
Abstract
Objectives
Several studies have recently demonstrated that only marginal improvements in platelet and leukocyte concentrations are achieved following standard injectable platelet-rich fibrin (i-PRF) protocols. Due to these previous findings, a novel harvesting technique was recently developed to collect higher concentrations of platelets/leukocytes specifically from the buffy coat layer (C-PRF) following faster centrifugation protocols. The aim of this study was to investigate the regenerative properties and effects on growth factor release and cellular activity of PRF collected through this novel harvesting technique compared to standard i-PRF protocols.
Materials and methods
The upper 1-ml layer collected through standard i-PRF protocols at low centrifugation speeds was compared with 1 mL of C-PRF collected from the buffy coat layer following high centrifugation protocols (3000×g for 8 min on a horizontal centrifuge) to specifically concentrate cells within the platelet/leukocyte-rich buffy coat layer. Thereafter, the expression of seven different growth factors, including PDGF-AA, PDGF-AB, PDGF-BB, TGF-β1, VEGF, IGF-1, and EGF, was characterized for up to 10 days. Then, gingival fibroblast biocompatibility was investigated at 24 h (live/dead assay); migration was investigated at 24 h; proliferation was investigated at 1, 3, and 5 days; and the expression of PDGF and TGF-β was investigated at 3 days. Collagen 1 immunostaining was also quantified at 14 days.
Results
At all investigated time periods, a significant increase in growth factor release was observed in C-PRF. In particular, the release of PDGF-AA, TGF-β1, and EGF exhibited the highest increases when compared with that in i-PRF. While both i-PRF and C-PRF exhibited high biocompatibility and induced significantly higher fibroblast migration and proliferation when compared with that of the control tissue culture plastic group, C-PRF showed the greatest potential for cell migration and proliferation. Furthermore, C-PRF induced significantly higher mRNA levels of TGF-β and PDGF levels at 3 days and greater collagen 1 staining when compared with induced by i-PRF.
Conclusions
In the present study, it was found that C-PRF collected specifically from the buffy coat layer following higher centrifugation protocols exhibited an up to a threefold increase in growth factor release when compared with that exhibited by standard i-PRF. This significantly promoted higher gingival fibroblast migration, proliferation, gene expression, and collagen I synthesis.
Clinical relevance
The findings of the present study demonstrate that a more potent formulation of liquid platelet concentrate than that obtained from the upper plasma layer following a short and slow centrifugation protocol (i-PRF protocol) can be obtained for clinical use by specifically harvesting cells in the platelet- and leukocyte-rich buffy coat layer following an 8-min 3000×g centrifugation protocol (C-PRF protocol).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Platelet concentrates, as concentrates of autologous blood-derived growth factors, have been utilized in regenerative medicine and dentistry for over 2 decades [1, 2]. Platelet-rich plasma (PRP) was first developed for widespread use not only in regenerative dentistry but also in maxillofacial surgery, orthopedic surgery, and esthetic medicine [3,4,5,6,7]. Protocols for harvesting PRP involve the use of anticoagulants and high g-forces to selectively separate blood cells based on density. Due to these high g-forces, a top platelet-poor (acellular) layer is typically produced within the upper layer and a platelet-rich (buffy coat; middle) layer and a bottom red blood cell (RBC corpuscle) layer. Since anticoagulants are utilized, the cell layers are separated without coagulating, and the standard centrifugation cycles of specific harvesting kits typically range from 15 min to 1 h. Despite the widespread use of PRP, recently, concerns have been raised due to the finding that anticoagulant incorporation in formulations has been shown to negatively impact tissue regeneration [3, 8, 9].
Over the past decade [10], platelet-rich fibrin (PRF) has gained tremendous momentum, having been utilized for a variety of dental and medical procedures. PRF was developed as a second-generation platelet concentrate with the aim of eliminating the need for anticoagulants [10]. To accomplish this task, centrifugation needs to be carried out much more quickly and efficiently to prevent blood clotting prior to cell layer separation. Following a typical 8–12 min centrifugation period, a three-dimensional fibrin matrix that acts as a scaffold that favors the slow and gradual release of growth factors over time as the fibrin mesh is slowly degraded in the body over a 10–14 day period is produced [11,12,13]. PRF has since been extensively utilized in many fields of regenerative dentistry for the treatment of gingival recessions, intrabony defects, sinus grafting, extraction sockets, and many other conditions [14]. Advantages include faster healing, increased angiogenesis, lower costs (when compared to PRP), and complete immune biocompatibility [15,16,17,18].
