
Abstract
Neonatal hypertension is increasingly recognized as dramatic improvements in neonatal intensive care, advancements in our understanding of neonatal physiology, and implementation of new therapies have led to improved survival of premature infants. A variety of factors appear to be important in determining blood pressure in neonates, including gestational age, birth weight, and postmenstrual age. Normative data on neonatal blood pressure values remain limited. The cause of hypertension in an affected neonate is often identified with careful diagnostic evaluation, with the most common causes being umbilical catheter-associated thrombosis, renal parenchymal disease, and chronic lung disease. Clinical expertise may need to be relied upon to decide the best approach to treatment in such patients, as data on the use of antihypertensive medications in this age group are extremely limited. Available data suggest that long-term outcomes are usually good, with resolution of hypertension in most infants. In this review, we will take a case-based approach to illustrate these concepts and to point out important evidence gaps that need to be addressed so that management of neonatal hypertension may be improved.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Neonatal hypertension (HTN) was first described in the late 1970s [1, 2], and since that time, awareness has increased dramatically. Despite the increased knowledge, diagnosis and treatment of neonatal HTN remain challenging for many clinicians. Reasons for this include the paucity of normative data on neonatal blood pressure values, exclusion of neonates from clinical trials of antihypertensive medications [3], and the relative rarity of the condition. Even so, it is important to understand basic principles surrounding identification, evaluation, and management of the hypertensive neonate. This review will use a case-based approach to illustrate key aspects of this clinical problem, hopefully in a manner that will be useful to the reader. Those interested in HTN beyond the neonatal period should consult other references [4, 5].
Case 1
A 6-week-old former 28-week gestation infant is being cared for in the neonatal intensive care unit (NICU) where he is completing treatment for pneumonia and working to gain sufficient weight to be discharged home. In reviewing the infant’s chart, you notice blood pressure (BP) readings of 98/68, 105/70, and 96/64 over the past 24 h. What is your assessment of the infant’s BP?
Defining hypertension
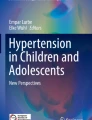
Defining HTN during the newborn period is challenging, as there are subtle complexities to changes in BP patterns in newborns. Similar to the changes seen in older children, where BP increases with age and body size [5], studies of term and preterm infants have shown that BP increases with gestational age and post-menstrual age, along with birth weight [6,7,8]. A large single-center study by Zubrow et al. provides useful data which defines the mean plus upper and lower 95% confidence intervals for the infants studied, and clearly demonstrate that BP increases with gestational age and birth weight [9]. A more recent study by Pejovic et al. assessed BP in hemodynamically stable term and preterm infants, finding that BP on day of age 1 correlated with gestational age and birth weight (Fig. 1) [10]. BP in preterm infants increases more rapidly over the first week or two than in term infants, and as premature infants mature, the strongest predictor of BP appears to be post-menstrual (sometimes termed post-conceptual) age [9, 10].

Linear regression of systolic (a), diastolic (b), and mean blood pressure (c) according to birth weight (1) and gestational age (2) on day 1 of life, with 95% confidence limits (upper and lower solid lines). Reprinted with permission from Pejovic et al [10]
Infant characteristics such as appropriateness of size for gestational age, gestational age at birth, and post-menstrual age appear to strongly influence BP [11]. Small for gestational age infants may be at increased risk of higher BP later in life, which may be in part due to decreased nephron development as well as other factors [11]. Additionally, multiple other factors impact BP in infants. Genetic factors may play a role, with one study identifying specific cytochrome P450 (CYP2D6) genotypes as being closely associated with higher BPs in preterm infants [12]. Maternal factors, such as underlying health, medications, and adequacy of nutrition prior to and during pregnancy can influence neonatal BP [13]. There is some suggestion in the literature that chorioamnionitis and HELLP (hemolysis, elevated liver enzymes, low platelets) syndrome may cause alterations in neonatal BP. Additionally, studies have found that higher infant BP is correlated with maternal body mass index > 30 kg/m2 and lower socioeconomic status [14].
In older children, HTN is defined as systolic and/or diastolic BPs persistently equal to or greater than the 95th percentile for age, gender, and height [5]. There is considerable variation in neonatal BP, both within the same infant over time and between infants based on a variety of aforementioned factors. These issues highlight the need for better normative BP data on infants, as there are no generally agreed-upon reference values available, leading to debate regarding how to define HTN. While no large studies exist, Dionne et al. utilized existing published data to derive systolic and diastolic BP percentiles based on post-menstrual age (Table 1) [15]. These values can be used clinically, and we suggest that BP values persistently above the 95th percentile should be closely monitored and BP values over the 99th percentile should be investigated and possibly treated depending on the clinical situation. In the above case, all three BP readings are in excess of the 99th percentile for an infant of 32 weeks post-menstrual age; therefore, as long as all blood pressure measurements were performed accurately, the diagnosis of HTN can be made and further workup initiated.
Case 2
You are participating in a multidisciplinary discharge conference at which infants nearing NICU discharge are reviewed. One infant being presented today carries a diagnosis of HTN and has two antihypertensive medications listed on her medication profile. She had had meconium aspiration and required a week of support with extracorporeal membrane oxygenation (ECMO) complicated by acute kidney injury (AKI), but never required dialysis and is now stable from a respiratory standpoint. The nursing discharge coordinator comments that he has not seen this situation for several years, and asks you to comment on the frequency of neonatal HTN, and the factors that might have led to this infant’s HTN.
Incidence of neonatal hypertension
The incidence of HTN varies dramatically depending on infant factors as well as their neonatal course. In available published case series, the incidence of neonatal HTN ranges from 0.2 to 3% [1, 2, 15]. In a study of 2500 Australian infants admitted to a NICU over 4 years, there was a 1.3% incidence of HTN [16]. In infants diagnosed with HTN in this study, common coexisting conditions included antenatal steroid exposure, maternal HTN, umbilical artery catheter placement, acute kidney injury, and chronic lung disease. A single-center case series more recently described an identical prevalence of HTN among over 4000 infants evaluated [17]. This group found that perinatal risk factors including maternal HTN, antenatal steroid administration, and maternal substance use were associated with HTN.
