
Abstract
Purpose
To evaluate the effect of preservative-free (PF) tafluprost on diurnal variation of intraocular pressure (IOP) and ocular perfusion pressure (OPP), measured by use of home IOP and blood-pressure (BP) monitoring devices, for primary open angle glaucoma (POAG) patients.
Methods
Twenty-two eyes from 22 patients with POAG were studied. Initially, IOP was measured at the hospital by Goldmann applanation tonometry (GAT) and Icare-ONE rebound tonometry. Each patient was then instructed how to use the Icare-ONE and BP home monitoring devices. IOP and BP were measured at home by the patients, every 4 h, before and 2 weeks after once daily treatment with PF tafluprost (0.0015 %) ophthalmic solution.
Results
Intraclass correlations between different IOP measurements were greater than 0.8. PF tafluprost reduced mean diurnal IOP significantly for patients with POAG, from 15.7 ± 1.2 mmHg at baseline to 12.5 ± 0.6 mmHg 2 weeks after treatment (p < 0.001). It increased mean diurnal OPP from 48.5 ± 7.3 mmHg at baseline to 51.3 ± 7.0 mmHg post-treatment (p < 0.017).
Conclusions
Icare-ONE enables glaucoma patients to measure their own diurnal IOP fluctuations. Patient-measured Icare-ONE IOP readings showed that PF tafluprost effectively reduced diurnal IOP in eyes with POAG.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Glaucoma, characterized by degeneration of the optic nerve and loss of retinal ganglion cells, leads to progressive irreversible loss of vision; it is the second most prevalent cause of blindness worldwide [1]. Therapeutic management of glaucoma includes intraocular pressure (IOP) reduction, ocular blood flow improvement, and neuroprotection. Currently, IOP reduction is the only treatment proved to slow the progression of glaucoma [2–4]. IOP can be reduced by medication, laser treatment, or surgical intervention. To avoid vision-threatening complications that may occur after surgery or laser treatment, medical therapy is usually the initial intervention used to reduce IOP [5]. Furthermore, medical treatment and surgery have similar outcomes for newly diagnosed, early glaucoma [6].
IOP measurements during office hours have been shown to incorrectly identify peaks and ranges [7]. Because a single IOP measurement is a poor predictor of highest 24-h IOP, measurement of diurnal IOP variation provides useful information for management of glaucoma. However, information about IOP fluctuations is limited, because of the impracticality of measuring IOP in a hospital over a period of several days. A portable home tonometer could be used to provide these data and aid the management of glaucoma patients.
The Icare rebound tonometer (Icare Finland, Helsinki, Finland) measures IOP without use of a topical anesthetic [8]. Studies have revealed good agreement between Icare tonometer and Goldmann applanation tonometer readings [9, 10]. Recently, the Icare-ONE tonometer was introduced as a home IOP monitoring device. Measurements taken with the Icare-ONE tonometer by both experienced and inexperienced technicians were comparable with Goldmann applanation tonometer measurements [11]. Asrani et al. [12] reported that the Icare rebound tonometer was accurate and reliable in the hands of patients, and recommended its use as an IOP home monitoring device.
Tafluprost is a relatively new prostaglandin analogue known to be effective in reducing the IOP of patients with glaucoma or ocular hypertension [13–17]. Tafluprost ophthalmic solution is available in a preservative-free (PF) form in some countries, and both preservative-free tafluprost and preservative-containing tafluprost have equivalent efficacy and tolerability [18]. As observed for other prostaglandin analogues, adverse effects of tafluprost include iris and lid pigmentation, increased eyelash growth, conjunctival hyperemia, and deepening of the upper eyelid sulcus [19, 20]. A recent post-marketing study of 4180 patients with glaucoma or ocular hypertension in Japan revealed tafluprost had a good safety profile, in good agreement with results from studies of other prostaglandin analogs [15]. PF tafluprost may be better tolerated by glaucoma patients who have ocular surface problems, for example dry eyes or corneal erosion.
