
Abstract
Purpose
To examine the effects of 12 weeks of periodized resistance training (RT) with and without combined creatine and whey protein supplementation on changes in body composition, muscular strength, and functional performance.
Methods
Twenty-two male volunteers (68.1 ± 6.1 years) were randomly assigned to one of three groups: RT plus supplementation (RTS, n = 7); RT only (RT, n = 7); or control (C, n = 8). RTS consumed 0.3 g/kg/day of creatine for 5 days followed by 0.07 g/kg/day. RTS also consumed one 35 g liquid protein ready-to-drink daily. RT and RTS trained 3 days/week.
Results
Following 12 weeks of training, there were no significant differences in the main measured outcome variables between RT and RTS. RTS increased relative (% change) lean body mass (LBM, 3.3 ± 3.1 %) compared with C (p = 0.01). Compared to baseline, RT increased LBM at week 6 (60.2 ± 8.3 to 61.6 ± 9.4 kg; p < 0.05), and decreased fat mass (20.8 ± 4.2 to 19.0 ± 3.9 kg; p = 0.05) and percentage body fat at week 12 (25.7 ± 3.8 to 23.8 ± 4.0 %; p = 0.05); RTS increased LBM at week 6 (p < 0.01) and week 12 (56.4 ± 4.3 to 58.2 ± 3.4 kg; p < 0.01), and decreased percentage body fat at week 12 (23.9 ± 4.4 to 22.0 ± 4.4 %; p < 0.01). In addition, compared to C, relative bench press 1-RM increased for RTS (72.4 ± 62.2 %; p < 0.01) and RT (50.1 ± 21.5 %; p = 0.05); relative leg press 1-RM increased for RTS (129.6 ± 39.4 %; p < 0.0001) and RT (112.9 ± 22.7 %; p < 0.0001); RTS increased relative Margaria stair-climbing power (38.3 ± 30.4 %; p < 0.05); and, relative 400-m walk time decreased for RT (−11 ± 9.2 %; p < 0.05) and RTS (−9.6 ± 9.4 %; p = 0.05). RT increased estimated VO2Max at week 6 (p < 0.01) and 12 (34.6 ± 1.9 to 36.4 ± 2.7 ml/kg/min; p = 0.01) compared to baseline. Lastly, RTS increased estimated VO2Max at week 12 (36.3 ± 2.7 to 37.5 ± 3.3 ml/kg/min; p = 0.05) compared to baseline.
Conclusion
Creatine and whey protein supplementation may not provide additional benefits in older adults performing periodized RT to augment muscular and functional performance.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Multiple factors contribute to sarcopenia, a phenomenon characterized by the age-related loss of skeletal muscle mass, with declines in muscular strength, power, and functional capacity, including physical activity levels across the lifespan and a less than optimal diet (Koopman and van Loon 2009). In addition to its role in disease progression, the strength loss and general neuromuscular deconditioning associated with sarcopenia decrease an individual’s capacity to perform activities of daily living (ADL) and reduce his or her ability to exercise (Hunter et al. 2004). These reductions in skeletal muscle contractile force accelerate in the fifth and sixth decades of life (Lindle et al. 1997; Samson et al. 2000), and many of the changes in physical function are related to this loss of muscular strength (Fiatarone et al. 1990). If left unaddressed, these changes in physical function can result in a progressive loss of mobility and independence leading to increased risk of falls, disability, and dependence.
Resistance training robustly stimulates skeletal muscle growth (Kraemer et al. 1999) and has become a primary intervention used to attenuate the deleterious effects of sarcopenia. The hypertrophic response to resistance training results from replication of myofibrils in parallel within existing muscle fibers, thereby promoting muscle fiber growth and concomitant increases in muscle force production. Evidence suggests that the effects of planned and systematically progressed (i.e., periodized) resistance training programs can serve as a countermeasure against the reductions in muscle mass, strength, power, physical activity, and ADL associated with sarcopenia (Kraemer et al. 1999; Hakkinen et al. 2000; Chodzko-Zajko et al. 2009). However, research examining the effects of periodized resistance training programs in older adults is limited (Kraemer et al. 1999; Hakkinen et al. 2000); specifically, more evidence is needed to establish the efficacy and safety of periodized resistance training programs aimed at eliciting the greatest possible acute anabolic stimulus leading to optimal chronic hypertrophic and strength adaptations. These programs would prescribe higher training intensities and relatively short rest interval lengths in between sets and exercises and incorporate multiple compound movements, appropriately sequenced in each training session, to optimally stimulate large muscle masses (Kraemer et al. 1990, 1999; Crewther et al. 2006).
Substantial evidence suggests that the therapeutic benefits of resistance training are physiologically limited in older adults (Dalbo et al. 2009). One potential physiological limitation may be that aging results in reduced concentrations of resting phosphocreatine (PCr), which is a primary and integral component of the PCr energy system that predominates during performance of short-duration, high-intensity activities such as resistance training (Smith et al. 1998; Dalbo et al. 2009). Intramuscular PCr concentrations are ~25 % lower in older adults compared to young adults (Campbell et al. 1999), and individuals with low total intramuscular PCr concentrations show an enhanced ability to increase intracellular PCr content following supplementation with creatine (Harris et al. 1992). Furthermore, research indicates that adults above the age of 50 who are acutely supplemented with creatine have increased resting levels of intramuscular PCr and faster PCr resynthesis after exercise (Becque et al. 2000). Therefore, creatine supplementation may be a safe and effective mean to diminish age-related declines in lean mass and muscular performance, if improvements in metabolism translate into greater resistance training-induced adaptations (Chrusch et al. 2001). Chrusch et al. (2001) reported that creatine supplementation, in combination with resistance training, increases lean tissue mass and enhances several muscular performance qualities which include maximal strength, strength-endurance, and dynamic power. These augmented performance adaptations may result from an improved ability to tolerate more intense and frequent resistance training stimuli, all potentially leading to an enhanced hypertrophic response as well. Several studies in young men and women have shown an ergogenic effect of creatine supplementation on resistance training-induced muscular performance adaptations (Earnest et al. 1995; Stone et al. 1999), but similar studies are limited in older adults and have yielded equivocal results (Brose et al. 2003; Bemben et al. 2010). Therefore, collectively, research till day indicates older adults may benefit more than young adults from a combination of short- or long-term resistance training and creatine supplementation (Kreider et al. 1998; Volek et al. 1999).
Consuming adequate dietary protein to support protein turnover and resistance training-induced hypertrophy, while preventing protein degradation, is vital to health maintenance throughout the lifespan and may potentially be essential in slowing the rate of decline in muscle mass as a result of sarcopenia and other age-related factors (Hulmi et al. 2009; Koopman and van Loon 2009). Ingestion of amino acids or protein stimulates muscle protein synthesis and inhibits protein breakdown resulting in a positive net protein balance in both young and older adults (Koopman and van Loon 2009). Protein intake, especially whey/milk protein supplementation, before and/or immediately after an acute resistance training bout, may promote greater protein anabolism than protein ingestion at other times (e.g., optimal to ingest within 2–5 h prior to and/or after an acute resistance training bout) (Esmarck et al. 2001; Andersen et al. 2005; Cribb and Hayes 2006). Thus, frequent ingestion of whey/milk protein, immediately following an acute resistance training bout as part of a short- or long-term relatively high frequency resistance training program, may be a highly effective protein supplementation strategy to elicit an enhanced hypertrophic response to and recover from intense resistance training leading to superior resistance training-induced muscular performance improvements.