Only one large, multicenter study of neonatal HTN has been reported in the literature. Using administrative data from a consortium of pediatric hospitals, an incidence of 1% in infants admitted to a NICU was reported [18]. In this study, HTN was associated with higher severity of illness, extracorporeal membrane oxygenation (ECMO) therapy, and either congenital or acquired renal disease. With these data in mind, you would state that the infant described in case 2 certainly represents an unusual situation, but that she had several factors during her NICU course that likely explain her persistent HTN.
While often diagnosed during an infant’s initial NICU admission, HTN can also be diagnosed long after hospital discharge. In a retrospective study of 650 infants seen in a follow-up clinic after discharge from a tertiary level NICU, Friedman and Hustead described an incidence of HTN (defined as a systolic BP higher than 113 mmHg on three consecutive visits over 6 weeks) of 2.6% [19]. Neonates diagnosed with HTN following discharge were detected at a mean age of approximately 2 months corrected gestational age (approximately 48 weeks post-menstrual age) and were more likely to have more complex and longer NICU courses with lower initial APGAR scores and longer NICU stays. A more recent study by Shah et al. in a single-center outpatient HTN clinic reported similar findings, with 13 of 36 hypertensive infants diagnosed following discharge from the NICU [20]. These findings support the current clinical practice guidelines for routine BP monitoring in all children following discharge from the NICU [5].
Case 3
A 36-week gestation infant is admitted to the NICU because of mild respiratory distress. Serial antenatal ultrasounds had demonstrated a large “cystic” structure in the left renal fossa, but no other abnormalities. The infant’s BP has been ranging from 95/60 to 118/78, even when sleeping. You obtain a follow-up renal ultrasound that demonstrates severe hydronephrosis on the left with dilated calyces, dilated pelvis, and no distal ureteral dilatation. The right kidney and bladder are normal. What is the most likely cause of the infant’s elevated BP?
Etiology of hypertension in neonates
As in older infants and children, there are many potential etiologies of HTN in neonates (Table 2), with the largest percentage of cases caused by catheter-associated thromboembolism, renal parenchymal disease, and chronic lung disease. However, often no underlying cause is identified—this was illustrated in a recent multicenter case series that reported an inability to determine the etiology in approximately 50% of hypertensive infants [21].
The most common renovascular abnormality associated with HTN in neonates is thrombus formation associated with umbilical artery catheter (UAC) placement. This association was first described in the 1970s by Neal and colleagues [22] and has since been confirmed epidemiologically and experimentally by other investigators. HTN appears to develop in infants with UACs even when actual thrombi were not found in renal arteries. Therefore, it is thought that catheter-related HTN is related to thrombus formation related to vascular endothelium disruption at the time of line placement, to which preterm infants may be particularly susceptible. Epidemiologic studies have typically reported rates of thrombus formation around 25% [23]. Longer duration of catheter placement has been associated with higher risk of thrombus formation [24]; however, the location of line placement does not appear to matter, with a Cochrane review finding that HTN occurred at equal frequency with either “high” or “low” UAC positioning [25].
Other renovascular abnormalities may also lead to HTN in the neonatal time period. Renal vein thrombosis classically presents with a triad of flank mass, hematuria, and HTN [26]. The HTN may be quite severe in these cases and frequently persists beyond the neonatal period [27]. Fibromuscular dysplasia (FMD) and resultant renal arterial stenosis is an important cause of renovascular HTN in the neonate, as many infants with FMD will have normal-appearing main renal arteries but significant branch vessel disease that can cause severe HTN [28]. In addition, in FMD, renal arterial stenosis may also be accompanied by other vascular abnormalities [28, 29]. Miscellaneous vascular problems that may also cause neonatal HTN include arterial calcification (either idiopathic or caused by systemic illness) and compression of the renal arteries by tumors.
The second most common cause of neonatal HTN is congenital renal abnormalities. Both autosomal dominant and autosomal recessive polycystic kidney disease (PKD) may present with HTN, autosomal recessive PKD more commonly leads to HTN early in life, sometimes in the first months of life [30]. HTN may be seen in infants with renal dysplasia and hydronephrosis as well; this is the most likely cause of HTN in the infant described in case 3. Less frequently, HTN has also been reported in infants with unilateral multicystic dysplastic kidneys (MCDK), possibly due to excess renin production [31]. Obstructive uropathy, such as ureteropelvic junction obstruction, may be accompanied by HTN, which often normalizes after surgical correction but persistent HTN has occasionally been reported [32]. Additionally, acquired causes of renal parenchymal diseases (such as cortical necrosis or acute tubular necrosis) may be accompanied by HTN, usually due to hyperreninemia or volume overload [33].
Bronchopulmonary dysplasia (BPD)-associated HTN was first described in the mid-1980s by Abman and colleagues [34], who reported that the incidence of HTN in infants with BPD was 43%, versus an incidence of 4.5% in infants without BPD. Over half of the hypertensive infants with BPD were not diagnosed until after NICU discharge, highlighting the importance of monitoring BP following NICU discharge [5]. Multiple studies have confirmed that HTN occurs more frequently in infants with BPD compared to comparable infants without BPD, and appears to be more common with increasing severity of pulmonary disease [21, 35]. Factors such as hypoxemia and increased severity of BPD appear to be correlated with the development of HTN. A recent study by Seghal et al. found alterations in aortic wall thickness and vasomotor functioning in infants with BPD, suggesting another potential mechanism for the higher incidence of HTN in this population [36]. The high incidence of HTN in infants with lung disease reinforces that infants with severe BPD are clearly at increased risk of HTN and need close monitoring of BPs, both during their NICU stay and after hospital discharge.
HTN may also be seen in disorders of several other organ systems, either as the presenting symptom or accompanying other signs and symptoms. Coarctation of the aorta may be detected in the neonate, and has been frequently implicated as a cause of HTN [37]. The HTN seen in these neonates may persist even beyond successful surgical repair, and appears to be more severe in those with later surgical correction [38]. Disorders of the endocrine system, particularly congenital adrenal hyperplasia, hyperthyroidism, and hyperaldosteronism may also present with HTN in the neonatal period [15]. Neurologic abnormalities, including seizures, intracranial HTN, and pain, also may commonly cause episodic neonatal HTN [39]. Neonatal pain, which includes procedural and/or postoperative pain, should be carefully evaluated and treated with adequate analgesia whenever present.
