
Abstract
The aim of this study was to evaluate to which extend adult reference intervals (RIs) could be applied in children. A local paediatric population (aged 1 to < 20 years), based on first draw samples from general practitioners (GPs), was established. Children with samples taken at a hospital or > 3 samples from GPs were excluded. Analytes evaluated included haematological, liver and pancreatic function, kidney function, electrolytes, and metabolism parameters. Applicability of adult RIs in children aged 1–17 years was evaluated using individuals aged 18–19 years as reference groups for the adult RIs. The local population consisted of 31,024 children with 282,721 analyses in total. For each analyte, 17 age strata and two gender strata were established. Partitioning was not warranted in 51% of the male strata and in 69% of the female strata. Adult RIs could be applied in 42% for children aged 1–< 10 years, 57% for children aged 10–< 15 years, and 85% for children aged 15–<18 years.
Conclusion: for certain analytes, there is no need to partition between adult and paediatric RIs, but a need for age- and gender-specific RIs remains for several clinical laboratory tests.
What is Known: • Establishing paediatric reference intervals (RIs) is time consuming, costly, and not feasible for many laboratories. Transference of RIs established elsewhere often leads to misclassification of paediatric laboratory results. • Adult RIs are often more easily established and validated. | |
What is New: • Adult RIs can be applied to children as young as 2 years for some analytes. Conversely, for some analytes, adult RIs cannot be applied in children aged 1–17 years. • Laboratory data can be applied in evaluating the need for partitioning in reference intervals. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Reliable paediatric reference intervals (RIs) are fundamental for the interpretation of laboratory results, and thus correct diagnosis and treatment of patients [1]. Establishing paediatric RIs can however be a precarious, costly, and time-consuming process, as sampling from healthy, representative children is recommended according to the Clinical and Laboratory Standards Institute (CLSI) guideline on establishing and verifying reference intervals [2]. Sampling from especially young children is furthermore technically difficult and associated with ethical considerations [3]. As an alternative, the CLSI notes that laboratories can transfer paediatric RIs established elsewhere onto their local population [2]. However, applicability of a transferred RI is questionable due to a substantial variation in methodology applied in the studies establishing paediatric RIs, which leads to vast differences in published paediatric RIs [4]. This is reflected by the fact that seemingly comparable RIs classify samples differently [4]. Generally, adult RIs are well documented [1], and the establishment of adult RIs tends to be more feasible than performing paediatric RIs. Therefore, the aim of this study was to apply a data mining approach to evaluate the extend of which partitioning between adult and paediatric RIs was warranted and thus whether adult RIs could be applied in a local paediatric population.
Methods
We defined a local paediatric population based on anonymous laboratory data of paediatric samples (age 1 to < 20 years) from general practitioners (GPs) analysed over a five-year period (September 2012–August 2017) at the Department of Clinical Biochemistry and Immunology, Lillebaelt Hospital (LH) and the Department of Clinical Biochemistry and Pharmacology, Odense University Hospital (OUH). Data were analysed and handled in agreement with the Danish Data Protection Agency and the regulations established by the National Committee on Health Research Ethics in Denmark. Both hospitals are situated in the region of Southern Denmark and have a catchment area of approx. 730,000 patients and analyse blood samples from local GPs. To ensure an overall healthy population, children who had samples requested from others than the local GP (i.e., a hospital department) in the corresponding period were excluded. Children with > 3 repeat measurements in the time period were also excluded and only the first sampling was included for further analysis. We evaluated children age 1 to 17 years, while individuals aged 18–19 years constituted the reference adult group. Each subgroup (1-year, gender subdivided stratum) was compared with this adult reference group to establish if the distribution allowed common reference intervals; i.e., if partitioning between adults and children was recommended or not. In accordance with the Clinical and Laboratory Standards Institute (CLSI) guideline on defining, establishing, and verifying RIs [2], ≥ 120 samples were required in each subgroup, and strata with < 120 samples were not evaluated.