In 2017, it was demonstrated that by further reducing centrifugation speed and time and by using centrifugation tubes with more hydrophobic materials (to reduce clotting times), injectable PRF (termed i-PRF) with advantages over PRP was obtained [19]. Furthermore, a number of studies have further demonstrated that the cellular activity of i-PRF is superior to that of PRP [19,20,21,22]. More recently, however, several studies have begun to comment on the surprisingly low yield of isolated platelets and leukocytes following the centrifugation protocols of i-PRF [23, 24]. Although greater cell activity is observed when utilizing i-PRF, the release of several growth factors from PRP, as well as the total platelet yield, is higher [19].
Owing to these combined findings, alternative protocols to further improve the platelet and leukocyte yields of i-PRF have been attempted. For instance, an increase in the centrifugation time from 3 to 4 to 8 min to further accumulate platelets in the upper i-PRF layer has been proposed [25]. Alternatively, an increase in centrifugation speed has also been proposed (2700 rpm (~ 700×g) at the RCF-max; ~ 400×g at the RCF-clot), which has since been shown to lead to higher platelet yields and concentrations [26, 27]. We have previously shown that the production of PRF via horizontal centrifugation (as opposed to conventional fixed-angle centrifugation) leads to up to a fourfold increase in platelet and leukocyte yields [24].
In parallel, a novel technique to quantify cells within platelet concentrates following centrifugation by sequentially pipetting 1 mL layers of blood following centrifugation was proposed [24]. This highly effective quantification method reveals the exact concentration/location of various blood cells in 10 separate layers following centrifugation and provides a tool to directly investigate PRF protocols based on the final cell composition. By utilizing such approaches, it was found that, compared with baseline values, approximately 35% and 30% increases in the yields of total platelets and leukocytes, respectively, were observed when standard i-PRF protocols were followed.
Surprisingly, it was also found that following L-PRF protocols (2700 rpm for 12 min), the majority of cells were found within the buffy coat layer, with the upper 4 mL being completely devoid of cells [28]. There was an approximately tenfold increase in baseline concentrations specifically in this 0.3–0.5 mL buffy coat layer directly above the RBC corpuscle layer produced using higher centrifugation protocols [28]. The PRF obtained from this harvesting technique was given the working name concentrated PRF (C-PRF). It was hypothesized that based on the extensive increase in the yield of platelets and leukocytes, C-PRF would exhibit higher growth factor release as well as superior cellular activity. Therefore, the aim of this study was twofold. First, a new centrifugation protocol was developed with the aim of accumulating the greatest concentrations of platelets and leukocytes within the buffy coat. To achieve this, a horizontal centrifuge was utilized. The second aim was to compare the total growth factor release of PRF obtained through this newly developed C-PRF protocol with that of PRF obtained through the clinically utilized liquid i-PRF protocol over a 10-day period and to investigate the regenerative properties of human gingival fibroblasts in vitro.
Materials and methods
Preparation of i-PRF and C-PRF
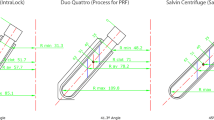
Blood samples were collected from 6 volunteer donors (12 total samples) who gave informed consent, and the blood was then processed for i-PRF and C-PRF preparation. All procedures performed in this study involving human participants were performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. No internal review board (IRB) was required for this study because the human samples were not identified, as previously described (BASEC-Nr: Req-2017-00824) [19]. All blood samples were obtained from members of our laboratory between the ages of 30 and 60. For i-PRF preparation, 2 tubes of 10 mL of whole blood without anticoagulants were centrifuged at 300×g for 5 min on a horizontal centrifuge (5702 Eppendorf, Hamburg, Germany) based on previous findings that horizontal centrifugation protocols generate higher concentrations than those generated by fixed-angle centrifugation protocols [24]. C-PRF protocols were developed utilizing a horizontal centrifuge with a maximum g-force of 3000×g. Utilizing 9-mL plastic white PET tubes (Greiner, Bio-One, USA), the collected blood was centrifuged at 3000×g for 5 min, 8 min, or 12 min to determine the cell layer separation following protocols that utilized a previously described complete blood count quantification system [24]. Following protocol optimization, the 1-mL upper liquid layer of the i-PRF and C-PRF samples were collected from the buffy coat layer (Fig. 1), transferred to 6-well plastic culture dishes containing 5 ml of cell culture media (DMEM; Gibco, Life Technologies, Carlsbad, CA, USA) and processed as described below.