The purpose of this pilot investigation was to examine changes in lean body mass, fat mass, upper and lower body muscular strength and strength-endurance, functional performance, and aerobic capacity in older men (60–80 years), in response to a 12-week, non-linearly periodized resistance training program with and without creatine supplementation combined with whey/milk protein ingestion immediately post-resistance exercise. We hypothesized that all participants would experience significant improvements in body composition, muscular performance, and functional performance, following the resistance training program, and those participants who were supplemented with combined creatine and whey/milk protein would experience enhanced training adaptations.
Methods
Study participants
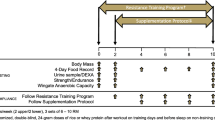
Twenty-two men (68.1 ± 6.1 years) volunteered to take part in this pilot investigation and were randomly assigned to one of three treatment groups (resistance training plus combined creatine and protein supplementation: RTS, n = 7; resistance training only: RT, n = 7; or control: C, n = 8). Study participants assigned to the control group underwent all testing procedures and completed a 3-day diet recall immediately prior to and immediately following a 12-week control period. During the control period, control study participants were asked to continue their usual activities of daily living, recreational activities, and dietary routines while refraining from beginning any sort of structured and consistent resistance training regimen. Following the 12-week control period, seven of the eight control group participants were randomly assigned to either the RT or RTS treatment group and completed the 12-week resistance training program with (RTS) or without (RT) combined creatine and protein supplementation. Participant characteristics (age, height, and weight) were recorded (Table 1).
All subjects were healthy, recreationally active, and none of the subjects were considered competitive weight lifters or engaged in any specific training/training cycle outside of this investigation. None of the subjects was taking any dietary or performance-enhancing supplements. All study participants were screened for uncontrolled hypertension, completed a Physical Activity Readiness Questionnaire (PAR-Q) to ensure they were qualified to participate in an exercise program, and provided medical clearance from their physician not more than 3 months prior to study enrollment, indicating that they did not have any known acute or chronic disease. Exclusion criteria included: acute illness such as infection, recent surgery, and trauma; chronic illness such as asthma, cardiac disease, kidney disease, liver disease, seizure disorders, anemia, and diabetes; musculoskeletal injury preventing the ability to perform resistance training and walking on a treadmill; and allergies to soy, milk, or whey protein. Last, each subject had the risks of the investigation explained to him and signed an informed consent form prior to participation in this study. The University of Southern California Health Sciences Campus Institutional Review Board approved all procedures involved in the study.
Dietary records
At baseline and study week 12, dietary intake was assessed via a 3-day dietary record in order to determine if any changes in the participants’ diet occurred throughout the intervention period. The diet re-calls were analyzed using a commercially available program (Nutritionist Pro, Axxya Systems, Stafford, TX).
Creatine supplementation protocol
RTS consumed 0.3 g/kg body weight/day of creatine for the first 5 days (i.e., loading phase) as developed by Hultman et al. (Hultman et al. 1996). Following the loading phase, RTS consumed 0.07 g/kg body weight/day of creatine until completion of the study (i.e., maintenance phase). Creatine supplements were provided in encapsulated powder (tablet) form and contained pure creatine monohydrate (MET-Rx Creatine 4200, MET-Rx Nutrition, Inc., Boca Raton, FL); to the nearest gram, the dosage was divided into three equal portions during the loading phase and one portion during the maintenance phase. Participants were encouraged to consume the supplements during or after meals, in equal intervals throughout the day, during the loading phase, and consumed maintenance doses immediately post-resistance exercise and with a meal on non-training days. After each resistance exercise session, participants were reminded about proper compliance to the creatine supplementation protocol and given a new set of supplements to be consumed before the next training session.
Protein supplementation protocol
RTS consumed one ready-to-drink (RTD) liquid whey protein supplement (Pure Protein, Worldwide Sport Nutritional Supplements, Inc., Bayport, NY), containing 35 g of protein and 170 kilocalories, immediately post-resistance exercise for the entire duration of the training intervention (36 training sessions total) and in the morning on non-training days. Therefore, protein supplements were consumed 7 days/week. Following each resistance exercise bout, the primary investigator distributed and watched participants consuming the supplement in its entirety, reminded them about proper compliance to the protein supplementation protocol on non-training days, and distributed the protein supplements to be consumed the next day (non-training day, in addition to their normal food intake). It is important to note that the dietary re-calls indicated that all study participants consumed >1.0 g protein/kg body weight/day, which likely allowed for maintenance of whole-body leucine metabolism and whole-body composition in this population of older adults (Campbell et al. 2001).
Resistance training program
Proper breathing and exercise technique were demonstrated during baseline testing and then again in the first training session. Participants were closely and individually supervised by an exercise specialist for all testing and training sessions, with proper lifting technique as a top priority. Participants were encouraged to continue normal activities of daily living and eating routines outside of the resistance training protocol.
RT and RTS underwent a progressive overload, total-body periodized resistance training program, which was performed with a 3-day/week frequency for 12 weeks (36 total training sessions). The only difference between RT and RTS was the combined creatine and protein supplementation regimen that RTS followed in addition to the 12-week RT program (performed by both RT and RTS). For this investigation, the compliance rate to the resistance training was established at 85 % (31 out of 36 training sessions completed); the mean compliance rate for all participants in this study was 94 % (on average, 34 out of 36 training sessions completed). Each training session began with a 5–10 min, low-moderate intensity warm-up on a treadmill and optional stretching exercises. Resistance exercise sequence was controlled for during each training session. Throughout the training program, sets/exercise ranged from 2 to 6 for a total of 5–6 exercises in each training session. The resistance exercises utilized in the RT program included: bilateral leg press (45° angle of push; plate-loaded), flat bench machine chest press (bench press; supine; right and left machine handles move independently of each other; plate-loaded), lat pulldown (seated; cable), seated row (non-trunk supported; cable), dumbbell step-ups (free weights; 12–18 inch step height), dumbbell Romanian deadlifts (free weights), bilateral knee extension/flexion (seated; machine). Low-intensity, body weight plyometrics and agility drills preceded all resistance exercise sessions and focused on dynamic balance, change of direction, coordination, and proper (jump) landing technique; these drills took approximately 5–10 min, serving as an auxiliary component of the warm-up.
Across the 3 days of resistance training throughout a week of training (1 microcycle), each training session emphasized a specific performance quality. Specifically, Day 1 emphasized hypertrophy with repetitions progressing from 12 to 8 across the RT program. Day 2 emphasized strength development with repetitions progressing from 6 to 3 across the RT program. Day 3 emphasized power production with repetitions progressing from 6 to 4 across the RT program and performed as “explosively” as possible, while maintaining full range of motion and proper lifting technique; the power loads corresponded to ~70 % of a participant’s max load tolerated for the prescribed power repetition maximum (RM) assignment (e.g., 70 % of the load prescribed on Day 2, for the same RM assignment), so participants were encouraged to emphasize their “intent to move loads with as much velocity as possible.” The rest interval length in between sets was 60 s, for all exercises, throughout the entire RT program. Between exercises, from the end of the last working set of one exercise to the first warm-up set of the next exercise, the rest interval length was kept between 60 s and 2 min. Training logs were maintained in detail for each study participant by the primary investigator, which detailed expected/actual training loads, sets, and repetitions for each exercise for every training session, in addition to participants’ subjective feedback during each training session (e.g., fatigued, relative ease handling loads, relative difficulty handling loads, etc.).