We evaluated analytes for which adult RIs are well established by Rustad et al. [5] and Nordin et al. [6]. Analytes included haematological parameters, liver and pancreatic function tests, kidney function tests, electrolytes, and metabolism, see Table 1 for details. Haematological parameters in the local dataset were analysed using Sysmex XN-9000 (Sysmex, Kobe, Japan). The remainder was analysed with Cobas® 6000 (Roche Diagnostics, Switzerland) (LH until September 2015), Architect (Abbott Diagnostics, USA) (OUH until August 2017), and Cobas® 8000 (Roche Diagnostics, USA) (OUH August 2017 onwards, LH September 2015 onwards). Units are declared according to the International System of Units (SI), and SI units are used throughout this article.
Statistics
The LH/OUH dataset was partitioned into 1-year age stratifications and subdivided into gender partitions. The dataset was transformed to a Gaussian distribution using the Box-Cox method and outliers were removed after stratification using Tukey’s method [7]. Each stratified subgroup was compared with data from the adult group of the same gender (18–19 years) to evaluate whether partitioning was required or whether the same RI was appropriate. We used two partitioning criteria in accordance with Harris et al. [8]. First, we used Harris and Boyd’s method [9], which evaluates difference in mean between two subgroups:
In which, \( {\overline{x}}_i \) is the mean, si is the standard deviation (SD), and ni the sample size of the subgroup. The suggested critical value of z* [8] was calculated as
If z < z*, partitioning was not recommended, and the adult RI could be accepted. Secondly, we applied the standard deviation (SD) criterion, in which the SDs of the subgroups were compared. If the ratio between the SDs exceeded 1.5, partitioning was warranted [8]. Thus, if neither the Harris and Boyd nor the SD criteria warranted partitioning, the adult RI was applicable for the specific paediatric subset. For calculation example, see supplementary data 1.
Frequencies are reported as numbers and percentages. Normally distributed data are presented as mean and standard deviation (SD), whilst median and interquartile range is used for non-normally distributed data. Data were analysed with Stata software package (Stata 15.1; StataCorp, College Station, TX, USA) and GraphPad Prism 5.0 (GraphPad Software, La Jolla, CA, USA).
Results
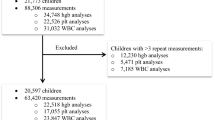
The final LH/OUH population consisted of 31,024 (Fig. 1), predominantly female (55%), children with 282,721 analyses in total (Table 1 and supplementary Table 1). For each analyte, 17 age strata and two gender strata were established. Data on amylase, aspartate transaminase, conjugated bilirubin, creatinine kinase, glucose, magnesium, phosphate, and total protein were excluded due to insufficient data (i.e., ≤ 120 individuals per subgroup). The most frequent analyses in the local population were leukocytes (lkc), creatinine (Cr), alanine transaminase (ALT), haemoglobin (hgb), potassium (K), sodium (Na), and alkaline phosphatase (ALP), which constituted 54% of the total analyses.

Establishment of local dataset
There were 850 (425 male and 425 female) possible paediatric partitions. Of these, 231 (54%) of the male (M) strata and 247 (58%) of the female (F) strata contained > 120 individuals (for details on number of samples for each analyte and partition, see supplementary Table 1). Table 2 shows where partitioning was warranted according to the criteria. Partitioning was not warranted in 118 (51%) of the male strata and in 171 (69%) of the female strata (for details on z, z*3, and SD ratio values, see supplementary Table 2), i.e., adult RIs could overall be applied in 289 (60%) out of the 478 partitions evaluated. For ALP (M) and GGT (M), partitioning was necessary for all paediatric subgroups evaluated according to the z*3 and the SD criteria. Conversely, EVF (F), Erc (F), MCH (F), Lkc (F), Plt (F), Fe (F), Alb (F), LDH (F), BUN, UA, Na (F), K, Ca, CHOL (M), HDL, and TGL did not warrant any partitioning, indicating that adult RIs could be applied for all paediatric strata evaluated. The need for partitioning decreased with increasing age, but the age for which adult RIs could be applied varied according to analyte, see Table 2. Adult RIs could be applied in 65 (42%) out of 153 partitions for children aged 1–< 10 years evaluated. In comparison, in 107 (57%) of the 188 partitions for children aged 10–< 15 years, and 117 (85%) of the 137 partitions for children aged 15–< 18 years evaluated, adult RIs were regarded applicable. For two analytes (ALP (M) and GGT (M)), partitioning was also warranted in children aged 17 years. For 7 analytes (Hgb (F), MCHC (M), Fe (M), Alb (M), AMYP (M) CHOL (F), and LDL), there was an inconsistency between applicability of adult RIs and increasing age, as the adult RIs were applicable in the youngest and oldest age partitions evaluated but not in all of the age partitions in-between these.
