
Abstract
This narrative review aims to summarize the recent findings on the adjuvant application of creatine supplementation in the management of age-related deficits in skeletal muscle, bone and brain metabolism in older individuals. Most studies suggest that creatine supplementation can improve lean mass and muscle function in older populations. Importantly, creatine in conjunction with resistance training can result in greater adaptations in skeletal muscle than training alone. The beneficial effect of creatine upon lean mass and muscle function appears to be applicable to older individuals regardless of sex, fitness or health status, although studies with very old (>90 years old) and severely frail individuals remain scarce. Furthermore, there is evidence that creatine may affect the bone remodeling process; however, the effects of creatine on bone accretion are inconsistent. Additional human clinical trials are needed using larger sample sizes, longer durations of resistance training (>52 weeks), and further evaluation of bone mineral, bone geometry and microarchitecture properties. Finally, a number of studies suggest that creatine supplementation improves cognitive processing under resting and various stressed conditions. However, few data are available on older adults, and the findings are discordant. Future studies should focus on older adults and possibly frail elders or those who have already experienced an age-associated cognitive decline.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Older individuals commonly experience losses of cognitive performance, bone mass, muscle mass, and functionality. These features largely contribute to the development of frailty, which is a complex multidimensional syndrome characterized by loss of reserves (e.g., energy, physical capacity, cognition health) that gives rise to vulnerability (Hogan et al. 2003). Ultimately, this condition can predispose to poor quality of life, impaired performance in activities of daily living, increased risk of fall and consequently, mortality (Ruiz et al. 2008; Tinetti et al. 1988). There are only a few strategies capable of attenuating age-related physiological decline and the development of frailty in senescence. Exercise training has been thought to be the cornerstone in the prevention and treatment of this condition (Ferri et al. 2003). Moreover, there is strong evidence pointing out the efficacy of specific dietary interventions in adding to the well-known beneficial effects of training to older individuals, with proteins, amino acids and creatine being the most studied nutrients in this context (Gualano et al. 2014; Tieland et al. 2012). Whilst a number of recent reviews have addressed the therapeutic role of increased dietary intake of proteins and amino acids as a measure to counteract frailty in elderly (Bauer et al. 2013; Breen and Phillips 2011; Wall et al. 2014), much less attention has been given to creatine.
The creatine/phosphorylcreatine system plays a crucial bioenergetic role in some tissues with high metabolic demand (e.g., skeletal muscle, bone, and brain), by transferring the N-phosphoryl group from phosphorylcreatine to adenosine diphosphate (ADP) to re-synthesize adenosine triphosphate (ATP), via a reversible reaction catalyzed by creatine kinase (CK). Furthermore, the creatine/phosphorylcreatine system can also act as a spatial energy buffer to shuttle high-energy phosphates between mitochondria and cellular ATP utilization sites (Gualano et al. 2012; Wallimann and Hemmer 1994; Wallimann et al. 1977, 1992, 2011; Wyss and Kaddurah-Daouk 2000). Creatine supplementation is considered an efficient strategy in improving energy provision in excitable tissues. In addition, a growing body of evidence supports the role of creatine in enhancing training volume, thereby maximizing systemic exercise adaptations (for comprehensive reviews, see (Gualano et al. 2009, 2012; Wallimann et al. 2011). Therefore, either “directly” (by supplying extra energy to a target tissue) or “indirectly” (by improving training quality), creatine has emerged as a relevant dietary intervention able to partially offset frailty in the elderly. This narrative review aims to summarize the recent findings on the application of creatine supplementation as an adjuvant therapy in the management of age-related deficits in muscle, bone and brain metabolism in older individuals.
Creatine supplementation and skeletal muscle
Exercise training has been considered one of the most efficient interventions to counteract the decline in muscle mass and function in older individuals (Ferri et al. 2003). Furthermore, there is a growing body of evidence showing that nutritional strategies may be effective in sparing muscle mass in this population, with creatine supplementation being a case in point (Rawson and Venezia 2011). The next sections will cover the main potential mechanisms behind the anabolic effect of creatine, the possible aging-related deficiency in muscle creatine content, the response of aging muscle to creatine accumulation following dietary creatine intake, and the recent clinical findings concerning creatine supplementation on muscle mass and function in older individuals.
What are the mechanisms underlying the anabolic effect of creatine?
There are a few potential mechanisms to explain the anabolic effect of creatine in skeletal muscle. It has been speculated that creatine supplementation could elicit gains in muscle mass through the activation of a number of anabolic signalling molecules. This premise relies on the fact that creatine is osmotically active since it is taken up into target cells by a specialized 2Na+:1Cl−:1 creatine cotransporter (CrT solute carrier SLC6A8) (Guimbal and Kilimann 1993) and hence, may induce cellular swelling, which may act as a trigger to increase the expression of genes and proteins linked to muscle hypertrophy (Parise et al. 2001; Safdar et al. 2008). In fact, a microarray study revealed that a 10-day creatine supplementation regimen was able to modulate mRNA content of genes and protein content of kinases involved in osmosensing, which could stimulate genes related to anabolic signal transduction (Safdar et al. 2008). Supporting these findings, an experimental study showed that five days of creatine supplementation increased muscle mRNA expression of insulin growth factor (IGF)-I and IGF-2 at rest, but not during or following exercise (Deldicque et al. 2005). Moreover, creatine was able to increase the phosphorylation state of eukaryotic translation initiation factor eIF4E-binding protein 1 (4E-BP1) versus placebo 24 h following an exercise session (Deldicque et al. 2005). Importantly, the role of creatine supplementation in stimulating IGF-1 expression was confirmed by others (Burke et al. 2008). Collectively, these data suggested that creatine supplementation could facilitate muscle anabolism by increasing the expression of growth factors and the phosphorylation of anabolic signalling proteins.
Of particular interest to older populations, satellite cells and their myogenic regulatory factors also seem to be responsive to creatine supplementation. For instance, 12 weeks of creatine supplementation along with resistance training increased mRNA expression of myogenic regulatory factors (i.e., myogenin and MRF-4) in untrained males (Willoughby and Rosene 2003). In agreement with these findings, an in vitro study revealed that creatine induced differentiation of myogenic satellite cells (Vierck et al. 2003). These data were corroborated by a subsequent experimental study in which creatine supplementation enhanced satellite cell mitotic activity following compensatory hypertrophy, which was induced in rat plantaris muscle by removing the soleus and gastrocnemius muscles (Dangott et al. 2000). Importantly, findings from a human study demonstrated that 16 weeks of creatine supplementation in combination with resistance training amplified the training-induced increase in satellite cell number and myonuclei concentration in skeletal muscle fibers, which could allow for enhanced muscle fiber growth in response to strength training as typically seen after creatine intake (Olsen et al. 2006).
It is currently controversial as to whether the anabolic effect of creatine supplementation is due to a “direct” action of creatine on the skeletal muscle or an “indirect” effect of creatine maximizing the anabolic stimulus of training. Two studies using isotopic techniques (the gold-standard for measuring protein balance) did not show any additional benefit of short-term creatine supplementation (i.e., up to 5 days), combined or not with a resistance training session, on protein balance in healthy young individuals (Louis et al. 2003a, b), suggesting that acute creatine intake may be unable to modulate either fractional protein synthesis or protein degradation in humans, despite the “pro-anabolic” molecular responses commonly reported in the literature (Deldicque et al. 2005; Burke et al. 2008; Willoughby and Rosene 2003). These studies favor the hypothesis that, at least in young humans, the inclusion of regular training appears to be necessary to cause the hypertrophic stimulus observed with creatine supplementation. Notably, when training load was deliberately equalized in both creatine and placebo groups during a resistance-training program, the previously claimed effect of this dietary supplement on muscle mass or function was no longer observed (Syrotuik et al. 2000). This further supports the notion that the anabolic effects of creatine supplementation (both at the molecular and phenotype level) may be primarily mediated by an enhanced training stimulus. Importantly, most of these experimental and clinical studies comprised young individuals; therefore, the potential mechanisms by which creatine supplementation may increase lean mass and function in elderly subjects remain largely unexplored.
Is muscle creatine content reduced in the elderly?