Visual representation of layer separation following either the i-PRF (300×g for 5 min) or C-PRF protocol (3000×g for 8 min). Plasma was collected from the buffy coat region within the 1-mL layer above the RBC layer
Complete blood count analysis of C-PRF
Three volunteers donated 6 tubes of blood for each of the 3 tested protocols and an additional 1 tube of blood that acted as a control. Each pair of tubes was utilized to balance the centrifuge during the centrifugation cycle and centrifuged for 3000×g for 5, 8, or 12 min. All tubes, from the top 1-mL layer through the bottom 1-mL layer, were investigated as previously described [24].
Protein quantification by ELISA
To determine the amount of growth factors released from i-PRF and C-PRF at 15 min, 60 min, 8 h, 1 day, 3 days, and 10 days, samples were placed in an incubator at 37 °C to allow for growth factor release into the culture media. At each time point, 5 mL of culture media was collected, frozen, and replaced with 5 mL of additional culture media. Protein quantification was carried out using ELISA. At the designated time points, PDGF-AA (DY221, range = 15.60–1000 pg/mL), PDGF-AB (DY222, range = 15.60–1000 pg/mL), PDGF-BB (DY220, 31.20–2000 pg/mL), TGF-β1 (DY240, range = 31.20–2000 pg/mL), VEGF (DY293B, range = 31.20–2000 pg/mL), EGF (DY236, range = 3.91–250 pg/mL) and IGF-1 (DY291, range = 31.20–2000 pg/mL) were quantified using an ELISA kit (DuoSet, R&D Systems, Minneapolis, MN, USA) according to the manufacturer’s protocol as previously described [29]. Absorbance was measured at 450 nm and 540 nm using a microplate reader (Tecan Infinite 200 Pro, Tecan Group Ltd., Männedorf, Switzerland), and the difference in the values were used for further calculation.
Cell culture
Platelet concentrates, including i-PRF and C-PRF, were incubated for 3 days, and conditioned media was collected and utilized in future experiments as 20% of the total volume as previously described [19]. Human gingival fibroblasts (HGF-1) were purchased from ATCC (Manassas, VA, USA). All cells were detached from tissue culture plastic using 0.25% EDTA-trypsin (Gibco) prior to reaching confluency. The cells used for experimental seeding were from passages 4–6. The cells were cultured in a humidified atmosphere at 37 °C in growth medium consisting of DMEM (Gibco), 10% fetal bovine serum (FBS; Gibco), and 1% antibiotics (Gibco). The medium was changed 2 times per week. The cells were seeded in 20% conditioned media from i-PRF or C-PRF in growth medium at a density of 10,000 cells per well in 24-well plates for cell viability and proliferation experiments and at a density of 50,000 cells per well in 24-well plates for real-time PCR and collagen staining. Control cells were incubated in DMEM and collected at the same time as the cells incubated in PRF conditioned media.
Cell viability assay
Twenty-four hours after the cells were seeded on a φ13-mm plastic tissue culture coverslips (Sarstedt, Newton, NC, USA), they were evaluated using a live–dead staining assay according to the manufacturer’s protocol (Enzo Life Sciences AG; Lausen, Switzerland). Fluorescence images were quantified with a fluorescence microscope (Nikon Eclipse E800, Nikon, Tokyo, Japan). Thereafter, cell viability was expressed as the percentage of live cells versus dead cells following growth in i-PRF or C-PRF conditioned media in culture.
Cell migration assay
The migration assay was performed using a 24-well plate and polyethylene terephthalate filters with a pore size of 8 μm (ThinCert™, Greiner Bio-One GmhH, Frickenhausen, Germany). After being starved in DMEM containing 0.5% FBS for 12 h, 10,000 resuspended cells were seeded in the upper compartment in DMEM containing 0.5% FBS. The lower compartment of each well was filled with 20% conditioned media in DMEM containing 10% FBS. After 24 h, the cells were fixed with 4% formaldehyde for 2 min. Thereafter, the cells were permeabilized with methanol for 15 min and stained with Giemsa solution (Merck, Darmstadt, Germany) for 20 min. The upper side of the filter membrane was rinsed and gently wiped with a cotton swab to remove the cell debris. The number of cells on the lower side of the filter was counted with the counting tool of a digital microscope (Keyence).