Several analytes had fewer than 120 individuals per strata, and applicability of adult RIs could therefore not be evaluated. This was most pronounced for the younger children, as 34% of the strata for children aged 1–< 10 years had ≥ 120 individuals. In comparison, 74% of the strata from children aged 10–< 15 years and 91% of strata from children aged 15–< 18 years had ≥ 120 individuals). Table 3 summarized the age and gender partitions, for which adult reference intervals could be applied.
Discussion
The present study shows that for several analytes there is no need for partitioning between adults and children, meaning that in a majority of cases, adult RIs can be applied in a paediatric population. Overall, our data showed that in a local paediatric population adult RIs could be applied in 60% of cases, and there was a decreasing need for partitioning between adults and children with increasing age.
The need for partitioning was variable and depended on the specific analyte in question. Whilst some adult RIs were universally applicable for the age strata tested, others were only applicable for the oldest age groups. Our results are in line with the results from the CALIPER Pediatric Reference Interval Database [10, 11], which did not find partitioning warranted for Na, K, Ca, or TGL for children aged 1–< 19 years indicating an age- and gender-independent physiological function. Electrolytes, including Na, K, and Ca have low intra- and inter-individual biological variation [12], which supports the fact that no age- or gender-related partitioning is needed for these analytes. In contrast hereto, we found that adult RIs for Hgb could only be applied in boys aged > 16 years. Adult Hgb RIs could however be applied in girls as young as 5 years. The German KiGGS study [13] and the CALIPER study [14] found similar results, with greater variability in male Hgb levels than in females, supporting our findings.
Childhood can be divided into separate developmental stages [15], with transitioning between these stages being highly individual, e.g., the onset of puberty [16]. Our finding of a decreasing need for partitioning with increasing age depict the physiological changes occurring with the transition from one stage to another. Interestingly, for some analytes, results stated that partitioning was warranted even for individuals aged 17 years, which generally surpasses the age when individuals are viewed as paediatric patients. Our results show that adult levels are reached at different ages, according to analyte and gender, which is important to bear in mind when diagnosing and treating children in general and teenagers in particular.
The Harris and Boyd criteria for partitioning used in this study is one of two methods recommended in the CLSI guideline [2]. The decision threshold of z*3 is based on a normal deviate testing of the significance of the difference between the means between two subgroups [8, 9]. Studies have suggested the criterion being relatively permissive of partitioning [17, 18]. The approach used in this study, where we combined the z*3 criterion with the SD1/SD2 ≤ 1.5 criterion, is therefore likely a conservative estimate of the applicability of adult RIs in children, and several “grey areas”, in which the clinical implications of partitioning versus non-partitioning has to be assessed, may exist. That the data state that separate RIs are warranted for Na for boys aged 4–13 years is an example hereof, as it is highly improbable that there is an actual, clinically relevant difference in Na between boys aged 4–12 and boys aged > 13 years. The approach applied here, however, ensures that for the paediatric strata where no indication for partitioning was found, application of the adult RIs is sound. Furthermore, several studies on paediatric reference intervals do not specify the method used for age and gender partitioning, as an undefinable subjective evaluation has been used [4]. This can lead to misinterpretation of biochemical results, and the method outlined here can be of assistance in determining when partitioning is statistically reasonable.
