
Abstract
Comorbid anxiety is common among children with Autism Spectrum Disorder (ASD), and parents of children with ASD are more likely to have anxiety disorders. This study investigated the relationship between parents’ state and trait anxiety and parent-reported internalizing and externalizing symptoms among adolescents (n = 30) with ASD, as well as the relationship of parents’ anxiety symptoms and adolescent treatment response in the context of a randomized controlled trial. Parental state anxiety correlated with severity of adolescent anxiety, and trait anxiety in parents correlated with parent-reported adolescent internalizing and externalizing symptoms. Also, parents of adolescent treatment responders experienced a decrease in their own trait anxiety. Findings highlight the importance of considering parental anxiety when targeting anxiety among youth with ASD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anxiety symptoms are common in ASD (White et al. 2009) and diagnosable anxiety disorders occur in approximately 40 % of children and adolescents with ASD (van Steensel et al. 2011). When present, problems with anxiety among adolescents with ASD contribute to adverse outcomes, such as decreased response to treatment (e.g., social skills training) and poorer relationships with family and teachers (Mayes et al. 2011; Settipani et al. 2012; Sukhodolsky et al. 2008; White et al. 2009). However, we know little about the potential relationship between anxiety symptoms in parents of children with ASD, much less the possible influence of parental anxiety on adolescents with ASD. This is an important consideration given that previous research, mostly in non-ASD samples, indicates multiple pathways for shared pathogenesis of anxiety in parents and children, including shared genetic vulnerabilities (Hettema et al. 2001; Tambs et al. 2009), parental (environmental) influences on the etiology of anxiety in children and adolescents (Degnan et al. 2010; McLeod et al. 2007), and possible effects of parent pathology, such as anxiety disorders, on symptom reporting and treatment outcome for their children (Cobham et al. 2010; Creswell et al. 2008; Liber et al. 2008; Niditch and Varela 2011).
Parenting behaviors have been theorized to play a role both in the development of anxiety (e.g., frequent criticism or less warmth) and the maintenance of anxiety behaviors (e.g., overprotective behavior that reinforces avoidance) (Degnan et al. 2010; Wood et al. 2003). Trait anxiety has been also been studied in the context of parent and child anxiety (van der Bruggen et al. 2010; Wood et al. 2003). High trait anxiety, or the general tendency to respond to situations with anxiety (Spielberger et al. 1983), has been associated with anxiety disorder diagnoses that tend to be chronic, such as Generalized Anxiety Disorder (Chambers et al. 2004), whereas state anxiety, the measure of a person’s anxiety at that moment, is transitory and fluctuates across time (Spielberger et al. 1983). One potential factor in the relationship between parental anxiety and child anxiety is parental control, the over-involvement or pressure parents place on their children to behave in an appropriate manner (van der Bruggen et al. 2010). It has been theorized that parents with high levels of trait anxiety perceive situations involving their children as more threatening and exhibit higher levels of parental control as a result; however, this theorized relationship has not been consistently observed in the research (McLeod et al. 2007; van der Bruggen et al. 2010).
While parents who themselves have anxiety disorders have been shown to be more likely to have children diagnosed with anxiety, parental anxiety has also been correlated with poorer treatment outcome for their children with anxiety (Bodden et al. 2008; Creswell et al. 2008), although this finding is not consistent across all studies (Berman et al. 2000). Informant discrepancies are another consideration when assessing child symptoms (De Los Reyes and Kazdin 2005). Potential for a reporting bias among parents with higher anxiety has been well-studied among the typically developing population, and higher levels of parental depression symptoms and stress levels have also been shown to predict informant bias (see Hughes and Gullone 2010, for a review). Parents who self-report high anxiety tend to report more anxiety symptoms in their children (Briggs-Gowan et al. 1996; Jaffe et al. 2010; Najman et al. 2000).
The relationship between anxiety symptoms among parents and symptoms of anxiety in their children with ASD has only recently been explored. There is evidence that parents of children with ASD are more likely to have affective disorders, including anxiety disorders, when compared to population norms (Lainhart 1999; Mazefsky et al. 2008; Micali et al. 2004; Uljarevic et al. 2012). Prevalence estimates of affective disorders among parents have varied widely across studies, from 10 to 23 % (Daniels et al. 2008; Lainhart 1999; Mazefsky et al. 2010), and studies have found that onset of depression or anxiety symptoms among parents typically predates birth of the child with ASD, suggesting that higher rates of anxiety problems in the parents are not due, at least solely, to the increased stress of raising a child with ASD (Bolton et al. 1998; Mazefsky et al. 2008). Nonetheless, the literature has also established that parents of children with ASD experience higher levels of parenting stress than parents of typically developing children (Benson 2010; Dunn et al. 2001; Johnson et al. 2011; Lyons et al. 2009), as well as parents of children with intellectual disability or other developmental disorders (Dunn et al. 2001). This heightened parental stress may also contribute to higher levels of affective disorder pathology among parents, especially when combined with other risk factors such as perceived lack of social support and maladaptive coping strategies (Dunn et al. 2001; Johnson et al. 2011; Lyons et al. 2009).
