the mode of anxiety transmission from one generation to another is unclear and complicated by shared genetic influence (Rapee et al. 2009), some researchers hypothesize that “interpretation bias” (the cognitive interpretation of ambiguous situations as threatening) may contribute to the development of anxiety in children, since children observe their parent’s behavior and may internalize their parent’s “maladaptive” cognitions (Creswell et al. 2005). In fact, clinically anxious children interpret ambiguous situations as significantly more threatening than non-anxious children, and maternal and child threat interpretations are significantly correlated (Creswell et al. 2005). When stimuli are perceived as threatening, avoidant behavior may develop. Avoidance may lead to decreased opportunity to manage fearful situations, which in turn results in fewer chances to develop alternative coping behaviors (Reaven and Hepburn 2006). Avoidant coping may also lead to a decreased sense of competence and further avoidance of feared stimuli, contributing to the maintenance of anxiety over time (Dadds and Barrett 2001; Manassis and Bradley 1994).
In an effort to enhance treatment effects for typically developing child participants, recent research has targeted parent variables as part of youth anxiety treatment programs; however, these studies have yielded mixed results (Cobham et al. 1998; Creswell et al. 2008). On the one hand, when parental anxiety was targeted as part of a child anxiety treatment program, the efficacy of the CBT treatment increased for children of anxious parents, while treatment efficacy did not increase for children of non-anxious parents (Cobham et al. 1998). Other treatment studies have found that although children with anxious parents did less well compared to their counterparts with non-anxious parents, treating maternal anxiety did not improve child treatment outcome, suggesting that other parenting factors such as over-involvement may be a better target for intervention (Creswell et al. 2008).
Additional research has explored the reciprocal influence and bidirectional nature of the parent–child relationship in the treatment of childhood anxiety in the typically developing population (Silverman et al. 2009). Rather than targeting parent factors (e.g., parental anxiety) as a way to improve childhood anxiety, some studies suggest that targeting youth anxiety is the key to creating corresponding improvements in parent variables. In a treatment study with children ages 7–16, Silverman et al. (2009) found that when children’s symptoms improved, corresponding improvements were also noted in parental anxiety, providing preliminary support for youth-to-parent treatment influence.
Very few studies have explored the relationship between parental anxiety and anxiety in youth with ASD. However, it is known that parents of children with ASD experience more psychiatric symptoms than do parents of typically developing children or children with other developmental disabilities (Murphy et al. 2000; Rao and Beidel 2009). In addition, parents face greater burdens caring for children with ASD compared with parents of typically developing children, which may lead to high rates of caregiver stress (Estes et al. 2009; Lecavalier et al. 2006; Orsmond et al. 2006). Constant caregiving, with little relief even as children move through adolescence and into young adulthood, tends to be the norm rather than the exception for families of children with ASD (Reaven 2011). Several studies have implicated the presence of maladaptive behavior as greatly contributing to caregiver stress (Estes et al. 2009; Lecavalier et al. 2006). In efforts to manage these behaviors, parents of youth with ASD may adopt a protective parenting style towards their children, who by definition present with marked challenges in social functioning, communication, and behavior (Reaven and Hepburn 2006). Thus, for families of youth with ASD, parental anxiety and stress may be inextricably woven into parenting behaviors, and distinguishing between when to protect youth and when to encourage youth to face fears can be challenging (Reaven and Hepburn 2006).
Conner et al. (2013) examined the relationship between parental state and trait anxiety and treatment response in adolescents with ASD in one of the first studies to empirically investigate the potential association. Multimodal Anxiety and Social Skills Intervention (MASSI; White et al. 2013) was the treatment implemented in this study. MASSI consists of three main treatment components: parent involvement, individual therapy, and group therapy. Core elements of the program included psychoeducation about ASD and anxiety, social skill development, and exposure practice. The researchers examined whether parental state (anxiety at the moment) or trait anxiety (chronic anxiety symptoms) influenced parent report of adolescent anxiety symptoms. Thirty adolescents, ages 12–17, participated in the study, along with both their mothers (n = 29) and their fathers (n = 29). Results indicated that parental state anxiety was significantly correlated with parent report of anxiety in teens. Further, significant decreases in parental trait anxiety were apparent post-treatment for parents of treatment responders, but not for parents of treatment non-responders, providing preliminary evidence of youth-to-parent influence in ASD families.
The purpose of the present study was to examine the relationship between parental anxiety and response to treatment in youth with ASD, and to determine whether the findings reported by Conner et al. (2013) would replicate with a sample of participants with a greater age range (7–18 years), with a mix of fathers and mothers as parent participants, and with a similar but non-identical intervention. Specifically, the objectives of the present study were to: (1) explore the relationship between parental anxiety and parent report of anxiety in youth with ASD; and (2) examine the relationship between parental anxiety and youth treatment outcome, especially for parents of treatment responders versus non-responders. Similar to previous research, it was hypothesized that parental anxiety would be positively correlated with parent report of youth anxiety. It was also hypothesized that parents of treatment responders would demonstrate significant decreases in trait anxiety compared to parents of non-responders.