Proliferation assay
HGF-1 cells were quantified by a luminescent cell viability assay (CellTiter-Glo®, Promega, Madison, WI, USA) at 1, 3, and 5 days. At the designated time points, living cells were quantified using a luminescence plate reader (TECAN Infinite 200 Pro).
Real-time PCR analysis
Total RNA was harvested from HGF-1 cells 3 days post-stimulation to investigate the mRNA levels of TGF-β and PDGF-A. Primers and probes for the genes were generated based on the primer sequences shown in Table 1. RNA isolation was performed using a High Pure RNA Isolation Kit (Roche, Basel, Switzerland). A Nanodrop 2000 spectrophotometer (Thermo, Wilmington, DE, USA) was used to quantify total RNA levels. Real-time RT-PCR was performed by the GoScript™ Reverse Transcription system (Promega) and quantified on an Applied Biosystems 7500 Fast machine using GoTaq® qPCR Master Mix (Promega). The ∆∆Ct method was used to calculate gene expression levels normalized to the expression of glyceraldehyde 3-phosphate dehydrogenase (GAPDH).
Collagen immunofluorescence staining
Fourteen days after being seeded on plastic tissue culture coverslips, HGF-1 cells were fixed with 4% formaldehyde for 10 min, permeabilized in PBS containing 0.2% Triton X-100 and blocked in PBS containing 1% bovine serum albumin (BSA, Sigma) for 1 h. Subsequently, the cells were incubated overnight at 4 °C with a mouse monoclonal collagen type I (COL-1) antibody (sc-59772, Santa Cruz, Dallas, TX, USA) diluted 1:200 in PBS containing 1% BSA. After washing with PBS, the cells were incubated for 1 h at 37 °C with a FITC-conjugated mouse IgG secondary antibody (sc-516140, Santa Cruz) diluted 1:100 in PBS containing 1% BSA. Prior to viewing, the samples were mounted with Vectashield containing DAPI nuclear staining (Vector, Burlingame, CA, USA). Images were captured by a Nikon Eclipse E800 fluorescence microscope. The optical density of the fluorescence staining for collagen from 3 independent experiments was quantified using ImageJ software (NIH, Bethesda, MD, USA).
Statistical analysis
All experiments were performed in triplicate, and three independent experiments were performed for each condition. The means and standard errors (SEs) were calculated, and the statistical significance of the data was analyzed using one-way analysis for the cell viability, migration, and real-time PCR analysis experiments and using two-way analysis of variance followed by the Tukey test for the ELISA and proliferation experiments (*, p values < 0.05 was considered significant) by GraphPad Prism 8.2 software (GraphPad Software, Inc., La Jolla, CA, USA).
Results
Optimization of C-PRF protocols
Prior to initiating the C-PRF experiments, protocols of 3000×g for 5 min, 8 min, and 12 min were compared with those of optimizing the accumulation of cells within the buffy coat layer. It was found that the 5-min protocol was unable to concentrate all cells within the buffy coat layer, with the platelets remaining in the upper 4-mL layer (Supplemental Fig. 1A). Following the 8-min protocol, the sequential pipetting method results revealed that the majority of platelets and leukocytes were located within the buffy coat layer 6 region (Fig. 2). No further advantage was observed following the 12-min protocol (Supplemental Fig. 1B). For comparison purposes, a standard i-PRF protocol illustrated in Fig. 2, resulted in a slight concentration of platelets and leukocytes in the upper 1-mL layer from which i-PRF was harvested. Note that many platelets/leukocytes, however, remained in the RBC layers. To harvest C-PRF, a 1-mL layer within this buffy coat layer was collected and processed for further analysis (Fig. 1).

The concentrations of different cell types found in each layer from the 1-mL layer through the 10th 1-mL layer obtained through (A) the i-PRF protocol (300×g for 5 min) and (B) the C-PRF protocol (3000×g for 8 min). Note that in the PRF obtained through the i-PRF protocol, the majority of platelets and leukocytes was located in the 1-mL buffy coat layer. In the PRF obtained through the C-PRF protocol, although a higher concentration of platelets and leukocytes was found in the upper 1-mL layer, the majority of the platelets and leukocytes was actually located in the RBC layers
Growth factor release from i-PRF and C-PRF
In the first set of experiments, the release of growth factors, including PDGF-AA, PDGF-AB, PDGF-BB, TGF-β1, VEGF, EGF, and IGF-1, from i-PRF and C-PRF was investigated by ELISA (Figs. 3 and 4). The release of all growth factors over the entire 10-day (240 h) period was marked and significant. The C-PRF protocols resulted in a significant 2- to 3-fold increase in the release of many of the growth factors investigated. The increases in the release of PDGF-AA, TGF-β1, and EGF from C-PRF compared with those from i-PRF were the most pronounced (Figs. 3 and 4).