There is evidence suggesting that muscle creatine content may fluctuate as a function of lifespan. Some investigations suggested that muscle creatine content could be decreased in older individuals when compared with their younger peers (Forsberg et al. 1991; Moller et al. 1980), although conflicting data do exist (Kent-Braun and Ng 2000; Rawson et al. 2002). The mechanisms underlying a potential aging-induced muscle creatine reduction are multiple and may involve: (a) preferential Type II fiber atrophy, which has been shown to have greater phosphorylcreatine content than Type I fibers; (b) progressive reduction of meat consumption, which is the primary dietary source of creatine; (c) reduction in physical activity levels, which may be itself implicated in Type II fiber atrophy (Rawson and Venezia 2011; Tesch et al. 1989). Noticeably, creatine transporter (CreaT) protein content was shown to be unaffected in older individuals (Tarnopolsky et al. 2003b), suggesting that aging per se may not be responsible for reduced muscle creatine content; rather, age-associated changes in behavior (e.g., insufficient physical activity levels and meat intake) seem to better explain any possible reduction in muscle creatine content. To our knowledge, there are no longitudinal studies confirming that senescence leads to decreased muscle creatine content, nor are there any cross-sectional studies controlling all the confounding variables that could influence any possible difference in creatine content (if any) in older and younger subjects.
Can creatine supplementation increase muscle creatine content in the elderly?
There are controversial results regarding the efficacy of creatine supplementation in augmenting muscle creatine content in older individuals, possibly due to the fact that baseline creatine content (a major factor inversely related to muscle creatine accretion) has varied among studies (Rawson et al. 2002; Smith et al. 1998). However, the existing findings generally demonstrate that post-supplementation muscle creatine may reach similar values in younger and older individuals alike, suggesting an efficient response in the elderly (Brose et al. 2003; Eijnde et al. 2003; Rawson et al. 2002; Smith et al. 1998). This assumption, however, is based on a limited number of investigations. Rawson and Venezia (2011) reviewed four studies involving older individuals supplemented with creatine and found increased muscle creatine content in all of them (+5 to 36 %), irrespective of sex, fitness status or supplementation protocol (i.e., acute or chronic regimen, with doses varying from 5 to 20 g day−1) (Brose et al. 2003; Eijnde et al. 2003; Rawson et al. 2002; Smith et al. 1998). However, the large inter-individual variation with respect to muscle creatine accretion suggests that some older individuals may be unresponsive to creatine supplementation, a finding which has also been reported in younger adults (Syrotuik and Bell 2004). Data suggest that a higher proportion of Type II fibers and greater fiber cross-sectional area are determining factors for muscle creatine accumulation after creatine supplementation in young individuals (Syrotuik and Bell 2004). Whether these factors (or others) play a role in creatine accumulation in older individuals needs further investigation.
Can creatine supplementation improve muscle mass and function in the elderly?
In a meta-analysis published in 2003, 43 out of 67 studies showed that creatine supplementation led to increased lean and/or body mass in young and middle-aged adults (Branch 2003). Interestingly, these data may also hold true for older adults. A more recent meta-analysis comprising 357 older adults demonstrated that creatine supplementation during resistance training can enhance muscle mass gain, strength, and functional performance over resistance training alone (Devries and Phillips 2014). This conclusion was confined to studies involving healthy older individuals, due to the paucity of investigations with frailer individuals at the time of the publication. However, recent data have shown that creatine supplementation may also improve muscle mass and function in older individuals with physical impairments. For example, a six-month randomized controlled trial demonstrated that creatine supplementation combined with resistance training was capable of increasing appendicular lean mass, maximal strength and muscle function to a greater extent than resistance training or creatine supplementation alone in vulnerable older individuals (i.e., physically inactive and with disease symptoms). Interestingly, the incidence of sarcopenia throughout the trial was lower in the creatine versus placebo groups (Gualano et al. 2014).
Short-term creatine supplementation (i.e., 5–7 days), even without exercise training, has been shown to be sufficient to increase total body mass (likely due to water retention), enhance fatigue resistance, increase muscle strength, or improve the performance of activities of daily living in older individuals (Gotshalk et al. 2008; Rawson and Clarkson 2000; Rawson et al. 1999; Stout et al. 2007). Moreover, the combination of creatine supplementation and resistance training seemed to act synergistically in producing greater effects in skeletal muscle than resistance training alone (Gualano et al. 2014; Neves et al. 2011; Tarnopolsky et al. 2007; Wilkinson et al. 2015).
It is notable that some studies have failed to find beneficial effects of creatine supplementation on body composition (Bermon et al. 1998; Gualano et al. 2010; Rawson et al. 1999), exercise tolerance (Jakobi et al. 2001), and muscle function (Bermon et al. 1998; Rawson and Clarkson 2000; Rawson et al. 1999) in elderly individuals. According to Rawson and Venezia (2011), a number of factors may contribute to the discordance in the literature, such as: (a) low sample sizes (i.e., n ≤ 25), (b) short-term follow-ups (i.e., ≤14 weeks); (c) co-supplementation of creatine with other dietary aids (i.e., protein and conjugated linoleic acid); (d) samples excessively heterogeneous (i.e., age between 56 and 71 years); (e) incomplete phenotypical characterization of samples (i.e., no clear description on physical activity level, chronic diseases, and use of medications). The conduct of high-quality, adequately powered, randomized controlled trials remains imperative to determine under which conditions creatine supplementation can benefit elderly populations.
Although gains in lean mass have been commonly attributed to creatine supplementation (Devries and Phillips 2014), the current literature does not allow a definitive conclusion as to what extent creatine-induced water retention contributes to these findings. There is limited evidence showing that creatine supplementation, when combined with resistance training, can promote morphological changes in skeletal muscle, including increases in Type I, IIa and IIx fibers (Brose et al. 2003). However, it is conceivable that any increases in lean mass or body mass observed after short-term creatine supplementation (i.e., up to 7 days) are mainly accounted for by intracellular water retention rather than accretion of contractile proteins. In medium- to long-term interventions (i.e., months to years), particularly in the presence of resistance training, it is possible that water retention plays a gradually less important role in lean mass gains. Prospective studies involving accurate muscle morphological measures are necessary to confirm this speculation.
A recent meta-analysis revealed that resistance-trained young individuals experienced greater gains in lean body mass and muscle strength when whey proteins were consumed within a multi-ingredient supplement containing creatine, when compared to the ingestion of an iso-energetic equivalent carbohydrate or non-whey protein supplement (Naclerio and Larumbe-Zabala 2015). Studies involving older individuals co-supplementing with creatine and proteins are scarce and contradictory, possessing small samples, with short-term follow-ups, and with heterogeneous outcomes and experimental designs [Bemben et al. 2010; Candow et al. 2008; Eliot et al. 2008; Villanueva et al. 2014; Collins et al. 2016 (in press)]. The potential role of co-supplementation with creatine, amino acids and/or proteins in sparing muscle mass and improving functionality in older individual merits further investigation.
Further to its anabolic effects, creatine supplementation appears to mediate other physiological and molecular responses in the skeletal muscle that could be advantageous to older individuals. For instance, creatine supplementation in association with a training program was shown to improve glycemic control in older type-2 diabetic patients (Gualano et al. 2010). Creatine-induced glucose uptake was attributed to increases in muscle AMP-activated protein kinase (AMPK) protein expression (Alves et al. 2012a) and glucose transporter type-4 (GLUT-4) translocation (Gualano et al. 2010). Given that insulin resistance is a common feature in older populations, these findings reveal a potentially novel therapeutic role of dietary creatine intake concomitantly to training in the elderly.
To summarize this section, acute and chronic creatine supplementation can improve lean mass and muscle function in older populations. Importantly, creatine in conjunction with resistance training can result in greater adaptations in skeletal muscle as compared with resistance training alone (Aguiar et al. 2013; Alves et al. 2013; Candow et al. 2008; Gualano et al. 2014; Neves et al. 2011; Tarnopolsky et al. 2007; Wilkinson et al. 2015). The beneficial effect of creatine upon lean mass and muscle function appears to be applicable to older individuals, regardless of sex, fitness or health status, although studies with very old (>90 years) and severely frail individuals remain scarce and the underlying muscle mechanisms are unclear (Fig. 1 illustrates the potential effects of creatine supplementation with or without training in the skeletal muscle). The optimal supplementation protocol to elicit the greatest anabolic stimulus remains unknown, with recent evidence showing that doses as low as 1 g day−1 of creatine (which provided two to threefold increases in the daily amount of dietary creatine) for 12 months were insufficient to induce any gains in lean mass or function in postmenopausal women (Lobo et al. 2015); studies employing higher-dose protocols may shed light on a possible dose–response to creatine supplementation in this population. Finally, further larger studies testing the effects of co-supplementation with creatine and other potential anabolic nutrients (e.g., proteins and amino acids) in older individuals remain necessary.