Non-renal intra-abdominal processes constitute another important group of etiologies of HTN in neonates. Tumors, including neuroblastoma and Wilms’ tumor as well as many others, can cause HTN either due to production of vasoactive substances such as catecholamines or due to direct compression on renal vessels and/or ureters [37]. Maternal placental chorioangioma has also been reported in case reports to be associated with severe transient neonatal HTN [40]. Infants undergoing abdominal wall closure (e.g., gastroschisis or other abdominal wall surgical procedures) commonly have HTN, with one third to one half of neonates demonstrating HTN following the procedure. This is thought to be due to increased intra-abdominal pressure and resultant changes in renal blood flow as well as increased catecholamine secretion. A recent single-institution case series of infants with giant omphaloceles undergoing repair found that almost 80% of patients had HTN, but that most resolved prior to discharge [41].
In infants receiving care in the NICU, medication-induced HTN is an important group of causes. Medications which may be given to treat lung disease, such as dexamethasone or theophylline, have been shown to increase BPs, as have other adrenergic agents, ophthalmic phenylephrine drops, and prolonged use of pancuronium [42]. Medication-induced HTN is often dose-dependent and resolves with dose-reduction or withdrawal of the offending agent [43]. Substance use during pregnancy also may result in neonatal HTN, with maternal cocaine and heroin use during pregnancy have been reported to cause HTN. Additionally, in infants of drug-addicted mothers, withdrawal from sedative or analgesics may be associated with HTN as well [44]. HTN may be seen in neonates receiving parenteral nutrition, due to salt and water overload, or from hypercalcemia either due to excessive calcium intake or from vitamin A or D intoxication. Medication may also result in HTN by causing acute kidney injury. Due to challenges detecting AKI in neonates, HTN may be the first indication of renal injury and may lead to retrospective identification of AKI in this patient population.
There are multiple other causes of neonatal HTN that will not be covered in this review for space reasons but are listed in Table 2. An increasingly described association is HTN associated with ECMO (see case 2 above), which has been reported to occur in up to half of neonates requiring ECMO therapy [45]. The pathogenesis of ECMO-associated HTN appears to be multifactorial and may be due to fluid overload and impaired water and renal sodium handling and does not appear to be related to alterations in renin activity [46].
Case 4
A term neonate is transported to your hospital’s NICU from an outside facility for evaluation and management of severe congestive heart failure. After initial stabilization, the infant’s BPs are noted to be as high as 125/85, with none below 100/68. You get an urgent page from the attending cardiologist, who “thought there was something abnormal with the kidneys” when she was performing a bedside echocardiogram. What studies should be done to further evaluate the infant’s HTN?
Clinical presentation and diagnostic evaluation
Most hypertensive newborns are asymptomatic and will be discovered on routine monitoring of vital signs, which can make it challenging to identify infants with true HTN meriting further evaluation and treatment. Given their nonverbal status, neonates may not manifest symptoms even with severe HTN, and in cases where signs or symptoms are present, the magnitude of HTN may not correlate with the presence or severity of symptoms. Cardiogenic shock and congestive heart failure (as in case 4), two rare and severe presentations of neonatal HTN, can result in massive cardiovascular collapse which may be life threatening [47, 48]. Often, HTN is accompanied by nonspecific signs such as irritability, lethargy, poor feeding, unexplained tachypnea or seizures—frequently only appreciated in retrospect.
Ensuring accurate blood pressure measurement
Accurate BP measurement in neonates is essential to correctly identify HTN. The gold standard for BP measurement in neonates is direct intra-arterial measurement, with both umbilical artery and peripheral artery catheters finding similar values [49]. However, in clinical practice, indirect measurement of BP is more common and practical, with oscillometric devices the most common method of measurement. Oscillometric devices are easy to use in clinical care, and allow frequent monitoring over time. Studies demonstrate good correlation between invasive monitoring and oscillometric assessment; however, accuracy may vary depending on the size of the infant, with oscillometric devices more likely to over-read BP in smaller neonates [50]. Auscultation can also be considered, although this is difficult in neonates. However, its use should be considered to confirm elevated BP readings obtained with oscillometric devices, particularly in the NICU graduate or asymptomatic infant with observed elevated BPs [50].
The accuracy of BP measurement in neonates can be impacted by many factors. BP is most accurate in a quiet, resting infant and higher in those who are crying; however, other activities such as feeding or even non-nutritive sucking may increase BP as well (Fig. 2) [51, 52]. A consistent measurement technique is essential to obtain accurate BP values. Standardized protocols for measurement of BP are available [53, 54] and help to ensure that accurate BP values are obtained to guide clinical decision-making. Elements of these standardized protocols include proper infant positioning, measurement technique (including appropriate cuff size), and timing of measurement (Table 3) [55].

Effect of infant state on blood pressure (BP) (black bars, systolic BP; gray bars, diastolic BP). Data adapted from Satoh et al [52]
Diagnostic approach to hypertension
In many neonates, the cause of HTN can be identified from history and physical examination. A focused history should be obtained, including prenatal history including maternal medication use, details of delivery including concerns for perinatal asphyxia, and details of the neonatal history including presence of concurrent medical conditions associated with HTN, current and past medications, and any procedures the neonate has undergone (e.g., UAC placement).
A careful physical examination should be performed, which may indicate the primary etiology of HTN or may detect pathologic effects of HTN or end-organ dysfunction due to HTN, such as neurologic abnormalities, hypertensive retinopathy, or congestive heart failure. All infants with HTN should have BP readings obtained in all four extremities to rule out coarctation of the aorta or an aortic thrombus occluding the thoracic or abdominal aorta. However, given that in neonates upper and lower BPs can be similar, an echocardiogram is required to confirm the diagnosis of coarctation [55]. The infant’s general appearance should be assessed for dysmorphic features which may suggest an underlying syndrome such as Williams syndrome that includes HTN as a clinical manifestation. Careful cardiac and abdominal examinations should be performed, as abdominal distention or a mass may be indicative of obstructive uropathy, polycystic kidney disease, or abdominal tumors.
Laboratory testing should be directed towards assessment of renal function and determining whether renal parenchymal disease is present. Further diagnostic testing should be guided by the initial evaluation and individualized for each infant, and may include measurement of thyroxine, aldosterone, or cortisol (Table 4). Plasma renin activity can be quite high in neonates especially those born prematurely [56]; however, it may also be suppressed in neonates with pulmonary disease [21] making interpretation challenging. Given these concerns, measurement of plasma renin activity should be deferred unless other electrolyte abnormalities (e.g., hypokalemia) suggest a monogenic form of HTN [57].