The CLSI guideline [2] mentions the robust method by Horn and Pesce [19] for establishing RIs with < 120 reference individuals. With the robust method, there is no limit of required observations. However, identification of and direct sampling on healthy and representative children is still required, thereby favouring validation of transferred RIs with an indirect method. The indirect sampling method outlined here is both feasible and reliable for evaluating the local applicability of RIs. In children, RIs are often transferred from the literature, as this is a more feasible approach than the establishment of laboratory specific RIs. Importantly, we have recently shown that published paediatric RIs differ considerably in terms of methodology applied for establishing the RIs and subsequently also in classification of healthy paediatric samples. Thus, we found that 65% of a local paediatric haemoglobin results were shown to change classification from normal (within the RI limits) to abnormal (above or below the RI limits) [4]. Several large and well-documented studies on adult RIs exist [5, 6, 10, 20], and applying adult RIs in paediatric populations could be advantageous where physiological differences are insignificant, because adherence to the recommendations regarding the establishment of a RI is more feasible in adults than in children.
There are some limitations to our approach; even though children with > 3 repeat samples and hospital contacts were excluded from the local population, it does not guarantee a completely healthy population, as an indication for biochemical analysis has been present for each child included. As the study was conducted on anonymous laboratory data, information regarding life style was not available. However, we believe that the approach outlined here ensures that critically ill children and children with prolonged illness have been excluded. Furthermore, the size of the dataset, which consists of > 31,000 children, ensures that few abnormal (i.e., diseased) values will have little influence and would be expected to be removed as outliers. As the inclusion of diseased children would in worst case tend to skew data and therefore expectedly lead to partition recommendation, it does not limit the results where partition is not recommended. The approach outlined here is thus feasible for evaluating transference of adult RIs onto paediatric populations. Another limitation is that the adult population in this study constituted 18–19 year olds. Individuals aged > 18 years are often regarded as adults, particularly in terms of RIs, but they may not be representative of an entire adult population, which has to be taken into account. Our data show the importance of partitioning based on physiology, which is reflected in the data and thus the need for age- and gender-specific partitioning. Generally, partitioning is only relevant in cases where it is of clinical relevance and thus illustrates a clinically relevant difference. In this study, data for MCHC (M), Fe (M), Alb (M), CHOL (F), and LDL suggest varying partitioning between adult and paediatric values according to age. It is however unlikely that this depicts a true, clinically significant difference. The method used in this study is permissive of separate partitions. Albeit this being a potential pitfall, the method ensures that in cases where no partitioning was found warranted, the RI can safely be applied. Altogether, our data underline the importance of combining clinical evaluation with biochemical results for correct diagnosis and management of the individual patient, which has also been stated by Harris and Boyd [8, 9, 17], Lahti et al. [18, 21, 22] and several others working with reference intervals [3, 23,24,25]. In children, it is vital to have RIs partitioned based on physiology, as emphasised in the CLSI guideline [2]. In prospective studies using a direct sampling approach, physiological considerations are important to ensure sufficient number of samples to establish the RI partitions needed. In that aspect, the indirect approach outlined here is more robust, as physiology is reflected in the biochemical results. Therefore, evaluating the need for partitioning is based on physiology in the indirect method. A final limitation of our study is that it only covers the most commonly applied analytes. With the data mining approach outlined here, it is possible to access large datasets that enable validation of complex analytes with statistical validity. There is a need for larger studies to validate our findings and evaluate data for rare analyses.
We do not advocate for the use of the adult RIs established by Rustad et al. [5] and Nordin et al. [6] in paediatric populations as we did not test whether there reference intervals were appropriate for the adult population. Rather, we wanted to contribute to a re-evaluation of the conventionally used partitioning between children and adults, and therefore the need for establishing specific paediatric reference intervals with the well-known problems connected hereto.
In conclusion, for several analytes, there is no need to partition between adult and paediatric RIs, but a need for age- and gender-specific RIs remains for several clinical laboratory tests and careful evaluation of the clinical implications of specific reference intervals must be always be considered. The use of laboratory data is however a feasible and reliable approach to evaluate the applicability of reference intervals.
