
Abstract
Objectives
The associations of PM with the risk and prognosis of breast cancer have not been determined. This systematic review aimed to provide an updated understanding of the relationship between PM exposure level and breast cancer incidence and mortality.
Methods
Articles from Web of Science and PubMed databases were methodically inspected until March 8, 2020. In final, 15 studies were kept for analysis, which provided necessary information to estimate the impact of PM on breast cancer risk and prognosis. These studies were combined for quantitative analyses to evaluate the effect of per 10 μg /m3 increment exposure of PM2.5 (< 2.5 μm in aerodynamic diameter) and PM10 (< 10 μm in aerodynamic diameter) using random-effects model.
Results
PM2.5 exposure was associated with increased breast cancer mortality (relative risk [RR] = 1.09; 95% confidence interval [CI]: 1.02, 1.16; PQ-test = 0.158). No association of PM2.5 (1.02; 0.97, 1.18; 0.308) and PM10 (1.03; 0.98, 1.09; 0.009) with the increase incidence of breast cancer was observed. Stratified analysis suggested that PM2.5 was associated with the increase mortality of breast cancer (1.10; 1.03, 1.17; 0.529) in subgroup of developed country. PM10 was associated with breast cancer incidence based on studies published after 2017 (1.08; 1.00, 1.15; 0.157) and European studies (1.15; 1.06, 1.25; 0.502).
Conclusions
Our study indicated that PM2.5 exposure was related to breast cancer mortality. Further researches in this field are needed to validate the conclusion.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Breast cancer has developed into one of the most prevalent cancers threatening the survival of women worldwide. According to the latest report released by the American Cancer Society, new incidence of breast cancer in 2019 will rank first among all female cancer (n = 268,600), accounting for 30%, and the mortality of breast cancer will be the second highest (n = 41,760), accounting for 15% in America (Siegel et al. 2019).
Air pollution exposure is closely linked to a variety of cancer risks, and the International Agency for Research on Cancer (IARC) Working Group incorporated PM into human carcinogens in 2013 (Loomis et al. 2013). PM2.5 exposure can cause oxidative damage to DNA and increase the expression level of oxidation markers such as 8-hydroxy-deoxyguanosine (8-OHdG) and nuclear 7, 8-Dihydro-8-Oxo-2′-deoxyguanosine (8-oxo-DG) (Soberanes et al. 2012; Vattanasit et al. 2014). Cellular responses include release of inflammatory mediators, activation of transcription factors, kinase cascades, etc. ultimately lead to cell apoptosis or damage, which may be one of the potential mechanisms of PM on carcinogenesis (Ghio et al. 2012). In the past decades, accumulating epidemiological studies have demonstrated that PM exposure increases lung cancer incidence and mortality (Guo et al. 2016; Pun et al. 2017; Raaschou-Nielsen et al. 2013, 2016; Villeneuve et al. 2015), as well as other diseases (e.g., gastric cancer, dermatomyositis, heart failure (Shah et al. 2013; Weinmayr et al. 2018; Zantos et al. 1994)). It has been found that individuals living in urban areas are at higher risk of breast cancer and have higher PM2.5 exposure (Brody et al. 2009). Mammograms show extremely and heterogeneously dense breasts in women exposed to high PM2.5, which is an independent risk factor for breast cancer that has been extensively studied (Yaghjyan et al. 2017). In addition, PM has the effect of increasing the number of DNA strand breaks and reducing estrogen activity in MCF-7 and T47D-KBluc human breast cancer cells (Chen et al. 2013). The associations between breast cancer and PM10 (< 10 μm in aerodynamic diameter) or PM2.5 (< 2.5 μm in aerodynamic diameter) exposure have been explored; however, the conclusions are still inconsistent (Datzmann et al. 2018; Hart et al. 2016; Hu et al. 2013; Reding et al. 2015). For example, Hu et al 2013 found that PM2.5 and PM10 was significantly associated with breast cancer mortality. However, Hart et al 2016 did not observe the similar relationship between PM2.5, PM10 and breast cancer risk.
Even though there are no animal studies on PM exposure and breast cancer risk, some scholars have conducted related cell line studies and found that hydroxylated polycyclic aromatic hydrocarbons (hydroxy-PAHs) contained in PM can interact with estrogen receptors, which is one of the possible mechanisms that PM is associated with breast cancer risk (Wenger et al. 2009). To gain a more comprehensive understanding of PM and breast cancer risk, and provide relevant evidence for future public health issues, we conducted this meta-analysis to investigate the association between incidence and mortality of breast cancer and PM, mainly for coarse particles (PM10) and fine particles (PM2.5).
Methods
Literature search
We manually retrieved PubMed and Web of Science databases using two sets of keywords in the title or abstract: (1) “air pollution”, “particulate matter”; (2) “breast neoplasms”, “breast tumors”, “breast cancer”, “breast carcinomas”, and the language of results were limited to English. Comprehensive search criteria and procedures are listed in Supplement A. Besides, we additionally identified references of eligible studies and relevant reviews to check possible articles. We have restricted the literature to human studies published before March 8, 2020.