Among youth with ASD, the reliability of self-report of psychiatric symptoms has been questioned (Mazefsky et al. 2011; White et al. 2012b). A recent study of child- and parent-report of anxiety symptoms in ASD found that informant concordance was associated with higher verbal cognitive and metacognitive abilities among the youth with ASD (Blakeley-Smith et al. 2012). Under-reporting of anxiety symptoms has also been observed among adolescents with comorbid anxiety disorders compared to parent- and clinician-report, suggesting that multiple informants may be especially important when assessing individuals with ASD (White et al. 2012b). Thus, establishing whether factors such as parent psychopathology influence parent report among the ASD population is important to consider for diagnosing comorbid conditions.
The current study explored the relationship between parental anxiety symptoms and adolescent anxiety severity in a sample of youth with comorbid anxiety disorders and ASD. It was hypothesized that parents’ trait anxiety would be significantly correlated with their adolescent’s anxiety severity. Additionally, it was hypothesized that there would be evidence of reporter bias, in which parents who endorsed higher levels of anxiety symptoms (both trait and state) would report more severe symptoms (both of anxiety and other internalizing and externalizing symptoms) in their adolescents, after controlling for child factors such as ASD symptom severity, social difficulties, and verbal cognitive functioning. In the context of a pilot randomized controlled trial (RCT; White et al. 2012a), we also sought to assess the relationship between parental anxiety and adolescents’ treatment outcomes following cognitive-behavioral therapy targeting anxiety reduction in the adolescents. It was hypothesized that adolescents with more trait anxious parents would have worse treatment outcomes than adolescents of less anxious parents.
Methods
Participants
To be eligible for the RCT, participants had to be between the ages of 12 and 17 years, have an ASD diagnosis supported by the ADOS (Lord et al. 2002) and ADI-R (Lord et al. 1994), and meet diagnostic criteria for at least one of four anxiety disorders (Social Phobia, Generalized Anxiety Disorder, Specific Phobia, or Separation Anxiety Disorder), as determined by the ADIS-C/P (Silverman and Albano 1996). Participants also had to have a current verbal IQ of 70 or above.
Procedures
The study was approved by the university’s human subjects review board. The treatment (Multimodal Anxiety and Social Skills Intervention; White et al. 2010), developed specifically for adolescents ages 12 through 17 with high-functioning ASD and co-occurring anxiety, integrated a social skill development focus with evidence-based approaches for the treatment of childhood anxiety. All parents provided consent and adolescents provided assent prior to data collection. ASD and anxiety disorder diagnoses were confirmed prior to randomization (to active treatment or waitlist). For more details on participant inclusion criteria and the treatment program, see White et al. 2012a.
Measures
Aberrant Behavior Checklist (ABC; Aman et al. 1985). The ABC is a behavior rating scale developed for children with development disabilities, comprised of 58 parent-rated items that are divided among five subscales (Irritability, Social Withdrawal, Stereotypic Behaviors, Hyperactivity, and Inappropriate Speech). Internal consistency ranges from .86 to .95 across the five subscales, and test–retest reliability ranges from .96 to .99 (Aman et al. 1985). The ABC was administered at the baseline visit, prior to randomization. The current study utilized the Irritability and Hyperactivity subscales, which demonstrated excellent internal consistency in the sample (alpha = .93 and .95, respectively).
Child and Adolescent Symptom Inventory-20 (CASI-20; Sukhodolsky et al. 2008). A brief parent-report measure of child/adolescent anxiety, the CASI-20 was derived from the larger pool of anxiety items on the Child and Adolescent Symptom Inventory (Gadow and Sprafkin 1998). Questions that relied heavily on language or reflected other conditions such as Attention-Deficit/Hyperactivity Disorder (e.g., motor restlessness) or ASD (e.g., repetitive behaviors) were excluded from the derived scale. Although the measure has not been widely used to assess treatment outcome, there is preliminary evidence for its reliability and utility in ASD samples (Sukhodolsky et al. 2008). In the present study, the CASI-20 was chosen as the primary outcome measure because it provides a dimensional measure of anxiety severity without being tied to a specific anxiety disorder. The CASI-20 was administered at the baseline timepoint to parents (Parent reporter; CASI-20-P). In addition to being completed by the parents of the participants, one additional familiar adult reporter was asked to complete the CASI-20 for each participant (Other reporter; CASI-20-O). Consistent with previous research (Sukhodolsky et al. 2008), alpha in this sample was high (parent-report: .85; other-report: .88).