Most hypertensive neonates will require one or more imaging studies to determine the cause of their HTN. Renal ultrasonography with Doppler evaluation is the initial imaging modality of choice, and may identify renal masses, urinary tract obstruction, or renal cystic disease, with Doppler flow studies assisting in the diagnosis of renal vessel thrombosis. Radionucleotide imaging may demonstrate renal perfusion abnormalities due to thromboembolic phenomenon [58]; however, the utility of this modality may be limited in the neonatal time period due to immature renal function and therefore plays little role in the assessment of hypertensive infants. Other studies, including echocardiograms and voiding cystourethrograms, should be performed as clinically indicated.
In neonates with extreme BP elevation, the clinician should consider vascular imaging to evaluate renovascular HTN, particularly renal artery stenosis. In our experience, neither computed tomographic angiography nor magnetic resonance angiography has sufficient resolution to detect most cases of renal artery stenosis in neonates. Arteriography offers the only accurate method of diagnosing renal artery stenosis, particularly given the high incidence of branch vessel disease seen in neonates [59]. However, most centers lack both the equipment and expertise to perform this procedure safely in newborns [60]. Therefore, in neonates with suspected renal artery stenosis, it may be more appropriate to control HTN medically until the neonate is large enough for an arteriogram to be performed safely for both definitive diagnosis and endovascular treatment.
Case 5
You are consulted by the NICU to see a 2-month-old former 26-week gestation infant with BPD who remains on supplemental oxygen. Over the last 2–3 weeks, the NICU team has noted that the infant’s BPs have been mostly around 100/65, with none below 85/55. The infant’s workup which included laboratory evaluation showing normal kidney function and imaging, including echocardiogram and renal ultrasound, does not demonstrate any other etiology of her hypertension. What should be done to manage the infant’s HTN?
Approach to treatment
While data on the treatment of HTN in neonates is limited, the approach to management is similar to that in older children, except that non-pharmacologic therapy has a very limited role (if any) in the treatment of hypertensive neonates. Of note, confirmation of elevated blood pressure through accurate measurement techniques (as discussed above) is essential prior to initiating any interventions or treatment. The first intervention should be the correction of iatrogenic causes of HTN whenever present, such as inotrope administration, dexamethasone or other medications, hypercalcemia, or volume overload. Specific approaches may be warranted in other hypertensive neonates, such as treatment of pain, correction of hypoxemia in infants with BPD, and hormonal replacement in those with endocrine disorders.
Initiation of antihypertensive medications may need to be considered in many hypertensive neonates such as the one mentioned above. Clinical criteria for initiating therapy are not well defined, so except in severe HTN with end-organ manifestations (e.g., heart failure or seizures), this can be a difficult decision. No studies exist on the adverse effects of chronic HTN in infancy, and few antihypertensive medications have ever been studied in neonates. Of note, available case series and other studies describe a wide variety of antihypertensive medications prescribed to hypertensive neonates [18, 19, 61]. Additionally, as noted previously, determining what BP threshold at which to consider treatment can be difficult due to the lack of robust normative data. Therefore, clinical expertise should be used to guide decision-making. Given the information available for the infant described in case 5, antihypertensive medication treatment would be a key consideration given the persistence of elevated BP readings over several weeks.
The infant with acute severe hypertension
In infants with acute severe HTN (previously called hypertensive emergency), defined as hypertension with evidence of end-organ dysfunction, intravenous infusions of antihypertensive agents should be utilized. Continuous intravenous infusions have several advantages; most importantly, they allow for quick titration of the infusion rate to achieve the desired BP control. Unfortunately, few data are available regarding the use of intravenous infusions in neonates. As with all patients with severe HTN, care should be taken to avoid cerebral ischemia and hemorrhage due to rapid reduction of BP, a problem that premature infants may be at increased risk of due to periventricular circulation immaturity [62]. In the setting of severe HTN, oral agents should be avoided given their variable duration of effect, onset of action, and unpredictable response. Published reports suggest that the calcium channel blocker nicardipine may be particularly useful in infants with acute severe HTN [63, 64]. Other drugs that have been successfully used in neonates include nitroprusside [65], esmolol [66], and labetalol [67]. Whatever agent is chosen for use, BP should be monitored continuously via an indwelling arterial catheter, or by frequently repeated cuff readings to titrate dose to achieve the desired effect.
Intermittently administered intravenous agents have a role in treatment of some hypertensive infants, particularly in those with mild-to-moderate HTN that cannot tolerate oral therapy due to gastrointestinal dysfunction (Table 5). Hydralazine and labetalol in particular have been widely used in infants, and appear to be well tolerated [15]. Additional details of managing infants with acute severe HTN are available elsewhere [68].
The stable infant with moderate hypertension
Oral antihypertensives (Table 5) should be used in cases of less severe HTN or infants with chronic HTN controlled with intravenous medications to transition to oral therapy. We often start oral therapy with the calcium channel blocker isradipine [69, 70]. While amlodipine may also be used, it has a slower onset of action, and its prolonged duration of effect may be less useful in the acute setting. Both isradipine and amlodipine can be compounded into a 1 mg/mL solution, allowing for administration of the small doses required in neonates. Other useful vasodilators include hydralazine and minoxidil. Beta blockers may need to be avoided in chronic therapy of neonatal HTN, particularly in infants with chronic lung disease. In infants with BPD, diuretics not only control HTN but may improve pulmonary status [21, 71]. Use of oral antihypertensive therapy would be appropriate for the infant described in case 5.
In neonates, the use of angiotensin-converting enzyme inhibitors (ACEI) and other agents affecting the renin-angiotensin-aldosterone system (RAAS) is controversial. While captopril has been demonstrated to be effective in hypertensive neonates, it may cause an exaggerated fall in BP, especially in premature infants [72, 73]. Additionally, hyperkalemia, acute kidney injury, and severe hypotension have also been reported with ACEI treatment due to RAAS activation in neonates [74, 75], which reflects the importance of the RAAS in nephron development [76, 77]. Although few data exist on this topic, the concern with overuse of ACEI in infants is that they may impair the final stages of renal maturation. While a recent systematic review provides additional data on the safety of ACEI [3], we typically avoid use of ACEI until infants have reached a corrected post-menstrual age of 44 weeks.