Studies of high-tension and normal-tension glaucoma have shown that tafluprost has IOP-reducing effects [15–17, 19, 21]. Recently, Konstas et al. [22] demonstrated it effectively reduced IOP when IOP was measured over a period of 24 h in a hospital. Although measurement of IOP in a hospital by use of the Goldmann applanation tonometer (GAT) may be more accurate, this might not reflect the patient’s usual daily IOP. Therefore, we conducted this study to investigate the effect of PF tafluprost on diurnal variation of IOP measured by use of the Icare-ONE rebound tonometer by patients with newly diagnosed bilateral primary open-angle glaucoma (POAG). We also evaluated the effect of tafluprost on ocular perfusion pressure (OPP) calculated from blood pressure (BP) readings obtained by use of a BP home monitoring device.
Patients and methods
This study included 25 consecutive patients diagnosed with POAG in both eyes at Korea University Guro Hospital between March and September 2013. Ethical approval for this study was obtained from the Institutional Review Board of Korea University Guro Hospital. Informed consent was obtained from all participants. The study adhered to the tenets of the Declaration of Helsinki. A detailed eye examination, including GAT, Humphrey central 30-2 threshold testing (Zeiss-Humphrey, San Leandro, CA, USA), dilated 30-degree stereoscopic photography and 50-degree red-free photography by use of a Zeiss FF450 IR plus (Carl Zeiss Meditec, Dublin, CA, USA), and measurement of peripapillary retinal nerve fiber layer thickness by use of time domain optical coherence tomography (Stratus OCT TM model 3000; Carl Zeiss Meditec, Oberkochen, Germany) was performed both eyes of the study subjects.
Open angle glaucoma was diagnosed when glaucoma hemifield test results were outside normal limits or the standard deviation, with a p value of less than 0.05, or when there was a cluster of three points or more in the pattern of the deviation plot in a single hemifield with a p value of less than 0.05, with one of the p values less than 0.01 on the Humphrey Swedish interactive threshold algorithm 30-2 test [23]; and/or a retinal nerve fiber layer defect combined with a corresponding optic disc change. Gonioscopy excluded angle closure, rubeosis, and secondary glaucoma. Exclusion criteria included a history of corneal disease, ocular inflammation or infection, previous intraocular surgery, previous treatment for glaucoma, and visual field defects caused by nonglaucomatous disorders. Patients with a high degree of myopia (spherical equivalent refraction ≤−6 D), astigmatism (cylindrical equivalent refraction ≥3 D), or best corrected visual acuity <20/25 were excluded.
The right eye of each patient was evaluated in this study. Initially, IOP was measured by use of a Goldmann applanation tonometer (GAT-IOP) by an experienced member of staff. Next, another member of staff measured IOP by use of an Icare-ONE rebound tonometer (IC-IOPi). Each patient was then taught how to use the Icare-ONE rebound tonometer, and the patients themselves measured IOP with the Icare-ONE (IC-IOPp). To evaluate learning of use of the Icare-ONE rebound home tonometer, intraclass correlation between IC-IOPp and IC-IOPi was calculated. Patients were also taught use of a portable BP monitoring device (Omron HEM-705CP; Europe, Hoofddorp, The Netherlands).
Patients were asked to measure IOP and BP at home by use of both monitoring devices on two separate occasions two weeks apart: before and after treatment with PF tafluprost 0.0015 % ophthalmic solution (Taflotan S®; Santen, Osaka, Japan) once daily, dosed both eyes, at 20:00 ± 1:00 h. IC-IOPp readings were obtained, at home, by each patient, with the patient in a seated position every 4 h for 24 h without medication (at 6 p.m., 10 p.m., 2 a.m., 6 a.m., 10 a.m., and 2 p.m.), and every 4 h for 24 h under medication (at 6 p.m., 10 p.m., 2 a.m., 6 a.m., 10 a.m., and 2 p.m.). Five min after the IOP measurements, the patient took BP measurements while seated. Patients were instructed to maintain their normal daily activities during the day, go to bed at 10 p.m., and to wake at 6 a.m.