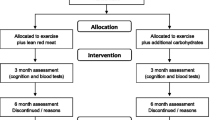
Potential molecular, biochemical and physiological effects of creatine supplementation in the skeletal muscle. Dietary creatine can be taken up by skeletal muscle via a specific transporter (CreaT), and, hence, increase muscle creatine content (both in younger and older individuals). Increased muscle creatine content could lead to extracellular water absorption via osmosis to restore intramuscular protein levels. The resulting increase in mechanical stress caused by the expansion in intracellular water could activate osmosensing genes, which could act as an anabolic stimulus for protein synthesis. Additionally, increased muscle creatine could activate myogenic regulatory factors (i.e., MRF4 and myogenin), which, in turn, could promote activation, proliferation, and differentiation of satellite cells, which are thought to increase myonuclei population improving the machinery for myofibrillar protein synthesis. Creatine supplementation could also enhance myofibrillar protein synthesis by increasing the expression of genes and proteins involved in classical anabolic signalling (e.g., IGF-1 and mTOR expression). Importantly, increased muscle creatine content could enhance training quality, which could facilitate complex mechanotransduction processes (including those aforementioned), ultimately resulting in increased myofibrillar protein synthesis. Finally, creatine supplementation could increase AMPK expression, which could lead to GLUT-4 translocation; this mechanism could explain the effect of creatine supplementation in improving glucose uptake. Whether these molecular responses are mediate by energy buffering, physiochemical attributes of the compound, cell volume regulation, or creatine intake’s direct influence on cellular metabolism via gene modulation remain unclear; nor is currently known as to which extension creatine supplementation per se (without training) can effectively trigger phenotypical adaptions (e.g., increased muscle mass). All of these potential mechanisms need further confirmation in older individuals. CreaT creatine transporter, GLUT-4 glucose transporter type-4, AMPK Adenosine Monophosphate-activated protein kinase, 4-EBP1 eukaryotic translation initiation factor eIF4E-binding protein 1, IGF-1 insulin growth factor-1, Akt protein kinase B, p70 S6K p70 ribosomal S6 protein kinase, mTOR mammalian target of rapamycin, sat. cell satellite cell, prot protein, reg regulatory, Cr creatine. References can be found in the text
Creatine supplementation and bone
Creatine supplementation has potential to affect bone as phosphorylcreatine is used to resynthesize ATP through the creatine kinase reaction in bone cells (Wallimann and Hemmer 1994). Creatine added to cell culture medium increases the metabolic activity, differentiation and mineralization of osteoblast cells involved in bone formation (Gerber et al. 2005). Osteoblasts contain receptor activator for the nuclear factor-kappaB ligand (RANKL) which binds to RANK on osteoclasts precursor cells, stimulating differentiation of these cells into mature osteoclasts (i.e. cells involved in bone resorption) (Leibbrandt and Penninger 2009). This normally activates osteoclasts, so that bone formation is coupled to resorption. In this way, bone constantly turns over in a cycle of remodeling. Increased osteoblast cell activity stimulates the production of osteoprotegerin (OPG) which acts as a decoy receptor for RANKL, preventing RANKL binding with RANK and therefore inhibiting osteoclast cell differentiation, resulting in less bone resorption (Yasuda et al. 1998). Through this activation of osteoblasts (Gerber et al. 2005) creatine may, therefore, also inhibit osteoclasts. In fact, there is evidence that abundance of the brain-type cytoplasmic creatine kinase (Ckb) is highly increased during osteoclastogenesis, and that decreasing Ckb abundance by RNA interference or blocking its enzymatic activity with cyclocreatine (i.e., a synthetic creatine analog), suppressed the bone-resorbing activity of osteoclasts grown in vitro (Chang et al. 2008). Interestingly, in vivo experiments showed that Ckb−/− mice were less susceptible to bone loss induced by ovariectomy, lipopolysaccharide challenge or interleukin-1 treatment than wild-type controls (Chang et al. 2008). Moreover, treatment with cyclocreatine or adenoviruses harboring Ckb small hairpin RNA prevented bone loss in rodents (Chang et al. 2008). Collectively, these data reveal an important role for Ckb in the bone-resorbing function of osteoclasts.
Osteoclast activity can be indirectly assessed in humans by measuring break-down products of type I collagen in blood or urine, such as cross-linked n-telopeptides of Type I collagen (NTx). The first studies to assess effects of creatine on NTx showed this marker of bone resorption was reduced 19–72 % with creatine supplementation (3–3.5 g day−1, 12–16 weeks) compared to placebo in boys with muscular dystrophy (Louis et al. 2003c; Tarnopolsky et al. 2004). Young healthy adults who supplemented with creatine (9 g day−1, 5 weeks) during resistance training reduced NTx by 30 % compared to placebo (Cornish et al. 2009). In aging males, creatine supplementation (0.1 g kg−1) during 10 weeks of supervised resistance training (3 g week−1) decreased NTx by 27 % compared to an increase of 13 % for the placebo group (Candow et al. 2008).
While these studies suggest a beneficial effect of creatine on bone cells, others have failed to observe the same benefits. Daily ingestion of creatine (1 g day−1) for 52 weeks in postmenopausal women had no effect on serum C-terminal telopeptide of type I collagen (CTX; indicator of bone resorption) (Creatine: pre 0.39 ± 0.17 ng mL−1, post 0.83 ± 2.9 ng mL−1; Placebo: pre 0.38 ± 0.16 ng mL−1, post 0.68 ± 1.7 ng mL−1) or Procollagen type I N-propeptide (P1NP; indicator of bone formation) (Creatine: pre 53.1 ± 30.6 µg L−1, post 57.5 ± 27.8 µg L−1; Placebo: pre 50.4 ± 23.3 µg L−1, post 55.0 ± 22.5 µg L−1) (Lobo et al. 2015). Previous work from the same laboratory also failed to observe a beneficial effect from creatine supplementation (20 g day−1 for 5 days + 5 g day−1 for 161 days) on CTX or P1NP in postmenopausal women (Gualano et al. 2014), and no effects of 0.1 g kg−1 g day−1 creatine for 12 weeks on CTX or P1NP in children and teenagers with childhood systemic lupus erythematosus (Hayashi et al. 2014). In healthy older adults, creatine supplementation (5 g day−1) during 14–24 weeks of resistance training had no effect on NTx (Tarnopolsky et al. 2007) or serum osteocalcin (an indicator of bone formation) compared to placebo (Brose et al. 2003).
Can creatine supplementation promote bone accretion in experimental models?
In young male rats (5 weeks of age), creatine supplementation (2 % wet weight) for 8 weeks increased lumbar spine bone mineral density by 41 % and femoral load to failure by 12 % compared to placebo (Antolic et al. 2007). In ovariectomized Wistar rats, an animal model of postmenopausal osteoporosis, creatine ingestion (300 mg kg−1 for 8 weeks) led to a significant increase in lumbar bone phosphate content, which could lead to greater bone quality over time (de Souza et al. 2012). In contrast to these studies, creatine supplementation (300 mg kg−1) for 12 weeks, with or without aerobic exercise, had no effect on bone mineral density, bone strength or bone histomorphometry properties in ovariectomized Wistar rats (Murai et al. 2015). Creatine administration (5 mg kg−1) for 9 weeks also had no effect on bone mineral density in hypertensive male rats, a representative model of osteoporosis (Alves et al. 2012b).
Can creatine supplementation promote bone accretion in humans?
There are a limited number of studies examining the effects of creatine supplementation on properties of bone accretion, most of which have used dual energy X-ray absorptiometry to assess changes in areal bone mineral density (i.e. in g/cm−2) or bone mineral content (g). In young boys with Duchenne muscular dystrophy or Becker dystrophy who were independent of wheelchairs, 12 weeks of creatine supplementation (3 g day−1) improved whole-body and lumbar spine bone mineral density by 2–3 % over placebo (Louis et al. 2003c); however, Tarnopolsky et al. (2004) failed to replicate these findings after 16 weeks of creatine supplementation using a similar dose (~3.5 g day−1) in young boys with muscular dystrophy.