Clinical Global Impressions-Improvement Scale (CGI-I; Guy 1976). A masked (to treatment condition), trained observer completed the CGI-I, a clinician-rated measure of improvement compared to baseline. The CGI-I contains a 7-point scale (from 1 = “very much improved” to 7 = “very much worse”). The CGI-I has been used in many different clinical populations and has demonstrated acceptable reliability and validity, including in research of social anxiety disorder (Zaider et al. 2003). The CGI-I was completed at endpoint, immediately after treatment completion. In the trial, a treatment responder was defined as a rating of 1 (“very much improved”) or 2 (“much improved”), and all other endpoint ratings were considered non-responders.
Developmental Disability–Child Global Assessment Scale (DD-CGAS; Wagner et al. 2007). The DD-CGAS is a reliable and valid (test–retest, r = .86; internal consistency, alpha = .79) clinician-rated scale of global functioning in children with ASD. It is completed based on clinician-review of all available information, including other measures, parent reports, and direct observations. Scores can range from 1 to 100, with higher scores indicating better overall functioning. The DD-CGAS was completed at baseline and endpoint by an evaluator masked to treatment assignment.
Short Mood and Feelings Questionnaire (SMFQ; Angold et al. 1995). The SMFQ is a 13-item measure of depressive symptoms in children and adolescents. Each item is scored as “true,” “sometimes true,” or “not true,” based on the last 2 weeks. The current study utilized the parent-report version of the SMFQ, which was administered at baseline. The SMFQ demonstrated acceptable internal consistency (alpha = .91) in the current sample.
Social Responsiveness Scale (SRS; Constantino and Gruber 2005). The SRS is a parent-report measure of ASD severity, with 65 items that assess the severity of social impairment, social awareness, social cognition deficits, social communication deficits, and autistic behaviors (restricted interests and repetitive behaviors). The SRS has been used extensively in the ASD literature (see Bölte et al. 2008, for review), both as a diagnostic tool and as an assessment of treatment response, and the current study utilized the SRS at baseline. Alpha in this sample was high (.93).
State-Trait Anxiety Inventory (STAI; Spielberger et al. 1983). The STAI is a 40-item self-report questionnaire that assesses both stable trait symptoms of anxiety and state or current anxiety. The trait scale includes 20 items about how the individual generally feels, rated on a 4-point scale ranging from “almost never” to “almost always.” The state scale includes 20 items about how the individual feels at the given moment, rated on a 4-pont scale ranging from “not at all” to “very much so.” Parents in both the treatment and waitlist control group completed the STAI at baseline, and the treatment group (n = 15) also completed the STAI post-treatment. Consistent with previous research (Barnes et al. 2002), derived internal consistency for the current sample was acceptable (trait = .91; state = .92).
Wechsler Abbreviated Scale of Intelligence (WASI; Psychological Corporation 1999). The WASI is a reliable and valid brief measure of intelligence. Participants completed the two verbal subtests (Vocabulary and Similarities). The WASI was completed at an intake appointment as an eligibility measure.
Analyses
Data were analyzed with IBM SPSS Statistics Version 20. Pearson bivariate and partial correlations were computed to assess relationships between measures of parent anxiety, adolescent anxiety, child functioning, and other symptoms. Independent samples t-tests were conducted among the entire sample (treatment and waitlist conditions) to examine potential differences in parental anxiety between the parents of treatment responders and the parents of non-responders. A paired-samples t test was also conducted to investigate changes in parental anxiety from pre- to post-treatment among the treatment group (the waitlist group did not have endpoint STAI data).
Complete data were available for all 30 participants on the parent- and self-report baseline measures. Eighteen teachers, 1 school therapist, 1 school aide, 1 school principal, 1 church youth leader, and 1 aunt completed the CASI-20-O, for a total of 23 participants with CASI-20-O data. Seven participants had missing CASI-20-O data, due to the family’s inability to name an available familiar adult to complete the measure or no response from the selected adult. Five participants had missing endpoint data because they discontinued the study, for reasons determined unrelated to the treatment program. For the analyses related to treatment outcome, only those participants who received at least 80 % of the treatment (≥12 individual sessions) were included, reducing the sample by eight (n = 22). The questionnaire data were fairly normally distributed. The anxiety measures included some extreme (high) scores, although skewness and kurtosis were within acceptable levels. Given that the sample was selected for having problems with anxiety, such elevations were interpreted as being accurate assessments and not as problematic outliers. No transformations of the data were made.