Inclusion and exclusion criteria
Studies evaluating the association between breast cancer incidence, mortality and PM exposure were incorporated into this systematic review. The included literature must provide quantitative estimates of PM2.5 or PM10 exposure and breast cancer incidence or mortality, and reported odds ratio (OR) or hazard ratio (HR) or relative risk (RR) with a 95% confidence interval (CI). Literature that reported the association between breast cancer risk and other contaminants instead of PM were excluded. Furthermore, no sufficient data or the data provided cannot be converted to PM exposure standardized increment (per 10 μg/m3) were excluded.
Regarding multiple publications containing overlapping study populations, we selected the publication with the longest follow-up years and the largest number of cases. Review articles were excluded. We conducted initial screening by browsing the title and abstract of retrieved articles, followed by full-text reading for eligibility, with the reasons for exclusion recorded.
Data extraction
The following data from eligible studies were extracted: country, the first author, publication year, the number of events and participants, follow-up years, mean age or range of age, pollutants (PM2.5 and PM10), outcome (incidence or mortality), adjusted risk estimates ([RR] or [HR]) and their 95% Cl, study type, study source, PMID, exposure assessment method, exposure distribution, adjusted risk factors. If the information above was not available, we contacted the author for further information in the original study. To ensure the accuracy of the derived data, the entire process was performed independently by two authors (Qing Guo and Xi Wang).
Quality assessment
The included cohort studies and case–control studies were evaluated for methodological quality by Newcastle–Ottawa scale (NOS), a nine-point scoring system for meta-analysis (Stang 2010) (Supplement B), which is comprised of three segments: selection, comparability, and outcome. High-quality studies have scores of 7–9, medium-quality studies have 4–6, and low-quality studies have scores of 4 or less (Wang et al. 2019; Xiong et al. 2019).
Statistical analyses
The HRs in the cohort studies were approximated to RRs, and unified risk estimates in this meta-analysis were reported as RRs. A generalized linear model was applied to examine the relationship between PM exposure and breast cancer risk (Liao et al. 2011; Pope et al. 2011; Yin et al. 2017). To convert all study estimates into standardized increments of PM exposure (per 10 μg/m3), we used the following formula to recalculate risk estimates for each study (Shah et al. 2013):
where the RR was indicated as a continuous measure of interquartile range, the increment in IQR was used instead (Kim et al. 2018). The random-effects model was employed to combine RRs and 95% CI to allow between-study and within-study heterogeneity contribute to the variance (Borenstein et al. 2010; Hamra et al. 2014). We used I2 values (Low: 25%; moderate: 50%; high: 75%) and Q test (statistically significant when P value < 0.1) to evaluate the heterogeneity (Higgins et al. 2003). Further, we performed subgroup analyses based on geographic location, country development, publication year, and follow-up time, respectively. To avoid the potential publication bias, Egger’s tests were created, with the two-sided P value < 0.05. Besides, we provided forest and funnel plots to visually present the impact of a single study on the overall results, and performed trim and fill analyses in case of asymmetrical funnel plots. All statistical analyses in this systematic review were performed by Stata software version 12.0.
Results
Literature selection
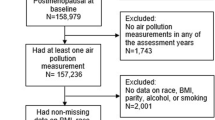
A total of 1787 articles (105 from PubMed, 1667 from Web of Science and 15 from reference lists) were identified. After excluding the duplicates, titles and abstracts of 1,682 studies were reviewed. Screening out the irrelevant researches, we inspected the full-text of 35 possible studies for the eligibility subsequently, of which 20 studies were excluded for some reason: (1) fifteen studies have no correlation with this systematic review; (2) there were three reviews; (3) one study provided relevant data but could not be converted into valid information. Ancona et al. (2015) conducted research on PM10 from incinerators and breast cancer risk. The exposure level of PM10 was quite low (0.027 n/m3 between the 95th and 5th percentiles), and the study found no association between PM10 and breast cancer mortality (HR = 0.97; 95% CI 0.71–1.33). When this data was standardized using the corresponding formula, the estimate was 0 (95% CI 0–\(\infty \)). (4) Tagliabue et al (2016)’s target population was a group of women who had been diagnosed with breast cancer before the study begins. Based on this, the relationship between PM2.5 exposure and breast cancer mortality was studied. This is inconsistent with the inclusion criteria, and its research data will lead to a positive result of the combined estimates in this systematic review. The screening process was shown in Supplementary Fig. 1. Finally, 15 articles [12 cohort studies (Andersen et al. 2017a; Andersen et al. 2017b; Bai et al. 2019; Cheng et al. 2019; Datzmann et al. 2018; DuPre et al. 2019; Hart et al. 2016; Reding et al. 2015; To et al. 2015; Turner et al. 2017; White et al. 2019; Wong et al. 2016), 2 case–control studies (Hu et al. 2013; Hung et al. 2011) and 1 cross-sectional study (Iwai et al. 2005)] covering 6,265,721 participants were included in the meta-analysis.
