
Abstract
Introduction
Surgical treatment of AIS aims to correct the coronal and sagittal alignment of the spine. The global alignment of the spine may be normalized through reciprocal changes between the fused spine and adjacent segments. We propose a new classification system describing the specific sagittal patterns induced by AIS to define reproducible guidelines for the surgical strategy.
Methods
We analyzed 100 consecutive AIS patients aged between 12 and 18 years candidate for spinal fusion. The following parameters were measured and compared for each pattern: spino-pelvic parameters, magnitude and length of the lumbar sagittal angle, magnitude and length of the thoracic sagittal angles (T1T12 and T4T12 angles, TKmax), T10 L2 angle, C7 slope and C2C7 angle.
Results
Three parameters strongly differentiated the four patterns: thoracic sagittal angles (T1T12 and T4T12 angles, TKmax), T10 L2 angle and C7 slope. Less than half of the patients (44%) had a normal sagittal shape. Within, Type 2 characterized by thoracic hypokyphosis, Type 2a (thoracic hypokyphosis) were mostly Lenke type 1 or 2 curves, and type 2b (thoracic hypokyphosis with TL kyphosis) occurred specifically in double major or TL/L curves. Type 3 were two-curve sagittal shape with cervicothoracic kyphosis and TL lordosis (9%), mainly in Lenke 1 curves.
Discussion
This new classification summarizes all the pathological scenarios of the sagittal alignment of AIS into four patterns. A specific surgical planning can be extrapolated for each pattern. In type 1, the objective is to preserve the sagittal shape. In type 2, the objective is to restore thoracic kyphosis. In type 2b, TL junction should be straightened. In type 3, the objective is to reshape the lower arc of thoracic sagittal angle and straighten the TL junction.
Graphical abstract
These slides can be retrieved under Electronic Supplementary Material.

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Scoliosis is a three-dimensional deformity resulting from intervertebral movements leading to spinal torsion, mainly intervertebral extension and transverse rotation. These movements automatically produce lateral inclination, which we characterize conventionally on the frontal view by the Cobb angle [1]. Somerville used the term of “rotational lordosis”, as an holistic definition of the deformity, giving as much importance to the sagittal as the transverse plane [2]. Spinal extension, or lordosis of the spine, is described as the precursor movement.
In AIS, sagittal spine alignment may differ from the normal subject as a result of the structural deformity of the spine. Analysis of these modifications is important to define guidelines for the therapeutic strategy. It is at first sight complex due to the polymorphism of the curve types.
In 2003, Mac-Thiong et al. [3] described the sagittal spinal parameters in a population of AIS and showed that sagittal spinal alignment depends on the location of the apex of the scoliotic curve. Thoracic scoliosis may induce a decrease in thoracic kyphosis, whereas thoracolumbar and lumbar deformities maintain a kyphotic thoracic spine and tend to increase the upper lumbar lordosis [4].
However, the usual sagittal parameters derived from the description of the normal spine do not help to describe the real impact of scoliosis on global and regional organization of the spine in AIS. Indeed, the structural changes within the scoliotic deformity that are now well described induce junction orientation changes, due to intersegment reciprocity. In order to make the erect position sustainable and energetically economic, sagittal curvatures are organized by reciprocity. This organization follows strict physiological rules, to maintain alignment between the barycenter and joint centers of the lower extremities [5]. In the non-scoliotic population, Roussouly has described four types of back according to the sacral slope, directly correlated the pelvic incidence, and showed the repercussion of pathological conditions on sagittal mismatching and imbalance [6, 7].
The segmental analysis of the spinal deformity and the differentiation between structural sagittal changes linked to scoliosis and junction adaptation mechanisms can provide a synthetic understanding of the sagittal analysis of AIS. A classification integrating this global and specific description is still lacking in our practice. It is in this objective that we built this new classification system.
Even though the Lenke classification has emerged as the gold standard classification system in the description of AIS deformity and as a guidance for surgical planning, the sagittal modifiers proposed by Lenke had little echo and did not give rise to the same accuracy in terms of recommendation guidelines as the frontal types and modifiers. Figure 1 shows two similar curves according to Lenke classification which are dramatically different in terms of sagittal organization.