Abbreviations
- Alb:
-
Albumin
- ALP:
-
Alkaline phosphatase
- ALT:
-
Alanine transaminase
- AMY:
-
Amylase
- AMYP:
-
Amylase, pancreatic
- AST:
-
Aspartate transaminase
- Bil, conj:
-
Bilirubin, conjugated
- BUN:
-
Blood urea nitrogen
- Ca:
-
Calcium
- CHOL:
-
Cholesterol
- CK:
-
Creatine kinase
- CLSI:
-
Clinical and Laboratory Standards Institute
- Cr:
-
Creatinine
- Erc:
-
Erythrocytes
- EVF:
-
Erythrocyte volume fraction
- F:
-
Female
- Fe:
-
Iron
- Glu:
-
Glucose
- GGT:
-
γ-Glutamyl transferase
- GP:
-
General practitioner
- HDL:
-
High-density lipoprotein
- Hgb:
-
Haemoglobin
- K:
-
Potassium
- LDH:
-
Lactate dehydrogenase
- LDL:
-
Low-density lipoprotein
- LH:
-
Lillebaelt Hospital
- Lkc:
-
Leukocytes
- M:
-
Male
- MCH:
-
Mean corpuscular haemoglobin
- MCHC:
-
Mean corpuscular haemoglobin concentration
- MCV:
-
Mean corpuscular volume
- Mg:
-
Magnesium
- Na:
-
Sodium
- OUH:
-
Odense University Hospital
- P:
-
Phosphate
- PLT:
-
Platelets
- RI:
-
Reference interval
- SI:
-
System of units
- SD:
-
Standard deviation
- TGL:
-
Triglyceride
- TP:
-
Total protein
- UA:
-
Uric acid
References
AACC. AACC calls on congress to fund CDC effort to improve pediatric medical testing: AACC.org; 2019 [Available from: https://www.aacc.org/media/press-release-archive/2019/03-mar/aacc-calls-on-congress-to-fund-cdc-effort-to-improve-pediatric-medical-testing
(CLSI) CaLSI. Defining, establishing, and verifying reference intervals in the clinical laboratory; approved guideline 2010
Tahmasebi H, Higgins V, Fung AWS, Truong D, White-Al Habeeb NMA, Adeli K (2017) Pediatric reference intervals for biochemical markers: gaps and challenges, recent national initiatives and future perspectives. EJIFCC. 28(1):43–63
Alnor AB, Vinholt PJ (2019) Paediatric reference intervals are heterogeneous and differ considerably in the classification of healthy paediatric blood samples. Eur J Pediatr
Rustad P, Felding P, Franzson L, Kairisto V, Lahti A, Martensson A et al (2004) The Nordic Reference Interval Project 2000: recommended reference intervals for 25 common biochemical properties. Scand J Clin Lab Invest 64(4):271–284
Nordin G, Martensson A, Swolin B, Sandberg S, Christensen NJ, Thorsteinsson V et al (2004) A multicentre study of reference intervals for haemoglobin, basic blood cell counts and erythrocyte indices in the adult population of the Nordic countries. Scand J Clin Lab Invest 64(4):385–398
Tukey JW (1977) Exploratory data analysis. Addison-Wesley, Reading
Harris EK, Wong ET, Shaw ST Jr (1991) Statistical criteria for separate reference intervals: race and gender groups in creatine kinase. Clin Chem 37(9):1580–1582
Harris EK, Boyd JC (1990) On dividing reference data into subgroups to produce separate reference ranges. Clin Chem 36(2):265–270
Adeli K, Higgins V, Trajcevski K, White-Al HN (2017) The Canadian laboratory initiative on pediatric reference intervals: a CALIPER white paper. Crit Rev Clin Lab Sci 54(6):358–413
Colantonio DA, Kyriakopoulou L, Chan MK, Daly CH, Brinc D, Venner AA, Pasic MD, Armbruster D, Adeli K (2012) Closing the gaps in pediatric laboratory reference intervals: a CALIPER database of 40 biochemical markers in a healthy and multiethnic population of children. Clin Chem 58(5):854–868