Protein quantification of (A) PDGF-AA, (B) PDGF-AB and (C) PDGF-BB at each time point over a 10-day (240 h) period for both PRF obtained through the i-PRF protocol and that obtained through the C-PRF protocol, as determined by ELISA (Data represents means ± SE, *indicates a significant difference between groups (p < 0.05), * indicates significantly higher than the other group (p < 0.05))

Protein quantification of (A) TGF-β1, (B) VEGF (C) EGF and (D) IGF-1 at each time point over a 10-day (240-h) period for both PRF obtained through the i-PRF protocol and that obtained through the C-PRF protocol, as determined by ELISA (Data represents means ± SE, *indicates significantly higher than the other group (p < 0.05))
Biocompatibility of i-PRF and C-PRF with human gingival fibroblasts
In the first cell culture experiment, the effects of i-PRF and C-PRF on the cell viability of human gingival fibroblasts were investigated. It was found that both i-PRF and C-PRF demonstrated excellent cell biocompatibility, as demonstrated by the high percentage of living cells (> 95%, green cells, Fig. 5) and few observable dead cells (red cells). It was therefore concluded that both i-PRF and C-PRF were fully biocompatible in the present in vitro cell culture model (Fig. 5).

Live/dead assay of human gingival fibroblasts treated with i-PRF and C-PRF at 24 h, including the merged fluorescence images of live/dead staining. The viable cells appear green, and the dead cells appear red. Data represents means ± SE
Influence of i-PRF and C-PRF on human gingival fibroblast activity
Following the confirmation of high cell survival in the biocompatibility assays, the effects of i-PRF and C-PRF on gingival fibroblast migration and proliferation and the mRNA expression of TGF-β and PDGF-A were then investigated (Fig. 6). It was first found that while i-PRF induced a twofold increase in cell migration when compared with that observed in the control, a significantly higher fourfold increase was observed when cells were cultured with C-PRF (Fig. 6A). Furthermore, compared with i-PRF, C-PRF also induced significantly higher cell proliferation 3 and 5 days after seeding (Fig. 6B). The analysis of mRNA levels revealed that compared with the control both i-PRF and C-PRF were able to significantly upregulate TGF-β 3 days after seeding, inducing a relative 50% increase in gene expression (Fig. 6C). Significant 250% and 400% increases in the PDGF-A mRNA level were observed for i-PRF and C-PRF, respectively (Fig. 6D). The analysis of COL1 immunostaining revealed that C-PRF was able to significantly increase COL1A staining when compared with that in the i-PRF and control tissue culture plastic groups (Fig. 6E, F).

(A) Cell migration at 24 h and (B) cell proliferation at 1, 3, and 5 days in HGF-1 cells. (C, D) Real-time PCR analysis of the mRNA levels of (C) TGF-β and (D) PDGF in human gingival fibroblasts treated with i-PRF and C-PRF at 3 days. (E) Quantitative and (F) representative staining of collagen I at 14 days (data represents means ± SE, * indicates significantly higher than the control group (p < 0.05), ** indicates significantly higher than all other groups (p < 0.05), # indicates significantly lower than all groups (p < 0.05))
Discussion
The use of regenerative modalities in dentistry has gradually become more prominent in recent years with the aim of improving the standard of care of a variety of treatment modalities in the fields of periodontology and implant dentistry. One such proposed method to regenerate lost tissues is the use of platelet concentrates, including PRP and PRF, which both aim to concentrate supraphysiological doses of autologous growth factors derived from the patient’s own blood [29, 30].
In 2017, it was shown that i-PRF favored the formation of a stable fibrin clot, which has been shown to increase the slow and gradual release of growth factors over time [19]. Nevertheless, the release of lower quantities and concentrations of growth factors than expected from i-PRF have been reported. Since then, it has been demonstrated that the initially developed i-PRF protocols utilizing a fixed-angle rotor at low g-forces are unable to concentrate platelets and leukocytes to sufficient levels, generating only an approximately 35% total platelet yield following centrifugation. For these reasons, attempts to improve i-PRF formulations by either altering the time of centrifugation or the g-forces used or by utilizing horizontal centrifugation with modifications to the protocols [24].