Methods
Participants
Families were recruited through Colorado Multiple Institution Review Board (COMIRB)-approved study announcements, which were mailed to local schools, clinics, and parent groups. Informed consent and assent were obtained from all study participants prior to data collection and treatment.
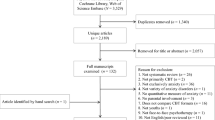
The study drew upon two participant cohorts that were part of larger ongoing research projects examining the nature and treatment of anxiety in children with ASD. The school-aged cohort included 10 families of children between the ages of 7 and 14 years (M = 10.4 years, SD = 2.2) who participated in a randomized controlled trial of Facing Your Fears: Group Therapy for Managing Anxiety in Children with High-Functioning Autism Spectrum Disorders (FYF) (see Reaven et al. 2011). The adolescent cohort included 21 families of teens between the ages of 13 and 18 (M = 15.5 years, SD = 1.3) who were involved in the adolescent adaptation of the intervention (see Reaven et al. 2012b). The total sample was comprised of 31 youth (M age = 13.8 years, SD = 3.0) with ASD and anxiety and their parents (M age = 44.4 years, SD = 9.1). Participant characteristics are summarized in Table 1. In the majority of cases (84 %), mothers were the respondents on study measures.
Inclusion criteria for youth participants were: (a) chronological age of 7–14 years for the school-aged cohort and 13–18 years for the adolescent cohort; (b) confirmed diagnosis of ASD, as determined by expert clinical review on the Autism Diagnostic Observation Schedule (ADOS; Lord et al. 2002) administered within a year prior to treatment, the Social Communication Questionnaire (SCQ; Berument et al. 1999), and a background questionnaire including questions regarding early language milestones; (c) ability to speak in full, complex sentences, reflected in the ability to complete Module 3 or 4 of the ADOS; (d) estimated verbal IQ of 70 or higher on a standardized cognitive evaluation administered within two years prior to recruitment; and (e) clinically significant anxiety symptoms, defined by a score above the clinical cutoff for social (SOC), separation (SEP), and/or generalized anxiety (GAD) on the Screen for Child Anxiety and Related Emotional Disorders (SCARED; Birmaher et al. 1999)—Parent version.
Participants were excluded if: (a) the child’s primary psychiatric symptoms reflected another condition such as depression or psychosis; (b) the child displayed significant problem behaviors or psychiatric illness that prevented him/her or others from accessing the FYF curriculum; or (c) one parent could not commit to attending at least 80 % of treatment sessions. (For further participant details, see Reaven et al. 2012a, b.)
Procedure
Study procedures were completed in compliance with COMIRB for both the school-aged and adolescent cohorts. Families contacted the research clinic and received information regarding study goals and procedures. If the study was of interest to the parent, a research assistant conducted a brief telephone screen for eligibility. If the child was a potentially eligible participant, the family was invited to the research clinic to complete a battery of measures including ASD assessment, cognitive testing (if necessary), anxiety measures, and additional assessments not reported in this study. Families were compensated for their participation in the assessment, both pre- and post-intervention.
FYF Intervention
The FYF intervention is a 14-week, group cognitive behavior therapy (CBT) program designed to reduce anxiety symptoms in youth with high-functioning ASD. Two separate intervention manuals were created for the school-aged and adolescent age groups (Reaven et al. 2011, unpublished manual). Although the sequence and delivery format of intervention strategies differed slightly for school-aged and adolescent groups given their different developmental needs, both intervention groups received the critical components of CBT (i.e., graded exposure, somatic management, cognitive self-control, and a focus on improving emotion regulation). Modifications to traditional CBT activities were made in order to meet the cognitive, linguistic, and social needs of youth with ASD, in line with previous recommendations (Moree and Davis 2010; Reaven et al. 2009). For the school-aged cohort, the provision of visual structure and support, a predictable routine for each session, and a token reinforcement program were included to enhance the accessibility of the content. Use of multiple choice lists, written examples of core concepts, hands-on activities, an emphasis on creative outlets for expression, a focus on strengths and special interests, multiple opportunities for repetition and practice, and video self-modeling were used throughout both the original FYF program (Reaven et al. 2011), as well as the adolescent version (FYF-A; Reaven et al., unpublished manual). In addition to the modifications outlined in the original FYF, FYF-A incorporated technology (e.g., Apple iPod Touch), a social skills module, and increased opportunities for in-session exposure practice. Parents attended every session for the duration of the intervention, participating in the full 90-min session across all age groups, although teens in the adolescent cohort worked more independently throughout the treatment program, while children in the younger cohort interacted more frequently with their parents. Both FYF and FYF-A include well-developed parent curricula that encourage parent support while reviewing key CBT components. Parents are also asked to increase awareness of their own anxiety and how their anxiety may or may not influence parenting behaviors (Please refer to Reaven et al. 2012a, b for more detailed information regarding the FYF/FYF-A programs.).