Similar curves types according to Lenke classification can have dramatically different sagittal patterns. These two cases share the same Lenke type with similar lubar and sagittal modifiers, type 1C(N)
The new AIS specific sagittal classification system that we propose in the present paper is born after the preliminary study of Yu and Roussouly on the cervical spine behavior in idiopathic scoliosis. As shown by many authors, there is a high incidence of cervical kyphosis in thoracic AIS [8,9,10]. Yu et al. [11] proposed two mechanisms which may produce cervical kyphosis in AIS, as a junctional response to the structural sagittal changes: either a response to the horizontalization of the T1 plateau due to thoracic hypokyphosis, or the inclusion of the cervical spine in the kyphotic segment above the lumbar lordosis, due to the upward displacement of the inflection point between lumbar lordosis and thoracic kyphosis.
From this first analysis, considering the structural parameters that must be corrected in AIS sagittal deformity, we propose a new specific sagittal classification, integrating the structural sagittal modifications induced by the tridimensional deformity and the junctional compensations implemented to maintain a global economic sagittal alignment of the spine. The aim of our work is to describe this classification and to present the therapeutic recommendations that arise from it.
Materials and methods
From a monocentric prospective surgical database, we extracted hundred consecutive AIS patients aged between 12 and 18 years, candidate to posterior spinal fusion (primary inclusion from 2011 to 2013).
For each case, we analyzed full standing AP and lateral digital radiographs of the spine, and reducibility test radiographs routinely taken in the preoperative evaluation. All radiographs were performed using a standardized protocol, and patients were asked to stand in a relaxed position and to look straight forward.
All measurements were taken on Keops Analyzer® (SMAIO®, France) by the same operator, an experienced spine deformity surgeon. Based on AP and reducibility test radiographs, patients were classified according to the Lenke classification. Each curve was characterized by location, apex and main curve Cobb angle.
Figure 2 summarizes the radiographic spinal sagittal parameters that were measured on Keops Analyzer® (SMAIO, France):

New sagittal classification for AIS
-
Inferior cervical spine angle (C2C7) formed by the tangent to the inferior endplates of C2 and C7
-
Global cervical spine angle (C1 C7)
-
C2C6 angle (Hilibrand cervical angle)
-
C7 slope: formed by the tangent to the inferior endplate of C7 and the horizontal reference line.
-
Magnitude of thoracic kyphosis (TK): (T1 T12), (T4T12) and maximum sagittal kyphotic angle (SKA)
-
Length of SKA: number of kyphotic vertebrae
-
Magnitude of lumbar lordosis: (L1 S1), maximum sagittal lordotic angle (SLA)
-
Length of SLA: number of lordotic vertebrae
-
Thoracolumbar junction angle (T10 L2).
The following spino-pelvic parameters were analyzed:
-
PI (pelvic incidence) angle between the perpendicular of the sacral plate and the line joining the middle of the sacral plate and the hip axis,
-
SS (sacral slope) angle between the sacral plate and the horizontal line
-
PT (pelvic tilt) angle between the vertical line and the line joining the middle of the sacral plate and the hip axis, which is positive when the hip axis lies in front of the middle of the sacral plate.
Statistical analysis
The mean and the SD of the quantitative variables and the number and the frequencies of the modalities of the qualitative variables have been computed.
We separated the cohort into four groups according to the type of sagittal pattern in the new classification system (Fig. 2).
To assess the differences between the groups, p values have been computed using Fisher exact tests for qualitative variables and ANOVA or Kruskal–Wallis tests for quantitative variables. ANOVA is used if no deviation from normality is detected by a Shapiro–Wilk test.
A correlation analysis was done by computing the Spearman (nonparametric) correlation and testing it for the hypothesis that it is null. The correlation between several couples of parameters has been computed.
The significance level is set at 5% in all the analysis. No multiplicity correction has been performed. The analysis was done using R 3.2.5.