The Icare-ONE and its characteristics were explained to the patients. Patients were instructed in its use, with their dominant hand, in front of a mirror. Three valid consecutive sets of measurements, with six measurements for each set, were obtained with the Icare-ONE placed 4–8 mm from the center of the cornea. Invalid measurements, i.e. those with a high standard deviation, were indicated by a flashing red signal “REPEAT”. Invalid measurements because of incorrect positioning or a probe malposition were indicated by a flashing signal “POSITION” or “PROBE”. Invalid measurements and apparent misreadings, for example <6 or >35 mmHg were discarded, and additional measurements were conducted. The average of each set was obtained automatically, and the average values were used for statistical analysis. Precise values stored in the memory of the tonometer were obtained by use of Icare PRO LINK software. After IOP measurements, the participant measured BP by use of a portable BP monitoring device (Omron HEM-705CP) for 5 min after resting seated in a chair. BP measurements were taken twice at with 1-min interval. A form was supplied to participants to report home BP and IOP readings. OPP was calculated by use of the formula: OPP = (1/3 systolic BP + 2/3 diastolic BP) × 2/3 − IOP [24].
Before the study, it was estimated that 22 patients would be required to detect a difference of 1.2 mmHg between baseline and post-treatment at a significance level of 0.05, a power of 80 %, and a given standard deviation of 2.0 mmHg. To allow for withdrawal, 25 patients were enrolled in the study. Sample size was calculated by use of PASS 2008 (NCSS, Kaysville, UT, USA). Pre-treatment and post-treatment IOP and OPP values were compared by use of the Wilcoxon signed rank test; p values of <0.05 were regarded as statistically significant. The correlation between the reduction in mean IOP after treatment and baseline IOP was assessed by use of nonparametric Spearman correlation analysis. Bland–Altman analysis was used to assess bias and 95 % limits of agreement between instruments. All statistical analysis was performed by use of SPSS 21.0 software (SPSS Inc., Chicago, IL, USA).
Results
Of the 25 patients in this study, two were excluded because of such adverse effects as hyperemia and tingling sensation, and one patient was excluded because of poor adherence. After instructions had been given on how to perform the Icare-ONE home tonometry, all the patients proved successful in using the Icare-ONE rebound tonometer. Data from 22 patients were analyzed. There were 19 men and 3 women, with a mean age of 45.9 ± 13.1 years (range 21–67 years). Patient characteristics are listed in Table 1.
Nonparametric Spearman correlation revealed a high correlation between IC-IOPi and IC-IOPp (ρ = 0.823; p < 0.001), and between IC-IOPp and GAT-IOP (ρ = 0.688; p < 0.001). Patient-measured IOP values (IC-IOPp) were within 3 mmHg of the instructor-measured IOP values (IC-IOPi) for 91 % of patients, and IC-IOPi values were within 3 mmHg of GAT-IOP values for 82 % of patients (Fig. 1). Mean GAT-IOP was 16.0 ± 3.4 mmHg (range 10.0–26.0 mmHg). Mean IC-IOPp was 15.9 ± 3.8 mmHg (range 6.5–25.5 mmHg) and mean IC-IOPi was 15.6 ± 3.9 mmHg (range 8.5–25.5 mmHg).