Studies involving aging adults have also produced inconsistent results. Healthy postmenopausal women who supplemented with creatine (0.1 g kg−1 day−1, or ~7 g day−1) during 52 weeks of supervised resistance training (3 days week−1) experienced a significant increase in femoral shaft sub-periosteal width (an indicator of bone bending strength; Beck et al. 2011) and a decrease in the rate of bone mineral density loss in the femoral neck (−1.2 %) compared to women on placebo (−3.9 %; Chilibeck et al. 2015). These results support previous findings from the same lab of a significant increase in upper-limb bone mineral content from creatine supplementation (0.3 g kg−1 for 5 days + 0.07 g kg−1 for 79 days; corresponding to about 26 g for 5 days + 6 g for 70 days) and resistance training in healthy older males (Creatine: pre 433 ± 77 g, post 447 ± 82 g, Placebo: pre 405 ± 97 g, post 401 ± 98 g, p < 0.05; Chilibeck et al. 2005).
Others have not observed the same benefits in older adults. Lobo et al. (2015) investigated the effects of low-dose creatine (1 g day−1) without exercise training for 52 weeks on properties of bone in postmenopausal women. Creatine had no greater effect on bone mineral density or bone microarchitecture (cortical bone density; trabecular bone volume, number, thickness, as assessed by high-resolution peripheral quantitative tomography) compared to women on a placebo. Creatine supplementation (20 g day−1 for 5 days + 5 g day−1 for 24 weeks), with or without resistance training (2 days week−1), had no effect on bone mineral density (whole-body, lumbar spine, femur) in postmenopausal women (Gualano et al. 2014). Tarnopolsky et al. (2007) investigated the effects of creatine supplementation (5 g day−1 for 24 weeks) and resistance training (2 days week−1) in healthy older adults (71 years, n = 21) and found no beneficial effect from creatine on bone mineral density (whole body, hip, lumbar spine) compared to placebo.
Differences in dosing and length of interventions may explain some of the discrepancies between studies. For example, in the study of Chilibeck et al. (2015), the creatine dosage was about 7 g day−1 compared to 1–5 g day−1 in the studies of Lobo et al. (2015), Gualano et al. (2014) and Tarnopolsky et al. (2007). Furthermore, the study of Chilibeck et al. (2015) was 52 weeks with greater training frequency (3 days week−1) whereas the studies showing no effect from creatine on bone used exercise training programs lasting 24 weeks (Gualano et al. 2014; Tarnopolsky et al. 2007) with lower training frequency (2 days week−1). Bone turnover is a long process and exercise and nutritional supplement interventions of at least 1 year, and preferable 2 years, are needed to produce effects on bone (Chilibeck et al. 2013). Although the study by Chilibeck et al. (2005) found significant increases in arm bone mineral content after only 12 weeks of creatine supplementation, this study is limited in that the bone results were from sub-regions of dual energy X-ray absorptiometry whole-body scans, which may have poor precision (Chilibeck et al. 1994).
The 12-month study by Lobo et al. (2015) had no training component to the design, and as mentioned above, used a very low dose of creatine (i.e. 1 g day−1). Creatine supplementation increases phosphorylcreatine in aged muscle (Brose et al. 2003), and by doing so, may allow older individuals to train at higher volumes and increase muscle mass (Chrusch et al. 2001). This increased training volume and muscle mass may provide additional strain on bone (through increased muscle pull on bone) and stimulate bone formation. Support from this notion is that during creatine supplementation, the increase in muscle mass correlates with an increase in bone mass (Chilibeck et al. 2005).
Creatine supplementation appeared to be relatively safe in the longer-term studies (i.e., 6–12 months) of older individuals (Chilibeck et al. 2015; Tarnopolsky et al. 2007; Gualano et al. 2014; Lobo et al. 2015). There is some concern that high doses of creatine may adversely affect kidney or liver, as evidenced in some animal studies (Edmunds et al. 2001; Tarnopolsky et al. 2003a). Some of these long-term studies excluded participants with signs of kidney and/or liver dysfunction at baseline (Chilibeck et al. 2015; Tarnopolsky et al. 2007); therefore, the safety of creatine in these studies can only be assumed in participants without kidney or liver dysfunction prior to supplementation. These studies all carefully followed adverse events, and included participants taking a variety of medications (with the exception of medications that affect bone metabolism). None reported kidney or liver adverse events by blood or urine markers, or interactions with medications (Chilibeck et al. 2015; Tarnopolsky et al. 2007; Gualano et al. 2014; Lobo et al. 2015). Two of the studies reported gastrointestinal adverse events that were “mild” in severity in 2–33 % of participants (Chilibeck et al. 2015; Tarnopolsky et al. 2007). As some of these studies excluded participants at baseline who had liver or kidney dysfunction, we suggest that older individuals with kidney or liver dysfunction not supplement with creatine until future studies can demonstrate safety in these participants.
In summary, creatine may affect the bone remodeling process, either by stimulating osteoblasts to increase bone formation or by inhibiting osteoclasts to reduce bone resorption. As bone formation is linked to resorption through the bone remodeling cycle, the effects on one type of bone cell (i.e., osteoblasts or osteoclasts) may not be exclusive of effects on the opposite type of bone cell. Results of studies using serum or urinary markers of bone formation and resorption are inconsistent with respect to the beneficial effects of creatine. Future studies of creatine supplementation should investigate effects of creatine on RANK/RANKL/OPG to better assess the mechanisms by which creatine may affect the coupling of bone formation to bone resorption. The effects of creatine on bone accretion are also inconsistent. In aging adults, creatine supplementation (of at least 7 g day−1) may have beneficial effects on bone mineral density if combined with higher-frequency (≥3 days week−1) resistance training for long durations (i.e. at least 12 months). Studies of creatine supplementation in humans of shorter durations or using lower doses showed no benefit on bone properties. Animal research is also equivocal with some showing benefits of creatine supplementation, including increases in direct measures of bone strength, while others have not replicated these findings. Additional human clinical trials are needed using larger sample sizes of mixed gender, longer durations of resistance training (>52 weeks), higher creatine dosages (>7 g), and further evaluation of bone mineral, bone geometry and microarchitecture properties.
Creatine supplementation and brain
Compared to skeletal muscle, where about 95 % of the creatine in the body is stored, there is very little creatine in the brain. However, the brain is responsible for up to 20 % of energy consumption, and creatine and phosphorylcreatine are essential to maintain nervous system energy levels (reviewed in Beard and Braissant 2010; Wyss and Kaddurah-Daouk 2000). Relative to changes in brain creatine content consequent to diseases such as major depression (Allen 2012; Kato et al. 1992), schizophrenia (Öngur et al. 2009), or creatine deficiency syndromes (Beard and Braissant 2010), far less is known about the effects of healthy aging on brain creatine (Rawson and Venezia 2011). Brain creatine is inversely correlated with age and performance on the mini-mental state exam (Laakso et al. 2003), and can also be increased with memory training (Valenzuela et al. 2003). Although brain creatine should not be viewed as constant across the lifespan, longitudinal data on age-related changes in brain creatine are lacking.
As described elsewhere in this review, there is a great deal of research that demonstrates the efficacy of creatine supplementation on improving muscle and bone health in older adults. Additionally, creatine supplementation has an excellent safety profile in young and older adults and in several patient populations (reviewed in Gualano et al. 2012; Kim et al. 2011; Persky and Rawson 2007; Rae and Broer 2015). While the effects of creatine monohydrate supplementation on skeletal muscle metabolism and function have been well described, far less is known about the effects of creatine monohydrate intake on the brain. A small number of groups have investigated the effects of creatine supplementation on brain creatine or on cognitive processing, although these studies have primarily focused on younger adults (reviewed in Rae and Broer 2015; Rawson and Venezia 2011). This section will summarize the most recent developments regarding the effects of creatine supplementation on the brain.
Can creatine supplementation increase brain creatine levels in older adults?
Dechent et al. (1999) first demonstrated that creatine supplementation could increase brain creatine levels in humans. These findings were supported in most (six) (Dechent et al. 1999; Hellem et al. 2015; Kondo et al. 2011; Lyoo et al. 2003; Pan and Takahashi 2007; Turner et al. 2015), but not all (one) (Wilkinson et al. 2006) studies (reviewed by Rae and Broer 2015; Rawson and Venezia 2011). It is difficult to directly compare these investigations due to differences in methodology in brain creatine assessment (total creatine assessed with 1H-NMR vs. phosphorylcreatine assessed with 31P-NMR), supplement dose, supplement duration, and population (e.g., vegetarians vs. omnivores; athletes vs. depressed vs. apparently healthy). Also, as with skeletal muscle, initial brain creatine levels, which may or may not be lower in vegetarians (Yazigi Solis et al. 2014), are inversely related to the increase in brain creatine post-supplementation (Pan and Takahashi 2007). A final complicating factor in the comparison of these studies is that there appears to be regional differences in brain creatine content, and, subsequently, regional differences in the response to creatine supplementation (Dechent et al. 1999). If there is a significant increase in brain creatine or phosphorylcreatine, subsequent to creatine ingestion, which seems probable, the increase has been shown to be smaller than seen in muscle following creatine ingestion (e.g. 20 vs. 8 %) (Harris et al. 1992; Dechent et al. 1999; reviewed in Rawson and Venezia 2011).