Results
AIS sagittal types distribution
Forty-four percent of the patients were categorized as type 1—normal sagittal shape. Type 2, characterized by thoracic hypokyphosis with cervical kyphosis, represented the main sagittal type (47%). As all patients with T10 L2 angle > 10° had a type 2 pattern, we could differentiate two subgroups within type 2. Type 2a was characterized by hypokyphotic thoracic spine with cervical kyphosis (preserving three alternating sagittal curves); type 2b was characterized by thoracic hypokyphosis and thoracolumbar kyphosis, sagittal shape including four alternate sagittal curves (Fig. 2).
The less frequent type 9(%), sagittal type 3, was characterized by only two alternating sagittal curves: a proximal cervicothoracic kyphosis and a long thoracolumbar lordosis.
Lenke-type distribution
Patients’ subgroups according to the different sagittal patterns were comparable in age and main curve amplitude (Table 1) but showed different distributions of Lenke types (Table 2). AIS with sagittal type 1 (normal) or 2a (thoracic hypokyphosis) were mainly thoracic curves. AIS with sagittal type 2b (thoracic hypokyphosis + TLK) were mostly TL or L curves, thoracic curves with more distal thoracic apex location (< T9). AIS with sagittal type 3 were mainly Lenke curve types 3, 4, 5 or 6, meaning double curves or TL/L, in which an apical structural deformity was expressed within the area of the TL junction. Sagittal type 3 could be characterized in all Lenke types but the main denominator was the fact that the apex of one of the structural curves was included in the thoracolumbar junction (TLJ), meaning that intervertebral extension movement created an extension of this area, pushing the inflexion point upward.
Roussouly type distribution
There was no statistical difference in terms of distribution of sagittal types according to Roussouly classification (Table 3).
Radiographic parameters analysis
As shown in Table 4, the four AIS sagittal types were highly discriminated by the following spinal segmental parameters: cervical sagittal angle, C7 slope, thoracic sagittal angles (TK), T10L2 angle, sagittal lumbar angle (LL) and the number of vertebrae included in the lordosis.
Significant differences exist in terms of sagittal curvature lengths.
Type 1, representing the normokyphotic pattern, had a harmonious repartition of three sagittal curves with 11 ± 2.2 vertebrae participating in thoracic kyphosis and 5.1 ± 0.87 vertebrae in the lumbar lordosis. Mean thoracic kyphosis was T1T12: 34° ± 12°; T4T12: 30° ± 13°. C7 slope was positive, allowing the expression of a cervical straight or lordotic spine. The thoracolumbar area (T10L2) was straight.
Type 2 is defined by thoracic hypokyphosis [T1T12: 18° ± 9.8° (type 2a), 11° ± 13° (type 2b)] and decreased C7 slope, which induces cervical kyphosis (C2C7: type 2a: 17° ± 12°; type 2b: 18° ± 9.8°). Two subtypes could be differentiated according to the TL junction. In type 2b, T10L2 is kyphotic (12° ± 5.2° vs 0.49° ± 9.3°, p inferior to 0.001). In this subgroup, patients have four alternating sagittal curves (cervical kyphosis, thoracic hypokyphosis, TLK and short lumbar lordosis).
Sagittal type 3 is defined by two alternating curves. The length of lumbar sagittal curve is significantly modified (8.1 ± 0.93 LLmax vertebrae vs total: 5.3 ± 1.3; p < 0.0001), due to TL junction hyperextension (T10 L2: − 13° ± 5.6°). The inflection point between LL and TK is proximally shifted, shortening the area of expression of thoracic kyphosis in the thoracic area and resulting in a global cervicothoracic kyphosis. The cervical spine is therefore kyphotic (C2C7: 26° ± 15°, p < 0.0001), with reduced C7 slope (8.6 vs − 17, p > 0.0001).
Correlation analysis between regional parameters and spino-pelvic parameters
We did not find any difference in terms of spino-pelvic parameters between the different sagittal patterns (Table 5). Strong correlation remained between spino-pelvic parameters. Thoracic kyphosis was correlated with LL, C7 slope and cervical lordosis. Cervical lordosis was moderately correlated to C7 slope. C7 plumb line was only correlated with C7 slope. T10L2 angle was moderately correlated to SSA and sacral slope.
Discussion
We could resume the sagittal alignment of AIS into four sagittal patterns. The determining criteria of each pattern were highly discriminative, the most discriminant parameters being the length of the LSA, T10L2, TK, C7 slope and the cervical sagittal angle.