Results
Prevalence of Anxiety in Parents
Parental state and trait anxiety were measured via the STAI. Mean state anxiety was 34.37 for the sample at baseline (SD = 10.42; range = 20–64). Baseline mean trait anxiety was 36.17 (SD = 9.21; range = 22–52). These are comparable to published mean total STAI scores for non-clinical adults [(i.e., STAI-State = 35.20 (SD = 10.61); STAI-Trait = 34.79 (SD = 9.22); (Spielberger et al. 1983)], t(479) = 0.42, p = 0.68 and t(479) = 0.79, p = 0.43, respectively. At baseline, parents completed a clinical interview and were asked about parental psychiatric history. Among the mothers (n = 29), seven (24.14 %) self-reported previous and/or current anxiety problems. In addition, eight (27.59 %) of the fathers (n = 29) were identified by their spouses as having experienced previous and/or current anxiety problems. The male guardian of one participant was unable to definitively report on the psychiatric history of the adolescent’s biological parents.
Factors Contributing to Parental Anxiety and Relationship with Parent-Report
Prior to treatment, parental STAI-State scores significantly correlated with parent-reported anxiety symptoms in the adolescents on the CASI-20-P, after controlling for CASI-20-O (r = .462, p = .030). However, parental STAI-Trait scores were not significantly correlated with CASI-20-P scores after controlling for CASI-20-O (r = .292; p = .187).
Adolescent depression (as measured by the SMFQ) was not found to be significantly correlated with parental trait anxiety, but both the ABC hyperactivity and irritability subscales were found to be significantly correlated with parental trait anxiety (Table 1). For parental state anxiety, significant correlations were found for parent-reported symptoms of depression, r = .516, p = .003; hyperactivity, r = .606, p < .001; and irritability, r = .702, p < .001 in their children. However, child ASD severity (SRS total score) was not found to be correlated with either parental state (r = .282, p = .130) or trait (r = .075, p = .693) anxiety.
Treatment Response Effects
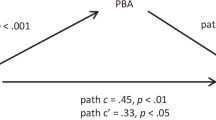
The baseline state and trait anxiety of parents of adolescents determined treatment responders (n = 13) were compared to non-responders’ (n = 9) parents’ anxiety (Fig. 1). Parental state anxiety was found to not significantly differ among parents of treatment responders and non-responders at baseline (t(20) = .399, p = .694). Mean parental trait anxiety also did not differ significantly for the treatment responders (M = 33.08, SD = 7.57) and non-responders (M = 39.44, SD = 10.64), (t(20) = 1.645, p = .116). A paired-sample t-test was conducted for both the treatment responders (n = 6) and non-responders (n = 7) in the initial treatment group to determine whether parents’ trait anxiety decreased over the course of treatment. Due to the lack of endpoint STAI data for the waitlist group, the treatment responders from this group could not be included in the analyses. A significant decrease from baseline (M = 32.33, SD = 6.98) to endpoint (M = 27.67, SD = 5.82) on the parental STAI-Trait was observed (t(5) = −2.870; p = .035) for the parents of treatment responders. For the parents of non-responders, STAI-Trait scores did not significantly change from baseline (M = 41.67, SD = 10.27) to endpoint (M = 42.56, SD = 10.33), t(8) = −.364; p = .725. In contrast, parents’ STAI-State anxiety did not significantly decrease in parents of responders (tI5) = 1.154; p = .301) or in parents of non-responders (t(5) = −.489; p = .638).

Parent STAI-Trait scores and adolescent treatment response on the CGI-I
Among participants in the treatment group who received the full dose of the intervention (i.e., ≥80 % of intended sessions) (n = 13), baseline STAI-Trait was negatively correlated with the change score of DD-CGAS from baseline to endpoint (r = −.561; p = .046). Baseline STAI-State scores were not correlated with change on the DD-CGAS (r = .022; p = .943). Correlations were also run among the entire treatment group sample (n = 15), and the significance of the results did not change.
Discussion
Among a sample of adolescents with comorbid ASD and anxiety, symptomatic anxiety pooled within families. Support was not found for our first hypothesis, that parental trait anxiety would be correlated with severity of youth anxiety. Parental state, but not trait, anxiety, was significantly correlated with parent-report adolescent anxiety. We found support for our second hypothesis, that more anxious parents may exhibit a response bias (i.e., reporting more severe symptoms, both of anxiety and other internalizing and externalizing symptoms, in their adolescents). These findings may underscore the potential importance of considering how anxiety in the parent may affect (possibly bias) reporting about their child’s behavior, with respect to symptoms of anxiety as well as other behavioral difficulties. An alternative, and plausible, explanation for the observed association between parent anxiety and parent-report of child symptoms is that some parents are more able to accurately report on their children’s mental health symptoms. It is also possible that parents with anxiety are better identifiers and reporters of their adolescent’s anxiety, given their first-hand experience with anxiety.