Can creatine supplementation improve cognitive processing in older adults?
The effects of creatine monohydrate ingestion on cognitive processing have been previously reviewed (Rae and Broer 2015; Rawson and Venezia 2011). The majority of these investigations have focused on apparently healthy young adults, so any extrapolations to older adults must be approached with caution. Also, as with the investigations into the effects of creatine supplementation on brain creatine levels, direct comparison between studies is difficult due to differences in supplement dose (2.5–20 g day−1) and duration (5 days to 24 weeks), populations (e.g. young vs. old; vegetarian vs. omnivores), additional stress (e.g., sleep or oxygen deprivation vs. rested) and various cognitive outcome assessments. A final complication is that the majority of the studies that assessed brain creatine pre- and post-supplementation did not measure cognitive processing, and the majority of studies that assessed cognitive processing pre- and post-supplementation do not have direct measures of changes in brain creatine to support their findings.
Nonetheless, of 11 studies, 9 reported significant improvements in some aspect of cognitive processing following creatine monohydrate supplementation. Five studies were focused on rested volunteers (4 showed beneficial effects of creatine) (Hammett et al. 2010; Ling et al. 2009; Rae et al. 2003; Rawson et al. 2008; Benton and Donohoe 2011), two on sleep deprived volunteers (both showed beneficial effects) (McMorris et al. 2006, 2007b), one on oxygen deprived volunteers (beneficial effects) (Turner et al. 2015), one on mentally fatigued volunteers (beneficial effects) (Watanabe et al. 2002), and two on older adults described below (Alves et al. 2013; McMorris et al. 2007a).
McMorris et al. (2007a) examined the effects of creatine monohydrate ingestion (20 g day−1 for 7 days) in older adults (76 years old) and found improvements in some, but not all aspects of cognitive processing. For example, while performance on random number generation and a forward recall verbal short-term memory test were unaffected by supplementation, performance on forward and backward recall spatial short-term memory tests, a forward recall verbal short-term memory test, and a long-term memory test were improved (McMorris et al. 2007a). Alves et al. (2013) examined the combined effects of creatine supplementation and resistance training on physical and mental function. Compared to placebo ingestion or placebo ingestion plus strength training, creatine supplementation alone, or combined with strength training, did not improve cognitive processing or mood, assessed with a modified Geriatric Depression Scale, the Mini-Mental State Examination, Stroop Test, Trail Making Test, Digit Span Test, and Delayed Recall Test. At this point in time, a number of studies suggest that creatine supplementation improves cognitive processing under resting and various stressed conditions. However, fewer data are available on older adults.
How does creatine supplementation improve cognitive processing?
Although the direct mechanism through which creatine supplementation improves cognitive processing is not known, the best explanation is that increasing brain creatine levels improves brain energy metabolism. During intense exercise, muscle ATP needs are increased, but increasing muscle creatine through supplementation provides a larger reserve for ATP production and subsequently improves exercise performance. Similarly, increasing brain creatine with supplementation, improves energy availability, and subsequently improves brain performance (i.e. cognitive processing). Improved cognitive processing subsequent to creatine supplementation has been shown during increased brain activity (Watanabe et al. 2002), increased brain and muscle activity (McMorris et al. 2006, 2007b), when brain metabolism is compromised by hypoxia (Turner et al. 2015), when brain creatine might be decreased due to a low creatine diet (Rae et al. 2003) or aging (McMorris et al. 2007a), and also under resting conditions (Hammett et al. 2010; Ling et al. 2009; Rae et al. 2003; Benton and Donohoe 2011). As mentioned previously, with the exception of one study of hypoxic volunteers (Turner et al. 2015), studies that report improved cognitive processing subsequent to creatine supplementation did not asses changes in brain creatine levels to confirm the hypothesis that increased energy availability is the mechanism for improved cognitive processing (Hammett et al. 2010; Ling et al. 2009; Rae et al. 2003; Benton and Donohoe 2011; McMorris et al. 2006, 2007a, b; Watanabe et al. 2002).
Why does not creatine supplementation improve cognitive processing in older adults in every study?
It is difficult to explain the discrepant findings, due to the small number of studies that focused on older adults (n = 2), and also due to differences in methodologies and populations described elsewhere in this review. Clearly, creatine is important in both muscular and cerebral energetics, and although there are many similarities between the two tissues, there are important differences as well. For instance, in skeletal muscle, there is separation of the sites of creatine synthesis (liver, pancreas, kidneys) and storage/utilization (muscle). Thus, skeletal muscle is designed to take up creatine from periphery. The brain, however, has a more limited capacity to take up creatine, and the two enzymes involved in creatine synthesis, AGAT (arginine: glycine amidinotransferase) and GAMT (guanidinoacetate methyltransferase) are present in nervous tissue, suggesting that the brain is capable of creatine synthesis (Beard and Braissant 2010; Braissant 2012; Rae and Broer 2015). Further, the SLC6A8 creatine transporter (i.e. CRT1 or CreaT) is expressed in micro-capillary endothelial cells at the blood–brain barrier, but not in the surrounding astrocytes. This is suggestive of a possible, albeit limited permeability of the brain to peripheral creatine. In fact, in the three creatine deficiency syndromes identified in humans, AGAT and GAMT deficiencies are responsive to creatine therapy, while SLC6A8 deficiencies are not. Thus, although increased brain creatine and improved cognitive processing following oral creatine monohydrate supplementation have been shown, increasing brain creatine levels through oral supplementation is likely more difficult than increasing muscle creatine levels.
Although the majority of peer reviewed studies suggest that oral creatine monohydrate supplementation can improve cognitive processing, currently, only two studies have investigated older adults, and the data are discrepant. Nonetheless, creatine monohydrate is an inexpensive, safe nutrient that stands to offer many benefits to older adults across multiple systems. Future studies should focus on older adults and possibly frail elders or those who have already experienced an age-associated cognitive decline. Additionally, dose–response studies are needed, as the optimal dose for increasing brain creatine levels is not known.
Concluding remarks
Creatine supplementation, particularly along with resistance training, emerges as a potential nutritional intervention capable of improving health in aging. The beneficial effects of creatine on muscle function and lean mass in elderly individuals are consistent and supported by meta-analytic data, whereas the actions of this nutrient on bone and brain metabolism remain promising but require further high-quality clinical studies involving older individuals.