Surgical correction of hypertension
In a limited set of clinical scenarios, surgery may be indicated for treatment of neonatal HTN. This is most commonly seen in infants with aortic coarctation or renal obstruction [78]. As previously discussed, in neonates with renal artery stenosis, medical management with BP control may be necessary until the infant has grown enough to safely undergo definitive vascular repair [79]. However, in severe cases of neonatal renal artery stenosis where endovascular approach is impossible and BP remains poorly controlled, unilateral nephrectomy may be needed [80]. In infants with malignant causes of HTN, such as neuroblastoma, surgical tumor removal may be indicated, possibly following chemotherapy. In infants with MCDK with severe HTN, nephrectomy may be considered if BP control remains challenging [81].
Outcomes
For most neonates diagnosed with HTN, the long-term outcomes should be good. However, our knowledge is limited by a paucity of data, and long-term outcome studies of infants with neonatal HTN are needed. Outcomes are largely dependent on the underlying cause of HTN, as some forms of neonatal HTN, such as HTN-related renal parenchymal disease or polycystic kidney disease, may persist beyond infancy [18, 19]. Neonates with renal vessel thrombosis may continue to be hypertensive, and in some cases, this HTN merits unilateral nephrectomy for BP control [82]. HTN may persist in children despite vascular repair in both cases of renal vessel thrombosis as well as aortic coarctation [38]. This late HTN should be carefully monitored in patients after vascular surgery, and may represent continued vascular abnormalities, but also could represent re-stenosis and prompt further imaging.
However, most causes of neonatal HTN are related to umbilical catheter placement or are idiopathic, and available information suggests that HTN in these clinical situations will resolve over time [16, 21, 83, 84]. Often, these infants may initially require increases in their antihypertensive therapy over the first several months of life as they demonstrate catchup growth. However, after the first several months, it is usually possible to wean their medication either by decreasing the dose or by making no further dose increases as the infant grows. Despite the fact that long-term follow-up data is sparse on neonates with HTN, one study indicates that most infants will be off medication by 6 month of age [17].
Long-term monitoring of infants with neonatal HTN is essential. For those discharged on antihypertensive treatment, we find home BP monitoring is a useful tool to monitor and adjust medication doses between office visits. While setting up such services can be challenging, we feel it should be strongly considered. Given the issues with measurement of BP in neonates, use of an oscillometric device is the best option for home monitoring. While no data has been published regarding the outcome of hypertensive infants in late childhood or adolescence, it is prudent to follow all patients with neonatal HTN with periodic monitoring of BPs and renal function, at least until the HTN has resolved. Serial ultrasonography may be helpful to follow renal growth, or the evolution of renal parenchymal disease.
As nephrogenesis continues through most of prenatal development, and is completed at 36 weeks gestation, many neonates may be born prior to the completion of nephron development [85]. While nephrogenesis may continue in premature infants for up to 40 days following birth, these nephrons are abnormal and age at an accelerated rate [86]. Therefore, premature infants do not develop the full complement of glomeruli of term infants. Reduced nephron mass appears to be a risk factor for the development of adult HTN [87]. In a recent single-center case series, there was a high incidence of prematurity in children with otherwise unexplained HTN [88]. Therefore, hypertensive neonates (as well as normotensive neonates born prematurely) may be at increased risk during late adolescence or early adulthood compared to term infants for the development of HTN [89].
Conclusions
Normal BP values in neonates are dependent on many factors, including birth weight, gestational age, and post-menstrual age, with maternal health and other perinatal factors also playing important roles. HTN is more frequently observed in neonates with concurrent conditions such as bronchopulmonary dysplasia and renal parenchymal disease or in those who have undergone umbilical arterial catheterization. The diagnosis of neonatal HTN is made more challenging due to difficulties with measurement in the neonate as well as the lack of standardized norms. A diagnostic evaluation should be undertaken, and in most infants, it will result in determination of an underlying cause of HTN. Treatment should be determined by severity of the HTN; when pharmacotherapy is indicated, it may include intravenous and/or oral therapy. Despite the increased knowledge over the past several decades, there remain many areas in which better data are needed, particularly with respect to diagnostic thresholds and antihypertensive medications. Most infants with neonatal HTN will resolve their HTN over time, although a small number may have persistent BP elevation.
Key summary points
-
1.
By allosteric modulation of the calcium-sensing receptor, calcimimetics make the receptor more sensitive to circulating calcium, reading its actual concentration as a higher one, thus leading to suppression of PTH secretion.
-
2.
By inhibiting the activity of Na+–K+–2Cl– cotransporter in the TAL, calcimimetics cause a decrease in calcium reabsorption and possible hypercalciuria. The latter is amenable to treatment with thiazide diuretics.
-
3.
The use of calcimimetics to suppress PTH production in several pediatric genetic and acquired disorders, in which kidney function is normal, seems to be safe and effective.
-
4.
The main adverse effects of treatment with calcimimetics include clinically nausea and vomiting, and biochemically hypocalcemia and hypercalciuria. Careful attention should be paid to hypocalcemia that may require additional active vitamin D metabolites.
Multiple Choice Questions (Answers are provided following the reference list)
-
1.
Which of the following is not part of the typical initial evaluation of a neonate with hypertension?
-
a)
BUN and Creatinine
-
b)
Urinalysis
-
c)
Thyroid studies
-
d)
Renal ultrasound with Doppler
-
e)
Medication review
-
a)
-
2.
What is the most frequently implicated etiology for a neonate with hypertension?
-
a)
Renal vein thrombosis
-
b)
Dexamethasone
-
c)
Bronchopulmonary dysplasia
-
d)
Catheter-associated thromboembolism
-
e)
Malignant tumors
-
a)
-
3.
Which is a true statement regarding measurement of neonatal blood pressure?
-
a)
Blood pressures obtained in the calf are equivalent to upper arm blood pressure values for the first 6 months
-
b)
Measurement of blood pressure should be performed during feeding for optimal accuracy
-
c)
Positioning of infant does not alter blood pressure measurement
-
d)
Blood pressure should not be obtained more than one time, as repeated assessment may impact accuracy
-
a)
-
4.