Throughout the entire resistance training program, all sets were performed maximally for the assigned number of repetitions and with proper lifting technique. Furthermore, it is important to note that study participants were never expected to perform sets to absolute failure; given an appropriate loading progression with alterations in set/repetition schemes throughout and across microcycles, the repetition maximum assignments allowed for successful completion of the assigned number of repetitions at the load(s) prescribed across multiple sets and with minimal need for assistance/“spotting.” Therefore, training loads used throughout the program were individually progressed in a safe and effective manner in order to employ a progressive overload/challenge to the neuromuscular system and elicit the greatest training-induced neuromuscular adaptations possible without inducing excessive neuromuscular fatigue effects (e.g., as a result of inappropriate overloading and/or training to failure every set/exercise in each training bout).
Testing
All testing procedures were conducted in the order described below prior to 12 weeks of resistance training (Baseline), after completion of 18 training sessions (week 6) and after completion of 36 training sessions (week 12), in the Clinical Exercise Research Center on the University of Southern California Health Sciences Campus. All testing procedures were performed in a single testing session, and the day/time of day for testing was consistent for each study participant throughout the study.
Body composition
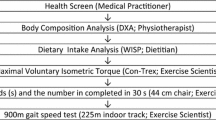
Estimates for lean body mass (LBM), fat mass, and body fat percentage were measured by whole-body dual-energy X-ray absorptiometry (DXA; GE Lunar iDXA, Waukesha, WI). Before scanning, all participants were required to take off all removable objects containing metal (i.e., jewelry and clothing with metal). Scans were performed with the study participants lying in a supine position and properly aligned with the DXA scanning table’s centerline longitudinal axis. Participants’ hands remained in a pronated or neutral position within the scanning region, and the participants were asked to remain completely immobile until the completion of the scan as signaled by the technician. The DXA scans were performed in the Clinical Exercise Research Center; from scans performed in our laboratory, the coefficients of variation for fat mass and LBM measurements associated with DXA are <1.7 %, and the reliability of the DXA scans are 0.99.
Aerobic capacity (VO2Max) test
Part I (Preliminary warm-up/determination of walking speed): Participants were fitted with a heart rate monitor consisting of an elastic band strapped around the chest, the resting heart rate was measured, and participants were familiarized with how to walk on a treadmill at a moderate speed and 0 % grade for 2–3 min without the use of railings; this allowed for a warm-up and acclimatization to the treadmill walking movement. Part II (4-min, single-stage sub-maximal walking test): Participants walked on the treadmill at a brisk pace between 2.5 and 4.0 mph, at a 5 % grade, for 4 min without the use of railings. A post-test heart rate was recorded immediately at the end of the 4-min walk, and a VO2Max value was estimated. This single-stage submaximal treadmill walking test was validated by correlating the estimated VO2Max and the measured VO2Max in the cross-validation group. A correlation (r) of 0.96 was obtained with a multiple correlation (R) of 0.86 (SEE = 4.85 mL kg−1 min−1) (Ebbeling et al. 1991).
Functional testing
Margaria power test: to measure stair-climbing power we utilized the Margaria Power Test (Margaria et al. 1966) which is not threshold limited. Participants ascended a 12-step staircase (each 17.5 cm) as rapidly as possible, with an approach length of 1–3 steps, without the use of railings, and with times recorded by an electronic stopwatch to the nearest 0.01 s upon subject foot contact with the fourth and eigth steps (beginning and end of test, respectively). The same evaluator recorded the times during all testing sessions for every participant; three trial times were recorded with the best time taken as the final measurement. Dynamic Power was determined by calculating the product of the participant’s weight in kilograms, the vertical distance ascended, and acceleration of gravity divided by the time elapsed. Test–retest reliability is 0.85, with CV’s of 2 % over 4-weeks of testing. 400-m Walk: traditional tests of habitual gait are sometimes not sufficiently sensitive to detect low levels of dysfunction. Therefore, we utilized an outdoor 400-m timed walk to the nearest 0.01 s with the participants walking as fast as possible. The reliability coefficient was 0.81.
Dynamic strength testing
Maximum voluntary muscle strength was assessed for the leg press and flat bench machine chest press exercises using the 1-RM method; dynamic strength testing always proceeded in this order, and the two lifts were separated by 3–5 min of passive rest. Prior to assessing maximal voluntary muscle strength, all study participants were familiarized with the resistance exercise movements used in 1-RM testing [i.e., leg press and flat bench machine chest press (bench press)]. The 1-RM protocol consisted of three sub-maximal warm-up sets of 6, 4, and 3 repetitions, respectively, each followed by an approximate 1-min rest period before the first 1-RM attempt. Loads were progressively increased with each 1-RM attempt (~5–20 pounds each attempt), and participants consistently needed approximately a 1- to 2-min rest period between each subsequent 1-RM attempt. A true 1-RM was determined in 2–6 attempts for every participant.
Strength-endurance testing
Strength-endurance was assessed ~5 min following dynamic strength testing, for the leg press and flat bench machine chest press exercises; strength-endurance testing always proceeded in this order, and the two lifts were separated by 3–5 min. Strength-endurance was determined by the maximum number of repetitions that could be performed with full range of motion and proper lifting technique across three repeated sets with each set separated by a 1-min rest period. At baseline, week 6, and 12, strength-endurance testing loads corresponded to 70 % 1-RM at baseline, week 6, and 12, respectively, and no warm-up was needed prior to strength-endurance testing. To calculate the outcome measure (volume-load) for this test, we calculated the product of the total number of complete repetitions performed across the three working sets and the testing load utilized (in kg).
Statistical analyses
Baseline characteristics including demographics, body composition components (LBM and fat mass), 1-RM strength, strength-endurance, and functional measures were compared using one-way ANOVA among the three treatment groups (Control, RT, and RTS) to detect any grouping effects. Repeated measure analysis of three visits by three treatment groups was conducted to assess the effects on body composition components, 1-RM strength, strength-endurance, and functional measures. Treatment-by-visit interactions were examined to determine whether three treatments had different outcome responses after 6 weeks (18 sessions) and 12 weeks (36 sessions) of training. This is a study with small sample size, so we used p < 0.1 as the threshold for significant interactions. Overall and pairwise comparisons between treatment groups for Baseline vs. week 6, Baseline vs. week 12, and week 6 vs. week 12 had also been conducted for outcomes with significant Tx-by-Visit interactions. Percentage changes from Baseline to week 12 of the ten outcome measures were calculated and compared using one-way ANOVA for global treatment effects. Pairwise comparisons between any pair of the three treatment groups were assessed in the ANOVA analysis using Tukey’s method to adjust for multiple comparisons.
Seven of the eight control group participants were later randomly assigned to either the RTS or RT treatment group and completed the 12-week resistance training program with (RTS) or without (RT) combined creatine and protein supplementation. This enabled us to compare the treatment effects of RT versus RTS with a larger sample size. Repeated measure analysis of two treatment by three visits had been applied to determine the effects on outcome measures. Comparisons between RT and RTS had then been conducted for the changes from Baseline to week 6, Baseline to week 12, and week 6 to week 12. Percentage changes from Baseline to week 12 was calculated and compared between RT and RTS group by standard t test.