In the present study, a novel harvesting technique whereby total platelets and leukocytes are specifically concentrated within the buffy coat layer following higher speed centrifugation (3000×g for 8 min) was developed. This protocol also does not utilize anticoagulants and produces PRF that remains in liquid formulation following centrifugation. The results revealed found that over 99% of total platelets was obtained and that the leukocyte yield was greater than 80%. Previously, it was shown that switching from a fixed-angle centrifuge to a horizontal centrifuge most prominently improved the concentration of leukocytes. Leukocytes are immune cells that play vastly important roles in host immune system defense as well as tissue regeneration by directing and recruiting various cell types during the wound healing process [31,32,33]. Following the development of adequate protocols to concentrate platelets and leukocytes within a concentrated volume within the buffy coat layer for the generation of C-PRF (Fig. 2), a comparative series of in vitro experiments was performed to determine the effect of C-PRF on growth factor release and gingival fibroblast activity.
It was first found that the release of all tested growth factors markedly increase over a 10-day period when compared with that in the i-PRF group. Furthermore, C-PRF induced a fourfold significant increase in cell migration and proliferation in gingival fibroblasts when compared with that induced by i-PRF and further stimulated the gene expression of regenerative growth factors and the synthesis of collagen.
One interesting finding was the visible changes in the plasma layer following higher centrifugation protocols. It was observed that the upper plasma layer was typically clearer than the white layer visible within the buffy coat layer. This layer was generally found directly above the red corpuscle layer and required careful harvesting. In the present study, an 18–21 gauge needle was needed to collect the C-PRF. It is also interesting to note that in the present study, a total volume of 1 mL was collected from the plasma layer for all samples. However, the PRF buffy coat typically ranges from 0.2 to 0.3 mL prior to harvesting (data under review). Therefore, clinicians have the ability to modify the final concentration of platelets and leukocytes by increasing or decreasing the total volume while maintaining a relatively fixed cell yield.
The present study further highlights the need for future research in the field. To date, it remains relatively unknown the most optimal protocol available with a wide range of available centrifugation protocols and hardware available on the market [34]. Furthermore, most systematic reviews of randomized clinical studies have demonstrated that PRF more favorably induces soft tissue regeneration when compared with bone regeneration [14]. There remains great interest in continuously and steadily increasing our understanding of platelet concentrates and the role of the various cell types found in their formulations. Currently, there remains a need to develop PRF tubes that further delay the clotting properties of liquid i-PRF and/or C-PRF while simultaneously eliminating the need for unnecessary anticoagulants or the addition of other nonautogenous to their formulations. Furthermore, animal and clinical studies investigating the ability of C-PRF to lead to further clinical improvements in wound healing remain necessary.
Conclusion
In summary, the results of the present study demonstrate a successful harvesting technique for the collection of concentrated PRF, demonstrating improved platelet and leukocyte concentrations when compared with those obtained through conventional i-PRF protocols. C-PRF induced an up to two-to-threefold increase in growth factor release during a 10-day period and further elicited fourfold increases in gingival fibroblast migration, PDGF gene expression, and collagen I synthesis when compared with that induced by PRF obtained through conventional approaches. Future animal and human studies are now needed to specifically investigate the regenerative potential of C-PRF to further characterize the impact of C-PRF in the clinic.