Overall meta-estimates
The characteristics of the included 15 articles are summarized in Table 1: 9 of the included studies were conducted in North America, 3 in Europe, and 3 in Asia. The follow-up duration for each study was longer than 4 years. Detailed information on PM exposure measurement of the included literature in Supplementary Table 4. The estimated effect values for a single study are shown in Supplementary Fig. 2 and Supplementary Fig. 3, and the pooled results are grouped by the outcome (incidence or mortality) related to PM2.5 and PM10. All estimates represent changes in breast cancer incidence and mortality associated with per 10 μg/m3 increment exposure in PM.
In this meta-analysis, PM2.5 was related to the incidence of breast cancer (RR = 1.09; 95% CI 1.02–1.16; I2 = 17.4%; PQ-test = 0.158). No significant association between breast cancer mortality and PM2.5 was observed (1.20; 0.92–1.48; 52.5%; 0.078). The estimates of incidence and mortality for breast cancer with PM10 were 1.03 (0.98–1.09; 65.1%; 0.009) and 1.07 (0.93–1.20; 56.4%; 0.130), respectively.
We analyzed the relationship between PM2.5 and the incidence and mortality of breast cancer (Table 2). The meta-estimates for PM2.5 and breast cancer incidence by follow-up period (< 11 years and ≥ 11 years) were 1.11 (95% CI 0.97–1.25), 1.01 (0.94–1.08), respectively. By continent, the meta-estimates for North America and Europe were 1.03 (0.96–1.11) and 0.99 (0.75–1.23), respectively. When the meta-analyses were performed by the publication time (before 2017 and after 2017), the meta-estimates were 1.05 (0.84–1.25) and 1.02 (0.99–1.05), respectively. The relationship between PM2.5 and breast cancer mortality was also conducted. With regard to follow-up period (< 11 years and ≥ 11 years), the meta-estimates were 1.42 (0.70–2.13), 1.06 (0.94–1.17), respectively. And for the continent, the meta-estimates were 1.06 (0.94–1.18) for North America and 1.11 (1.00–1.21) for Asia. The meta-estimates were 1.10(1.03–1.17) for developed country and 1.36(0.65–2.07) for developing country. The significant relationship between PM2.5 exposure and breast cancer mortality was found in the subgroup for the publication time before 2017 (1.11; 1.00–1.22), and the meta-estimates showed 1.06 (0.94–1.17) for studies published after 2017.
As shown in Table 3, the meta-estimates of PM10 and breast cancer incidence were 1.05 (0.95–1.15) for follow-up period (< 11 years) and 1.02 (0.97–1.08) (≥ 11 years). When analyzed by geographic location (North America and Europe), the meta-estimates were 0.98 (0.97–1.00), 1.15 (1.06–1.25), respectively. And for the publication time, the meta-estimates were 0.98 (0.97–1.00) for the group of before 2017 and 1.08 (1.00–1.15) for the group of after 2017. There are 2 studies included that explored the association between PM10 and breast cancer mortality. And the meta-estimates were 1.13 (1.02–1.25) for follow-up period (< 11 years) and 0.99 (0.86–1.14) (≥ 11 years), same as the meta-estimates for publication time (before 2017 and after 2017).
Sensitivity analyses
We conducted sensitivity analyses of PM (PM2.5, PM10) exposure and breast cancer incidence and mortality. After omitting the study by Datzmann et al. (2018), it indicated that the heterogeneity changed from P = 0.009, I2 = 65.1% to P = 0.547, I2 = 0.0% in the study of PM10 and breast cancer incidence. This study is a large sample semi-individual cohort study, which may be the explanation for heterogeneity. After deleting the study by Wong et al. (2016) in the analysis of PM2.5 and breast cancer mortality, the P value increased from 0.158 to 0.537, and I2 changed from 37.2% to 0.0%. HRs were used in the study by Wong et al. (2016); however, we utilized RRs in this meta-analysis (He et al. 2017).
Publication bias
Asymmetry was found in the funnel plots (Supplementary Fig. 4, (b), (c)) in the preliminary visual judgment of publication bias. Therefore, Egger’s tests were conducted to provide more specific information in the analysis of breast cancer incidence and mortality with PM (PM2.5, PM10), and we did not find publication bias. In the analysis of PM2.5 exposure and breast cancer incidence and mortality, Egger’s tests showed P = 0.407, P = 0.120, respectively. With regard to the association between PM10 exposure and breast cancer incidence, the P value in Egger’s tests was 0.063. No publication bias of the relationship between PM10 and breast cancer mortality was performed owing to the limitation of the number of relevant studies (n = 2).
