
Abstract
Purpose
Thoracic kyphosis (TK) remained in the shadow of lumbar lordosis. Based on Berthonnaud and Roussouly segmentation, TK is divided into two arches: upper TK (UTK) and lower TK (LTK). The purpose of this study is to propose a normative description of the TK arches in an asymptomatic adults’ population and their correlation with spinal and pelvic parameters.
Methods
This is an observational study performed on asymptomatic healthy Caucasians volunteers aged between 18 and 45 years. Each patient had a standardized standing biplanar full spine X-rays. Using KEOPS®, sacropelvic parameters and global spinal parameters (LL, TK) as well as the inflexion point location were measured. The upper lumbar lordosis angle (ULL) as well as LTK and UTK was calculated. Patients were classified according to Roussouly morphotypes of normal spine.
Results
A total of 373 adults (F/M = 1.4/1) were enrolled with mean age of 27 years. Mean UTK averaged 25.8°, while mean LTK averaged 19.8° (p < 0.001). UTK angle values were statistically the same in the five different Roussouly spinal shapes (p > 0.05), while LTK values were variable among different Roussouly spine subtypes (p < 0.05). Finally, TK showed the highest correlation with the LL mainly with the ULL (Pearson = 0.66).
Conclusion
In asymptomatic young adults, thoracic kyphosis is composed by two unequal arches, a stable UTK and a variable LTK, with an apex around T8 and T9 vertebra, depending on the spinal morphotype according to Roussouly classification. This should be taken into consideration when analyzing spine sagittal compensation and preparing corrections to minimize risk of mechanical complications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Human bipedalism is an exclusive, stable and ergonomic posture. This upright position adoption has resulted in the ability of pelvis retroversion and in the appearance of characteristic spinal curves [1]. From Hippocrates, then Galen, the spinal curvatures are classically segmented in sacral kyphosis, lumbar lordosis, thoracic kyphosis and cervical lordosis [2]. Kyphosis originates from Greek kyphos (κυφός) meaning “hump” [2]. While lumbar lordosis (LL) was extensively studied in recent literature, thoracic (TK) remains in the shadow compared to its lumbar counterpart [3, 4].
TK is classically measured between the lower endplate of T12 and the upper endplate of T1 (or T3) [5]. Nonetheless, since the description of the inflexion point by Berthonaud et al. [3] and the description of the classical LL segmentation by Roussouly et al. [6, 7], the maximal TK that spans the spine from an inflexion point to another should be used to define TK (Fig. 1). Based on the description of Berthonaud et al., the LL was divided into two arches: the lower LL (LLL) that is always equal to the sacral slope (SS) and the upper LL (ULL) that was found to be around 20° [3]. Nonetheless, the authors described similar two arches for the TK: the upper TK (UTK) and the lower TK (LTK) that were defined based on the apex of the TK (Fig. 1). ULL and LTK are mathematically equal (alternate angles) [3]. Recently, Clément et al. used a different sagittal segmentation to simplify the estimation of the theoretical TK (TTK) and found it equal to: TTK = 2*(PT + LL-PI) [8] (PI : pelvic incidence; PT: pelvic tilt) without clearly defining the normal values of the two arches of the TK (Fig. 2).

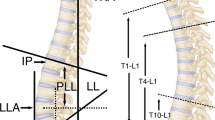
Spinal segmentation as described by Berthonnaud et al. [4]. Each curve is limited by two inflexion points (big yellow dots). The lumbar lordosis is divided into two arches separated by the apex (the point where the tangent to the curve is vertical). The lower lumbar lordosis is equal to sacral slope. The upper lumbar lordosis is equal to the lower thoracic kyphosis

Representation of the segmentation described by Berthonnaud et al. [4] (in red) and by Clément et al. [8] in white. The former segmentation is based on inflexion points and apexes of curves, while the latter is totally arbitrary. Note that even if the angles are equal, the number of vertebras forming every curve is different
To our knowledge, no study has evaluated the values of the two arches of TK in asymptomatic individuals. This study aims to propose a normative description of the two arches of TK in an asymptomatic population and to study their correlation to spinal and pelvic parameters as well as to the Roussouly subtypes of normal spine. An external validation of the TK formula proposed by Clément et al. is to be attempted.