What is the most common long-term outcome of neonatal hypertension?
-
a)
Resolution of hypertension during NICU stay
-
b)
Ongoing hypertension requiring stable but ongoing antihypertensive management
-
c)
Progression of disease with escalation of antihypertensive therapy
-
d)
Resolution of hypertension by 1 year of age
-
e)
Surgical correction
-
a)
-
5.
Which of the following is not a recommended class of blood pressure medication for premature neonates with hypertension?
-
a)
Calcium channel blockers
-
b)
Direct vasodilator
-
c)
β - antagonists
-
d)
Angiotensin receptor blockers
-
e)
Diuretics
-
a)
Change history
27 June 2019
The original version of this article unfortunately contained a mistake. Due to a production error, the wrong “Key summary points” were included. The correct key summary points are listed below.
References
Adelman RD (1978) Neonatal hypertension. Pediatr Clin N Am 25:99–110
Watkinson M (2002) Hypertension in the newborn baby. Arch Dis Child Fetal Neonatal Ed 86:F78–F81
Snauwaert E, Vande Walle J, De Bruyne P (2016) Therapeutic efficacy and safety of ACE inhibitors in the hypertensive paediatric population: a review. Arch Dis Child 102:63–71
Dionne JM (2018) Neonatal and infant hypertension. In: Flynn JT, Ingelfinger JR, Redwine KM (eds) Pediatric Hypertension, 4th edn. Springer Science+Business Media, New York, pp 539–563
Flynn JT, Kaelber DC, Baker-Smith CM, Blowey D, Carroll AE, Daniels SR, de Ferranti SD, Dionne JM, Falkner B, Finn SK, Gidding SS, Goodwin C, Leu MG, Powers ME, Rea C, Samuels J, Simasek M, Thaker VV, Urbina EM, Subcommittee on Screening and Management of High Blood Pressure in Children (2017) Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics 140:e20171904
Kent AL, Kecskes Z, Shadbolt B, Falk MC (2007) Blood pressure in the first year of life in healthy infants born at term. Pediatr Nephrol 22:1743–1749
Hegyi T, Anwar M, Carbone MT, Ostfeld B, Hiatt M, Koons A, Pinto-Martin J, Paneth N (1996) Blood pressure ranges in premature infants: II. The first week of life. Pediatrics 97:336–342
Georgieff MK, Mills MM, Gómez-Marín O, Sinaiko AR (1996) Rate of change of blood pressure in premature and full term infants from birth to 4 months. Pediatr Nephrol 10:152–155
Zubrow AB, Hulman S, Kushner H, Falkner B (1995) Determinants of blood pressure in infants admitted to neonatal intensive care units: a prospective multicenter study. J Perinatol 15:470–479.
Pejovic B, Peco-Antic A, Marinkovic-Eric J (2007) Blood pressure in non-critically ill preterm and full-term neonates. Pediatr Nephrol 22:249–257
Lurbe E, Garcia-Vicent C, Torro I, Fayos JL, Aguillar F, de Llano JM, Fuentes G, Redon J (2007) First-year blood pressure increase steepest in low birthweight newborns. J Hypertens 25:81–86
Dagle JM, Fisher TJ, Haynes SE, Berends SK, Brophy PD, Horriss FH, Murray JC (2011) Cytochrome P450 (CYP2D6) genotype is associated with elevated systolic blood pressure in preterm infants after discharge from the neonatal intensive care unit. J Pediatr 159:104–109
Kent AL, Chaudhari T (2013) Determinants of neonatal blood pressure. Curr Hypertens Rep 15:426–432
Sadoh WE, Ibhanesehbor SE, Monguno AM, Gubler DJ (2010) Predictors of newborn systolic blood pressure. West Afr J Med 29:86–90
Dionne JM, Abitbol CL, Flynn JT (2012) Hypertension in infancy: diagnosis, management and outcome. Pediatr Nephrol 27:17–32 Erratum in: Pediatr Nephrol. 2012; 27:159–60
Seliem WA, Falk MC, Shadbolt B, Kent AL (2007) Antenatal and postnatal risk factors for neonatal hypertension and infant follow-up. Pediatr Nephrol 22:2081–2087
Sahu R, Pannu H, Yu R, Stete S, Bricker JT, Gupta-Malhotra M (2013) Systemic hypertension requiring treatment in the neonatal intensive care unit. J Pediatr 163:84–88
Blowey DL, Duda PJ, Stokes P, Hall M (2011) Incidence and treatment of hypertension in the neonatal intensive care unit. J Am Soc Hypertens 5(6):478–483
Friedman AL, Hustead VA (1987) Hypertension in babies following discharge from a neonatal intensive care unit. Pediatr Nephrol 1:30–34
Shah AB, Hashmi SS, Sahulee R, Pannu H, Gupta-Malhotra M (2015) Characteristics of systemic hypertension in preterm children. J Am Soc Hypertens 17:364–370
Jenkins RD, Aziz JK, Gievers LL, Moorers HM, Fino N, Rozansky DJ (2017) Characteristics of hypertension in premature infants with and without chronic lung disease: a long-term multi-center study. Pediatr Nephrol 32:2115–2124
Neal WA, Reynolds JW, Jarvis CW, Williams HJ (1972) Umbilical artery catheterization: demonstration of arterial thrombosis by aortography. Pediatrics 50:6–13
Seibert JJ, Taylor BJ, Williamson SL, Williams BJ, Szabo JS, Corbitt SL (1987) Sonographic detection of neonatal umbilical-artery thrombosis: clinical correlation. Am J Roetgenol 148:965–968
Boo NY, Wong NC, Zulkifli SS, Lye MS (1999) Risk factors associated with umbilical vascular catheter-associated thrombosis in newborn infants. J Paediatr Child Health 35:460–465
Barrington KJ (1999) Umbilical artery catheters in the newborn: effects of position of the catheter tip. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.cd000505
Lau KK, Stoffman JM, Williams S (2007) Neonatal renal vein thrombosis: review of the English-language literature between 1992 and 2006. Pediatrics 120:e1278–e1284
Marks SD, Massicotte MP, Steele BT, Matsell DG, Filler G, Shah PS, Perlman M, Rosenblum ND, Shah VS (2005) Neonatal renal venous thrombosis: clinical outcomes and prevalence of prothrombotic disorders. J Pediatr 146:811–816
Tullus K, Brennan E, Hamilton G, Lord R, McLaren CA, Marks SD, Roebuck DJ (2008) Renovascular hypertension in children. Lancet 371:1453–1463
Das BB, Recto M, Shoemaker L, Mitchell M, Austin EH (2007) Midaortic syndrome presenting as neonatal hypertension. Pediatr Cardiol 29:1000–1001