Correlations between different IOP measurement devices. a Significant positive correlation was obtained between IOP measured by use of the Icare-ONE rebound tonometer by the member of staff (IC-IOPi) and IOP measured by use of the Icare-ONE by patients (IC-IOPp) (Spearman correlation coefficient ρ = 0.823; p < 0.001). b Significant positive correlation was observed between IOP measured by use of a Goldmann applanation tonometer (GAT-IOP) by an experienced member of staff and IOP measured by use of the Icare-ONE by patients (IC-IOPp) (Spearman correlation coefficient ρ = 0.688; p < 0.001)
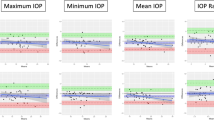
Intraclass correlations between the different testing methods are shown in Table 2. All correlations were >0.8, indicating good agreement between all methods. The Bland–Altman plot in Fig. 2 illustrates the agreement between GAT-IOP and IC-IOPp. The analysis showed that, on average, GAT-IOP was approximately 0.1 mmHg higher than IC-IOPp. Table 3 shows IOP and OPP at baseline and after PF Tafluprost treatment. After two weeks of treatment with topical PF tafluprost 0.0015 %, IOP decreased significantly at all time points (p < 0.001) (Fig. 3). Maximum IOP, minimum IOP, and mean range of variation of IOP decreased significantly (p < 0.001) (Table 3). OPP increased significantly at every time point assessed from baseline (p = 0.017 at 6 p.m., p = 0.002 at 10 p.m., p = 0.008 at 2 a.m., p = 0.014 at 6 a.m., p = 0.001 at 10 a.m., and p < 0.001 at 2 p.m.) (Fig. 4). Systolic or diastolic BP were not significant different either pre-treatment (p = 0.7) or post-treatment (p = 0.1).

Bland–Altman plot of agreement between IOP taken with a Goldmann applanation tonometer (GAT-IOP) and that taken using the Icare-ONE by patients (IC-IOPp). The dotted line indicates the mean difference (bias); the dashed line indicates the 95 % limits of agreement (−5.3 to 5.2 mmHg). The slope of the regression line (r 2 = 0.03) is not significantly different from zero (p = 0.261)

Mean diurnal variation of IOP (mean ± standard deviation) at baseline and over a treatment period of 24 h. IOP decreased significantly at every time point assessed after treatment (*p < 0.001, n = 22)

Mean diurnal variation of OPP (mean ± standard deviation) at baseline and over a treatment period of 24 h. Mean diurnal variation in OPP increased significantly at every time point assessed (*p < 0.02, n = 22)
The incidence of local adverse side effects was 8 % overall: two patients had mild conjunctival hyperemia and foreign body sensation in the treated eyes. However, iris or lid pigmentation, increased eyelash growth, and deepening of upper eyelid sulcus were not observed for any patient during the 2-week study period. There were no systemic adverse side effects.
Discussion
Currently, measurement of diurnal IOP fluctuation is hard to achieve at a patient’s home. A pressure phosphene tonometer is used for home IOP monitoring but its correlation with GAT reported to be poor [25]. A contact lens sensor (Sensimed Triggerfish®; Sensimed, Lausanne, Switzerland) was introduced for continuous monitoring of IOP over a 24-h period [26]. However, because the contact lens sensor does not display the output signal in mmHg, but in arbitrary units that are proportional to the electric signal generated by the contact lens-embedded strain gauge [26], the clinical significance of the results is unclear. Icare tonometry is reported to be easily used by school children without use of topical anesthetics, and good intra-observer and inter-observer reproducibility has been reported [27]. Several studies have demonstrated that Icare rebound tonometry is highly comparable with GAT [9, 10, 27]. These findings suggest that the Icare-ONE rebound tonometer has the potential to be useful for home IOP monitoring.
Asrani et al. [12] reported that 81 % of patient-measured Icare-ONE cases values were within 3 mmHg of the GAT-IOP and that 88 % of measurements were in agreement with physician-measured Icare-ONE readings. Moreno-Montañés et al. [28] reported that 67.7 % of Icare-ONE values measured by patients were within 3 mmHg of GAT values. We found that 82 % of patient-measured Icare-ONE IOP readings were within 3 mmHg of the GAT-IOP. And 91 % of patient-measured Icare-ONE IOP readings were within 3 mmHg of the physician-measured Icare-ONE readings.