Methods
This observational study was conducted on asymptomatic patients aged less than 45 years. The entire population was Caucasian, and all patients consented on participating in the study. Inclusion criteria were (1) patients aged between 18 and 45 years, and (2) absence of current or history of spinal, hip or pelvic disease. Exclusion criteria were (1) history of low back pain, (2) hip or lower limb discrepancy or disease, (3) radiographic abnormalities such as scoliosis, spondylolisthesis or Scheuermann’s kyphosis and (4) early degenerative changes.
The radiographic protocol was standardized. For each subject, simultaneous biplanar X-ray images by slot scanning of the whole body in the upright position were done using ultra-low radiation doses. The resulting X-ray included the area from the base of the skull to the proximal femur with care to limit the coronal pelvic rotation. Subjects stood in a comfortable position, shoulders and elbows flexed, with hands placed on supports without grasping them, with hips and knees fully extended. This standing position with the hands supported, while flexing the shoulders 30 degrees was found to be the best way to position the arms anterior to the spine with the least effect on overall sagittal balance in a healthy cohort [9].
All measurements were taken by a single observer using KEOPS software (SMAIO, France). This software was found to have better repeatability and reproducibility of computerized radiologic measurements when compared to manual standard radiologic measures [10]. It included the measure of sacropelvic parameters (PI, PT and SS), and local and global spinal parameters (LL, TK), as well as the inflexion point location and the apex of the curvatures; KEOPS software also performed subject distribution according to the Roussouly criteria. Then the upper lumbar lordosis angle (ULL) was calculated by subtracting SS from LL (Fig. 1). Since the LTK is always equal to ULL (alternate angles), the UTK is calculated by subtracting ULL from TK. Due to the variability of the inflexion points and apex positioning the number of vertebrae included in each part of curves was noted.
Data were analyzed using SPSS 20.0 software (SPSS Inc., Chicago, IL, USA). Quantitative variables were compared using the t test and paired t test. Pearson's correlation test (R) was used to evaluate different correlations. In accordance with Cohen, statistically significant correlation was considered large clinically if R > 0.5, moderate if 0.3 ≤ R ≤ 0.5 and small if R < 0.3 [11]. p = 0.05 was chosen as significance level.
Results
A total of 373 adult volunteers were enrolled in the study. Mean age was 27 years (range, 18–45 years), with 217 females and 156 males (F/M ratio of 1.4/1). Descriptive statistics of the spinal and pelvic parameters are shown in Table 1. The upper lordosis vertebra was L1 in 45% of the cases and was located between T12 and L2 in 88% of the cases. The upper thoracic vertebra was T2 in 56% of the cases and was located between T1 and T3 in 96% of the cases. There was no difference between the upper thoracic vertebras in different Roussouly subtypes. The apex of the thoracic kyphosis was mainly located at T9 for types 1 and 2 of Roussouly spinal morphotypes, whereas it is mainly located at T8 for type 3, anteverted type 3 and type 4 morphotypes (p = 0.012).
UTK and LTK
The mean ULL, and thus the LTK, was found to be 19.8°, while the mean UTK was found to be 25.8° with a 6° of significant statistical difference (p < 0.001). The main difference is that ULL is spanned over 2.9 vertebrae, whereas LTK is spanned over 4.9 vertebrae (p < 0.001). This difference is maintained when analyzing different Roussouly subtypes. The UTK is formed by a mean 6.5 vertebrae that is the same between the different Roussouly subtypes. Table 2 describes the LTK and the UTK in the different Roussouly spinal shapes. The UTK spans over 6.5 vertebras, and no difference was observed between UTK angle values in the five different spinal shapes (p > 0.05). However, statistically significant difference was found in mean LTK values between the different Roussouly subtypes of spine. To add to that, the ratio of the UTK to the total TK was found to be comparable between the different Roussouly spine subtypes and had an average of 55% (Table 2).