Discussion
The meta-analysis included 15 studies, twelve of which were cohort studies, two were case–control studies and one was a cross-sectional study, covering populations in 10 countries. The results suggest that PM2.5 exposure is related to breast cancer mortality. No association of PM2.5 and PM10 with the increase incidence of breast cancer was found. It should be pointed out that Hung et al. studied the relationship between PAH and breast cancer mortality using PM2.5 as an indicator, which could make the relationship between breast cancer and PM2.5 exposure more positive.
In the subgroup analyses, when was stratified by follow-up period, geographic location, country development, and publication year, most of the results were similar. Regarding the breast cancer risk associated with PM2.5 exposure, it showed that the meta-estimates of the Asian population or developing countries were higher than that of the North American population or developed countries. In terms of the relationship between PM10 and breast cancer risk, the meta-estimates for breast cancer incidence in the European population were significantly higher than those in North America. Moreover, compared with studies published after 2017, studies published before 2017 found a lower correlation between PM10 exposure and breast cancer incidence, which is different from the findings of PM2.5 mentioned above.
According to the difference of aerodynamic diameter, PM contains ultrafine particles (PM0.1), fine particles (PM2.5), and coarse particles (PM10), in which PM2.5 and PM10 are widely concerned in relation to public health (Pope et al. 2011). However, PM2.5 and PM0.1 cause more damage, probably because they are more easy to pass through the barrier of the body and eventually penetrate to the alveoli (Valavanidis et al. 2008). Both long-term exposure and short-term exposure to PM can have adverse effects on human beings, which has developed into a serious public health problem (Brunekreef and Holgate 2002).
The reason for a higher cancer risk caused by exposure to PM has not been fully elucidated. Possible mechanisms are as follows: (1) PM entering the body induces the production of reactive oxygen species, which causes oxidative stress reaction and ultimately leads to DNA damage (Crobeddu et al. 2017; Risom et al. 2005). In addition, studies have found that PM2.5 is associated with lipid peroxidation, especially in newborns, which may also be a potential reason for PM to threaten human health (Ambroz et al. 2016). (2) Another possible mechanism involves an inflammatory response. Reactive oxygen intermediates can cause inflammation by activating the expression of TNF-α, IL-1α(Rahman and MacNee 1998). It has been found that PM can cause an increase in the expression level of C-reactive protein (CRP) in the body and can be used as an indicator of inflammation (Donaldson et al. 2001). In a cohort study of older adults, after more than 12 weeks of measurement, it was found that interleukin-6 (IL-6) was associated with exposure to traffic-related contaminants (Zhang et al. 2016a). Changes in the levels of these inflammation-related substances are indicative of the possibility of inflammation compared to normal bodies. (3) The physical properties and chemical composition of PM2.5 related to carcinogenesis are unfavorable, and will change with season and geographical location (Bell et al. 2007). Studies have found that PM2.5 can carry heavy metals (vanadium, nickel, etc.), organics, black carbon, nitrates, polycyclic aromatic hydrocarbons (PAH) and other substances (Mannucci et al. 2019; White et al. 2019). Prolonged exposure to PAH increases the risk of breast cancer in women (Lee et al. 2019; Stults and Wei 2018). PAH with lipophilic properties can be stored in the adipose tissue of the breast and combine with DNA to form the PAH-DNA adduct, which changes the structure and function of DNA (Agudo et al. 2017; Morris and Seifter 1992; Shen et al. 2017; Zhang et al. 2019). Another possible mechanism has been found in animal experiments, PAH may enhance its carcinogenicity and cytotoxicity by affecting the estrogen metabolic pathway (Kummer et al. 2008; Zhang et al. 2016b).
The literature included in this meta-analysis has identified breast cancer risk factors as potential confounders. Among the adjusted models for breast cancer morbidity or mortality outcomes, we chose the model that takes into account the most comprehensive risk factors. Detailed information of risk factors that have been adjusted in the included studies are shown in Supplementary Table 5. A meta-analysis based on retrospective and prospective studies showed that both active and passive smoking increased breast cancer risk (Macacu et al. 2015). Female estrogen and progesterone (ER and PR) receptors have also been found to be associated with breast cancer risk. In a cohort study of Japan, long-term smoking patients with ER+ or PR+ before menopause increased the mortality of breast cancer (Kakugawa et al. 2015). Studies have found that pesticide exposure is related to breast cancer risk, which may be associated with some of the chemicals carried by PM (Engel et al. 2005). And as mentioned above, PM is easily present in adipose tissue. We therefore speculate that obese women are at higher risk of breast cancer if the other conditions are the same or similar (Niehoff et al. 2017). Unhealthy behaviors such as motor vehicle pollutant exposure, smoking, potato consumption during breastfeeding may also lead to an increase in heavy metals (Pb, Cd) of breast milk, therefore, it is particularly important to monitor the pollutant exposure and develop healthy lifestyles (Garcia-Esquinas et al. 2011; Rebelo and Caldas 2016).