Bland–Altman analysis revealed a mean difference of 0.1 mmHg between Icare-ONE patient-measured IOP and GAT readings (Fig. 3). Moreno-Montañés et al. [28] and Rosentreter et al. [29] report differences of 0.3 and 0.6 mmHg between Icare-ONE and GAT, respectively. The intraclass correlation between physician-measured Icare-ONE IOP and GAT-IOP was 0.89. These results are similar to results reported by Asrani et al. [12]; Halkiadakis et al. [30] and Asrani et al. [12] reported that the intraclass correlation between technician-measured Icare rebound tonometer readings and GAT readings was 0.85, and Halkiadakis et al. [30] also reported intraclass correlation of 0.85 between Icare-ONE tonometer values and GAT, indicating excellent agreement between these techniques. Our study of Asian glaucoma patients has also revealed good correlation between Icare-ONE tonometer and GAT readings.
Several workers have reported the IOP-lowering efficacy of tafluprost. Hommer et al. [31] and Rossi et al. [32] reported mean diurnal IOP reduction by PF tafluprost ranging from 22.9 to 32.1 % from the untreated baseline. In a recent study of Korean glaucoma patients IOP reduction was 23 % from baseline [33]. Konstas et al. [22] compared 24-h IOP data after tafluprost and latanoprost treatment of open-angle glaucoma patients, and reported that mean IOP decreased from 24.9 to 17.8 mmHg in the tafluprost-instilled group. In this study we found that mean diurnal IOP decreased from 15.7 ± 1.2 to 12.5 ± 0.6 mmHg after instillation of PF tafluprost for 2-weeks. As far as we are aware this is the first evaluation of the 24-h IOP-reducing effect of PF tafluprost by use of the Icare-ONE home tonometer.
This study revealed that 2-week treatment with tafluprost reduced both the maximum and minimum IOP and the range of variation of diurnal IOP. High mean diurnal IOP and a wider range of variation of diurnal IOP have been shown to be associated with progression of glaucomatous field defects [34]. Konstas et al. [22] showed that the PF tafluprost 24-h IOP fluctuation was 3.2 ± 1.7 mmHg. In this study we found that IOP fluctuations decreased from 8.6 ± 5.0 mmHg at baseline to 4.6 ± 2.6 mmHg after PF tafluprost instillation. The two 24-h IOP studies have several methodological differences. Konstas et al. [22] performed 24-h IOP monitoring in the habitual position during the daytime (10 a.m., 2 p.m., 6 p.m., 10 p.m.) by Goldmann tonometry and during the night (2 a.m., 6 a.m.) by Perkins supine tonometry, whereas we performed 24-h IOP monitoring in the sitting position only by use of the Icare-ONE. It is well-known that IOP measured in the supine position is higher than that in the sitting position [35]. However, we observed greater 24-h IOP fluctuation than reported in the study by Konstas et al. [22] (4.6 ± 2.6 vs 3.2 ± 1.7 mmHg). Different study populations might have also contributed to this discrepancy.
In addition to elevated IOP, reduced or unstable OPP has been shown to affect glaucomatous optic nerve damage [36]. A reduction in nocturnal BP may adversely affect OPP; glaucoma patients may experience lower OPP at night [31]. In our study tafluprost significantly increased OPP without any effect on BP. A previous study reported that latanoprost significantly increased OPP with no effect on BP [24].
This is the first study to use the Icare-ONE rebound tonometer for home monitoring of diurnal IOP for glaucoma patients both before and after treatment with anti-glaucoma medication. The Icare-ONE rebound tonometer has been shown to be both accurate and reliable in the hands of patients [12]. Monitoring of 24-h IOP of glaucoma patients is very useful for accurate diagnosis and proper treatment. Twenty-four-hour IOP monitoring usually requires hospitalization for a day or longer; however, the cost of hospitalization can be a burden to both patients and society. Use of an Icare-ONE rebound tonometer enables doctors to obtain information about patients’ diurnal IOP changes with more ease. Moreover, when combined with a BP-monitoring home device, OPP, also, can be calculated.