Correlations between TK and different spinal parameters
TK showed the highest correlation with the LL (moderate correlation) (Table 3). When studying correlation between the lumbar lordosis arches and the TK, the lower lumbar arch, which is equal to SS, showed a weak correlation, whereas the upper arch showed stronger correlation (Pearson's correlation of 0.66).
Measured TK versus TTK
Finally, a comparison was made between the measured TK with TTK that was calculated according to the formula proposed by Clément et al. [8]. Mean TTK was 39.6° (SD = 9.7°) and was found to be significantly different with the mean measured TK (45.6°; p < 0.001) with a mean difference of 6°.
Discussion
Since the description of the pelvic parameters by Duval-Beaupère [12], sagittal balance publications have increased exponentially over the last decade [13]. The majority of the scientific works dedicated to describe the sagittal spinal parameters in asymptomatic adults focus mainly on the description of LL, its apex and two arches [3, 14,15,16]. As for TK evaluation, and due to a poor visualization of the upper thoracic spine on X-rays, the TK analysis focused only on T5–T12 segment and on T1 tilt. Until recently, TK was described by Clément et al. as a harmonious curve with two equal arches [8].
It is necessary to describe here the spinal segmentation. The spinal segmentation proposed by Berthonnaud et al. was based on a geometrical model of each spinal curvature [3]. Each curve, either LL or TK, may be segmented into two tangent arches around the apex of each curve. The apex is defined as the point where the curve is tangent to vertical line. Based on this curve segmentation, a lower and an upper arch or each curve LL and TK is defined, each curve being separated by the inflexion point (IP) where LL transitions in TK. LLL is bounded by the sacral plateau distally and the horizontal line through the lumbar apex. The ULL is limited by the same horizontal line and the perpendicular line to the spine on the thoracolumbar IP distally. The center of each arc is positioned on the lumbar apex, but the radius of the two arches is unequal and depends on the number of vertebras in the curve. The same construct is applied on TK, limited proximally by the cervico-thoracic inflexion point and IP distally. Clément proposed recently a new segmentation based on the same limits (SP and IP for LL) [8]. They designed LL global angle as the intersection of SP line and IP line, and they divided this angle by a horizontal line passing through the summit of LL angle (Fig. 2). Even if the absolute value of the angles coming from this construction is equal to the construction with AL, the curve limitation on the second construction had no sense and did not obey to a geometrical curve model. The second construct introduced the idea that both LL and TK curves had the same radius and would be modelized as a single arch of circle that is absolutely not the case as shown by several authors [6, 17].
Based on this segmentation Clement has defined an equation: TK = 2*(PT + LL − PI) [8]. There was a mean difference between the actual TK and TTK of 6°. This difference may be due to difference in age of both population: Clement’s cohort was younger, aged between 13 and 20 years. This may explain a TK angle higher in this study with only young adults included.
Our study found that TK is formed, similar to LL, by two unequal arches that are separated by an apex around T8 and T9 with a variable lower arch and a constant upper arch 25.8°. Roussouly et al. described a lower arch equal to SS and an upper LL arch that they found to be constant around 20° [6]. This paper showed that the ULL is slightly variable among the different Roussouly subtypes when the major variability of LL was due to LLL changes. This reciprocal variation of the ULL and LTK may play a pivotal role in compensation in adult spinal deformity. First of all, ULL variation occurs in limited number of vertebras while the LTK is spanned around nearly the double number of vertebras. If either the ULL length is increased by an excessive surgical correction, the LTK is decreased, and the compensating LTK should have a greater increase in a limited number of vertebrae. This mechanism may also explain the proximal junctional kyphosis (PJK) that occurs with a higher LL apex as described by Sebaaly et al. [18] as well as the compensatory PJK as described by Lafage et al. [19]. Of course, this mechanism is increased if ULL is artificially increased in length and angle. This is the case when LL reconstruction plays on ULL instead of LLL. This could also explain also the upper thoracic PJK. When the TK is not respected by the surgical reduction flattening too much TK, this action displaces the TK apex too high and imposes a forward over bending of the free spine over the instrumentation to restitute the UTK.