Measures
Background Information
Parents completed a demographic questionnaire on their children’s medical and early language history, race/ethnicity, parental education, and other family information.
Diagnosis of ASD
Diagnostic status was determined by expert clinical review of the ADOS (Lord et al. 2002) and the SCQ (Berument et al. 1999). The ADOS is a semi-structured, play-based observational assessment of youth social and communicative behaviors indicative of ASD. It is considered best practice in the clinical diagnosis of ASD, in conjunction with parent interview (National Research Council 2001; Wilkinson 2010). The instrument demonstrates sensitivity above 90 % and specificity above 80 % (Lord et al. 2002). Research personnel were trained to 85 % reliability on the full range of ADOS scores prior to administration, and 18 % of ADOS assessments were videotaped and scored for inter-rater reliability. Mean percent agreement on algorithm items was 88 % (range 81–94 %). The SCQ is a 40-item parent-report measure of lifetime and current symptoms of ASD. The measure has good specificity (.80) and sensitivity (.96) (Berument et al. 1999).
Cognitive Screening
Potential participants lacking standardized cognitive assessment within 2 years prior to treatment were administered the Wechsler Abbreviated Scales of Intelligence (WASI; Weschler 2002), a measure of verbal and nonverbal IQ, to help determine eligibility.
Screen for Child Anxiety and Related Emotional Disorders
The SCARED—Parent version (Birmaher et al. 1999) is a 41-item, parent-report inventory of child anxiety symptoms. The measure includes five anxiety subscales (panic/somatic, generalized anxiety disorder (GAD), separation anxiety, social phobia, and school avoidance), as well as a total score with an optimal cutoff of 25 for clinically significant anxiety (Birmaher et al. 1999). The SCARED demonstrates good convergent and divergent validity with other psychiatric assessment tools, as well as strong sensitivity (.71) and specificity (.67) in typically developing samples (Birmaher et al. 1997, 1999; Monga et al. 2000). Among youth with ASD, the parent and child versions of the SCARED show a similar five-factor structure, moderate convergent validity with the Anxiety Disorders Interview Schedule (ADIS; Silverman and Albano 1996), and good sensitivity (.71) and specificity (.67) (Stern et al. 2014). The extended 71-item version of the SCARED also shows strong internal consistency (α > .9) and moderate convergent validity with the ADIS among youth with ASD (van Steensel et al. 2012b). Finally, the SCARED has been judged to be “potentially appropriate” as an outcome measure for anxiety in ASD (Lecavalier et al. 2014).
Parent report of youth anxiety was used in this study rather than child self-report due to the difficulties that some youth with ASD may have in identifying and expressing their own emotions (Blakeley-Smith et al. 2012). In fact, some researchers have been reluctant to rely primarily on child self-report as an accurate reflection of symptom presentation because of the tendency of youth with ASD to under-report their symptoms (Chalfant et al. 2007; Storch et al. 2012).
The SCARED was administered within 6 weeks prior to the start and following the end of each intervention group. Given that it was used as a post intervention measure, directions on the SCARED were modified to read “over the last 2 weeks” rather than “over the last 3 months” for both administrative time points. The STAI and the SCARED were always completed during the same assessment session.
State–Trait Anxiety Inventory
As with the SCARED, parents of youth participants in the FYF treatment completed the State–Trait Anxiety Inventory (STAI; Spielberger et al. 1983) within six weeks prior to the start and following the end of the intervention. The STAI is a widely used self-report measure of anxiety that differentiates between state anxiety (i.e., a temporary experience of anxiety in specific situations) and trait anxiety (i.e., a general, dispositional tendency to feel anxious across situations). The STAI consists of two 20-item scales (one for each type of anxiety). Scores for both scales range from 20 to 80, with higher scores indicating greater anxiety. Norms provided in the manual indicate mean state-anxiety scores for working adult males and females of 35.7 and 35.2, respectively. Mean trait-anxiety scores for these two groups are 34.9 and 34.8, respectively (Spielberger et al. 1983). More recent research that examined control subjects, patients with anxiety disorders, and patients with mood disorders yielded mean state-anxiety scores of 41.6, 51.0, and 53.8 and mean trait-anxiety scores of 42.5, 52.9, and 58.7, respectively (Kaneda and Fujii 2000). The measure demonstrates good internal consistency (αtrait scale = .89; αstate scale = .91), good test–retest reliability for the trait scale (r = .88) (Barnes et al. 2002), and good concurrent validity with other anxiety measures (Spielberger et al. 1983). The STAI was used in the current study as an indicator of parental anxiety.