References
Chow TW, McIntire LV, Peterson DM (1983) Importance of plasma fibronectin in determining PFP and PRP clot mechanical properties. Thromb Res 29:243–248
Delaini F, Poggi A, Donati MB (1982) Enhanced affinity for arachidonic acid in platelet-rich plasma from rats with Adriamycin-induced nephrotic syndrome. Thromb Haemost 48:260–262
Marx RE (2004) Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg 62:489–496
Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR (1998) Platelet-rich plasma: growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 85:638–646
Cai YZ, Zhang C, Lin XJ (2015) Efficacy of platelet-rich plasma in arthroscopic repair of full-thickness rotator cuff tears: a meta-analysis. J Shoulder Elbow Surg 24:1852–1859. https://doi.org/10.1016/j.jse.2015.07.035
Meheux CJ, McCulloch PC, Lintner DM, Varner KE, Harris JD (2016) Efficacy of intra-articular platelet-rich plasma injections in knee osteoarthritis: a systematic review. Arthroscopy 32:495–505. https://doi.org/10.1016/j.arthro.2015.08.005
Singh B, Goldberg LJ (2016) Autologous platelet-rich plasma for the treatment of pattern hair loss. Am J Clin Dermatol 17:359–367. https://doi.org/10.1007/s40257-016-0196-2
Anfossi G, Trovati M, Mularoni E, Massucco P, Calcamuggi G, Emanuelli G (1989) Influence of propranolol on platelet aggregation and thromboxane B2 production from platelet-rich plasma and whole blood. Prostaglandins Leukot Essent Fat Acids 36:1–7
Fijnheer R, Pietersz RN, de Korte D, Gouwerok CW, Dekker WJ, Reesink HW, Roos D (1990) Platelet activation during preparation of platelet concentrates: a comparison of the platelet-rich plasma and the buffy coat methods. Transfusion 30:634–638
Choukroun J, Adda F, Schoeffler C, Vervelle A (2001) Une opportunité en paro-implantologie: le PRF. Implantodontie 42:e62
Toffler M (2014) Guided bone regeneration (GBR) using cortical bone pins in combination with leukocyte-and platelet-rich fibrin (L-PRF). Compendium of Continuing Educ Dentist 35:192–198
Lekovic V, Milinkovic I, Aleksic Z, Jankovic S, Stankovic P, Kenney E, Camargo P (2012) Platelet-rich fibrin and bovine porous bone mineral vs. platelet-rich fibrin in the treatment of intrabony periodontal defects. J Periodontal Res 47:409–417
Shivashankar VY, Johns DA, Vidyanath S, Sam G (2013) Combination of platelet rich fibrin, hydroxyapatite and PRF membrane in the management of large inflammatory periapical lesion. J Conserv Dent 16:261
Miron RJ, Zucchelli G, Pikos MA, Salama M, Lee S, Guillemette V, Fujioka-Kobayashi M, Bishara M, Zhang Y, Wang HL, Chandad F, Nacopoulos C, Simonpieri A, Aalam AA, Felice P, Sammartino G, Ghanaati S, Hernandez MA, Choukroun J (2017) Use of platelet-rich fibrin in regenerative dentistry: a systematic review. Clin Oral Investig 21:1913–1927. https://doi.org/10.1007/s00784-017-2133-z
Medina-Porqueres I, Alvarez-Juarez P (2015) The efficacy of platelet-rich plasma injection in the management of hip osteoarthritis: a systematic review protocol. Musculoskelet Care 14:121–125. https://doi.org/10.1002/msc.1115
Salamanna F, Veronesi F, Maglio M, Della Bella E (2015) New and emerging strategies in platelet-rich plasma application in musculoskeletal regenerative procedures: general overview on still open questions and outlook. Biomed Res Int 2015:846045. https://doi.org/10.1155/2015/846045
Albanese A, Licata ME, Polizzi B, Campisi G (2013) Platelet-rich plasma (PRP) in dental and oral surgery: from the wound healing to bone regeneration. Immun Ageing 10:23. https://doi.org/10.1186/1742-4933-10-23
Panda S, Doraiswamy J, Malaiappan S, Varghese SS, Del Fabbro M (2014) Additive effect of autologous platelet concentrates in treatment of intrabony defects: a systematic review and meta-analysis. J Investig Clin Dent 7:13–26. https://doi.org/10.1111/jicd.12117
Miron RJ, Fujioka-Kobayashi M, Hernandez M, Kandalam U, Zhang Y, Ghanaati S, Choukroun J (2017) Injectable platelet rich fibrin (i-PRF): opportunities in regenerative dentistry? Clin Oral Investig 21:2619–2627. https://doi.org/10.1007/s00784-017-2063-9
Abd El Raouf M, Wang X, Miusi S, Chai J, Mohamed AbdEl-Aal AB, Nefissa Helmy MM, Ghanaati S, Choukroun J, Choukroun E, Zhang Y, Miron RJ (2017) Injectable-platelet rich fibrin using the low speed centrifugation concept improves cartilage regeneration when compared to platelet-rich plasma. Platelets. https://doi.org/10.1080/09537104.2017.1401058