Sagittal alignment is close to normal in 44% of the cohort. Preservation of a normal shape was defined by both qualitative criteria, meaning a harmonious sequence of three sagittal curves (cervical lordosis, thoracic kyphosis, lumbar lordosis), and quantitative criteria. As patients were analyzed using Keops software (SMAIO, Lyon, France), which is an update version of the previously validated Optispine software, we could verify individually that patients categorized as sagittal type 1 had sagittal parameters within the range of normal values, with respect to the spino-pelvic shape. Thoracic kyphosis is within the normal range (TKmax: 39° ± 13° (min 19°, max 57°) correlated with a positive C7 slope, which protects from cervical kyphosis. Distribution of Lenke types is comparable to the reference series of Lenke et al. [12], which may indicate that this pattern is not related to a certain type of scoliosis.
In contrast, more than half of AIS have a pathological profile requiring accurate characterization of sagittal modifications. Two pathological profiles can be defined, according to the existence of thoracic hypokyphosis either with or without thoraco lumbar kyphosis or TLJ hyperextension. In these pathological cases, Lenke type is determinant. Sagittal malalignment can be related to the structural deformity. Junctional modifications may be the compensatory consequences on the above and underlying segments.
Lenke classification has been widely used to guide decision-making in AIS surgery [12]. Controversy remains in some situations to decide whether or not to propose selective thoracic fusion. Moreover, there are still no specific guidelines regarding the contouring of the rod. In his classification, Lenke was the first to propose a characterization of the sagittal anomalies usually described in AIS within his global AIS classification system. However, it did not achieve a comprehensive system for the sagittal analysis. Guidelines were suggested mainly according to the coronal aspect of the deformity. The sole sagittal parameter which could indicate a more extensive fusion was TLK > 20° and PT kyphosis > 20°. Celestre et al. discussed the importance to consider the sagittal profile, especially the behavior of the TLJ but could not give clear conclusions regarding the optimal sagittal spinal alignment to achieve postoperatively [13]. More recently, Sebaaly et al. demonstrated that proximal junctional kyphosis was clearly related to the positioning of the point of inflection, in ASD surgery.
No significant difference was found in terms of spino-pelvic parameters showing that this classification specifically describes the pathological component of the sagittal alignment of AIS and the reciprocal junctional changes. Spino-pelvic parameters were comparable between the four types, as for Roussouly classification. As demonstrated previously by Roussouly and later Hu et al. [14, 15], the most expressed types of back in idiopathic scoliosis are Roussouly types 3 and 4 [12]. The Caucasian series reported an average pelvic incidence greater than normal (> 55°) but did not find any differences in terms of spino-pelvic alignment [3, 4, 16]. In the Chinese population, Yong et al. [17] showed that PI is comparable to the normal population (PI = 45°). Structural sagittal changes do not alter the correlations between the pelvic parameters and the lumbar spine. At most, we observe higher pelvic tilt depending on the Lenke type of scoliosis [18].
Although there is a different distribution of sagittal types within scoliosis types according to the Lenke classification, there is no direct correlation between Lenke types and sagittal shape produced by the deformity. Hu et al. [15] already characterized the sagittal alignment of each Lenke type and showed that coronal deformity had limited influence on sagittal parameters, as most of coronal and sagittal parameters were not significantly correlated. It thus appears that the sagittal alignment is specific to the structural movements induced by scoliosis in the profile, which justifies, in our opinion, a separate but complementary analysis of the frontal analysis.
AIS is a posterior imbalance of the spine [19]. Sagittal mal alignment is mainly a consequence of segmental hyperextension. Two sagittal parameters can be modified by the structural part of the deformity, according to the type of AIS: the thoracic kyphosis and the upper arch of the lumbar lordosis. Clément et al. confirm the role of reciprocity on the upper arch of the lumbar lordosis, showing that sagittal modifications can result either from the structural deformity or as a compensatory mechanism to thoracic hypokyphosis [4]. Junctional areas (cervicothoracic and thoracolumbar segments) may adapt to non physiological sagittal curves to maintain a global alignment and horizontal gaze.