Results
Analysis Plan
To explore whether there were unique treatment effects depending on parental anxiety, children were classified as either treatment responders or non-responders. Positive treatment response was defined as having clinically significant anxiety prior to treatment (SCARED total score of 25 or greater) and non-clinical levels of anxiety following treatment (SCARED total score below 25). This is a fairly conservative estimate of the impact of this intervention, in that it only captures movement across the clinical cutoff of 25. For instance, a participant who had very high anxiety score of 41 prior to treatment and improved to a score of 26 following treatment would not be considered a treatment responder because the post-treatment score did not fall below 25. This is also a more conservative approach than was used for our inclusion criteria (i.e., above the clinical cutoff on one of three subscales, but not necessarily the SCARED total score). However, this framework was considered appropriate give the exploratory focus of this analysis (Table 2).
Of the 31 youth participants, 10 were characterized as treatment responders, while 21 participants were characterized as treatment non-responders. Despite this conservative measure, 25 out of 31 participants (81 %) reported a drop in anxiety symptoms, and 55 % had a drop of at least 10 points reflecting a positive response to the intervention. Descriptive statistics were examined before exploring whether there were differences in parental anxiety between these groups. T tests (paired and independent sample) with an alpha of .05 were used to examine potential between-group differences.
Baseline Parent and Child Anxiety Symptoms
Parental anxiety was assessed using the STAI (Spielberger et al. 1983), and child anxiety was assessed using the SCARED (Birmaher et al. 1999). Each measure was examined for normality and skewness prior to analysis. All variables had kurtosis and skewness statistics within acceptable parameters except state anxiety post-treatment, which was positively skewed. Visual analysis of the distribution revealed two outliers accounting for this skewness, and natural log transformations were run to normalize the distribution. This procedure resulted in acceptable kurtosis and skewness levels. Importantly, the results of all statistical tests on the transformed data were the same as on untransformed data. Therefore, the results presented here are on untransformed data to facilitate comparison of our data with those of previous studies (Conner et al. 2013; Spielberger et al. 1983).
Child anxiety symptoms reported by the parent on the SCARED did not differ significantly at baseline between responders (M = 37.6, SD = 5.89) and non-responders (M = 34.1, SD = 17.9), t(29) = .60, p = .55; however, they did differ following treatment with responders reporting fewer symptoms (M = 17.0, SD = 7.3) than non-responders (M = 26.0, SD = 11.0), t(29) = 2.4, p = .03.
Relationship Between Parental Anxiety and Parent Report of Youth Anxiety
Prior to treatment, the mean state anxiety score for the whole group was 34.5 (SD = 10.6, range 20–58), and the mean trait anxiety score was 37.6 (SD = 10.2, range 23–62). These means are similar to both Conner et al. (2013) (state: t = .11, p = .97; trait: t = .53, p = .60) and the published norms Spielberger et al. 1983) (state: t = .35, p = .72; trait: t = 1.57, p = .12). There were no significant correlations between parental state anxiety and youth anxiety at baseline, r(31) = .21, p = .26, or post-treatment, r(31) = −.04, p = .84; neither were there significant correlations between parental trait anxiety and youth anxiety at baseline, r(31) = .07, p = .73, or post-treatment, r(31) = −.04, p = .85.
Treatment Effects
There were no significant differences between parents of treatment responders and non-responders reported on either state anxiety, t(29) = .29, p = .77, or trait anxiety, t(29) = 1.29, p = .21 at baseline. For parents of treatment responders, there was no change in parental state anxiety from pre-treatment (M = 35.3, SD = 10.0) to post-treatment (M = 32.5, SD = 10.1), t = .77, p = 46. However, there was a significant improvement in parental trait anxiety from pre-treatment (M = 41.0, SD = 10.5) to post-treatment (M = 33.1, SD = 7.3), t = 2.63, p = .03 for parents of treatment responders. Parents of treatment non-responders, on the other hand, did not demonstrate improved state anxiety from pre-treatment (M = 30.0, SD = 9.9) to post-treatment (M = 33.9, SD = 9.2), t(20) = 1.24, p = .23, or trait anxiety from pre- (M = 34.1, SD = 11.0) to post-treatment (M = 32.5, SD = 8.9), t(20) = .80, p = .43.Footnote 1
Discussion
The main objectives of the present study were: (1) to explore the relationship between parental anxiety and parent report of anxiety in youth with ASD; and (2) to examine the relationship between parental anxiety and response to treatment for anxiety in youth with ASD. Our first hypothesis was not supported, as results indicated that there was not a significant correlation between parent self-report of anxiety symptoms (neither state nor trait) and parent report of youth anxiety symptoms (measured via parent report on the SCARED) at either pre- or post-treatment. The lack of an association between parent self-report of anxiety and parent report of youth anxiety differs from both the Conner et al. (2013) findings, as well as previous literature related to parent report of child anxiety symptoms in typically-developing populations (Hughes and Gullone 2010).