References
Aguiar AF, Januário RS, Junior RP, Gerage AM, Pina FL, do Nascimento MA, Padovani CR, Cyrino ES (2013) Long-term creatine supplementation improves muscular performance during resistance training in older women. Eur J Appl Physiol 113:987–996. doi:10.1007/s00421-012-2514-6
Allen PJ (2012) Creatine metabolism and psychiatric disorders: Does creatine supplementation have therapeutic value? Neurosci Biobehav Rev 36(5):1442–1462
Alves CR, Ferreira JC, de Siqueira-Filho MA, Carvalho CR, Lancha AH Jr, Gualano B (2012a) Creatine-induced glucose uptake in type 2 diabetes: a role for AMPK-alpha? Amino Acids 43:1803–1807. doi:10.1007/s00726-012-1246-6
Alves CR, Murai IH, Ramona P, Nicastro H, Takayama L, Guimarães F, Lancha Junior AH, Irigoyen MC, Pereira RM, Gualano B (2012b) Influence of creatine supplementation on bone mass of spontaneously hypertensive rats. Braz J Rheumatol 52(3):453–461
Alves CR, Merege Filho CA, Benatti FB, Brucki S, Pereira RM, de Sa Pinto AL, Lima FR, Roschel H, Gualano B (2013) Creatine supplementation associated or not with strength training upon emotional and cognitive measures in older women: a randomized double-blind study. PLoS One 8(10):e76301
Antolic A, Roy BD, Tarnopolsky MA et al (2007) Creatine monohydrate increases bone mineral density in young Sprague-Dawley rats. Med Sci Sports Exerc 39(5):816–820
Bauer J, Biolo G, Cederholm T, Cesari M, Cruz-Jentoft AJ, Morley JE, Phillips S, Sieber C, Stehle P, Teta D, Visvanathan R, Volpi E, Boirie Y (2013) Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. J Am Med Dir Assoc 14:542–559. doi:10.1016/j.jamda.2013.05.021
Beard E, Braissant O (2010) Synthesis and transport of creatine in the CNS: importance for cerebral functions. J Neurochem 115(2):297–313
Beck TJ, Kohlmeier LA, Petit MA, Wu G, Leboff MS, Cauley JA, Nicholas S, Chen Z (2011) Confounders in the association between exercise and femur bone in postmenopausal women. Med Sci Sports Exerc 43:80–89
Bemben MG, Witten MS, Carter JM, Eliot KA, Knehans AW, Bemben DA (2010) The effects of supplementation with creatine and protein on muscle strength following a traditional resistance training program in middle-aged and older men. J Nutr Health Aging 14:155–159
Benton D, Donohoe R (2011) The influence of creatine supplementation on the cognitive functioning of vegetarians and omnivores. Br J Nutr 105(7):1100–1105
Bermon S, Venembre P, Sachet C, Valour S, Dolisi C (1998) Effects of creatine monohydrate ingestion in sedentary and weight-trained older adults. Acta Physiol Scand 164:147–155. doi:10.1046/j.1365-201X.1998.00427.x
Braissant O (2012) Creatine and guanidinoacetate transport at blood–brain and blood–cerebrospinal fluid barriers. J Inherit Metab Dis 35(4):655–664
Branch JD (2003) Effect of creatine supplementation on body composition and performance: a meta-analysis. Int J Sport Nutr Exerc Metab 13:198–226
Breen L, Phillips SM (2011) Skeletal muscle protein metabolism in the elderly: interventions to counteract the ‘anabolic resistance’ of ageing. Nutr Metab (Lond) 8:68. doi:10.1186/1743-7075-8-68
Brose A, Parise G, Tarnopolsky MA (2003) Creatine supplementation enhances isometric strength and body composition improvements following strength exercise training in older adults. J Gerontol A Biol Sci Med Sci 58:11–19
Burke DG, Candow DG, Chilibeck PD, MacNeil LG, Roy BD, Tarnopolsky MA, Ziegenfuss T (2008) Effect of creatine supplementation and resistance-exercise training on muscle insulin-like growth factor in young adults. Int J Sport Nutr Exerc Metab 18:389–398
Candow DG et al (2008) Low-dose creatine combined with protein during resistance training in older men. Med Sci Sports Exerc 40:1645–1652. doi:10.1249/MSS.0b013e318176b310
Chang EJ, Ha J, Oerlemans F, Lee YJ, Lee SW, Ryu J, Kim HJ, Lee Y, Kim HM, Choi JY, Kim JY, Shin CS, Pak YK, Tanaka S, Wieringa B, Lee ZH, Kim HH (2008) Brain-type creatine kinase has a crucial role in osteoclast-mediated bone resorption. Nat Med 14:966–972. doi:10.1038/nm.1860
Chilibeck P, Calder A, Sale DG, Webber C (1994) Reproducibility of dual-energy X-ray absorptiometry. Can Assoc Radiol J 45(4):297–302
Chilibeck PD, Chrusch MJ, Chad KE et al (2005) Creatine monohydrate and resistance training increase bone mineral content and density in older men. J Nutr Health Aging 9(5):352–355
Chilibeck PD, Vatanparast H, Pierson R, Case A, Olatunbosun O, Whiting SJ, Beck TJ, Pahwa P, Biem HJ (2013) Effect of exercise training combined with isoflavone supplementation on bone and lipids in postmenopausal women: a randomized clinical trial. J Bone Miner Res 28(4):780–793
Chilibeck PD, Candow DG, Landeryou T, Kaviani M, Paus-Jenssen L (2015) Effects of creatine and resistance training on bone health in postmenopausal women. Med Sci Sports Exerc. 47(8):1587–1595
Chrusch MJ, Chilibeck PD, Chad KE, Davison KS, Burke DG (2001) Creatine supplementation combined with resistance training in older men. Med Sci Sports Exerc 33(12):2111–2117
Collins J, Longhurst G, Roschel H, Gualano B (2016) Resistance training and co-supplementation with creatine and protein in older subjects with frailty. J Frailty Aging (in press)
Cornish SM, Candow DG, Jantz NT et al (2009) Conjugated linoleic acid combined with creatine monohydrate and whey protein supplementation during strength training. Int J Sport Nutr Exerc Metab 19(1):79–96
Dangott B, Schultz E, Mozdziak PE (2000) Dietary creatine monohydrate supplementation increases satellite cell mitotic activity during compensatory hypertrophy. Int J Sports Med 21:13–16. doi:10.1055/s-2000-8848
de Souza RA, Xavier M, da Silva FF, de Souza MT, Tosato MG, Martin AA, Castilho JC, Ribeiro W, Silveira L Jr (2012) Lasers Influence of creatine supplementation on bone quality in the ovariectomized rat model: an FT-Raman spectroscopy study. Med Sci 27(2):487–495
Dechent P, Pouwels PJ, Wilken B, Hanefeld F, Frahm J (1999) Increase of total creatine in human brain after oral supplementation of creatine-monohydrate. Am J Physiol 277(3 Pt 2):R698–R704
Deldicque L, Louis M, Theisen D, Nielens H, Dehoux M, Thissen JP, Rennie MJ, Francaux M (2005) Increased IGF mRNA in human skeletal muscle after creatine supplementation. Med Sci Sports Exerc 37:731–736
Devries MC, Phillips SM (2014) Creatine supplementation during resistance training in older adults—a meta-analysis. Med Sci Sports Exerc 46:1194–1203. doi:10.1249/MSS.0000000000000220
Edmunds JW, Jayapalan S, DiMarco NM, Saboorian MH, Aukema HM (2001) Creatine supplementation increases renal disease progression in Han:SPRD-cy rats. Am J Kidney Dis 37:73–78
Eijnde BO, Van Leemputte M, Goris M, Labarque V, Taes Y, Verbessem P, Vanhees L, Ramaekers M, Vanden Eynde B, Van Schuylenbergh R, Dom R, Richter EA, Hespel P (2003) Effects of creatine supplementation and exercise training on fitness in men 55–75 years old. J Appl Physiol 95:818–828. doi:10.1152/japplphysiol.00891.200200891.2002
Eliot KA, Knehans AW, Bemben DA, Witten MS, Carter J, Bemben MG (2008) The effects of creatine and whey protein supplementation on body composition in men aged 48 to 72 years during resistance training. J Nutr Health Aging 12:208–212
Ferri A, Scaglioni G, Pousson M, Capodaglio P, Van Hoecke J, Narici MV (2003) Strength and power changes of the human plantar flexors and knee extensors in response to resistance training in old age. Acta Physiol Scand 177:69–78. doi:10.1046/j.1365-201X.2003.01050.x
Forsberg AM, Nilsson E, Werneman J, Bergstrom J, Hultman E (1991) Muscle composition in relation to age and sex. Clin Sci (Lond) 81:249–256
Gerber I, Ap Gwynn I, Alini M et al (2005) Stimulatory effects of creatine on metabolic activity, differentiation and mineralization of primary osteoblast-like cells in monolayer and micromass cell cultures. Eur Cell Mater 15:108–122