Guay-Woodford LM, Desmond RA (2003) Autosomal recessive polycystic kidney disease: the clinical experience in North America. Pediatrics 111:1072–1080
Moralıoğlu S, Celayir AC, Bosnalı O, Pektas OZ, Bulut IK (2014) Single center experience in patients with unilateral multicystic dysplastic kidney. J Pediatr Urol 10:763–768
Gilboa N, Urizar RE (1983) Severe hypertension in newborn after pyeloplasty of hydronephrotic kidney. Urology 22:179–182
Selewski DT, Charlton JR, Jetton JG, Guillet R, Mhanna MJ, Askenazi DJ, Kent AL (2015) Neonatal acute kidney injury. Pediatrics 136:e463–e473
Abman SH, Warady BA, Lum GM, Koops BL (1984) Systemic hypertension in infants with bronchopulmonary dysplasia. J Pediatr 104:928–931
Abman SH (2002) Monitoring cardiovascular function in infants with chronic lung disease of prematurity. Arch Dis Child Fetal Neonatal Ed 87:F15–F18
Sehgal A, Malikiwi A, Paul E, Tan K, Menahem S (2016) Systemic arterial stiffness in infants with bronchopulmonary dysplasia: potential cause of systemic hypertension. J Perinatol 36:564–569
Flynn JT (2000) Neonatal hypertension: diagnosis and management. Pediatr Nephrol 14:332–341
Lee MG, Kowalski R, Galati JC, Cheung MM, Jones B, Koleff J, d’Udekem Y (2012) Twenty-four-hour ambulatory blood pressure monitoring detects a high prevalence of hypertension late after coarctation repair in patients with hypoplastic arches. J Thorac Cardiovasc Surg 144:1110–1116
Durand M, Sangha B, Cabal LA, Hoppenbrouwers T, Hodgeman JE (1989) Cardiopulmonary and intracranial pressure changes related to endotracheal suctioning in preterm infants. Crit Care Med 17:506–510
Abiramalatha T, Sherba B, Joseph R, Thomas N (2016) Unusual complications of placental chorioangioma: consumption coagulopathy and hypertension in a preterm newborn. BMJ Case Rep https://doi.org/10.1136/bcr-2016-215,734.
Peranteau WH, Tharakan SJ, Partridge E, Herkert L, Rintoul NE, Flake AW, Adzick NS, Hedrick HL (2015) Systemic hypertension in giant omphalocele: an underappreciated association. J Pediatr Surg 50:1477–1480.
Marinelli KA, Burke GS, Herson VC (1997) Effects of dexamethasone on blood pressure in premature infants with bronchopulmonary dysplasia. J Pediatr 130:594–602
Merritt JC, Kraybill EN (1981) Effect of mydriatics on blood pressure in premature infants. J Pediatr Ophthalmol Strabismus 18:42–46
Horn PT (1992) Persistent hypertension after prenatal cocaine exposure. J Pediatr 121:288–291
Becker JA, Short BL, Martin GR (1998) Cardiovascular complications adversely affect survival during extracorporeal membrane oxygenation. Crit Care Med 26:1582–1586
Boedy RF, Goldberg AK, Howell CG, Hulse E, Edwards EG, Kanto WP (1990) Incidence of hypertension in infants on extracorporeal membrane oxygenation. J Pediatr Surg 25:258–261
Louw J, Brown S, Thewissen L, Smits A, Eyskens B, Heying R, Cools B, Levtchenko E, Allegaert K, Gewillig M (2013) Neonatal circulatory failure due to acute hypertensive crisis: clinical and echocardiographic clues. Cardiovasc J Afr 24:72–75
Xiao N, Tandon A, Goldstein S, Lorts A (2013) Cardiogenic shock as the initial presentation of neonatal systemic hypertension. J Neonatal Perinatal Med 6:267–272
Butt WW, Whyte H (1984) Blood pressure monitoring in neonates: Comparison of umbilical and peripheral artery catheter measurements. J Pediatr 105:630–632
O’Shea J, Dempsey EM (2009) A comparison of blood pressure measurements in newborns. Am J Perinatol 26:113–116
Yiallourou SR, Poole H, Prathivadi P, Odoi A, Wong FY, Horne RS (2014) The effects of dummy/pacifier use on infant blood pressure and autonomic activity during sleep. Sleep Med 15:1508–1516
Satoh M, Inoue R, Tada H, Hosaka M, Metoki H, Asayama K, Murakami T, Mano N, Ohkubo T, Yagihashi K, Hoshi K, Suzuki M, Imai Y (2016) Reference values and associated factors for Japanese newborns’ blood pressure and pulse rate. J Hypertens 34:1578–1585
Stebor AD (2005) Basic principles of noninvasive blood pressure measurement in infants. Adv Neonatal Care 5:252–261
Nwankwo MU, Lorenz JM, Gardiner JC (1997) A standard protocol for blood pressure measurement in the newborn. Pediatrics 99:e10
Crossland DS, Furness JC, Abu-Harb M, Sadagopan SN, Wren C (2004) Variability of four limb blood pressure in normal neonates. Arch Dis Child Fetal Neonatal Ed 89:F325–F327
Richer C, Hornych H, Amiel-Tison C, Relier JP, Giudicelli JF (1977) Plasma renin activity and its postnatal development in preterm infants. Preliminary report. Biol Neonate 31:301–304
Vehaskari VM (2009) Heritable forms of hypertension. Pediatr Nephrol 24:1929–1937
Roth CG, Spottswood SE, Chan JC, Roth KS (2003) Evaluation of the hypertensive infant: a rational approach to diagnosis. Radiol Clin North Am 41:931–944
Vo NJ, Hammelman BD, Racadio JM, Strife CF, Johnson ND, Racadio JM (2006) Anatomic distribution of renal artery stenosis in children: implications for imaging. Pediatr Radiol 36:1032–1036
Peco-Antic A, Djukic M, Sagic D, Kruscic D, Krstic Z (2006) Severe renovascular hypertension in an infant with congenital solitary pelvic kidney. Pediatr Nephrol 21:437–440
Ravisankar S, Kuehn D, Clark RH, Greenberg RG, Smith PB, Hornik CP (2016) Antihypertensive drug exposure in premature infants from 1997 to 2013. Cardiol Young 27:905–911
Flynn JT, Tullus K (2008) Severe hypertension in children and adolescents: pathophysiology and treatment. Pediatr Nephrol 24:1101–1112
Flynn JT, Mottes TA, Brophy PD, Kershaw DB, Smoyer WE, Bunchman TE (2001) Intravenous nicardipine for treatment of severe hypertension in children. J Pediatr 139:38–43
Gouyon JB, Geneste B, Semama DS, Francoise M, Germain JF (1997) Intravenous nicardipine in hypertensive preterm infants. Arch Dis Child Fetal Neonatal Ed 76:F126–F127
Benitz WE, Malachowski N, Cohen RS, Stevenson DK, Ariagno RL, Sunshine P (1985) Use of sodium nitroprusside in neonates: efficacy and safety. J Pediatr 106:102–110.