The main advantages of this systematic review can be divided into three aspects. First, we set the incidence and mortality rates as different outcomes. We analyzed PM2.5 and PM10, which are currently recognized as having a greater impact on human health. With the progression of the disease stage, the risk of breast cancer death will increase significantly. However, early screening can reduce breast cancer mortality (Tagliabue et al. 2016). A prospective study involving women from more than 10 countries in Europe found that alcohol intake increased breast cancer risk and was positively correlated with drinking time (Romieu et al. 2015). A healthy lifestyle index score (HLIS) is negatively correlated with breast cancer, which indicates that the lifestyle of postmenopausal women is a likely factor influencing breast cancer risk (McKenzie et al. 2015). In this study, we found the association between PM2.5 exposure and breast cancer mortality, but not in breast cancer incidence. PM itself or its conjugates can produce molecular and cellular damage to breast tissues, but there are no relevant studies to clarify the molecular biological mechanism of PM exposure not related to breast cancer incidence. We believe that there are many reasons for the increase in breast cancer mortality. In addition to the biological role of PM, it is also related to the basic physiological state of the exposed population. This may be an explanation for the difference in results, and more future research is needed to confirm this view.
Second, we did not make restrictions on the publication time and geographic location of the literature, thus, we can expansively assess the incidence and mortality of breast cancer caused by PM exposure without time and space constraints. Third, the previous review qualitatively discussed the relationship between PM and breast cancer risk but did not yield quantitative results (White et al. 2018). However, we integrated data from existing relevant literature and used random effects models to estimate RR of cancer incidence/mortality and PM. Therefore, this study presents more exhaustive and effective information to date.
There are still some limitations of this meta-analysis that need to be noted: (1) Regarding breast cancer risk and PM exposure, although there is already a certain amount of research, more data is needed. Based on pre-defined inclusion/exclusion principles, this article contains 15 studies, but more robust statistical results require the support of a large amount of information. (2) This study conducted subgroup analyses, but due to the limitations of the number of articles and the content of these researches, it can only be restricted to the basic information level of the literature, and there are no more in-depth analyses of breast cancer risk. (3) The study does not distinguish between indoor pollution and outdoor pollution.
Conclusions
This study identified an association between PM2.5 exposure and breast cancer mortality. The atmospheric PM can come from multiple sources, and traffic-related exhaust emissions cannot be ignored. In the process of development, modern society needs to be alert to the human health risks caused by PM. Further, more large-scale studies and biological studies should be conducted to explore ways PM contributes to—or more likely is a surrogate of true risk factors for—breast cancer mortality.
Availability of data and materials
The datasets created and analyzed during the current study are available from the corresponding author by reasonable request.
Abbreviations
- N/A:
-
Not applicable
- RR:
-
Relative risk
- CI:
-
Confidence interval
- SD:
-
Standard deviation
- OR:
-
Odds ratio
- HR:
-
Hazard ratio
- NOS:
-
Newcastle–Ottawa scale
- CRP:
-
C-reactive protein
- IL-6:
-
Interleukin-6
- IQR:
-
Interquartile range
- ER:
-
Estrogen receptor
References
Agudo A et al (2017) Aromatic DNA adducts and breast cancer risk: a case-cohort study within the EPIC-Spain. Carcinogenesis 38:691–698. https://doi.org/10.1093/carcin/bgx047
Ambroz A et al (2016) Impact of air pollution on oxidative DNA damage and lipid peroxidation in mothers and their newborns. Int J Hyg Environ Health 219:545–556. https://doi.org/10.1016/j.ijheh.2016.05.010
Ancona C et al (2015) Mortality and morbidity in a population exposed to multiple sources of air pollution: a retrospective cohort study using air dispersion models. Environ Res 137:467–474. https://doi.org/10.1016/j.envres.2014.10.036
Andersen ZJ et al (2017) Long-term exposure to fine particulate matter and breast cancer incidence in the Danish nurse cohort study. Cancer Epidemiol Biomarkers Prev 26:428–430. https://doi.org/10.1158/1055-9965.Epi-16-0578