We did not find evidence to support the third hypothesis that the children of more anxious parents would fare less well in treatment. However, parents of adolescents who were treatment responders (judged by independent evaluators) experienced a significant decrease in their own trait anxiety. This is an interesting finding as the experimental treatment did not directly target parents’ anxiety; previous research has shown that parental anxiety typically hinders child response to treatment and does not decrease due to child’s treatment (Creswell et al. 2008). The added stressors present in raising a child with ASD, along with the parent involvement in this RCT, could have possibly contributed to the decrease in parental anxiety. Similar to Creswell et al. (2008) study, the reliability of these results should be considered with caution due to the small sample size. For instance, although the difference in trait anxiety between parents of responders and non-responders (to the treatment) was fairly large (effect size = .70), post hoc power analyses indicate we were underpowered to detect even large differences.
While parental state anxiety correlated with parent-reported child anxiety (after controlling for other-report), the relationship of parent anxiety and child symptoms was not specific to adolescent anxiety. Parents with higher state anxiety also reported greater symptoms of depression, irritability, and hyperactivity in their children. Parental trait anxiety was significantly correlated with parental report of adolescent hyperactivity, irritability, and with independently rated scores of overall adolescent functioning. Adolescent ASD symptom severity was not found to be significantly correlated with parental trait or state anxiety. Parental trait anxiety was significantly positively correlated with adolescents’ verbal IQ, suggesting that parents of higher cognitively functioning adolescents with ASD were more likely to report experiencing higher anxiety. This potentially indicates a directional influence, where greater verbal ability and global functioning (of child) predict higher parental trait anxiety.
Interestingly, while it was hypothesized that parents’ trait anxiety would be related to child anxiety, it was parents’ state anxiety that was correlated, after controlling for other-report of their child’s anxiety. While trait anxiety should be stable, perhaps state anxiety among parents was elevated at the baseline appointment due to the unfamiliarity of the treatment research situation. Parents of children with more severe anxiety symptoms may have been more anxious themselves at the baseline appointment, anticipating more anxiety (and perhaps undesired behaviors related to increased anxiety, such as behavioral outbursts or resistance) from their adolescents. In other words, the parents’ temporarily elevated STAI-State scores, owing to the context in which data were collected, may have influenced their reporting on measures of child symptoms. Parental trait anxiety otherwise acted as we expected. Parental trait anxiety was correlated with treatment response for the adolescents and decreased from baseline to endpoint, suggesting that trait anxiety, not state, is more likely to co-occur for parents of children with an anxiety disorder. This is consistent with findings that trait anxiety represents a vulnerability for developing an anxiety disorder, whereas state anxiety is more transient and context-dependent (Chambers et al., 2004), and that anxiety symptoms and anxiety disorder diagnoses pool within families (Hettema et al. 2001). Although parents’ mean STAI scores were similar to the population norms, it is notable that 24.14 % of the parents in this sample self-identified anxiety symptoms in themselves, and parents identified anxiety symptoms in 27.59 % of the other parents, as this is elevated compared to population norms (Kessler et al. 2005).
Limitations of the current study include the sample’s small size and treatment-seeking nature. Families who sought out an intervention study for anxiety and social skills may not be representative of all families with a child with ASD, and it may be possible that parents who recognize anxiety in their adolescents may also have more anxiety symptoms themselves. In addition, parents’ anxiety was assessed via a clinical interview and the STAI, but no formal diagnostic evaluations of their anxiety were made. Future research in this area should formally assess anxiety disorders among parents in order to better characterize and compare parent and child anxiety. Finally, a lack of STAI data for the waitlist group, following their treatment completion, limited the analyses as we were unable to compare the relationship of adolescent treatment response with change in parental anxiety for the full sample.
Results from this study indicate that anxiety symptoms in parents relate to their reports about their children’s functioning, and moreover, that parental anxiety symptoms may change with treatment that targets social skill development and anxiety reduction in the youth. Based on results from the current study and others (Benson 2010; Dunn et al. 2001; Johnson et al. 2011; Lyons et al. 2009; Mazefsky et al. 2008), this is a parent population that struggles with high levels of anxiety and stress. Treatment of parental anxiety prior to, or concurrent with, adolescent or child treatment may augment treatment response among children and adolescents. Future research should consider assessing parental anxiety when treating anxiety in youth with ASD, as this may be a factor that significantly affects the outcome of anxiety treatment, as it has been shown to do in typically developing children with anxiety (Creswell et al. 2008).
The findings from this study underscore the importance of using multiple reporters in the assessment of children and adolescents with ASD, as parents who reported higher anxiety symptoms in themselves reported more symptomatology in their adolescents, not only in anxiety, but also in mood and hyperactivity symptoms as well. Future research should employ multi-informant (parent-, self-, teacher-, and clinician-) reports in order to account for a potential bias among parents who also present with anxiety or other affective symptoms or diagnoses, and consider use of composite indices to decrease rater bias. The importance of using multiple reporters is important for clinical settings as well, when assessing anxiety symptomatology in adolescents with ASD in order to obtain an accurate picture of the client’s difficulties. Finally, educating parents about the possible familial effects of anxiety (e.g., with respect to modeling anxious avoidance) as well as how parents’ current anxiety can impact perception of their children’s behavior may be useful.