Results
Repeated measure analyses and analyses on percentage changes from Baseline to week 12 had produced similar results. Furthermore, the primary purpose is to assess the effects of 12 weeks of training. Therefore, in this section, we only report the results from the percentage changes analyses. In the following parts, any statement of comparison versus a control group is based on three treatment groups (C, n = 8; RT, n = 7; RTS, n = 7), and any statement of comparison between RTS versus RT is based on two treatment groups (RTS, n = 11; RT, n = 10). Also, relative (percentage) change (increase and/or decrease) in any given outcome measure refers to the percentage change between two different study time points in that outcome measure. Last, out of 25 total participants who signed an informed consent form volunteering to take part in this investigation, only three study participants dropped out within 4 weeks of beginning the training program due to personal, health, and/or work-related reasons unassociated with the investigation and were not included in final statistical analyses.
Subject characteristics and body composition
The three treatment groups were comparable in baseline age, height, weight, LBM, fat mass, and percentage body fat (p > 0.05; Table 1). There was a marginally significant increase in LBM for RTS, compared with C, following 12 weeks of resistance training (p = 0.08; Table 2). Fat mass and percentage body fat did not change for RT and RTS, compared to C, following 12 weeks of resistance training (p > 0.05; Table 2).
RT experienced significant increases in absolute LBM at week 6 (60.2 ± 8.3 to 61.6 ± 9.4 kg; p < 0.05; Fig. 1a), significant decreases in absolute fat mass at week 12 (20.8 ± 4.2 to 19.0 ± 3.9 kg; p = 0.05), and significant decreases in percentage body fat at week 12 (25.7 ± 3.8 to 23.8 ± 4.0 % body fat; p = 0.05; Fig. 1b) compared to baseline. Furthermore, RTS experienced significant increases in absolute LBM at week 6 (56.4 ± 4.3 to 57.9 ± 3.4 kg; p < 0.01; Fig. 1a) and week 12 (56.4 ± 4.3 to 58.2 ± 3.4 kg; p < 0.01; Fig. 1a), no significant changes in absolute fat mass and significant decreases in percentage body fat at week 12 (23.9 ± 4.4 to 22.0 ± 4.4 % body fat; p < 0.01; Fig. 1b) compared to baseline.

a Absolute values (mean ± SD) showing change from pre- to post-resistance training (Baseline to week 6 to week 12) for the resistance training only group (RT) and resistance training combined with creatine/protein supplementation group (RTS) for lean body mass. *Statistically significant difference (p ≤ 0.05) from corresponding value at baseline. b Absolute values (mean ± SD) showing change from pre- to post-resistance training (Baseline to week 6 to week 12) for the resistance training only group (RT) and resistance training combined with creatine/protein supplementation group (RTS) for percentage body fat. *Statistically significant difference (p ≤ 0.05) from corresponding value at baseline. c Spaghetti plot of absolute values showing change from pre- to post-resistance training (Baseline to week 6 to week 12) for the resistance training only group (RT) and resistance training combined with creatine/protein supplementation group (RTS) for lean body mass
Upper and lower body 1-repetition maximum strength
The three treatment groups were comparable in baseline bench press 1-RM and leg press 1-RM (p > 0.05; Table 1). There were greater increases in bench press 1-RM for RTS (p < 0.01; Table 2) and RT (p = 0.01; Table 2) compared with C, following 12 weeks of resistance training. Also, there were greater increases in leg press 1-RM for RTS (p < 0.001; Table 2) and RT (p < 0.01; Table 2), compared with C, following 12 weeks of resistance training.
RT experienced significant increases in absolute bench press 1-RM at week 6 (47.3 ± 24.1 to 61.8 ± 30 kg; p < 0.001; Fig. 2b) and week 12 (47.3 ± 24.1 to 71.8 ± 30.5 kg; p < 0.0001; Fig. 2b) compared to baseline. In addition, RT experienced significant increases in absolute bench press 1-RM at week 12 (61.8 ± 30 to 71.8 ± 30.5 kg; p = 0.005; Fig. 2b) compared to week 6. RTS experienced significant increases in absolute bench press 1-RM at week 6 (44.1 ± 13.6 to 60.9 ± 13.2 kg; p < 0.0001; Fig. 2b) and week 12 (44.1 ± 13.6 to 72.7 ± 15 kg; p < 0.0001; Fig. 2b) compared to baseline. RTS also experienced significant increases in absolute bench press 1-RM at week 12 (60.9 ± 13.2 to 72.7 ± 15 kg; p = 0.01; Fig. 2b) compared to week 6.

a Absolute values (mean ± SD) showing change from pre- to post-resistance training. (Baseline to week 6 to week 12) for the resistance training only group (RT) and resistance training combined with creatine/protein supplementation group (RTS) for 1-repetition maximum (1-RM) leg press strength. *Statistically significant difference (p ≤ 0.05) from corresponding value at baseline; †statistically significant difference (p ≤ 0.05) from corresponding value at week 6. b Absolute values (mean ± SD) showing change from pre- to post-resistance training (Baseline to week 6 to week 12) for the resistance training only group (RT) and resistance training combined with creatine/protein supplementation group (RTS) for 1-repetition maximum (1-RM) bench press strength. *Statistically significant difference (p ≤ 0.05) from corresponding value at baseline; †statistically significant difference (p ≤ 0.05) from corresponding value at week 6. c Spaghetti plot of absolute values showing change from pre- to post-resistance training (Baseline to week 6 to week 12) for the resistance training only group (RT) and resistance training combined with creatine/protein supplementation group (RTS) for 1-repetition maximum (1-RM) leg press strength. d Spaghetti plot of absolute values showing change from pre- to post-resistance training (Baseline to week 6 to week 12) for the resistance training only group (RT) and resistance training combined with creatine/protein supplementation group (RTS) for 1-repetition maximum (1-RM) bench press strength
RT experienced significant increases in absolute leg press 1-RM at week 6 (148.2 ± 59.1 to 204.1 ± 62.3 kg; p = 0.0001; Fig. 2a) and week 12 (148.2 ± 59.1 to 327.7 ± 87.3 kg; p < 0.0001; Fig. 2a) compared to baseline. In addition, RT experienced significant increases in absolute leg press 1-RM at week 12 (204.1 ± 62.3 to 327.7 ± 87.3 kg; p < 0.0001; Fig. 2a) compared to week 6. RTS experienced significant increases in absolute leg press 1-RM at week 6 (153.2 ± 48.6 to 260.5 ± 86.4 kg; p = 0.0001; Fig. 2a) and week 12 (153.2 ± 48.6 to 363.2 ± 131.4 kg; p < 0.0001; Fig. 2a) compared to baseline. RTS experienced significant increases in absolute leg press 1-RM at week 12 (260.5 ± 86.4 to 363.2 ± 131.4 kg; p < 0.001; Fig. 2a) compared to week 6.
Upper and lower body strength-endurance
The three treatment groups (C, n = 8; RT, n = 7; RTS, n = 7) were comparable in baseline bench press strength-endurance and leg press strength-endurance (p > 0.05; Table 1). There were greater increases in bench press strength-endurance for RT (p = 0.01; Table 2) and RTS (p = 0.005; Table 2), compared with C, following 12 weeks of resistance training. Also, there were greater increases in leg press strength-endurance for RT (p < 0.0001; Table 2) and RTS (p < 0.0001; Table 2), compared with C, following 12 weeks of resistance training.