Gotshalk LA, Kraemer WJ, Mendonca MA, Vingren JL, Kenny AM, Spiering BA, Hatfield DL, Fragala MS, Volek JS (2008) Creatine supplementation improves muscular performance in older women. Eur J Appl Physiol 102:223–231. doi:10.1007/s00421-007-0580-y
Gualano B, Artioli GG, Poortmans JR, Lancha Junior AH (2009) Exploring the therapeutic role of creatine supplementation. Amino Acids. doi:10.1007/s00726-009-0263-6
Gualano B, De Salles Painneli V, Roschel H, Artioli GG, Neves M Jr, De Sá Pinto AL, Da Silva ME, Cunha MR, Otaduy MC, Leite Cda C, Ferreira JC, Pereira RM, Brum PC, Bonfá E, Lancha AH Jr (2010) Creatine in Type 2 Diabetes: a randomized, double-blind, placebo-controlled trial. Med Sci Sports Exerc. doi:10.1249/MSS.0b013e3181fcee7d
Gualano B, Roschel H, Lancha-Jr AH, Brightbill CE, Rawson ES (2012) In sickness and in health: the widespread application of creatine supplementation. Amino Acids 43:519–529. doi:10.1007/s00726-011-1132-7
Gualano B, Macedo AR, Alves CR, Roschel H, Benatti FB, Takayama L, de Sá Pinto AL, Lima FR, Pereira RM (2014) Creatine supplementation and resistance training in vulnerable older women: a randomized double-blind placebo-controlled clinical trial. Exp Gerontol 53:7–15. doi:10.1016/j.exger.2014.02.003
Guimbal C, Kilimann M (1993) A Na(+)-dependent creatine transporter in rabbit brain, muscle, heart, and kidney. cDNA cloning and functional expression. J Biol Chem 268:8418–8421
Hammett ST, Wall MB, Edwards TC, Smith AT (2010) Dietary supplementation of creatine monohydrate reduces the human fMRI BOLD signal. Neurosci Lett 479:201–205
Harris RC, Söderlund K (1992) Hultman E (1992) Elevation of creatine in resting and exercised muscle of normal subjects by creatinesupplementation. Clin Sci (Lond) 83:367–374
Hayashi AP, Solis MY, Sapienza MT, Otaduy MC, de Sá Pinto AL, Silva CA, Sallum AM, Pereira RM, Gualano B (2014) Efficacy and safety of creatine supplementation in childhood-onset systemic lupus erythematosus: a randomized, double-blind, placebo-controlled, crossover trial. Lupus 23(14):1500–1511. doi:10.1177/0961203314546017
Hellem TL, Sung YW, Shi XF, Pett MA, Latendresse G, Morgan J, Huber RS, Kuykendall D, Lundberg KJ, Renshaw PF (2015) Creatine as a novel treatment for depression in females using methamphetamine: a pilot study. J Dual Diagn 11(3–4):189–202
Hogan DB, MacKnight C, Bergman H (2003) Models, definitions, and criteria of frailty. Aging Clin Exp Res 15:1–29
Jakobi JM, Rice CL, Curtin SV, Marsh GD (2001) Neuromuscular properties and fatigue in older men following acute creatine supplementation. Eur J Appl Physiol 84:321–328
Kato T, Takahashi S, Shioiri T, Inubushi T (1992) Brain phosphorous metabolism in depressive disorders detected by phosphorus-31 magnetic resonance spectroscopy. J Affect Disord 26(4):223–230
Kent-Braun JA, Ng AV (2000) Skeletal muscle oxidative capacity in young and older women and men. J Appl Physiol 89:1072–1078
Kim HJ, Kim CK, Carpentier A, Poortmans JR (2011) Studies on the safety of creatine supplementation. Amino Acids 40(5):1409–1418
Kondo DG, Sung YH, Hellem TL, Fiedler KK, Shi X, Jeong EK, Renshaw PF (2011) Open-label adjunctive creatine for female adolescents with SSRI-resistant major depressive disorder: a 31-phosphorus magnetic resonance spectroscopy study. J Affect Disord 135(1–3):354–361
Laakso MP, Hiltunen Y, Kononen M, Kivipelto M, Koivisto A, Hallikainen M, Soininen H (2003) Decreased brain creatine levels in elderly apolipoprotein E epsilon 4 carriers. J Neural Transm 110(3):267–275
Leibbrandt A, Penninger JM (2009) RANK(L) as a key target for controlling bone loss. Adv Exp Med Biol 647:130–145
Ling J, Kritikos M, Tiplady B (2009) Cognitive effects of creatine ethyl ester supplementation. Behav Pharmacol 20(8):673–679
Lobo DM, Tritto AC, da Silva LR, de Oliveira PB, Benatti FB, Roschel H, Nieß B, Gualano B, Pereira RM (2015) Effects of long-term low-dose dietary creatine supplementation in older women. Exp Gerontol 70:97–104
Louis M, Poortmans JR, Francaux M, Berré J, Boisseau N, Brassine E, Cuthbertson DJ, Smith K, Babraj JA, Waddell T, Rennie MJ (2003a) No effect of creatine supplementation on human myofibrillar and sarcoplasmic protein synthesis after resistance exercise. Am J Physiol Endocrinol Metab 285:E1089–E1094. doi:10.1152/ajpendo.00195.2003
Louis M, Poortmans JR, Francaux M, Hultman E, Berre J, Boisseau N, Young VR, Smith K, Meier-Augenstein W, Babraj JA, Waddell T, Rennie MJ (2003b) Creatine supplementation has no effect on human muscle protein turnover at rest in the postabsorptive or fed states. Am J Physiol Endocrinol Metab 284:E764–E770. doi:10.1152/ajpendo.00338.2002
Louis M, Lebacq J, Poortmans JR, Belpaire-Dethiou MC, Devogelaer JP, Van Hecke P, Goubel F, Francaux M (2003c) Beneficial effects of creatine supplementation in dystrophic patients. Muscle Nerve 27(5):604–610
Lyoo IK, Kong SW, Sung SM, Hirashima F, Parow A, Hennen J, Cohen BM, Renshaw PF (2003) Multinuclear magnetic resonance spectroscopy of high-energy phosphate metabolites in human brain following oral supplementation of creatine-monohydrate. Psychiatry Res 123(2):87–100
McMorris T, Harris RC, Swain J, Corbett J, Collard K, Dyson RJ, Dye L, Hodgson C, Draper N (2006) Effect of creatine supplementation and sleep deprivation, with mild exercise, on cognitive and psychomotor performance, mood state, and plasma concentrations of catecholamines and cortisol. Psychopharmacology (Berl) 185:93–103
McMorris T, Mielcarz G, Harris RC, Swain JP, Howard A (2007a) Creatine supplementation and cognitive performance in elderly individuals. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn 14(5):517–528
McMorris T, Harris RC, Howard AN, Langridge G, Hall B, Corbett J, Dicks M, Hodgson C (2007b) Creatine supplementation, sleep deprivation, cortisol, melatonin and behavior. Physiol Behav 90(1):21–28
Moller P, Bergstrom J, Furst P, Hellstrom K (1980) Effect of aging on energy-rich phosphagens in human skeletal muscles. Clin Sci (Lond) 58:553–555
Murai IH, Roschel H, Pabis LV, Takayama L, de Oliveira RB, Dos Santos Pereira RT, Dantas WS, Pereira RM, Jorgetti V, Ballester RY, Gualano B (2015) Exercise training, creatine supplementation, and bone health in ovariectomized rats. Osteoporos Int 26(4):1395–1404
Naclerio F, Larumbe-Zabala E (2015) Effects of whey protein alone or as part of a multi-ingredient formulation on strength, fat-free mass, or lean body mass in resistance-trained individuals: a meta-analysis. Sports Med. doi:10.1007/s40279-015-0403-y
Neves M Jr, Gualano B, Roschel H, Fuller R, Benatti FB, Pinto AL, Lima FR, Pereira RM, Lancha AH Jr, Bonfá E (2011) Beneficial effect of creatine supplementation in knee osteoarthritis. Med Sci Sports Exerc 43:1538–1543. doi:10.1249/MSS.0b013e3182118592
Olsen S, Aagaard P, Kadi F, Tufekovic G, Verney J, Olesen JL, Suetta C, Kjaer M (2006) Creatine supplementation augments the increase in satellite cell and myonuclei number in human skeletal muscle induced by strength training. J Physiol 573:525–534
Öngur D, Prescot AP, Jensen JE, Cohen BM, Renshaw PF (2009) Creatine abnormalities in schizophrenia and bipolar disorder. Psychiatry Res 172(1):44–48
Pan JW, Takahashi K (2007) Cerebral energetic effects of creatine supplementation in humans. Am J Physiol Regul Integr Comp Physiol 292(4):R1745–R1750
Parise G, Mihic S, MacLennan D, Yarasheski KE, Tarnopolsky MA (2001) Effects of acute creatine monohydrate supplementation on leucine kinetics and mixed-muscle protein synthesis. J Appl Physiol 91:1041–1047
Persky AM, Rawson ES (2007) Safety of creatine supplementation. Subcell Biochem 46:275–289
Rae CD, Broer S (2015) Creatine as a booster for human brain function. How might it work? Neurochem Int 89:249–259