References
Aman, M. G., Singh, N. N., Stewart, A. W., & Field, C. J. (1985). The aberrant behavior checklist: A behavior rating scale for the assessment of treatment effects. American Journal of Mental Deficiency, 89, 485–491.
Angold, A., Costello, E. J., Messer, S. C., Pickles, A., Winder, F., & Silver, D. (1995). Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. International Journal of Methods in Psychiatric Research, 5, 237–249.
Barnes, L. L. B., Harp, D., & Jung, W. S. (2002). Reliability generalization of scores on the Spielberger State-Trait Anxiety Inventory. Educational and Psychological Measurement, 62, 603–618. doi:10.1177/0013164402062004005.
Benson, P. R. (2010). Coping, distress, and well-being in mothers of children with autism. Research in Autism Spectrum Disorders, 4, 217–228. doi:10.1016/j.rasd.2009.09.008.
Berman, S. L., Weems, C. F., Silverman, W. K., & Kurtines, W. M. (2000). Predictors of outcome in exposure-based cognitive and behavioral treatments for phobic and anxiety disorders in children. Behavior Therapy, 31, 713–731. doi:10.1016/S0005-7894(00)80040-4.
Blakeley-Smith, A., Reaven, J., Ridge, K., & Hepburn, S. (2012). Parent–child agreement of anxiety symptoms in youth with autism spectrum disorders. Research in Autism Spectrum Disorders, 6, 707–716. doi:10.1016/j.rasd.2011.07.020.
Bodden, D. H. M., Bögels, S. M., Nauta, M. H., De Haan, E., Ringrose, J., Appelboom, C., et al. (2008). Child versus family cognitive-behavioral therapy in clinically anxious youth: an efficacy and partial effectiveness study. Journal of the American Academy of Child and Adolescent Psychiatry, 47, 1384–1394. doi:10.1097/CHI.0b013e318189148e.
Bölte, S., Poustka, F., & Constantino, J. N. (2008). Assessing autistic traits: Cross-cultural validation of the Social Responsiveness Scale (SRS). Autism Research, 1, 354–363. doi:10.1002/aur.49.
Bolton, P. F., Pickles, A., Murphy, M., & Rutter, M. (1998). Autism, affective and other psychiatric disorders: Patterns of familial aggregation. Psychological Medicine, 28, 385–395. doi:10.1017/S0033291797006004.
Briggs-Gowan, M. J., Carter, A. S., & Schwab-Stone, M. (1996). Discrepancies among mother, child, and teacher reports: Examining the contributions of maternal depression and anxiety. Journal of Abnormal Child Psychology, 24, 749–765. doi:10.1007/BF01664738.
Chambers, J. A., Power, K. G., & Durham, R. C. (2004). The relationship between trait vulnerability and anxiety and depressive diagnoses at long-term follow-up of Generalized Anxiety Disorder. Journal of Anxiety Disorders, 18, 587–607. doi:10.1016/j.janxdis.2003.09.001.
Cobham, V. E., Dadds, M. R., Spence, S. H., & McDermott, B. (2010). Parental anxiety in the treatment of childhood anxiety: A different story three years later. Journal of Clinical Child and Adolescent Psychology, 39, 410–420. doi:10.1080/15374411003691719.
Constantino, J. N., & Gruber, C. P. (2005). Social responsiveness scale. Los Angeles, CA: Western Psychological Services.
Corporation, Psychological. (1999). Wechsler abbreviated scale of intelligence. San Antonio, TX: Psychological Corporation.
Creswell, C., Willetts, L., Murray, L., Singhal, M., & Cooper, P. (2008). Treatment of child anxiety: An exploratory study of the role of maternal anxiety and behaviours in treatment outcome. Clinical Psychology & Psychotherapy, 15, 38–44. doi:10.1002/cpp.559.
Daniels, J. L., Forssen, U., Hultman, C. M., Cnattingius, S., Savitz, D. A., Feychting, M., et al. (2008). Parental psychiatric disorders associated with autism spectrum disorders in the offspring. Pediatrics, 121, e1357–e1362. doi:10.1542/peds.2007-2296.
De Los Reyes, A., & Kazdin, A. E. (2005). Informant discrepancies in the assessment of childhood psychopathology: A critical review, theoretical framework, and recommendations for further study. Psychological Bulletin, 131, 483–509. doi:10.1037/0033-2909.131.4.483.
Degnan, K. A., Almas, A. N., & Fox, N. A. (2010). Temperament and the environment in the etiology of childhood anxiety. Journal of Child Psychology and Psychiatry, 51, 497–517. doi:10.1111/j.1469-7610.2010.02228.x.
Dunn, M. E., Burbine, T., Bowers, C. A., & Tantleff-Dunn, S. (2001). Moderators of stress in parents of children with autism. Community Mental Health Journal, 37, 39–52. doi:10.1023/A:1026592305436.