The second interesting finding of this paper is that the UTK is a constant and constitutes around 55% of all TK. This nonvariability of the UTK could be explained by the spinal rigidity in the upper thoracic spine due to anatomical particularities of the rib cage and its relation to the spine. This very important finding could have pivotal implications in several pathologies involving the fusion of the upper thoracic spine. As a matter of fact, recent publications have evaluated the use of pre-contoured rods in the treatment of adolescent idiopathic scoliosis [20, 21]. The contouring of the rods should take into consideration this constancy in the UTK. Moreover, this could help to restitute normal alignment after treatment of lordotic type 2a scoliosis as described by Abelin-Genevois et al. [21].
Another finding is that the most variation of spinal segmentation occurs in its lowest part: the LLL which is equal to SS. UTK is quasi-constant (around 25°), and ULL and LTK are variable to a very small extent. As a matter of fact, the main change between the different subtypes is the number of vertebrae of every arch of TK and LL. The TK in type 1 is very long. And for the same value of angle, the number of vertebra is much less in type 4 spines (Fig. 3). Even for the same angle measure, the inflexion is greater with a lesser number of vertebras included, and that explains the curves inflexion variation in the various types.

A comparison between a type 1 morphotype and a type 4 morphotype. In type 1 (a), the apex of the TK is located in the T11–T12 disk. The value of the UTK is 28.2° and is formed by 10 vertebras. In type 4 (b), the apex of the TK is located in the T4 vertebral body. The value of the UTK is 27.5° and is formed by four vertebras
This study has certain limitations. The population mainly comprised young adults, and differences are likely to be found with adolescents or older patients. The population comprised only Caucasian subjects, and differences with Asian or African populations were not considered, as ethnic morphological differences may change the setting of balance parameters [22].
Conclusion
In asymptomatic young adults, thoracic kyphosis is made up by two unequal arches a globally stable UTK and a variable LTK, with an apex around T8 and T9 vertebra, depending on the spinal morphotype according to Roussouly classification. This concept has several implications on sagittal balance and spine compensatory mechanisms comprehension as more compensation occurs in variable parts of the spine. This new concept should be taken into consideration, while planning surgeries in adult spine deformity, aiming to reduce the incidence of mechanical complications, but also when using pre-contoured rods in scoliosis surgery in younger adults.
References
Berge C (1998) Heterochronic processes in human evolution: an ontogenetic analysis of the hominid pelvis. Am J Phys Anthropol 105:441–459. https://doi.org/10.1002/(SICI)1096-8644(199804)105:4%3c441::AID-AJPA4%3e3.0.CO;2-R
Vasiliadis ES, Grivas TB, Kaspiris A (2009) Historical overview of spinal deformities in ancient Greece. Scoliosis 4:6. https://doi.org/10.1186/1748-7161-4-6
Berthonnaud E, Labelle H, Roussouly P et al (2005) A variability study of computerized sagittal spinopelvic radiologic measurements of trunk balance. J Spinal Disord Tech 18:66–71
Berthonnaud E, Dimnet J, Roussouly P, Labelle H (2005) Analysis of the sagittal balance of the spine and pelvis using shape and orientation parameters. J Spinal Disord Tech 18:40–47. https://doi.org/10.1097/01.bsd.0000117542.88865.77
Bess S, Protopsaltis TS, Lafage V et al (2016) Clinical and radiographic evaluation of adult spinal deformity. Clin Spine Surg 29:6–16. https://doi.org/10.1097/BSD.0000000000000352