Wang X, Zhang Y, Choukroun J, Ghanaati S, Miron RJ (2017) Behavior of gingival fibroblasts on titanium implant surfaces in combination with either injectable-PRF or PRP. Int J Mol Sci. https://doi.org/10.3390/ijms18020331
Wang X, Zhang Y, Choukroun J, Ghanaati S, Miron RJ (2018) Effects of an injectable platelet-rich fibrin on osteoblast behavior and bone tissue formation in comparison to platelet-rich plasma. Platelets 29:48–55. https://doi.org/10.1080/09537104.2017.1293807
Varela HA, Souza JCM, Nascimento RM, Araujo RF Jr, Vasconcelos RC, Cavalcante RS, Guedes PM, Araujo AA (2019) Injectable platelet rich fibrin: cell content, morphological, and protein characterization. Clin Oral Investig 23:1309–1318. https://doi.org/10.1007/s00784-018-2555-2
Miron RJ, Chai J, Zheng S, Feng M, Sculean A, Zhang Y (2019) A novel method for evaluating and quantifying cell types in platelet rich fibrin and an introduction to horizontal centrifugation. J Biomed Mater Res A 107:2257–2271. https://doi.org/10.1002/jbm.a.36734
Wend S, Kubesch A, Orlowska A, Al-Maawi S, Zender N, Dias A, Miron RJ, Sader R, Booms P, Kirkpatrick CJ, Choukroun J, Ghanaati S (2017) Reduction of the relative centrifugal force influences cell number and growth factor release within injectable PRF-based matrices. J Mater Sci Mater Med 28:188. https://doi.org/10.1007/s10856-017-5992-6
Castro AB, Cortellini S, Temmerman A, Li X, Pinto N, Teughels W, Quirynen M (2019) Characterization of the leukocyte- and platelet-rich fibrin block: release of growth factors, cellular content, and structure. Int J Oral Maxillofac Implants 34:855–864. https://doi.org/10.11607/jomi.7275
Cortellini S, Castro AB, Temmerman A, Van Dessel J, Pinto N, Jacobs R, Quirynen M (2018) Leucocyte- and platelet-rich fibrin block for bone augmentation procedure: a proof-of-concept study. J Clin Periodontol 45:624–634. https://doi.org/10.1111/jcpe.12877
Miron RJ, Chai J, Zhang P, Li Y, Wang Y, Mourao C, Sculean A, Fujioka Kobayashi M, Zhang Y (2019) A novel method for harvesting concentrated platelet-rich fibrin (C-PRF) with a 10-fold increase in platelet and leukocyte yields. Clin Oral Investig. https://doi.org/10.1007/s00784-019-03147-w
Kobayashi E, Fluckiger L, Fujioka-Kobayashi M, Sawada K, Sculean A, Schaller B, Miron RJ (2016) Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin Oral Investig 20:2353–2360. https://doi.org/10.1007/s00784-016-1719-1
Fujioka-Kobayashi M, Miron RJ, Hernandez M, Kandalam U, Zhang Y, Choukroun J (2016) Optimized platelet rich fibrin with the low speed concept: growth factor release, biocompatibility and cellular response. J Periodontol. https://doi.org/10.1902/jop.2016.160443
Bielecki T, Dohan Ehrenfest DM, Everts PA, Wiczkowski A (2012) The role of leukocytes from L-PRP/L-PRF in wound healing and immune defense: new perspectives. Curr Pharm Biotechnol 13:1153–1162
Martin P (1997) Wound healing--aiming for perfect skin regeneration. Science 276:75–81
Barrick B, Campbell EJ, Owen CA (1999) Leukocyte proteinases in wound healing: roles in physiologic and pathologic processes. Wound Repair Regen 7:410–422
Miron RJ, Xu H, Chai J, Wang J, Zheng S, Feng M, Zhang X, Wei Y, Chen Y, Mourao C, Sculean A, Zhang Y (2019) Comparison of platelet-rich fibrin (PRF) produced using 3 commercially available centrifuges at both high (~700 g) and low (~200 g) relative centrifugation forces. Clin Oral Investig 24:1171–1182. https://doi.org/10.1007/s00784-019-02981-2
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Richard J Miron holds intellectual property on concentrated PRF. All other authors declare no conflict of interest.
Ethical approval
No ethical approval was required for this study, as the human samples were not identified in this study.
Informed consent
For this type of study, informed consent was not required, as no human or animal subjects were utilized.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(PNG 5805 kb)
Rights and permissions
About this article

Cite this article
Fujioka-Kobayashi, M., Katagiri, H., Kono, M. et al. Improved growth factor delivery and cellular activity using concentrated platelet-rich fibrin (C-PRF) when compared with traditional injectable (i-PRF) protocols. Clin Oral Invest 24, 4373–4383 (2020). https://doi.org/10.1007/s00784-020-03303-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-020-03303-7