This study had several limitations. First, the Icare-One IOP measurements obtained by the patients themselves without any observer may have been erroneous. However, patient and physician-measured Icare-ONE IOP readings were in good agreement. Furthermore, Moreno-Montañés et al. [28] report that most individuals can use the Icare-ONE after a short training session and that IOP values are reliable. Second, the sample size of this study was small and most participants were men. Third, because the participants in this study were relatively young, the results might not be generalizable to older glaucoma patients. It has recently been reported that, compared with GAT, the Icare-ONE underestimated IOP for the elderly [37]. Witte et al. [38] reported that differences between patient-measured Icare-ONE and the GAT results occasionally fluctuated substantially. However, for patients younger than 60 years the agreement was better. Therefore, the relatively young age of the participants may have reduced potential bias related to use of the Icare-ONE tonometer [28]. Younger age and less comorbidity may also affect the accuracy of measurements of OPP. Fourth, measurements obtained during the nighttime may not reflect IOP alterations in a recumbent posture (supine, prone, or lateral decubitus) [39–42] or what happens during physiological sleeping patterns, because our IOP measurements were obtained with the patients awake and seated. Finally, the relatively short treatment period of 2 weeks may not have been sufficient to assess the full IOP-reducing efficacy of PF tafluprost.
In conclusion, this study revealed that IOP readings obtained by use of the Icare-ONE rebound tonometer correlate well with GAT IOP readings. The good inter-observer reliability of these techniques suggest the feasibility of home monitoring of IOP. PF tafluprost was found to significantly reduce IOP and increase OPP over 24 h at all time points assessed.
References
Leske MC. Open-angle glaucoma—an epidemiologic overview. Ophthalmic Epidemiol. 2007;14:166–72.
Heijl A, Leske MC, Bengtsson B, Hyman L, Bengtsson B, Hussein M. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2002;120:1268–79.
The AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): the relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol. 2000;130:429–40.
Kass MA, Heuer DK, Higginbotham EJ, Johnson CA, Keltner JL, Miller JP, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:701–13.
The American Academy of Ophthalmology Panel. Preffered practice pattern guidelines: primary open-angle glaucoma. The American Academy of Ophthalmology. 2010. http://one.aao.org/preferred-practice-pattern/primary-openangle-glaucoma-ppp--october-2010. Accessed 21 Nov 2014.
Mills RP, Janz NK, Wren PA, Guire KE. Correlation of visual field with quality-of-life measures at diagnosis in the Collaborative Initial Glaucoma Treatment Study (CIGTS). J Glaucoma. 2001;10:192–8.
Hughes E, Spry P, Diamond J. 24-hour monitoring of intraocular pressure in glaucoma management: a retrospective review. J Glaucoma. 2003;12:232–6.
Kontiola A, Puska P. Measuring intraocular pressure with the pulsair 3000 and rebound tonometers in elderly patients without an anesthetic. Graefes Arch Clin Exp Ophthalmol. 2004;242:3–7.
Fernandes P, Diaz-Rey JA, Queiros A, Gonzalez-Meijome JM, Jorge J. Comparison of the ICare rebound tonometer with the Goldmann tonometer in a normal population. Ophthalmic Physiol Opt. 2005;25:436–40.
Martinez-de-la-Casa JM, Garcia-Feijoo J, Castillo A, Garcia-Sanchez J. Reproducibility and clinical evaluation of rebound tonometry. Invest Ophthalmol Vis Sci. 2005;46:4578–80.
Abraham LM, Epasinghe NC, Selva D, Casson R. Comparison of the ICare rebound tonometer with the Goldmann applanation tonometer by experienced and inexperienced tonometrists. Eye. 2008;22:503–6.
Asrani S, Chatterjee A, Wallace DK, Santiago-Turla C, Stinnett S. Evaluation of the ICare rebound tonometer as a home intraocular pressure monitoring device. J Glaucoma. 2011;20:74–9.