Wiest DB, Garner SS, Uber WE, Sade RM (1998) Esmolol for the management of pediatric hypertension after cardiac operations. J Thorac Cardiovasc Surg 115:890–897
Thomas CA, Moffett BS, Wagner JL, Mott AR, Feig DI (2011) Safety and efficacy of intravenous labetalol for hypertensive crisis in infants and small children. Pediatr Crit Care Med 12:28–32
Dionne JM, Flynn JT (2017) Management of severe hypertension in the newborn. Arch Dis Child 102:1176–1179
Flynn J, Warnick S (2002) Isradipine treatment of hypertension in children: a single-center experience. Pediatr Nephrol 17:748–753
Miyashita Y, Peterson D, Rees JM, Flynn JT (2010) Isradipine for treatment of acute hypertension in hospitalized children and adolescents. J Clin Hypertens 12:850–855
Kao LC, Durand DJ, McCrea RC, Birch M, Powers RJ, Nickerson BG (1994) Randomized trial of long-term diuretic therapy for infants with oxygen-dependent bronchopulmonary dysplasia. J Pediatr 124:772–781
O’Dea RF, Mirkin BL, Alward CT, Sinaiko AR (1988) Treatment of neonatal hypertension with captopril. J Pediatr 113:403–406
Tack ED, Perlman JM (1988) Renal failure in sick hypertensive premature infants receiving captopril therapy. J Pediatr 112:805–810
Ku LC, Zimmerman K, Benjamin DK, Clark RH, Hornik CP, Smith PB (2016) Safety of Enalapril in infants admitted to the neonatal intensive care unit. Pediatr Cardiol 38:155–161
Pandey R, Koshy RG, Dako J (2017) Angiotensin converting enzyme inhibitors induced acute kidney injury in newborn. J Matern Fetal Neonatal Med 30:748–750
Tufro-McReddie A, Romano LM, Harris JM, Ferder L, Gomez RA (1995) Angiotensin II regulates nephrogenesis and renal vascular development. Am J Physiol 269:F110–F115
Frölich S, Slattery P, Thomas D, Goren I, Ferreiros N, Jensen BL, Nusing RM (2017) Angiotensin II-AT1–receptor signaling is necessary for cyclooxygenase-2–dependent postnatal nephron generation. Kidney Int 91:818–829
Rajpoot DK, Duel B, Thayer K, Shanberg A (1999) Medically resistant neonatal hypertension: revisiting the surgical causes. J Perinatol 19:582–583
Bendel-Stenzel M, Najarian JS, Sinaiko AR (1996) Renal artery stenosis in infants: long-term medical treatment before surgery. Pediatr Nephrol 10:147–151
Kiessling SG, Wadhwa N, Kriss VM, Iocono J, Desai NS (2007) An unusual case of severe therapy-resistant hypertension in a newborn. Pediatrics 119:e301–e304
Abdulhannan P, Stahlschmidt J, Subramaniam R (2011) Multicystic dysplastic kidney disease and hypertension: clinical and pathological correlation. J Pediatr Urol 7:566–568
Mocan H, Beattie TJ, Murphy AV (1991) Renal venous thrombosis in infancy: long-term follow-up. Pediatr Nephrol 5:45–49
Adelman RD (1987) Long-term follow-up of neonatal renovascular hypertension. Pediatr Nephrol 1:35–41
Caplan MS, Cohn RA, Langman CB, Conway JA, Shkolnik A, Brouillette RT (1989) Favorable outcome of neonatal aortic thrombosis and renovascular hypertension. J Pediatr 115:291–295
The Low Birth Weight and Nephron Number Working Group (2017) The impact of kidney development on the life course: a consensus document for action. Nephron 136:3–49
Hughson M, Farris AB III, Douglas-Denton R, Hoy WE, Bertram JF (2003) Glomerular number and size in autopsy kidneys: the relationship to birth weight. Kidney Int 63:2113–2122
Keller G, Zimmer G, Mall G, Ritz E, Amann K (2003) Nephron number in patients with primary hypertension. N Engl J Med 348:101–108
Gupta-Malhotra M, Banker A, Shete S, Hashmi SS, Tyson JF, Barratt MS, Hecht JT, Milewicz DM, Boerwinkle E (2015) Essential hypertension vs. secondary hypertension among children. Am J Hypertens 28:73–80
Shankaran S, Das A, Bauer CR, Bada H, Lester B, Wright L, Higgins R, Poole K (2006) Fetal origin of childhood disease: intrauterine growth restriction in term infants and risk for hypertension at 6 years of age. Arch Pediatr Adolesc Med 160:977–981
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
The authors have no disclosures relevant to the content of this article.
Additional information
Multiple Choice Answers
1. c; 2. d; 3. a; 4. d; 5. d.
Rights and permissions
About this article

Cite this article
Starr, M.C., Flynn, J.T. Neonatal hypertension: cases, causes, and clinical approach. Pediatr Nephrol 34, 787–799 (2019). https://doi.org/10.1007/s00467-018-3977-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-018-3977-4