The cervical spine has long been the great forgotten in the overall sagittal analysis of the spine. Recent studies restore the importance of this segment in both sagittal understanding and surgical decision-making for optimal sagittal correction [9, 15, 20,21,22]. In healthy subjects, especially in children and adolescents, we showed strong correlations between the behavior of the cervical spine and the orientation of the upper segment of the thoracic spine materialized by C7 or T1 slope [23].
Of course, there are limitations to our work with respect to the initial description of a classification. Scoliosis is a complex and three-dimensional deformity. Stagnara emphasized the importance of the election plan as a more accurate and faithful picture of the true deformation. More recently, Newton et al. have confirmed that three-dimensional analysis is critical for adequate description of the sagittal deformity induced by AIS. Low dose 3D radiological analysis is now allowed by new technologies such as stereoradiography, which will necessarily require the validation of this classification by 3D analysis. Actually, we have already conducted this study, showing excellent concordance between 2D and 3D analysis, but the data remain to be published. Final and essential stage is to validate the proposed guidelines for sagittal correction, mainly by reducing complications related to a non harmonization of the profile in arthrodesis.
Conclusion
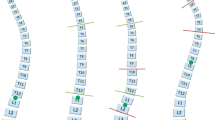
The objective of this classification is not only descriptive but is intended to be therapeutic. Characterization of pathological type allows to target the ideal location of the sagittal surgical correction and, in our hands, could guide bending of rods with respect to the specific spino-pelvic alignment of the patient and ideal placement and choice of implants to succeed in a faithful correction (Fig. 3).


Therapeutic recommendations for sagittal correction in AIS according to the sagittal pattern. a Type 1 preserve the sagittal shape in the rod contouring keep TL junction straight. b Type 2 restore thoracic kyphosis by pulling the thoracic apex backward straighten TL junction between T10 and L2 in case of type 2b. c Type 3 lengthen caudally thoracic kyphosis to restore the proper length of TK and reposition the inflection point between T12 and L1 by straightening the TL junction
As a conclusion, and from our experience with the use of this classification, we propose the following recommendations in terms of sagittal correction.
Type 1 has a harmonious sagittal alignment which should be preserved. The rod contouring should respect the length and magnitude of thoracic kyphosis and keep TL junction straight (Fig. 3a).
In type 2, the surgical strategy is to restore thoracic kyphosis which may require Ponte osteotomies around the apex in order to pull the thoracic apex backward. TL junction should be straightened in type 2b (Fig. 3b).
In type 3, the goal is to lengthen caudally the thoracic kyphosis, which may require Ponte osteotomies in the inferior part of the thoracic area. The inflection point should be repositioned at the TL junction (Fig. 3c).
References
Roaf R (1966) The basic anatomy of scoliosis. J Bone Jt Surg Br 48:786–792
Somerville EW (1952) Rotational lordosis; the development of single curve. J Bone Jt Surg Br 34-B:421–427
Mac-Thiong J-M, Labelle H, Charlebois M, Huot M-P, de Guise JA (2003) Sagittal plane analysis of the spine and pelvis in adolescent idiopathic scoliosis according to the coronal curve type. Spine 28:1404–1409
Clément J-L, Geoffray A, Yagoubi F, Chau E, Solla F, Oborocianu I, Rampal V (2013) Relationship between thoracic hypokyphosis, lumbar lordosis and sagittal pelvic parameters in adolescent idiopathic scoliosis. Eur Spine J 22:2414–2420
Duval-Beaupère G, Schmidt C, Cosson P (1992) A Barycentremetric study of the sagittal shape of spine and pelvis: the conditions required for an economic standing position. Ann Biomed Eng 20:451–462
Vaz G, Roussouly P, Berthonnaud E, Dimnet J (2002) Sagittal morphology and equilibrium of pelvis and spine. Eur Spine J 11:80–87