There may be several explanations for the absence of a relationship between parental anxiety and parent report of youth anxiety in this study. First, it may be that parent participants were able to differentiate their own anxiety symptoms from their children’s symptoms, suggesting that reports of youth anxiety symptoms were not influenced by parents’ anxiety status. Alternatively, differences in measurement of youth anxiety between the present study and other studies (e.g., Conner et al. 2013) may contribute to the lack of an association between parent self-report and parent report of youth anxiety (e.g., Child Adolescent Symptom Inventory-20 (CASI-20; Sukhodolsky et al. 2008) vs. the SCARED). Finally, the null finding may have occurred because the sample was underpowered.
Results of the study did support our second hypothesis. That is, trait anxiety significantly decreased for parents of treatment responders, but not for parents of treatment non-responders. State anxiety did not significantly improve for parents of treatment responders or non-responders. This finding indicates that parents of youth who improved after participation in the FYF treatment experienced their own reductions in trait anxiety. Improvement in anxiety symptoms for youth with ASD may have contributed to reductions in parental anxiety. Given that parents attended every session in the Facing Your Fears program for the entire 14 weeks, the strategies taught to youth with ASD might also have been helpful for some parents. Although strategies for identifying and managing parental anxiety are not directly targeted in FYF, there are discussions regarding parental anxiety and parenting style as it relates to youth anxiety. These discussions may have contributed to the observed decreases in parental trait anxiety.
The observed decrease in parental trait anxiety is consistent with findings reported by Conner et al. (2013), which indicated that trait anxiety decreased for parents of treatment responders, but not for parents of treatment non-responders. Our results also support the Conner et al. finding that children of more anxious parents were as likely to respond to treatment as were children of less anxious parents. This is in contrast to previous research with typically developing youth that found that parental anxiety negatively impact children’s response to treatment (Bodden et al. 2008; Cobham et al. 1998; Creswell and Cartwright-Hatton 2007; Creswell et al. 2008).
The present investigation and previous research exploring the relationship between parental anxiety and youth treatment outcome (i.e., Conner et al. 2013) included different measurement tools, unique intervention components, and participants from different age ranges. However, both studies found that trait anxiety decreased post-treatment for parents of treatment responders. Neither treatment program specifically targeted parental anxiety, although parents in both programs may have applied key CBT concepts to themselves as part of their participation in their child’s treatment program. Parents who participated in FYF did have the unique opportunity to directly discuss parental anxiety and the relationship between anxiety and parenting style; however, the extent to which this particular component of FYF contributed to the decreases in parental trait anxiety is unknown.
While modified CBT programs for youth with anxiety and ASD have demonstrated success for a majority of participants, there is still a substantial group of youth who do not demonstrate a significant, positive response to treatment (Reaven et al. 2012a; White et al. 2013). In addition to examining intervention-, therapist-, and child-specific factors that might impact outcome, looking more closely at family factors such as parental anxiety may yield relevant information regarding why some children fail to respond or show only modest improvement. Even though the results from both the current study and the Conner et al. (2013) study suggests that youth of more anxious parents are as likely to respond to treatment compared to children of less anxious parents, both studies had relatively small sample sizes. Given the more consistent findings from the general pediatric literature (Creswell et al. 2008) that parental anxiety may significantly affect youth treatment outcome, it may be premature to take parental anxiety off the table as a critical variable to explore. In fact, further examination of the association between parental anxiety and youth anxiety treatment outcome may provide additional clues for what to emphasize in intervention programs. In addition, given limited research, we cannot yet identify the core components of existing interventions that are likely to yield improvements in child or parental anxiety, nor do we know that improvements in parental anxiety will in fact lead to improvements in anxiety for youth with ASD. Further research is needed to explore whether directly targeting parental anxiety or other parenting behaviors (e.g., parental overprotection) may potentiate youth and parent outcomes.
Limitations and Future Directions
Although the age range of youth participants in the present study was broader than in previous research, the current sample was still relatively small in size and included only youth and families who were seeking treatment. Although including a mix of both mother and father participants had been anticipated for the present study, the vast majority of parent participants were mothers (84 %). Future studies should include more fathers in order to provide information about possible sex differences in parental anxiety and to examine whether mothers and fathers respond in the same way to anxiety interventions for themselves and their children. An additional limitation was that parental anxiety was assessed using a single self-report measure (STAI), and that parents were asked to report on both their own anxiety as well as their child’s anxiety, reflecting a potential confound. Similarly, youth treatment outcome was measured using a single measure (SCARED) for this study. Given the overlap between anxiety symptoms and core deficits of ASD (Kerns and Kendall 2012), clinician interview of anxiety symptoms may be preferable to parent report. Thus, future research should include additional informants or methods of anxiety assessment for both parental anxiety as well as youth anxiety outcome.