Rae C, Digney AL, McEwan RR, Bates TC (2003) Oral creatine monohydrate supplementation improves brain performance: a double-blind, placebo-controlled, cross-over trial. Proc R Soc Lond B Biol Sci 270(1529):2147–2150
Rawson ES, Clarkson PM (2000) Acute creatine supplementation in older men. Int J Sports Med 21:71–75. doi:10.1055/s-2000-8859
Rawson ES, Venezia AC (2011) Use of creatine in the elderly and evidence for effects on cognitive function in young and old Amino Acids 40:1349–1362. doi:10.1007/s00726-011-0855-9
Rawson ES, Wehnert ML, Clarkson PM (1999) Effects of 30 days of creatine ingestion in older men. Eur J Appl Physiol Occup Physiol 80:139–144
Rawson ES, Clarkson PM, Price TB, Miles MP (2002) Differential response of muscle phosphocreatine to creatine supplementation in young and old subjects. Acta Physiol Scand 174:57–65
Rawson ES, Lieberman HR, Walsh TM, Zuber SM, Harhart JM, Matthews TC (2008) Creatine supplementation does not improve cognitive function in young adults. Physiol Behav 95(1–2):130–134
Ruiz JR, Sui X, Lobelo F, Morrow JR Jr, Jackson AW, Sjostrom M, Blair SN (2008) Association between muscular strength and mortality in men: prospective cohort study. BMJ 337:a439
Safdar A, Yardley NJ, Snow R, Melov S, Tarnopolsky MA (2008) Global and targeted gene expression and protein content in skeletal muscle of young men following short-term creatine monohydrate supplementation. Physiol Genomics 32:219–228
Smith SA, Montain SJ, Matott RP, Zientara GP, Jolesz FA, Fielding RA (1998) Creatine supplementation and age influence muscle metabolism during exercise. J Appl Physiol 85:1349–1356
Stout JR, Sue Graves B, Cramer JT, Goldstein ER, Costa PB, Smith AE, Walter AA (2007) Effects of creatine supplementation on the onset of neuromuscular fatigue threshold and muscle strength in elderly men and women (64–86 years). J Nutr Health Aging 11:459–464
Syrotuik DG, Bell GJ (2004) Acute creatine monohydrate supplementation: a descriptive physiological profile of responders vs. nonresponders. J Strength Cond Res 18:610–617. doi:10.1519/12392.1
Syrotuik DG, Bell GJ, Burnham R, Sim LL, Calvert RA, McLean IM (2000) Absolute and relative strength performance following creatine monohydrate supplementation combined with periodized resistance training. Strength Cond Res 14:182
Tarnopolsky MA, Bourgeois JM, Snow R, Keys S, Roy BD, Kwiecien JM, Turnbull J (2003a) Histological assessment of intermediate- and long-term creatine monohydrate supplementation in mice and rats. Am J Physiol Regul Integr Comp Physiol 285:R762–R769
Tarnopolsky M, Parise G, Fu MH, Brose A, Parshad A, Speer O, Wallimann T (2003b) Acute and moderate-term creatine monohydrate supplementation does not affect creatine transporter mRNA or protein content in either young or elderly humans. Mol Cell Biochem 244:159–166
Tarnopolsky MA, Mahoney DJ, Vajsar J et al (2004) Creatine monohydrate enhances strength and body composition in Duchenne muscular dystrophy. Neurology 62(10):1771–1777
Tarnopolsky M, Zimmer A, Paikin J et al (2007) Creatine monohydrate and conjugated linoleic acid improve strength and body composition following resistance exercise in older adults. PLoS One 2:e991. doi:10.1371/journal.pone.0000991
Tesch PA, Thorsson A, Fujitsuka N (1989) Creatine phosphate in fiber types of skeletal muscle before and after exhaustive exercise. J Appl Physiol 66:1756–1759
Tieland M, Dirks ML, van der Zwaluw N, Verdijk LB, van de Rest O, de Groot LC, van Loon LJ (2012) Protein supplementation increases muscle mass gain during prolonged resistance-type exercise training in frail elderly people: a randomized, double-blind, placebo-controlled trial. J Am Med Dir Assoc 13:713–719. doi:10.1016/j.jamda.2012.05.020
Tinetti ME, Speechley M, Ginter SF (1988) Risk factors for falls among elderly persons living in the community. N Engl J Med 319:1701–1707. doi:10.1056/NEJM198812293192604
Turner CE, Byblow WD, Gant N (2015) Creatine supplementation enhances corticomotor excitability and cognitive performance during oxygen deprivation. J Neurosci 35(4):1773–1780
Valenzuela MJ, Jones M, Wen W, Rae C, Graham S, Shnier R, Sachdev P (2003) Memory training alters hippocampal neurochemistry in healthy elderly. Neuroreport 14(10):1333–1337
Vierck JL, Icenoggle DL, Bucci L, Dodson MV (2003) The effects of ergogenic compounds on myogenic satellite cells. Med Sci Sports Exerc 35:769–776. doi:10.1249/01.MSS.0000065005.96298.01
Villanueva MG, He J, Schroeder ET (2014) Periodized resistance training with and without supplementation improve body composition and performance in older men. Eur J Appl Physiol 114:891–905. doi:10.1007/s00421-014-2821-1
Wall BT, Cermak NM, van Loon LJ (2014) Dietary protein considerations to support active aging. Sports Med 44(Suppl 2):S185–S194. doi:10.1007/s40279-014-0258-7
Wallimann T, Hemmer W (1994) Creatine kinase in non-muscle tissues and cells. Mol Cell Biochem 133–134:193–220
Wallimann T, Turner DC, Eppenberger HM (1977) Localization of creatine kinase isoenzymes in myofibrils. I. Chicken skeletal muscle. J Cell Biol 75:297–317
Wallimann T, Wyss M, Brdiczka D, Nicolay K, Eppenberger HM (1992) Intracellular compartmentation, structure and function of creatine kinase isoenzymes in tissues with high and fluctuating energy demands: the ‘phosphocreatine circuit’ for cellular energy homeostasis. Biochem J 281(Pt 1):21–40
Wallimann T, Tokarska-Schlattner M, Schlattner U (2011) The creatine kinase system and pleiotropic effects of creatine. Amino Acids 40:1271–1296. doi:10.1007/s00726-011-0877-3
Watanabe A, Kato N, Kato T (2002) Effects of creatine on mental fatigue and cerebral hemoglobin oxygenation. Neurosci Res 42(4):279–285
Wilkinson ID, Mitchel N, Breivik S, Greenwood P, Griffiths PD, Winter EM, Van Beek E (2006) Effects of creatine supplementation on cerebral white matter in competitive sportsmen. Clin J Sport Med 16(1):63–67
Wilkinson TJ et al (2015) Can creatine supplementation improve body composition and objective physical function in rheumatoid arthritis patients? A randomised controlled trial. Arthritis Care Res (Hoboken). doi:10.1002/acr.22747
Willoughby DS, Rosene JM (2003) Effects of oral creatine and resistance training on myogenic regulatory factor expression. Med Sci Sports Exerc 35:923–929. doi:10.1249/01.MSS.0000069746.05241.F0
Wyss M, Kaddurah-Daouk R (2000) Creatine and creatinine metabolism. Physiol Rev 80:1107–1213
Yasuda H, Shima N, Nakagawa N et al (1998) Identity of osteoclastogenesis inhibitory factor (OCIF) and osteoprotegerin (OPG): a mechanism by which OPG/OCIF inhibits osteoclastogenesis in vitro. Endocrinology 139(3):1329–1337
Yazigi Solis M, de Salles Painelli V, Artioli GG, Roschel H, Otaduy MC, Gualano B (2014) Brain creatine depletion in vegetarians? A cross-sectional (1)H-magnetic resonance spectroscopy ((1)H-MRS) study. Br J Nutr 111(7):1272–1274
Acknowledgments
Bruno Gualano is financially supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), Conselho Nacional de Pesquisa e Tecnologia (CNPq) e Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
Bruno Gualano, Eric Rawson, and Darren G. Candow received financial support from Alzchem (Germany) for attending the scientific conference “Creatine in Health, Sport and Medicine 2015”. Bruno Gualano has also received a research grant from Alzchem for studies involving creatine supplementation. At the time this manuscript was prepared, Eric S. Rawson was a member of the Gatorade Sports Science Institute Expert Panel.
Additional information
Handling Editor: T. Wallimann and R. Harris.
Rights and permissions
About this article

Cite this article
Gualano, B., Rawson, E.S., Candow, D.G. et al. Creatine supplementation in the aging population: effects on skeletal muscle, bone and brain. Amino Acids 48, 1793–1805 (2016). https://doi.org/10.1007/s00726-016-2239-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00726-016-2239-7