RT experienced significant increases in absolute bench press strength-endurance at week 6 (589 ± 297 to 1,151 ± 416 kg; p = 0.0001; Fig. 3b) and week 12 (589 ± 297 to 1212 ± 524 kg; p < 0.0001; Fig. 3b) compared to baseline. RTS experienced significant increases in absolute bench press strength-endurance at week 6 (625 ± 199 to 1,180 ± 302 kg; p < 0.0001; Fig. 3b) and week 12 (625 ± 199 to 1,451 ± 450 kg; p < 0.0001; Fig. 3b) compared to baseline. In addition, RTS experienced marginally significant increases in absolute bench press strength-endurance at week 12 (1,180 ± 302 to 1,451 ± 450 kg; p = 0.06; Fig. 3b) compared to week 6.

a Absolute values (mean ± SD) showing change from pre- to post-resistance training (Baseline to week 6 to week 12) for the resistance training only group (RT) and resistance training combined with creatine/protein supplementation group (RTS) for leg press strength-endurance. *Statistically significant difference (p ≤ 0.05) from corresponding value at baseline; †statistically significant difference (p ≤ 0.05) from corresponding value at Week 6. b Absolute values (mean ± SD) showing change from pre- to post-resistance training (Baseline to week 6 to week 12) for the resistance training only group (RT) and resistance training combined with creatine/protein supplementation group (RTS) for bench press strength-endurance. *Statistically significant difference (p ≤ 0.05) from corresponding value at baseline
RT experienced significant increases in absolute leg press strength-endurance at week 6 (2,970 ± 1,632 to 7,175 ± 2,659 kg; p < 0.0,001; Fig. 3a) and week 12 (2,970 ± 1,632 to 9,283 ± 2,084 kg; p < 0.0,001; Fig. 3a) compared to baseline. RTS experienced significant increases in absolute leg press strength-endurance at week 6 (3,831 ± 2,027 to 8,850 ± 3,286 kg; p = 0.0001; Fig. 3a) and week 12 (3,831 ± 2,027 to 11,999 ± 4,226 kg; p < 0.0001; Fig. 3a) compared to baseline. In addition, RTS experienced significant increases in absolute leg press strength-endurance at week 12 (8,850 ± 3,286 to 11,999 ± 4,226 kg; p < 0.05; Fig. 3a) compared to week 6.
Functional measures
The three treatment groups (C, n = 8; RT, n = 7; RTS, n = 7) were comparable in baseline Margaria stair-climb power, 400-m walk time, and estimated VO2Max (p > 0.05; Table 1). There were marginally significant increases in Margaria stair-climb power for RTS compared with C (p = 0.14; Table 2) and compared with RT (p = 0.07; Table 2), following 12 weeks of resistance training. In addition, there were marginally significant decreases in 400-m walk time for RT (p < 0.05; Table 2), compared with C, following 12 weeks of resistance training. Last, there were marginally significant changes in VO2Max for RTS, compared with C, following 12 weeks of resistance training (p = 0.06; Table 2).
RT experienced no significant changes in Margaria stair-climb power, following 12 weeks of resistance training (p > 0.05; Table 2) compared to C. However, RTS experienced marginally significant increases in Margaria stair-climb power at week 12 (p = 0.14; Table 2) compared to C. Further, analyses between the two treatment groups (RT, n = 10; RTS, n = 11) revealed that increases in stair-climb power experienced by RTS at week 12 were also marginally significantly greater than RT at week 12 (p = 0.06; Table 3).
RT experienced significant decreases in absolute 400-m walk time at week 6 (207 ± 29 to 190 ± 29 s; p < 0.05) and week 12 (207 ± 29 to 183 ± 32 s; p < 0.005) compared to baseline. Furthermore, RTS experienced significant decreases in absolute 400-m walk time at week 6 (185 ± 22 to 169 ± 30 s; p < 0.01) and Week 12 (185 ± 22 to 169 ± 31 s; p < 0.01) compared to baseline.
RT experienced significant increases in absolute estimated VO2Max at week 6 (34.6 ± 1.9 to 36.9 ± 2.7 ml/kg/min; p < 0.01) and week 12 (34.6 ± 1.9 to 36.4 ± 2.7 ml/kg/min; p = 0.01) compared to baseline. Furthermore, RTS experienced significant increases in absolute estimated VO2Max at week 12 (36.3 ± 2.7 to 37.5 ± 3.3 ml/kg/min; p = 0.05) compared to baseline.
Dietary records
At baseline and study week 12, dietary intake was assessed via a 3-day dietary record in order to determine if any changes in the participants’ diet occurred throughout the intervention period. Dietary patterns were not significantly different among the three treatment groups.
Side effects
Subjects tolerated the creatine combined with protein supplementation protocol very well with no reports of gastrointestinal distress, muscular cramping, or any other subjective symptoms during the study.
Discussion
The current investigation demonstrated that 12 weeks of resistance training, utilizing a non-linear periodization scheme, with and without combined creatine and protein supplementation, enhanced upper and lower body muscular strength and strength-endurance in older men. Furthermore, resistance training in combination with creatine and protein supplementation enhanced improvements in dynamic stair-climbing power greater than resistance training alone. Finally, this study suggests that combining resistance training with creatine and protein supplementation results in notable changes in muscular performance and body composition, potentially as a result of augmented increases in LBM, which were not experienced through resistance training alone.
Research investigating the effects of resistance training without supplementation on alterations in LBM in older men has produced conflicting results with some studies reporting significant increases in LBM (Kraemer et al. 1999; Hakkinen et al. 2000; Weinheimer et al. 2012) and others reporting no increases (Campbell et al. 1994; Bermon et al. 1998). Similarly, studies examining the effect of resistance training combined with creatine and/or protein supplementation on LBM in older men have produced inconsistent results (Brose et al. 2003; Verdijk et al. 2009; Weinheimer et al. 2012). Overall, these equivocal findings may be explained by major differences in supplementation regimens including acute dosage amounts, frequency of dosing, and total duration of supplementation, as well as resistance training programing including exercise selection, training volume and intensity, frequency of training, and the duration of the training intervention. Likewise, results may be influenced by the type of instrumentation used across different studies and, thus, the precision of measurement to determine changes in LBM (e.g., DXA versus skinfolds).
By week 6 in the current investigation both RT and RTS increased LBM (statistically non-significant), and only RTS experienced additional increases in LBM from week 6 to week 12 that was marginally significantly different from baseline (compared to week 12). In addition, by week 12, only RTS experienced marginally significant decreases in percentage body fat compared to baseline. Therefore, the body re-composition experienced by RTS appears to be a result of increases in LBM with minimal reductions in fat mass.
The relative increases in strength reported in the current study are greater compared to previous studies examining the effects of resistance training with and without a creatine/protein supplementation in older men. Most studies have reported relative increases in strength ranging from 15 to 60 %, with these increases being exercise-specific (Bermon et al. 1998; Kraemer et al. 1999; Hakkinen et al. 2000; Brose et al. 2003). Furthermore, previous studies have reported ambiguous findings regarding the influence of resistance training with and without creatine supplementation on strength in older men; while some studies indicate that combined resistance training and supplementation lead to enhanced strength adaptations (Bermon et al. 1998; Chrusch et al. 2001; Gotshalk et al. 2002; Brose et al. 2003; Candow et al. 2008) compared to resistance training alone, other studies have concluded that creatine supplementation does not elicit additional improvements in strength when combined with a resistance training program (Eijnde et al. 2003; Bemben et al. 2010). Similar to the evidence pertaining to the effects of resistance training with and without supplementation on changes in LBM, these equivocal results may be explained by major differences in supplementation regimens and resistance training programing across studies.