Finally, the cross-sectional design of the current study limits our understanding of the directionality of findings. In other words, do youth treatment outcomes improve because parental anxiety decreases, or does parental anxiety decrease because their children respond to treatment? Silverman et al. (2009) reported that youth anxiety symptom improvement was associated with reductions in parental anxiety, even when parents were minimally involved in their child’s individual CBT treatment. Although these findings support the notion that youth-to-parent influence may occur in individual treatment settings, results may not be directly applicable to other treatment modalities, such as group interventions for youth with ASD. Process research involving more frequent assessment of parental and child anxiety symptoms during the course of treatment would help to identify directionality. As additional studies are completed, more specific recommendations may be offered for youth with ASD and anxiety who experience only limited responsiveness to treatment.
Despite these limitations, the current study provides preliminary insight regarding the role of parental anxiety in treating anxiety symptoms in youth with ASD. Given the prevalence of anxiety in this population and critical role of parents in supporting positive outcomes for youth with developmental disabilities, further research is needed to unpack the interaction between parental anxiety and children’s response to anxiety interventions. This study raises new questions regarding how children and adolescents with ASD who struggle with anxiety can best be supported both at home and in treatment settings.
Notes
These analyses are based on the SCARED total score, however, when applied to the individual subscales used as inclusion criteria, the results are similar.
References
Barnes, L. L., Harp, D., & Jung, W. S. (2002). Reliability generalization of scores on the Spielberger state–trait anxiety inventory. Educational and Psychological Measurement, 62, 603–618.
Berument, S. K., Rutter, M., Lord, C., Pickles, A., & Bailey, A. (1999). Autism screening questionnaire: diagnostic validity. The British Journal of Psychiatry, 175, 444–451.
Birmaher, B., Brent, D. A., Chiappetta, L., Bridge, J., Monga, S., & Baugher, M. (1999). Psychometric properties of the screen for child anxiety related emotional disorders (SCARED): A replication study. Journal of the American Academy of Child and Adolescent Psychiatry, 38, 1230–1236.
Birmaher, B., Khetarpal, S., Brent, D., Cully, M., Balach, L., Kaufman, J., & Neer, S. M. (1997). The screen for child anxiety related emotional disorders (SCARED): Scale construction and psychometric characteristics. Journal of the American Academy of Child and Adolescent Psychiatry, 36, 545–553.
Blakeley-Smith, A., Reaven, J., Ridge, K., & Hepburn, S. (2012). Parent–child agreement of anxiety symptoms in youth with autism spectrum disorders. Research in Autism Spectrum Disorders, 6, 707–716.
Bodden, D. H., Bögels, S. M., Nauta, M. H., De Haan, E., Ringrose, J., Appelboom, C., et al. (2008). Child versus family cognitive-behavioral therapy in clinically anxious youth: An efficacy and partial effectiveness study. Journal of the American Academy of Child and Adolescent Psychiatry, 47, 1384–1394.
Chalfant, A. M., Rapee, R., & Carroll, L. (2007). Treating anxiety disorders in children with high functioning autism spectrum disorders: A controlled trial. Journal of Autism and Developmental Disorders, 37, 1842–1857.
Cobham, V., Dadds, M., & Spence, S. (1998). The role of parental anxiety in the treatment of childhood anxiety. Journal of Consulting and Clinical Psychology, 66, 893–905.
Conner, C. M., Maddox, B. B., & White, S. W. (2013). Parents’ state and trait anxiety: Relationships with anxiety severity and treatment response in adolescents with autism spectrum disorders. Journal of Autism and Developmental Disorders, 43, 1811–1818.
Creswell, C., & Cartwright-Hatton, S. (2007). Family treatment of child anxiety: Outcomes, limitations and future directions. Clinical Child and Family Psychology Review, 10(3), 232–252.
Creswell, C., Schniering, C. A., & Rapee, R. M. (2005). Threat interpretation in anxious children and their mothers: Comparison with nonclinical children and the effects of treatment. Behaviour Research and Therapy, 43, 1375–1381.
Creswell, C., Willetts, L., Murray, L., Singhal, M., & Cooper, P. (2008). Treatment of child anxiety: An exploratory study of the role of maternal anxiety and behaviours in treatment outcome. Clinical Psychology & Psychotherapy, 15, 38–44.
Dadds, M. R., & Barrett, P. M. (2001). Practitioner review: Psychological management of anxiety disorders in childhood. Journal of Child Psychology and Psychiatry, 42, 999–1011.
de Bruin, E. I., Ferdinand, R. F., Meester, S., de Nijs, P. F., & Verheij, F. (2007). High rates of psychiatric co-morbidity in PDD-NOS. Journal of Autism and Developmental Disorders, 37, 877–886.