Gadow, K. D., & Sprafkin, J. (1998). Adolescent Symptom Inventory–4: Norms manual. Stony Brook, NY: Checkmate Plus.
Guy, W. (1976). Clinical global Impressions. ECDEU assessment manual for psychopharmacology, revised. Rockville, MD: National Institute of Mental Health, pp 218–222.
Hettema, J. M., Neale, M. C., & Kendler, K. S. (2001). A review and meta-analysis of the genetic epidemiology of anxiety disorders. American Journal of Psychiatry, 158, 1568–1578. doi:10.1176/appi.ajp.158.10.1568.
Hughes, E. K., & Gullone, E. (2010). Discrepancies between adolescent, mother, and father reports of adolescent internalizing symptom levels and their association with parent symptoms. Journal of Clinical Psychology, 66, 978–996. doi:10.1002/jclp.20695.
Jaffe, M., Gullone, E., & Hughes, E. K. (2010). The roles of temperamental dispositions and perceived parenting behaviours in the use of two emotion regulation strategies in late childhood. Journal of Applied Developmental Psychology, 31, 47–59. doi:10.1016/j.appdev.2009.07.008.
Johnson, N., Frenn, M., Feetham, S., & Simpson, P. (2011). Autism spectrum disorder: Parenting stress, family functioning and health-related quality of life. Families, Systems & Health, 29, 232–252. doi:10.1037/a0025341.
Kessler, R. C., Chiu, W. T., Demler, O., & Walters, E. E. (2005). Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62. doi:10.1001/archpsyc.62.6.617.
Lainhart, J. E. (1999). Psychiatric problems in individuals with autism, their parents and siblings. International Review of Psychiatry, 11, 278–298. doi:10.1080/09540269974177.
Liber, J. M., van Widenfelt, B. M., Goedhart, A. W., Utens, E. M. W. J., van der Leeden, A. J. M., Markus, M. T., et al. (2008). Parenting and parental anxiety and depression as predictors of treatment outcome for childhood anxiety disorders: Has the role of fathers been underestimated? Journal of Clinical Child and Adolescent Psychology, 37, 747–758. doi:10.1080/15374410802359692.
Lord, C., Rutter, M., DiLavore, P. C., & Risi, S. (2002). Autism diagnostic observation schedule. Los Angeles, CA: Western Psychological Services.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism diagnostic interview-revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24, 659–685. doi:10.1007/BF02172145.
Lyons, A. M., Leon, S. C., Roecker Phelps, C. E., & Dunleavy, A. M. (2009). The impact of child symptom severity on stress among parents of children with ASD: The moderating role of coping styles. Journal of Child and Family Studies, 19, 516–524. doi:10.1007/s10826-009-9323-5.
Mayes, S. D., Calhoun, S. L., Murray, M. J., Ahuja, M., & Smith, L. A. (2011). Anxiety, depression, and irritability in children with autism relative to other neuropsychiatric disorders and typical development. Research in Autism Spectrum Disorders, 5, 474–485. doi:10.1016/j.rasd.2010.06.012.
Mazefsky, C. A., Conner, C. M., & Oswald, D. P. (2010). Association between depression and anxiety in high-functioning children with autism spectrum disorders and maternal mood symptoms. Autism Research, 3, 120–127. doi:10.1002/aur.133.
Mazefsky, C. A., Folstein, S. E., & Lainhart, J. E. (2008). Overrepresentation of mood and anxiety disorders in adults with autism and their first degree relatives: What does it mean? Autism Research, 1, 193–197. doi:10.1002/aur.23.
Mazefsky, C. A., Kao, J., & Oswald, D. P. (2011). Preliminary evidence suggesting caution in the use of psychiatric self-report measures with adolescents with high-functioning autism spectrum disorders. Research in Autism Spectrum Disorders, 5, 164–174. doi:10.1016/j.rasd.2010.03.006.
McLeod, B. D., Wood, J. J., & Weisz, J. R. (2007). Examining the association between parenting and childhood anxiety: A meta-analysis. Clinical Psychology Review, 27, 155–172. doi:10.1016/j.cpr.2006.09.002.
Micali, N., Chakrabarti, S., & Fombonne, E. (2004). The broad autism phenotype: Findings from an epidemiological survey. Autism, 8, 21–37. doi:10.1177/1362361304040636.
Najman, J. M., Williams, G. M., Nikles, J., Spence, S., Bor, W., O’Callaghan, M., et al. (2000). Mothers’ mental illness and child behavior problems: Cause-effect association or observation bias? Journal of the American Academy of Adolescent Psychiatry, 39, 592–602. doi:10.1097/00004583-200005000-00013.
Niditch, L. A., & Varela, R. E. (2011). Mother-child disagreement in reports of child anxiety: Effects of child age and maternal anxiety. Journal of Anxiety Disorders, 25, 450–455. doi:10.1016/j.janxdis.2010.11.009.