The significant increases in muscular strength for RT and RTS in response to our resistance training program was expected; the strength improvements indicate that training loads used throughout the resistance training program were individually progressed in a safe and effective manner and employed a progressive overload/challenge to the participants’ neuromuscular systems to elicit muscular performance-enhancing neuromuscular adaptations without inducing excessive neuromuscular fatigue. Importantly, both RT and RTS continued to enhance both upper and lower body strength, with no apparent plateau in strength gains, through the entire 12 weeks of resistance training; there were significant increases in bench press strength ranging from a group mean average of 50 % (RT) to 72 % (RTS) and in leg press strength ranging from a group mean average of 113 % (RT) to 130 % (RTS). Therefore, RTS displayed, on average, an approximately 22 and 17 % greater increase in bench press strength and leg press strength, respectively, following 12 weeks of resistance training, but these relative change differences between RT and RTS were not statistically different. Last, the strength improvements in the current investigation were the result of an aggressively progressed, high volume, and intensity resistance training program; yet, there were no injuries reported. Our findings support periodized resistance training programs incorporating relatively high training volumes and intensities, while incorporating relatively short rest interval lengths in between sets can be safe and extremely effective for healthy older men, while promoting muscular strength performance improvements that are critically important to minimize fall risk and enhance overall health in older adults.
Currently, the most popular mechanism to explain the efficacy of creatine supplementation in both young and older adults is the enhancement of the PCr energy system allowing users to maintain a given (or greater) resistance training intensity for longer durations of time (i.e., increased total training volume-load and enhanced recovery in between training sets). Nevertheless, research till day also appears to be equivocal regarding the effects of creatine supplementation with and without protein supplementation on muscular endurance/time to fatigue in older adults (Dalbo et al. 2009). While creatine supplementation combined with resistance training has been found to enhance muscular endurance (Chrusch et al. 2001) and work capacity, and alone, reduces muscle fatigue (Rawson et al. 1999); other studies have found creatine supplementation combined with resistance training to have no significant effect on measures of dynamic endurance (Bermon et al. 1998) and time to fatigue (supplementation alone) (Jakobi et al. 2001). As previously mentioned, the inconsistency in findings may be explained by varying supplementation regimens, resistance training programs, and intervention durations.
We examined strength-endurance performance, which was measured by total volume-load (sets x repetitions x load) across three repeated sets of leg press and bench press to volitional fatigue at 70 % 1-RM; the strength-endurance testing loads were relative to the new 1-RM measures at each of the three testing time points (Baseline, week 6, and week 12) and, thus, were not absolute loads. Both RT and RTS experienced significant increases in strength-endurance; however, only RTS experienced additional gains in leg press strength-endurance that were significantly different between the week 6 and week 12 time points. Moreover, RT appeared to plateau in bench press strength-endurance between the week 6 and week 12 time points, while RTS continued to enhance bench press strength-endurance performance between those time points. These differences may be the result of several factors: (1) supplementation may be optimal to achieve maximal improvements in strength-endurance from resistance training, but an extended training period is necessary to adequately elevate muscle PCr concentrations through creatine loading and maintenance dosing phases; (2) an extended training period is necessary to allow for a sufficient time period for training-induced adaptations to occur as a result of, what may be, subtle increases in work capacity over multiple training bouts (i.e., enhanced tolerance of greater training volume-loads across training days and cycles); and (3) subtle differences between groups would not have been detected because a greater sample size would have been required. Our results most closely corroborate reports from a study conducted by Chrusch et al. (2001) that reported lower body muscle strength (1-RM leg press) and endurance (leg press) were significantly enhanced with creatine supplementation, while having no significant effect on maximal upper body strength (1-RM bench press) and endurance (bench press).
The measurements of functional performance used in the current study showed varied improvements between RT and RTS following the resistance training program. Group mean averages for Margaria stair-climbing power increased 11.5 and 38 % for RT and RTS, respectively. Furthermore, group mean averages of −11 and −10 % reductions for RT and RTS, respectively, in 400-m walking time are consistent with findings reported by other investigators (Buchner et al. 1996; Marsh et al. 2006). Our results confirm findings by Marsh et al. (Marsh et al. 2006) from a cross-sectional analysis of 384 women and 336 men, ≥65 years of age. They concluded that lower extremity muscle strength and power are both important predictors of 400-m walking time. Collectively, the functional performance results from the current study suggest that a periodized resistance training program with sufficient training volume and intensity, with and/or without combined creatine and protein supplementation, can increase LBM and improve muscular strength, which may lead to performance enhancements in functional tasks that have relevance to activities of daily living.
A limited number of studies have investigated the possible benefits of supplementation with creatine and protein on body composition in older adults and reported equivocal findings (Bermon et al. 1998; Rawson et al. 1999; Chrusch et al. 2001; Brose et al. 2003). Our findings indicate that RTS experienced marginally significant increases in LBM and marginally significant decreases in body fat percentage, when compared to C, these body composition outcomes were not statistically significant between the two groups. It is possible that significant differences were not observed between groups because: (1) resistance training combined with supplementation may be optimal to achieve maximal improvements in LBM and body composition, but not entirely necessary, if periodized resistance training alone, which incorporates a safe and progressive overload through varying combinations of higher volume/moderate intensity, lower volume/higher intensity, explosive/power training stimuli, and short rest interval lengths can induce marked improvements in body composition, muscular performance, and functional capacity; and (2) subtle differences between groups would not have been detected because a greater sample size or longer training period would have been required.
Current data regarding timing of protein ingestion with resistance exercise, in both young and older men, gives equivocal insight into the most appropriate time for older adults to consume protein in the context of resistance exercise to optimize muscle anabolism (Breen and Phillips 2012). A single bout of resistance-type exercise accelerates muscle protein synthesis within 2–4 h (Phillips et al. 1997). Muscle protein breakdown is also stimulated following a single bout of resistance-type exercise, although, to a lesser extent than protein synthesis (Biolo et al. 1995; Phillips et al. 1997). However, in the absence of nutrient intake (i.e., protein), an acute bout of resistance training can result in a negative net muscle protein balance (Phillips et al. 1997). Consequently, it appears both resistance-type exercise and nutrition are required to achieve a positive net protein balance leading to hypertrophy. Accordingly, some evidence suggests that post-resistance exercise protein ingestion represents an effective strategy to augment the anabolic response to training (Koopman et al. 2007; Koopman and van Loon 2009), and the timing of protein intake is critical to optimize the anabolic response to training (i.e., post-resistance exercise intake) (Esmarck et al. 2001; Koopman et al. 2007; Koopman and van Loon 2009). In Contrast, Verdijk et al. Verdijk et al. (2009) suggest that, provided adequate dietary protein is consumed, protein supplements taken in close proximity to resistance exercise do not augment hypertrophy in older adults. Collectively, research in older adult populations examining the optimal timing of protein intake to maximize resistance exercise-induced muscle protein anabolism is scarce (Esmarck et al. 2001; Onambele-Pearson et al. 2010; Dideriksen et al. 2011), and it appears that protein ingestion at doses of at least 20 g at intervals over a 24-h-period post-resistance exercise may be able to elicit a potent anabolic response in older adults and promote muscle protein accretion for hypertrophy (Breen and Phillips 2012).
In the current study, RTS ingested a whey/milk RTD protein supplement immediately after the cessation of each resistance exercise bout; this may be one explanation for the marginally significant enhancements in LBM, compared to C, which RTS, not RT, experienced. Even though these changes in LBM were not significantly different between RTS and RT, this observation indicates that more research is warranted to assess the impact of the timing of nutrient intake on the skeletal muscle adaptive responses to resistance training in older adults, as well as the possible mechanisms leading to enhanced acute and chronic skeletal muscle adaptive responses.