Andersen ZJ et al. (2017b) Long-Term Exposure to Ambient Air Pollution and Incidence of Postmenopausal Breast Cancer in 15 European Cohorts within the ESCAPE Project Environ Health Perspect 125:107005. https://doi.org/10.1289/ehp1742
Bai L et al (2019) Exposure to ambient air pollution and the incidence of lung cancer and breast cancer in the Ontario Population Health and Environment Cohort. Int J Cancer. https://doi.org/10.1002/ijc.32575
Bell ML, Dominici F, Ebisu K, Zeger SL, Samet JM (2007) Spatial and temporal variation in PM(2.5) chemical composition in the United States for health effects studies. Environ Health Perspect 115:989–995. https://doi.org/10.1289/ehp.9621
Borenstein M, Hedges LV, Higgins JP, Rothstein HR (2010) A basic introduction to fixed-effect and random-effects models for meta-analysis Res Synth. Methods 1:97–111. https://doi.org/10.1002/jrsm.12
Brody JG, Morello-Frosch R, Zota A, Brown P, Perez C, Rudel RA (2009) Linking exposure assessment science with policy objectives for environmental justice and breast cancer advocacy: the northern California household exposure study. Am J Public Health 99(Suppl 3):S600–609. https://doi.org/10.2105/ajph.2008.149088
Brunekreef B, Holgate ST (2002) Air pollution and health. Lancet 360:1233–1242. https://doi.org/10.1016/S0140-6736(02)11274-8
Chen ST, Lin CC, Liu YS, Lin C, Hung PT, Jao CW, Lin PH (2013) Airborne particulate collected from central Taiwan induces DNA strand breaks, Poly(ADP-ribose) polymerase-1 activation, and estrogen-disrupting activity in human breast carcinoma cell lines. J Environ Sci Health A Tox Hazard Subst Environ Eng 48:173–181. https://doi.org/10.1080/10934529.2012.717809
Cheng I et al (2019) Association between ambient air pollution and breast cancer risk: the multiethnic cohort study. Int J Cancer. https://doi.org/10.1002/ijc.32308
Crobeddu B, Aragao-Santiago L, Bui LC, Boland S, Baeza Squiban A (2017) Oxidative potential of particulate matter 2.5 as predictive indicator of cellular stress. Environ Pollut 230:125–133. https://doi.org/10.1016/j.envpol.2017.06.051
Datzmann T, Markevych I, Trautmann F, Heinrich J, Schmitt J, Tesch F (2018) Outdoor air pollution, green space, and cancer incidence in Saxony: a semi-individual cohort study. BMC Public Health 18:715. https://doi.org/10.1186/s12889-018-5615-2
Donaldson K, Stone V, Seaton A, MacNee W (2001) Ambient particle inhalation and the cardiovascular system: potential mechanisms 109:523–527. doi:10.1289/ehp.01109s4523
DuPre NC et al (2019) Particulate matter and traffic-related exposures in relation to breast cancer survival. Cancer Epidemiol Biomarkers Prev 28:751–759. https://doi.org/10.1158/1055-9965.Epi-18-0803
Engel LS et al (2005) Pesticide use and breast cancer risk among farmers' wives in the agricultural health study. Am J Epidemiol 161:121–135. https://doi.org/10.1093/aje/kwi022
Garcia-Esquinas E et al (2011) Mercury, lead and cadmium in human milk in relation to diet, lifestyle habits and sociodemographic variables in Madrid (Spain). Chemosphere 85:268–276. https://doi.org/10.1016/j.chemosphere.2011.05.029
Ghio AJ, Carraway MS, Madden MC (2012) Composition of air pollution particles and oxidative stress in cells, tissues, and living systems. J Toxicol Environ Health B Crit Rev 15:1–21. https://doi.org/10.1080/10937404.2012.632359
Guo Y et al (2016) The association between lung cancer incidence and ambient air pollution in China: A spatiotemporal analysis. Environ Res 144:60–65. https://doi.org/10.1016/j.envres.2015.11.004
Hamra GB et al (2014) Outdoor particulate matter exposure and lung cancer: a systematic review and meta-analysis. Environ Health Perspect 122:906–911. https://doi.org/10.1289/ehp.1408092
Hart JE, Bertrand KA, DuPre N, James P, Vieira VM, Tamimi RM, Laden F (2016) Long-term particulate matter exposures during adulthood and risk of breast cancer incidence in the Nurses' health study II prospective cohort. Cancer Epidemiol Biomark Prev 25:1274–1276. https://doi.org/10.1158/1055-9965.Epi-16-0246
He D, Wu S, Zhao H, Qiu H, Fu Y, Li X, He Y (2017) Association between particulate matter 25 and diabetes mellitus: a meta-analysis of cohort studies. J Diabetes Investig 8:687–696. https://doi.org/10.1111/jdi.12631
Higgins JPT, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. JBMJ 327:557–560. https://doi.org/10.1136/bmj.327.7414.557
Hu H, Dailey AB, Kan H, Xu X (2013) The effect of atmospheric particulate matter on survival of breast cancer among US females. Breast Cancer Res Treat 139:217–226. https://doi.org/10.1007/s10549-013-2527-9
Hung L-J, Tsai S-S, Chen P-S, Yang Y-H, Liou s-h, Wu T-N, Yang C-Y (2011) Traffic Air Pollution and Risk of Death from Breast Cancer in Taiwan: Fine Particulate Matter (PM 2.5 ) as a Proxy Marker Aerosol Air Qual Res 12