Takagi Y, Nakajima T, Shimazaki A, Kageyama M, Matsugi T, Matsumura Y, et al. Phamacological characteristics of AFP-168 (tafluprost), a new prostanoid FP receptor agonist, as an ocular hypotensive drug. Exp Eye Res. 2004;78:767–76.
Uusitalo H, Chen E, Pfeiffer N, Brignole-Baudouin F, Kaarniranta K, Leino M, et al. Switching from a preserved to a preservative-free prostaglandin preperation in topical glaucoma medication. Acta Ophthalmol. 2010;88:329–36.
Kuwayama Y, Nomura A. Prospective observational post-marketing study of tafluprost for glaucoma and ocular hypertension: short-term efficacy and safety. Adv Ther. 2014;31:461–71.
Nakano T, Yoshikawa K, Kimura T, Suzumura H, Nanno M, Noro T. Efficacy and safety of tafluprost in normal-tension glaucoma with intraocular pressure of 16 mmHg or less. Jpn J Ophthalmol. 2011;55:605–13.
Mizoguchi T, Ozaki M, Unoki K, Dake Y, Eto T, Arai M. A randomized crossover study comparing tafluprost 0.0015% with travoprost 0.004% in patients with normal-tension glaucoma (corrected). Clin Ophthalmol. 2012;6:1579–84.
van der Valk R, Webers CA, Schouten JS, Zeegers MP, Hendrikse F, Prins MH. Intraocular pressure-lowering effects of all commonly used glaucoma drugs-A meta-analysis of randomized clinical trials. Ophthalmology. 2005;112:1177–85.
Traverso CE, Ropo A, Papadia M, Uusitalo H. A phase II study on the duration and stability of the intraocular pressure-lowering effect and tolerability of tafluprost compared with latanoprost. J Ocul Phamacol Ther. 2010;26:97–104.
Sakata R, Shirato S, Miyata K, Aihara M. Incidence of deepening of the upper eyelid sulcus on treatment with a tafluprost ophthalmic solution. Jpn J Ophthalmol. 2014;58:212–7.
Chabi A, Varma R, Tsai JC, Lupinacci R, Pigeon J, Baranak C, et al. Randomized clinical trial of the efficacy and safety of preservative-free tafluprost and timolol in patients with open-angle glaucoma or ocular hypertension. Am J Ophthalmol. 2012;153:1187–96.
Konstas AG, Quaranta L, Katsanos A, Riva I, Tsai JC, Giannopoulos T, et al. Twenty-four hour efficacy with preservative free tafluprost compared with latanoprost in patients with primary open angle glaucoma or ocular hypertension. Br J Ophthalmol. 2013;97:1510–5.
Anderson DR, Patella VM. Automated static perimetry. 2nd ed. St. Louis: Mosby; 1999.
Drance SM, Crichton A, Mills RP. Comparison of the effect of latanoprost 0.005% and timolol 0.5% on the calculated ocular perfusion pressure in patients with normal-tension glaucoma. Am J Ophthalmol. 1998;125:585–92.
Li J, Herndon LW, Asrani SG, Stinnett S, Allingham RR. Clinical comparison of the proview eye pressure monitor with the Goldmann applanation tonometer and the tonopen. Arch Ophthalmol. 2004;122:1117–21.
Mansouri K, Shaarawy T. Continuous intraocular pressure monitoring with a wireless ocular telemetry sensor: initial clinical experience in patients with open angle glaucoma. Br J Ophthalmol. 2011;95:627–9.
Sahin A, Basmak H, Niyaz L, Yildirim N. Reproducibility and tolerability of the ICare rebound tonometer in school children. J Glaucoma. 2007;16:185–8.
Moreno-Montanes J, Martinez-de-la-Casa JM, Sabater AL, Morales L, Saenz C, Garcia-Feijoo J. Clinical evaluation of the new rebound tonometers Icare PRO and Icare ONE compared with the Goldmann tonometer. J Glaucoma. 2014. doi:10.1097/ijg.0000000000000058.