Roussouly P, Gollogly S, Berthonnaud E, Dimnet J (2005) Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine (Phila Pa 1976) 30:346–353. https://doi.org/10.1097/01.brs.0000152379.54463.65
Laouissat F, Sebaaly A, Gehrchen M, Roussouly P (2017) Classification of normal sagittal spine alignment: refounding the Roussouly classification. Eur Spine J. https://doi.org/10.1007/s00586-017-5111-x
Clément J-L, Solla F, Amorese V et al (2020) Lumbopelvic parameters can be used to predict thoracic kyphosis in adolescents. Eur Spine J. https://doi.org/10.1007/s00586-020-06373-z
Marks M, Stanford C, Newton P (2009) Which lateral radiographic positioning technique provides the most reliable and functional representation of a patient’s sagittal balance? Spine (Phila Pa 1976) 34:949–54. https://doi.org/10.1097/BRS.0b013e318199650a
Maillot C, Ferrero E, Fort D et al (2015) Reproducibility and repeatability of a new computerized software for sagittal spinopelvic and scoliosis curvature radiologic measurements: Keops? Eur Spine J 24:1574–1581. https://doi.org/10.1007/s00586-015-3817-1
Cohen J (1988) Statistical power analysis for the behavioural sciences, 2nd edn. Lawrence Erlbaum Associates, Hillsdale
Legaye J, Duval-Beaupère G, Hecquet J, Marty C (1998) Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J 7:99–103
Zhang Y, Wumaier M, He D et al (2020) The 100 top-cited articles on Spinal deformity: a bibliometric analysis. Spine (Phila Pa 1976) 45:275–283. https://doi.org/10.1097/BRS.0000000000003247
Pan C, Wang G, Sun J (2019) Correlation between the apex of lumbar lordosis and pelvic incidence in asymptomatic adult. Eur Spine J. https://doi.org/10.1007/s00586-019-06183-y
Roussouly P, Pinheiro-Franco JL (2011) Sagittal parameters of the spine: biomechanical approach. Eur Spine J 20(Suppl 5):578–585. https://doi.org/10.1007/s00586-011-1924-1
Vialle R, Levassor N, Rillardon L et al (2005) Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am 87:260–267. https://doi.org/10.2106/JBJS.D.02043
Boissière L, Takemoto M, Bourghli A et al (2016) Global tilt and lumbar lordosis index: two parameters correlating with health related quality of life scores; but how do they truly impact disability? Spine J. https://doi.org/10.1016/j.spinee.2016.10.013
Sebaaly A, Riouallon G, Obeid I et al (2018) Proximal junctional kyphosis in adult scoliosis: comparison of four radiological predictor models. Eur Spine J 27:613–621. https://doi.org/10.1007/s00586-017-5172-x
Lafage R, Line BG, Gupta S et al (2017) Orientation of the upper-most instrumented segment influences proximal junctional disease following adult spinal deformity surgery. Spine (Phila Pa 1976) 42:1570–1577
Ilharreborde B, Simon AL, Ferrero E, Mazda K (2019) How to optimize axial correction without altering thoracic sagittal alignment in hybrid constructs with sublaminar bands: description of the “Frame” technique. Spine Deform 7:245–253. https://doi.org/10.1016/j.jspd.2018.08.013
Abelin-Genevois K, Sassi D, Verdun S, Roussouly P (2018) Sagittal classification in adolescent idiopathic scoliosis: original description and therapeutic implications. Eur Spine J 27:2192–2202. https://doi.org/10.1007/s00586-018-5613-1
Weinberg DS, Morris WZ, Gebhart JJ, Liu RW (2016) Pelvic incidence: an anatomic investigation of 880 cadaveric specimens. Eur Spine J 25:3589–3595. https://doi.org/10.1007/s00586-015-4317-z
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None of the authors has any potential conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sebaaly, A., Silvestre, C., Rizkallah, M. et al. Revisiting thoracic kyphosis: a normative description of the thoracic sagittal curve in an asymptomatic population. Eur Spine J 30, 1184–1189 (2021). https://doi.org/10.1007/s00586-020-06670-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-020-06670-7