Roussouly P, Pinheiro-Franco JL (2011) Biomechanical analysis of the spino-pelvic organization and adaptation in pathology. Eur Spine J Suppl 5:609–618
Hilibrand AS, Tannenbaum DA, Graziano GP, Loder RT, Hensinger RN (1995) The sagittal alignment of the cervical spine in adolescent idiopathic scoliosis. J Pediatr Orthop 15:627–632
Canavese F, Turcot K, De Rosa V, de Coulon G, Kaelin A (2011) Cervical spine sagittal alignment variations following posterior spinal fusion and instrumentation for adolescent idiopathic scoliosis. Eur Spine J 20:1141–1148
Ilharreborde B, Vidal C, Skalli W, Mazda K (2013) Sagittal alignment of the cervical spine in adolescent idiopathic scoliosis treated by posteromedial translation. Eur Spine J 22:330–337
Yu M, Silvestre C, Mouton T, Rachkidi R, Zeng L, Roussouly P (2013) Analysis of the cervical spine sagittal alignment in young idiopathic scoliosis: a morphological classification of 120 cases. Eur Spine J 22:2372–2381
Lenke LG, Betz RR, Harms J, Bridwell KH, Clements DH, Lowe TG, Blanke K (2001) Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Jt Surg Am 83-A:1169–1181
Celestre PC, Carreon LY, Lenke LG, Sucato DJ, Glassman SD (2015) Sagittal alignment two years after selective and nonselective thoracic fusion for Lenke 1C adolescent idiopathic scoliosis. Spine Deform 3:560–565
Roussouly P, Labelle H, Rouissi J, Bodin A (2013) Pre- and post-operative sagittal balance in idiopathic scoliosis: a comparison over the ages of two cohorts of 132 adolescents and 52 adults. Eur Spine J 22(Suppl 2):S203–S215
Hu P, Yu M, Liu X, Zhu B, Liu X, Liu Z (2016) Analysis of the relationship between coronal and sagittal deformities in adolescent idiopathic scoliosis. Eur Spine J 25:409–416
Upasani VV, Tis J, Bastrom T, Pawelek J, Marks M, Lonner B, Crawford A, Newton PO (2007) Analysis of sagittal alignment in thoracic and thoracolumbar curves in adolescent idiopathic scoliosis: how do these two curve types differ? Spine 32:1355–1359
Yong Q, Zhen L, Zezhang Z et al (2012) Comparison of sagittal spinopelvic alignment in Chinese adolescents with and without idiopathic thoracic scoliosis. Spine 37:E714–E720
Abelin-Genevois K, Estivalezes E, Briot J, Sévely A, Sales de Gauzy J, Swider P (2015) Spino-pelvic alignment influences disc hydration properties after AIS surgery: a prospective MRI-based study. Eur Spine J 24:1183–1190
Newton PO, Fujimori T, Doan J, Reighard FG, Bastrom TP, Misaghi A (2015) Defining the “three-dimensional sagittal plane” in thoracic adolescent idiopathic scoliosis. J Bone Jt Surg Am 97:1694–1701
Norheim EP, Carreon LY, Sucato DJ, Lenke LG, Glassman SD (2015) Cervical spine compensation in adolescent idiopathic scoliosis. Spine Deform 3:327–331
Youn MS, Shin JK, Goh TS, Kang SS, Jeon WK, Lee JS (2016) Relationship between cervical sagittal alignment and health-related quality of life in adolescent idiopathic scoliosis. Eur Spine J. https://doi.org/10.1007/s00586-016-4488-2
Charles YP, Sfeir G, Matter-Parrat V, Sauleau EA, Steib J-P (2015) Cervical sagittal alignment in idiopathic scoliosis treated by posterior instrumentation and in situ bending. Spine 40:E419–E427
Abelin-Genevois K, Idjerouidene A, Roussouly P, Vital JM, Garin C (2014) Cervical spine alignment in the pediatric population: a radiographic normative study of 150 asymptomatic patients. Eur Spine J 23:1442–1448
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
K. Abelin-Genevois, S. Verdun and D. Sassi have no conflict of interest to disclose. P. Roussouly is shareholder of SMAIO, France. He is also a consultant for Kisco Systems and receives royalties from Medtronic, but these disclosures are not related to the present work.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Abelin-Genevois, K., Sassi, D., Verdun, S. et al. Sagittal classification in adolescent idiopathic scoliosis: original description and therapeutic implications. Eur Spine J 27, 2192–2202 (2018). https://doi.org/10.1007/s00586-018-5613-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-018-5613-1