Settipani, C. A., Puleo, C. M., Conner, B. T., & Kendall, P. C. (2012). Characteristics and anxiety symptom presentation associated with autism spectrum traits in youth with anxiety disorders. Journal of Anxiety Disorders, 26, 459–467. doi:10.1016/j.janxdis.2012.01.010.
Silverman, W. K., & Albano, A. M. (1996). Anxiety disorders interview schedule for DSM-IV. San Antonio, TX: The Psychological Corporation.
Spielberger, C. D., Gorssuch, R. L., Lushene, P. R., Vagg, P. R., & Jacobs, G. (1983). Manual for the state-trait anxiety inventory. Palo Alto, CA: Consulting Psychologists Press, Inc.
Sukhodolsky, D. G., Scahill, L., Gadow, K. D., Arnold, L. E., Aman, M. G., McDougle, C., et al. (2008). Parent-rated anxiety symptoms in children with pervasive developmental disorders: Frequency and association with core autism symptoms and cognitive functioning. Journal of Abnormal Child Psychology, 36, 117–128. doi:10.1007/s10802-007-9165-9.
Tambs, K., Czajkowsky, N., Røysamb, E., Neale, M. C., Reichborn-Kjennerud, T., Aggen, S. H., et al. (2009). Structure of genetic and environmental risk factors for dimensional representations of DSM-IV anxiety disorders. The British Journal of Psychiatry, 195, 301–307. doi:10.1192/bjp.bp.108.059485.
Uljarevic, M., Lidstone, J., Leekam, S. R., Kanaris, H., McKigney, A. M., Mullis, J., Paradice, R., & Nešić, M. (2012). Anxiety in children with autism spectrum disorders is associated with affective symptoms in their mothers. Poster session presented at the International Meeting for Autism Research, Toronto, Canada.
van der Bruggen, C. O., Bögels, S. M., & van Zeilst, N. (2010). What influences parental controlling behaviour? The role of parent and child trait anxiety. Cognition and Emotion, 24, 141–149. doi:10.1080/02699930802618843.
van Steensel, F. J. A., Bögels, S. M., & Perrin, S. (2011). Anxiety disorders in children and adolescents with autistic spectrum disorders: A meta-analysis. Clinical Child and Family Psychology Review, 14, 302–317. doi:10.1007/s10567-011-0097-0.
Wagner, A., Lecavalier, L., Arnold, L. E., Aman, M. G., Scahill, L., Stigler, K. A., et al. (2007). Developmental disabilities modification of the Children’s Global Assessment Scale. Biological Psychiatry, 61, 504–511. doi:10.1016/j.biopsych.2007.01.001.
White, S. W., Albano, A. M., Johnson, C. R., Kasari, C., Ollendick, T., Klin, A., et al. (2010). Development of a cognitive-behavioral intervention program to treat anxiety and social deficits in teens with high-functioning autism. Clinical Child and Family Psychology Review, 13, 77–90. doi:10.1007/s10567-009-0062-3.
White, S. W., Ollendick, T., Albano, A. M., Oswald, D., Johnson, C., Southam-Gerow, M. A., et al. (2012a). Randomized controlled trial: Multimodal anxiety and social skill intervention for adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders. doi:10.1007/s10803-012-1577-x.
White, S. W., Oswald, D., Ollendick, T., & Scahill, L. (2009). Anxiety in children and adolescents with autism spectrum disorders. Clinical Psychology Review, 29, 216–229. doi:10.1016/j.cpr.2009.01.003.
White, S. W., Schry, A. R., & Maddox, B. B. (2012b). Brief report: The assessment of anxiety in high-functioning adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 42, 1138–1145. doi:10.1007/s10803-011-1353-3.
Wood, J. J., McLeod, B. D., Sigman, M., Hwang, W. C., & Chu, B. C. (2003). Parenting and childhood anxiety: Theory, empirical findings, and future directions. Journal of Child Psychology and Psychiatry, 44, 134–151. doi:10.1111/1469-7610.00106.
Zaider, T. I., Heimberg, R. G., Fresco, D. M., Schneier, F. R., & Liebowitz, M. R. (2003). Evaluation of the clinical global impression scale among individuals with social anxiety disorder. Psychological Medicine, 33, 611–622. doi:10.1017/S0033291703007414.
Acknowledgments
This research was funded by a grant from the National Institute of Mental Health (White; K01MH079945).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Conner, C.M., Maddox, B.B. & White, S.W. Parents’ State and Trait Anxiety: Relationships with Anxiety Severity and Treatment Response in Adolescents with Autism Spectrum Disorders. J Autism Dev Disord 43, 1811–1818 (2013). https://doi.org/10.1007/s10803-012-1728-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-012-1728-0