Rosentreter A, Jablonski KS, Mellein AC, Gaki S, Hueber A, Dietlein TS. A new rebound tonometer for home monitoring of intraocular pressure. Graefes Arch Clin Exp Ophthalmol. 2011;249:1713–9.
Halkiadakis I, Stratos A, Stergiopoulos G, Patsea E, Skouriotis S, Mitropoulos P, et al. Evaluation of the Icare-ONE rebound tonometer as a self-measuring intraocular pressure device in normal subjects. Graefes Arch Clin Exp Ophthalmol. 2012;250:1207–11.
Hommer A, Mohammed RO, Burchert M, Kimmich F. IOP-lowering efficacy and tolerability of preservative-free tafluprost 0.0015% among patients with ocular hypertension or glaucoma. Curr Med Res Opin. 2010;26:1905–13.
Rossi GC, Pasinetti GM, Raimondi M, Ricciardelli G, Scudeller L, Blini M, et al. Efficacy and ocular surface tolerability of preservative-free tafluprost 0.0015%: a 6-month, single-blind, observational study on naive ocular hypertension or glaucoma patients. Expert Opi Drug Saf. 2012;11:519–25.
Hwang YH. Efficacy and tolerability of preservative-free tafluprost 0.0015% in Korean patients with glaucoma. Clin Ophthalmol. 2014;8:71–2.
Asrani S, Zeimer R, Wilensky J, Gieser D, Vitale S, Lindenmuth K. Large diurnal fluctuations in intraocular pressure are an independent risk factor in patients with glaucoma. J Glaucoma. 2000;9:134–42.
Tsukahara S, Sasaki T. Postural change of IOP in normal persons and in patients with primary wide open-angle glaucoma and low-tension glaucoma. Br J Ophthalmol. 1984;68:389–92.
Liu JH, Kripke DF, Twa MD, Hoffman RE, Mansberger SL, Rex KM, et al. Twenty-four-hour pattern of intraocular pressure in the aging population. Invest Ophthalmol Vis Sci. 1999;40:2912–7.
Sakamoto M, Kanamori A, Fujihara M, Yamada Y, Nakamura M, Negi A. Assessment of IcareONE rebound tonometer for self-measuring intraocular pressure. Acta Ophthalmol. 2014;92:243–8.
Witte V, Glass A, Beck R, Guthoff R. Evaluation of the self-tonometer Icare ONE in comparison to Goldmann applanation tonometry. Ophthalmologe. 2012;109:1008–13.
Lee JY, Yoo C, Jung JH, Hwang YH, Kim YY. The effect of lateral decubitus position on intraocular pressure in healthy young subjects. Acta Ophthalmol. 2012;90:68–72.
Lee JY, Yoo C, Kim YY. The effect of lateral decubitus position on intraocular pressure in patients with untreated open-angle glaucoma. Am J Ophthalmol. 2013;155:329–35.
Lee TE, Yoo C, Kim YY. Effects of different sleeping postures on intraocular pressure and ocular perfusion pressure in healthy young subjects. Ophthalmology. 2013;120:1565–70.
Kim KN, Jeoung JW, Park KH, Lee DS, Kim DM. Effect of lateral decubitus position on intraocular pressure in glaucoma patients with asymmetric visual field loss. Ophthalmology. 2013;120:731–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
S. Y. Cho, None; Y. Y. Kim, None; C. Yoo, None; T. -E. Lee, None.
About this article

Cite this article
Cho, S.Y., Kim, Y.Y., Yoo, C. et al. Twenty-four-hour efficacy of preservative-free tafluprost for open-angle glaucoma patients, assessed by home intraocular pressure (Icare-ONE) and blood-pressure monitoring. Jpn J Ophthalmol 60, 27–34 (2016). https://doi.org/10.1007/s10384-015-0413-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10384-015-0413-1