Previous literature suggests that there are large variances in the response to certain interventions including exercise-, nutrition-, and supplementation-related. The literature supports the notion of responders and non-responders to a particular treatment, indicating that there are inter-individual differences in response to certain stimuli such as chronic training programs (Bouchard and Malina 1986; Bouchard et al. 1992). Further, strong evidence suggests that there may be inter-individual differences in response to nutritional ergogenic aids such as creatine monohydrate; humans may have similar anatomical and physiological characteristics, but biological variability, perhaps due to genetic differences, may also account for the efficacy of nutritional interventions (Williams 1998; Syrotuik and Bell 2004; Bemben and Lamont 2005). Due to the likelihood that there may be some underlying biological factors that influence individuals who are responders and those who do not respond to acute oral creatine monohydrate ingestion, which assists in partially explaining the dichotomy of published performance results including our results in the present study, Syrotuik and Bell (2004) conducted a study to describe the physiological profile of responders versus non-responders to a 5-day creatine monohydrate load (0.3 g/kg BW/day). Results from this study indicated that individuals’ response to a creatine monohydrate loading period (i.e., extent of acute Cr uptake by the muscle cell) was variable and supports a person-by-treatment response with three responder types identified: 1. True responders; 2. Quasi-responders; and 3. Non-responders.
Although it is difficult to identify a specific and singular biological or determining factor that will predict those who will load (responder), versus those who will not load (non-responder) in response to an acute oral creatine monohydrate supplementation schedule, there appears to be a few related factors including: initial levels of cellular Cr + PCr with the responders generally displaying the lowest initial pre-load concentrations; muscle fiber type with responders exhibiting a greater percentage of type II muscle fibers; and, muscle fiber cross-sectional area (CSA) and fat-free mass content with responders showing the greatest pre-load muscle fiber CSA and fat-free mass (Syrotuik and Bell 2004). Therefore, in general, non-responders may have higher initial levels of cellular Cr + PCr, less type II muscle fibers, smaller muscle fiber CSA, and lower fat-free mass. Finally, according to Syrotuik and Bell (2004), the only 1-RM improvements associated with the 5-day creatine monohydrate load appeared in the “true responder” group. Thus, as the body composition and performance data from the present study confirm strength and conditioning professionals and clinical practitioners should consider that there may be a pre-existing muscle morphological profile, which determines whether an athlete, client, and/or patient will experience performance-based improvements from creatine monohydrate supplementation.
Taken together, the results from our study confirm that periodized resistance training is a highly effective countermeasure to age-related losses in skeletal muscle mass, muscular performance, and functional capacity. In addition, combined creatine and protein supplementation, in conjunction with a periodized resistance training program, elicited no adverse side effects and may augment these improvements. Last, these findings indicate that future research is needed with a larger sample size and longer resistance training/supplementation intervention to determine if the effects of combined resistance training and supplementation can lead to enhanced chronic body re-composition, muscular performance adaptations, and functional capacity over a longer period of time compared to RT alone.
The present study was limited by a small number of study participants in each training group (RT, n = 10; RTS, n = 11) and a relatively short training program duration of 12 weeks; future investigations should incorporate larger sample sizes to allow for maximal statistical power in addition to relatively long training programs (i.e., 16–24 weeks). Also, even though monitoring the study participants’ diet via a 3-day recall at study baseline and study week 12 revealed non-significant differences between RT and RTS, it is a limitation to assume that all study participants were eating similar to the recall logs and/or their normal diets for the entire duration of the investigation. Furthermore, the present study only examined older, untrained men; future research in this area could include investigations of middle-aged men, untrained and trained, and/or studies comparing young and older men, perhaps with a focus on responders versus non-responders. Last, the resistance exercise prescription in the present study utilized “RM loads,” which are commonly prescribed in addition to “%1-RM loads,” and this study did not include a determination of the molecular mechanisms contributing to the adaptive responses observed. Therefore, within a single investigation, using the same study sample, future research should aim to compare acute responses (e.g., acute hormonal/molecular responses), body composition changes, and muscular/functional performance changes in response to periodized resistance training alone, supplementation alone, and combined periodized resistance training and supplementation.
In summary, 12 weeks of periodized resistance training resulted in enhancements in LBM and body composition, improvements in upper and lower body muscular strength and strength-endurance, and increases in functional task performance in older men (60–80 years of age). In addition, participants who supplemented with creatine and protein experienced greater, but statistically non-significant, increases in LBM and improvements in relative upper and lower body maximum strength, as well as statistically significant increases Margaria stair-climbing power. While the mechanisms eliciting these changes remain to be elucidated, our results add to a body of literature suggesting that creatine combined with protein supplementation may not provide additional benefits to older men performing resistance-type exercise, while periodized resistance training alone, as prescribed in this investigation, may lead to optimal and augmented muscular and functional performance improvements in older adults.
Abbreviations
- ADL:
-
Activities of daily living
- BW:
-
Body weight
- C:
-
Control study group
- Cr:
-
Creatine
- CSA:
-
Cross-sectional area
- DXA:
-
Dual-energy X-ray absorptiometry
- LBM:
-
Lean body mass
- PCr:
-
Phosphocreatine
- PAR-Q:
-
Physical Activity Readiness Questionnaire
- RTD:
-
Ready-to-drink
- RM:
-
Repetition maximum
- RT:
-
Resistance training only study group
- RTS:
-
Resistance training plus combined creatine and protein supplementation study group
- RT program:
-
Resistance training program
References
Andersen LL, Tufekovic G et al (2005) The effect of resistance training combined with timed ingestion of protein on muscle fiber size and muscle strength. Metabolism 54(2):151–156
Becque MD, Lochmann JD et al (2000) Effects of oral creatine supplementation on muscular strength and body composition. Med Sci Sports Exerc 32(3):654–658
Bemben MG, Lamont HS (2005) Creatine supplementation and exercise performance. Sports Med 35(2):107–125
Bemben MG, Witten MS et al (2010) The effects of supplementation with creatine and protein on muscle strength following a traditional resistance training program in middle-aged and older men. J Nutr Health Aging 14(2):155–159
Bermon S, Venembre P et al (1998) Effects of creatine monohydrate ingestion in sedentary and weight-trained older adults. Acta Physiol Scand 164(2):147–155
Biolo G, Maggi SP et al (1995) Increased rates of muscle protein turnover and amino acid transport after resistance exercise in humans. Am J Physiol 268(3 Pt 1):E514–E520