Aarsand AK, Diaz-Garzon J, Fernandez-Calle P, Guerra E, Locatelli M, Bartlett WA et al (2018) The EuBIVAS: within- and between-subject biological variation data for electrolytes, lipids, urea, uric acid, total protein, total bilirubin, direct bilirubin, and glucose. Clin Chem 64(9):1380–1393
Dortschy R, Rosario AS, Scheidt-Nave C, Thierfelder W, Thamm M, Gutsche J, et al. (2009) Bevölkerungsbezogene Verteilungswerte ausgewählter Laborparameter aus der Studie zur Gesundheit von Kindern und Jugendlichen in Deutschland (KiGGS). In: Robert-Koch I, editor. Berlin
Adeli K, Raizman JE, Chen Y, Higgins V, Nieuwesteeg M, Abdelhaleem M et al (2015) Complex biological profile of hematologic markers across pediatric, adult, and geriatric ages: establishment of robust pediatric and adult reference intervals on the basis of the Canadian Health Measures Survey. Clin Chem 61(8):1075–1086
Rosenfeld RG, Nicodemus BC (2003) The transition from adolescence to adult life: physiology of the ‘transition’ phase and its evolutionary basis. Horm Res 60(Suppl 1):74–77
Palmert MR, Boepple PA (2001) Variation in the timing of puberty: clinical spectrum and genetic investigation. J Clin Endocrinol Metab 86(6):2364–2368
Harris EK, Boyd JC (1995) Statistical bases of reference values in laboratory medicine. Marcel Dekker, New York
Lahti A, Hyltoft Petersen P, Boyd JC, Fraser CG, Jorgensen N (2002) Objective criteria for partitioning Gaussian-distributed reference values into subgroups. Clin Chem 48(2):338–352
Horn PS, Pesce AJ, Copeland BE (1998) A robust approach to reference interval estimation and evaluation. Clin Chem 44(3):622–631
Koerbin G, Potter JM, Andriolo K, West NP, Glasgow N, Hawkins C, Cavanaugh JA, Hickman PE (2017) ‘Aussie Normals’: an a priori study to develop reference intervals in a healthy Australian population using the Beckman Coulter LH 750 Haematology Analyser as candidates for harmonised values. Pathology. 49(5):518–525
Lahti A (2004) Are the common reference intervals truly common? Case studies on stratifying biochemical reference data by countries using two partitioning methods. Scand J Clin Lab Invest 64(4):407–430
Lahti A, Petersen PH, Boyd JC, Rustad P, Laake P, Solberg HE (2004) Partitioning of nonGaussian-distributed biochemical reference data into subgroups. Clin Chem 50(5):891–900
Lykkeboe S, Nielsen CG, Christensen PA (2018) Indirect method for validating transference of reference intervals. Clin Chem Lab Med 56(3):463–470
Zierk J, Arzideh F, Rechenauer T, Haeckel R, Rascher W, Metzler M, Rauh M (2015) Age- and sex-specific dynamics in 22 hematologic and biochemical analytes from birth to adolescence. Clin Chem 61(7):964–973
Zierk J, Arzideh F, Haeckel R, Rascher W, Rauh M, Metzler M (2013) Indirect determination of pediatric blood count reference intervals. Clin Chem Lab Med 51(4):863–872
Author information
Authors and Affiliations
Contributions
Anne Bryde Alnor and Pernille Just Vinholt contributed equally to the present study.
The authors contributed equally to the present study.
Corresponding author
Ethics declarations
This article does not contain any studies with human participant or animals performed by any of the authors. The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 72 kb)
Rights and permissions
About this article

Cite this article
Alnor, A.B., Vinholt, P.J. Application of adult reference intervals in children. Eur J Pediatr 179, 483–491 (2020). https://doi.org/10.1007/s00431-019-03527-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-019-03527-0