Iwai K, Mizuno S, Miyasaka Y, Mori T (2005) Correlation between suspended particles in the environmental air and causes of disease among inhabitants: cross-sectional studies using the vital statistics and air pollution data in Japan. Environ Res 99:106–117. https://doi.org/10.1016/j.envres.2004.11.004
Kakugawa Y, Kawai M, Nishino Y, Fukamachi K, Ishida T, Ohuchi N, Minami Y (2015) Smoking and survival after breast cancer diagnosis in Japanese women: a prospective cohort study. Cancer Sci 106:1066–1074. https://doi.org/10.1111/cas.12716
Kim HB, Shim JY, Park B, Lee YJ (2018) Long-term exposure to air pollutants and cancer mortality: a meta-analysis of cohort studies. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph15112608
Kummer V, Maskova J, Zraly Z, Neca J, Simeckova P, Vondracek J, Machala M (2008) Estrogenic activity of environmental polycyclic aromatic hydrocarbons in uterus of immature Wistar rats. Toxicol Lett 180:212–221. https://doi.org/10.1016/j.toxlet.2008.06.862
Lee DG, Burstyn I, Lai AS, Grundy A, Friesen MC, Aronson KJ, Spinelli JJ (2019) Women's occupational exposure to polycyclic aromatic hydrocarbons and risk of breast cancer. Occup Environ Med 76:22–29. https://doi.org/10.1136/oemed-2018-105261
Liao CM et al (2011) Lung cancer risk in relation to traffic-related nano/ultrafine particle-bound PAHs exposure: a preliminary probabilistic assessment. J Hazard Mater 190:150–158. https://doi.org/10.1016/j.jhazmat.2011.03.017
Loomis D et al (2013) The carcinogenicity of outdoor air pollution. Lancet Oncol 14:1262–1263
Macacu A, Autier P, Boniol M, Boyle P (2015) Active and passive smoking and risk of breast cancer: a meta-analysis. Breast Cancer Res Treat 154:213–224. https://doi.org/10.1007/s10549-015-3628-4
Mannucci PM, Harari S, Franchini M (2019) Novel evidence for a greater burden of ambient air pollution on cardiovascular disease. Haematologica 104:2349–2357. https://doi.org/10.3324/haematol.2019.225086
McKenzie F et al (2015) Healthy lifestyle and risk of breast cancer among postmenopausal women in the European Prospective Investigation into Cancer and Nutrition cohort study. Int J Cancer 136:2640–2648. https://doi.org/10.1002/ijc.29315
Morris JJ, Seifter E (1992) The role of aromatic hydrocarbons in the genesis of breast cancer. Med Hypotheses 38:177–184. https://doi.org/10.1016/0306-9877(92)90090-y
Niehoff N et al (2017) Polycyclic aromatic hydrocarbons and postmenopausal breast cancer: an evaluation of effect measure modification by body mass index and weight change. Environ Res 152:17–25. https://doi.org/10.1016/j.envres.2016.09.022
Pope CA 3rd et al (2011) Lung cancer and cardiovascular disease mortality associated with ambient air pollution and cigarette smoke: shape of the exposure-response relationships. Environ Health Perspect 119:1616–1621. https://doi.org/10.1289/ehp.1103639
Pun VC, Kazemiparkouhi F, Manjourides J, Suh HH (2017) Long-term PM2.5 exposure and respiratory, cancer, and cardiovascular mortality in older US adults. Am J Epidemiol 186:961–969. https://doi.org/10.1093/aje/kwx166
Raaschou-Nielsen O et al (2013) Air pollution and lung cancer incidence in 17 European cohorts: prospective analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). Lancet Oncol 14:813–822. https://doi.org/10.1016/s1470-2045(13)70279-1
Raaschou-Nielsen O et al (2016) Particulate matter air pollution components and risk for lung cancer. Environ Int 87:66–73. https://doi.org/10.1016/j.envint.2015.11.007
Rahman I, MacNee W (1998) Role of transcription factors in inflammatory lung diseases. J Thorax 53:601–612. https://doi.org/10.1136/thx.53.7.601
Rebelo FM, Caldas ED (2016) Arsenic, lead, mercury and cadmium: Toxicity, levels in breast milk and the risks for breastfed infants. Environ Res 151:671–688. https://doi.org/10.1016/j.envres.2016.08.027
Reding KW et al (2015) Breast cancer risk in relation to ambient air pollution exposure at residences in the sister study cohort. Cancer Epidemiol Biomarkers Prev 24:1907–1909. https://doi.org/10.1158/1055-9965.Epi-15-0787
Risom L, Moller P, Loft S (2005) Oxidative stress-induced DNA damage by particulate air pollution. Mutat Res 592:119–137. https://doi.org/10.1016/j.mrfmmm.2005.06.012
Romieu I et al (2015) Alcohol intake and breast cancer in the European prospective investigation into cancer and nutrition. Int J Cancer 137:1921–1930. https://doi.org/10.1002/ijc.29469
Shah AS et al (2013) Global association of air pollution and heart failure: a systematic review and meta-analysis. Lancet 382:1039–1048. https://doi.org/10.1016/s0140-6736(13)60898-3