Estes, A., Munson, J., Dawson, G., Koehlere, E., Zhou, X.-H., & Abbott, R. (2009). Parenting stress and psychological functioning among mothers of preschool children with autism and developmental delay. Autism, 13, 375–387.
Ginsburg, G. S., & Schlossberg, M. C. (2002). Family-based treatment of childhood anxiety disorders. International Review of Psychiatry, 14, 143–154.
Hughes, E., & Gullone, E. (2010). Discrepancies between adolescent, mother, and father reports of adolescent internalizing symptom levels and their association with parent symptoms. Journal of Clinical Psychology, 66, 978–996.
Kaneda, Y., & Fujii, A. (2000). The relation between anxiety and depressive symptoms in normal subjects and patients with anxiety and/or mood disorders. The Journal of Medical Investigation, 47, 14–18.
Kerns, C., & Kendall, P. (2012). The presentation and classification of anxiety in autism spectrum disorder. Clinical Psychology: Science and Practice, 19, 323–347.
Lecavalier, L., Leone, S., & Wiltz, J. (2006). The impact of behavior problems on caregiver stress in young people with autism spectrum disorders. Journal of Intellectual Disability Research, 50, 172–183.
Lecavalier, L., Wood, J. J., Halladay, A. K., Jones, N. E., Aman, M. G., Cook, E. H., et al. (2014). Measuring anxiety as a treatment endpoint in youth with autism spectrum disorder. Journal of Autism and Developmental Disorders, 44, 1128–1143.
Leyfer, O., Folstein, S., Bacalman, S., Davis, N., Dinh, E., Morgan, J., & Lainhart, J. (2006). Comorbid psychiatric disorders in children with autism: Interview development and rates of disorders. Journal of Autism and Developmental Disorders, 36, 849–861.
Lord, C., Rutter, M., DiLavore, P. C., & Risi, S. (2002). Autism diagnostic observation schedule. Los Angeles, CA: Western Psychological Services.
Manassis, K., & Bradley, S. J. (1994). The development of childhood anxiety disorders: Toward an integrated model. Journal of Applied Developmental Psychology, 15, 345–366.
McClure, E. B., Brennan, P. A., Hammen, C., & Le Brocque, R. M. (2001). Parental anxiety disorders, child anxiety disorders, and the perceived parent–child relationship in an Australian high-risk sample. Journal of Abnormal Child Psychology, 29, 1–10.
Monga, S., Birmaher, B., Chiappetta, L., Brent, D., Kaufman, J., Bridge, J., & Cully, M. (2000). Screen for child anxiety-related emotional disorders (SCARED): Convergent and divergent validity. Depression and Anxiety, 12(2), 85–91.
Moree, B. N., & Davis, T. E. (2010). Cognitive-behavioral therapy for anxiety in children diagnosed with autism spectrum disorders: Modification trends. Research in Autism Spectrum Disorders, 4, 346–354.
Murphy, M., Bolton, P. F., Pickles, A., Fombonne, E., Piven, J., & Rutter, M. (2000). Personality traits of the relatives of autistic probands. Psychological Medicine, 30, 1411–1424.
National Research Council (US): Committee on Educational Interventions for Children with Autism. (2001). Educating children with autism. Washington, DC: National Academies Press.
Orsmond, G. I., Seltzer, M. M., Greenberg, J. S., & Krauss, M. W. (2006). Mother-child relationship quality among adolescents and adults with autism. American Journal on Mental Retardation, 111(2), 121–137.
Rao, P. A., & Beidel, D. C. (2009). The impact of children with high-functioning autism on parental stress, sibling adjustment, and family functioning. Behavior Modification, 33, 437–451.
Rapee, R. M., Schniering, C. A., & Hudson, J. L. (2009). Anxiety disorders during childhood and adolescence: Origins and treatment. Annual Review of Clinical Psychology, 5, 311–341.
Reaven, J. (2011). The treatment of anxiety symptoms in youth with high-functioning autism spectrum disorders: Developmental considerations for parents. Brain Research, 1380, 255–263.
Reaven, J., Blakeley-Smith, A., Culhane-Shelburne, K., & Hepburn, S. (2012a). Group cognitive behavior therapy for children with high-functioning autism spectrum disorders and anxiety: A randomized trial. Journal of Child Psychology and Psychiatry, 53, 410–419.
Reaven, J., Blakeley-Smith, A., & Leuthe, E. Facing your fears in adolescence (FYF-A). Unpublished manual.
Reaven, J., Blakeley-Smith, A., Leuthe, E., Moody, E., & Hepburn, S. (2012b). Facing your fears in adolescence: Cognitive-behavioral therapy for high-functioning autism spectrum disorders and anxiety. Autism Research and Treatment, 2012, 1–13.
Reaven, J., Blakeley-Smith, A., Nichols, S., Dasari, M., Flanigan, E., & Hepburn, S. (2009). Cognitive-behavioral group treatment for anxiety symptoms in children with high-functioning autism spectrum disorders: A pilot study. Focus on Autism and Other Developmental Disabilities, 24, 27–37.