Bouchard C, Malina RM (1986) Sport and human genetics. Human Kinetics, Champaign
Bouchard C, Dionne FT et al (1992) Genetics of aerobic and anaerobic performances.In: JH Hollosky (ed) Exerc Sport Sci Rev vol 20, Williams and Wilkins, Baltimore pp 27–58
Breen L, Phillips SM (2012) Nutrient interaction for optimal protein anabolism in resistance exercise. Curr Opin Clin Nutr Metab Care 15(3):226–232
Brose A, Parise G et al (2003) Creatine supplementation enhances isometric strength and body composition improvements following strength exercise training in older adults. J Gerontol A Biol Sci Med Sci 58(1):11–19
Buchner DM, Larson EB et al (1996) Evidence for a non-linear relationship between leg strength and gait speed. Age Ageing 25(5):386–391
Campbell WW, Crim MC et al (1994) Increased protein requirements in elderly people: new data and retrospective reassessments. Am J Clin Nutr 60(4):501–509
Campbell WW, Barton ML Jr et al (1999) Effects of an omnivorous diet compared with a lactoovovegetarian diet on resistance-training-induced changes in body composition and skeletal muscle in older men. Am J Clin Nutr 70(6):1032–1039
Campbell WW, Trappe TA et al (2001) The recommended dietary allowance for protein may not be adequate for older people to maintain skeletal muscle. J Gerontol A Biol Sci Med Sci 56(6):M373–M380
Candow DG, Little JP et al (2008) Low-dose creatine combined with protein during resistance training in older men. Med Sci Sports Exerc 40(9):1645–1652
Chodzko-Zajko WJ, Proctor DN et al (2009) American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med Sci Sports Exerc 41(7):1510–1530
Chrusch MJ, Chilibeck PD et al (2001) Creatine supplementation combined with resistance training in older men. Med Sci Sports Exerc 33(12):2111–2117
Crewther B, Keogh J et al (2006) Possible stimuli for strength and power adaptation: acute hormonal responses. Sports Med 36(3):215–238
Cribb PJ, Hayes A (2006) Effects of supplement timing and resistance exercise on skeletal muscle hypertrophy. Med Sci Sports Exerc 38(11):1918–1925
Dalbo VJ, Roberts MD et al (2009) The effects of age on skeletal muscle and the phosphocreatine energy system: can creatine supplementation help older adults. Dyn Med 8:6
Dideriksen KJ, Reitelseder S et al (2011) Stimulation of muscle protein synthesis by whey and caseinate ingestion after resistance exercise in elderly individuals. Scand J Med Sci Sports 21(6):e372–e383
Earnest CP, Snell PG et al (1995) The effect of creatine monohydrate ingestion on anaerobic power indices, muscular strength and body composition. Acta Physiol Scand 153(2):207–209
Ebbeling CB, Ward A et al (1991) Development of a single-stage submaximal treadmill walking test. Med Sci Sports Exerc 23(8):966–973
Eijnde BO, Van Leemputte M et al (2003) Effects of creatine supplementation and exercise training on fitness in men 55–75 year old. J Appl Physiol 95(2):818–828
Esmarck B, Andersen JL et al (2001) Timing of postexercise protein intake is important for muscle hypertrophy with resistance training in elderly humans. J Physiol 535(Pt 1):301–311
Fiatarone MA, Marks EC et al (1990) High-intensity strength training in nonagenarians. Effects on skeletal muscle. JAMA 263(22):3029–3034
Gotshalk LA, Volek JS et al (2002) Creatine supplementation improves muscular performance in older men. Med Sci Sports Exerc 34(3):537–543
Hakkinen K, Pakarinen A et al (2000) Basal concentrations and acute responses of serum hormones and strength development during heavy resistance training in middle-aged and elderly men and women. J Gerontol A Biol Sci Med Sci 55(2):B95–B105
Harris RC, Soderlund K et al (1992) Elevation of creatine in resting and exercised muscle of normal subjects by creatine supplementation. Clin Sci (Lond) 83(3):367–374
Hulmi JJ, Kovanen V et al (2009) Acute and long-term effects of resistance exercise with or without protein ingestion on muscle hypertrophy and gene expression. Amino Acids 37(2):297–308
Hultman E, Soderlund K et al (1996) Muscle creatine loading in men. J Appl Physiol 81(1):232–237
Hunter GR, McCarthy JP et al (2004) Effects of resistance training on older adults. Sports Med 34(5):329–348
Jakobi JM, Rice CL et al (2001) Neuromuscular properties and fatigue in older men following acute creatine supplementation. Eur J Appl Physiol 84(4):321–328
Koopman R, van Loon LJ (2009) Aging, exercise, and muscle protein metabolism. J Appl Physiol 106(6):2040–2048
Koopman R, Saris WH et al (2007) Nutritional interventions to promote post-exercise muscle protein synthesis. Sports Med 37(10):895–906
Kraemer WJ, Marchitelli L et al (1990) Hormonal and growth factor responses to heavy resistance exercise protocols. J Appl Physiol 69(4):1442–1450
Kraemer WJ, Hakkinen K et al (1999) Effects of heavy-resistance training on hormonal response patterns in younger vs older men. J Appl Physiol 87(3):982–992
Kreider RB, Ferreira M et al (1998) Effects of creatine supplementation on body composition, strength, and sprint performance. Med Sci Sports Exerc 30(1):73–82
Lindle RS, Metter EJ et al (1997) Age and gender comparisons of muscle strength in 654 women and men aged 20–93 year. J Appl Physiol 83(5):1581–1587
Margaria R, Aghemo P et al (1966) Measurement of muscular power (anaerobic) in man. J Appl Physiol 21(5):1662–1664
Marsh AP, Miller ME et al (2006) Lower extremity strength and power are associated with 400-meter walk time in older adults: The InCHIANTI study. J Gerontol A Biol Sci Med Sci 61(11):1186–1193
Onambele-Pearson GL, Breen L et al (2010) Influences of carbohydrate plus amino acid supplementation on differing exercise intensity adaptations in older persons: skeletal muscle and endocrine responses. Age (Dordr) 32(2):125–138
Phillips SM, Tipton KD et al (1997) Mixed muscle protein synthesis and breakdown after resistance exercise in humans. Am J Physiol 273(1 Pt 1):E99–E107
Rawson ES, Wehnert ML et al (1999) Effects of 30 days of creatine ingestion in older men. Eur J Appl Physiol Occup Physiol 80(2):139–144
Samson MM, Meeuwsen IB et al (2000) Relationships between physical performance measures, age, height and body weight in healthy adults. Age Ageing 29(3):235–242
Smith SA, Montain SJ et al (1998) Creatine supplementation and age influence muscle metabolism during exercise. J Appl Physiol 85(4):1349–1356
Stone MH, Sanborn K et al (1999) Effects of in-season (5 weeks) creatine and pyruvate supplementation on anaerobic performance and body composition in American football players. Int J Sport Nutr 9(2):146–165
Syrotuik DG, Bell GJ (2004) Acute creatine monohydrate supplementation: adescriptive physiological profile of responders vs nonresponders. J Strength Cond Res 18(3):610–617
Verdijk LB, Jonkers RA et al (2009) Protein supplementation before and after exercise does not further augment skeletal muscle hypertrophy after resistance training in elderly men. Am J Clin Nutr 89(2):608–616
Volek JS, Duncan ND et al (1999) Performance and muscle fiber adaptations to creatine supplementation and heavy resistance training. Med Sci Sports Exerc 31(8):1147–1156
Weinheimer EM, Conley TB et al (2012) Whey protein supplementation does not affect exercise training-induced changes in body composition and indices of metabolic syndrome in middle-aged overweight and obese adults. J Nutr 142(8):1532–1539
Williams MH (1998) The ergogenics edge. Human Kinetics, Champaign
Acknowledgments
The authors would like to thank the study participants, University of Southern California Clinical Exercise Research Center staff, and Adriana Del Padilla for their contribution to the successful completion of the experimental protocol.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by William J. Kraemer.
Rights and permissions
About this article
Cite this article
Villanueva, M.G., He, J. & Schroeder, E.T. Periodized resistance training with and without supplementation improve body composition and performance in older men. Eur J Appl Physiol 114, 891–905 (2014). https://doi.org/10.1007/s00421-014-2821-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-014-2821-1