Reaven, J., Blakeley-Smith, A., Nichols, S., & Hepburn, S. (2011). Facing your fears: Group therapy for managing anxiety in children with high-functioning autism spectrum disorders. Baltimore, MD: Brookes.
Reaven, J., & Hepburn, S. (2006). The parent’s role in the treatment of anxiety symptoms in children with autism spectrum disorders. Mental Health Aspects of Developmental Disabilities, 9, 73–80.
Silverman, W., & Albano, A. (1996). Anxiety disorders interview schedule for children for DSM-IV: (child and parent versions). San Antonio, TX: Psychological Corporation.
Silverman, W. K., Kurtines, W. M., Jaccard, J., & Pina, A. A. (2009). Directionality of change in youth anxiety treatment involving parents: An initial examination. Journal of Consulting and Clinical Psychology, 77, 474–485.
Spielberger, C. D., Gorsuch, R. L., Lushene, R., Vagg, P. R., & Jacobs, G. A. (1983). Manual for the State–Trait Anxiety Inventory STAI (Form Y). Palo Alto, CA: Mind Garden.
Sukhodolsky, D., Scahill, L., Gadow, K., Arnold, L., Aman, M., McDougle, C., et al. (2008). Parent-related anxiety symptoms in children with pervasive developmental disorder: Frequency and association with core autism symptoms and cognitive functioning. Journal of Abnormal Child Psychology, 36, 117–128.
Stern, J., Gadgil, M., Blakeley-Smith, A., Reaven, J., & Hepburn, S. (2014). Psychometric properties of the SCARED in youth with autism spectrum disorder. Research in Autism Spectrum Disorders, 8, 1225–1234.
Storch, E. A., Arnold, E. B., Lewin, A. B., Nadeau, J. M., Jones, A. M., De Nadai, A. S., et al. (2013). The effect of cognitive-behavioral therapy versus treatment as usual for anxiety in children with autism spectrum disorders: A randomized, controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 52, 132–142.
Storch, E., Ehrenreich May, J., Wood, J., Jones, A., Nadai, A., Lewin, A., et al. (2012). Multiple informant agreement on the anxiety disorders interview schedule in youth with autism spectrum disorders. Journal of Child and Adolescent Psychopharmacology, 22, 292–299.
van Steensel, F. J., Bögels, S. M., & Dirksen, C. D. (2012a). Anxiety and quality of life: Clinically anxious children with and without autism spectrum disorders compared. Journal of Clinical Child & Adolescent Psychology, 41, 731–738.
van Steensel, F., Deutschman, A., & Bögels, S. (2012b). Examining the screen for child anxiety-related emotional disorder-71 as an assessment tool for anxiety in children with high-functioning autism spectrum disorders. Autism, 17, 681–692.
Walkup, J. T., Albano, A. M., Piacentini, J., Birmaher, B., Compton, S. N., Sherrill, J. T., et al. (2008). Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. The New England Journal of Medicine, 359, 2753–2766.
Weschler, D. (2002). Weschler abbreviated scales of intelligence (WASI). San Antonio, TX: Psychological Corporation.
White, S. W., Ollendick, T., Albano, A. M., Oswald, D., Johnson, C., Southam-Gerow, M. A., et al. (2013). Randomized controlled trial: Multimodal anxiety and social skill intervention for adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 43, 382–394.
Wilkinson, L. A. (2010). School-age children with autism spectrum disorders: Screening and identification. European Journal of Special Needs Education, 25, 211–223.
Wood, J. J., Drahota, A., Sze, K., Har, K., Chiu, A., & Langer, D. A. (2009). Cognitive behavioral therapy for anxiety in children with autism spectrum disorders: A randomized, controlled trial. Journal of Child Psychology and Psychiatry, 50, 224–234.
Acknowledgments
The authors gratefully acknowledge the assistance of the clinicians who facilitated the treatment groups and the families who participated in this study. The project was funded in part through Autism Speaks and NIH—R33MH089291-03. Additional support came in part from core grants awarded to JFK Partners, the University Center for Excellence in Developmental Disabilities at the University of Colorado Anschutz Medical Campus from the U.S. Department of Health and Human Services, through the Administration on Developmental Disabilities, Grant #90DD0561. J.R., A.B.-S., and S.H. receive royalties from the Facing Your Fears Program, currently published by Paul Brookes Publishing (Reaven et al. 2011).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Reaven, J., Washington, L., Moody, E.J. et al. Examining the Relationship Between Parental Anxiety and Treatment Response in Children and Adolescents with Autism Spectrum Disorder and Anxiety. J Autism Dev Disord 45, 2464–2473 (2015). https://doi.org/10.1007/s10803-015-2410-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-015-2410-0