Shen J, Liao Y, Hopper JL, Goldberg M, Santella RM, Terry MB (2017) Dependence of cancer risk from environmental exposures on underlying genetic susceptibility: an illustration with polycyclic aromatic hydrocarbons and breast cancer. Br J Cancer 116:1229–1233. https://doi.org/10.1038/bjc.2017.81
Siegel RL, Miller KD, Jemal A (2019) Cancer statistics 2019(69):7–34. https://doi.org/10.3322/caac.21551
Soberanes S et al (2012) Particulate matter Air Pollution induces hypermethylation of the p16 promoter Via a mitochondrial ROS-JNK-DNMT1 pathway. Sci Rep 2:275. https://doi.org/10.1038/srep00275
Stang A (2010) Critical evaluation of the Newcastle–Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 25:603–605. https://doi.org/10.1007/s10654-010-9491-z
Stults WP, Wei Y (2018) Ambient air emissions of polycyclic aromatic hydrocarbons and female breast cancer incidence in US. Med Oncol 35:88. https://doi.org/10.1007/s12032-018-1150-3
Tagliabue G et al (2016) Atmospheric fine particulate matter and breast cancer mortality: a population-based cohort study. BMJ open 6:e012580. https://doi.org/10.1136/bmjopen-2016-012580
To T et al (2015) Chronic disease prevalence in women and air pollution—a 30-year longitudinal cohort study. Environ Int 80:26–32. https://doi.org/10.1016/j.envint.2015.03.017
Turner MC et al (2017) Ambient air pollution and cancer mortality in the cancer prevention study II. Environ Health Perspect 125:087013. https://doi.org/10.1289/ehp1249
Valavanidis A, Fiotakis K, Vlachogianni T (2008) Airborne particulate matter and human health: toxicological assessment and importance of size and composition of particles for oxidative damage and carcinogenic mechanisms. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev 26:339–362. https://doi.org/10.1080/10590500802494538
Vattanasit U, Navasumrit P, Khadka MB, Kanitwithayanun J, Promvijit J, Autrup H, Ruchirawat M (2014) Oxidative DNA damage and inflammatory responses in cultured human cells and in humans exposed to traffic-related particles. Int J Hyg Environ Health 217:23–33. https://doi.org/10.1016/j.ijheh.2013.03.002
Villeneuve PJ et al (2015) Long-term exposure to fine particulate matter air pollution and mortality among Canadian women. Epidemiology 26:536–545. https://doi.org/10.1097/ede.0000000000000294
Wang JH, Ma HH, Chou TA, Tsai SW, Chen CF, Wu PK, Chen WM (2019) Outcomes following total elbow arthroplasty for rheumatoid arthritis versus post-traumatic conditions: a systematic review and meta-analysis. Bone Joint J 101:1489–1497. https://doi.org/10.1302/0301-620x.101b12.Bjj-2019-0799.R1
Weinmayr G et al (2018) Particulate matter air pollution components and incidence of cancers of the stomach and the upper aerodigestive tract in the European Study of Cohorts of Air Pollution Effects (ESCAPE). Environ Int 120:163–171. https://doi.org/10.1016/j.envint.2018.07.030
Wenger D, Gerecke AC, Heeb NV, Schmid P, Hueglin C, Naegeli H, Zenobi R (2009) vitro estrogenicity of ambient particulate matter: contribution of hydroxylated polycyclic aromatic hydrocarbons. J Appl Toxicol 29:223–232. https://doi.org/10.1002/jat.1400
White AJ, Bradshaw PT, Hamra GB (2018) Air pollution and Breast Cancer: a review. Curr Epidemiol Rep 5:92–100. https://doi.org/10.1007/s40471-018-0143-2
White AJ, Keller JP, Zhao S, Carroll R, Kaufman JD, Sandler DP (2019) Air pollution, clustering of particulate matter components, and breast cancer in the sister study: a U.S.-wide cohort. Environ Health Perspect 127:107002. https://doi.org/10.1289/ehp5131
Wong CM et al (2016) Cancer mortality risks from long-term exposure to ambient fine particle. Cancer Epidemiol Biomarkers Prev 25:839–845. https://doi.org/10.1158/1055-9965.Epi-15-0626
Xiong H et al (2019) A prognostic role for non-thyroidal illness syndrome in chronic renal failure:a systematic review and meta-analysis. Int J Surg 70:44–52. https://doi.org/10.1016/j.ijsu.2019.08.019
Yaghjyan L, Arao R, Brokamp C, O'Meara ES, Sprague BL, Ghita G, Ryan P (2017) Association between air pollution and mammographic breast density in the Breast Cancer Surveilance Consortium. Breast Cancer Res 19:36. https://doi.org/10.1186/s13058-017-0828-3
Yin P et al (2017) Long-term fine particulate matter exposure and nonaccidental and cause-specific mortality in a large national cohort of Chinese men. Environ Health Perspect 125:117002. https://doi.org/10.1289/ehp1673
Zantos D, Zhang Y, Felson D (1994) The overall and temporal association of cancer with polymyositis and dermatomyositis. J Rheumatol 21:1855–1859
Zhang X et al (2016a) Associations of oxidative stress and inflammatory biomarkers with chemically-characterized air pollutant exposures in an elderly cohort. Environ Res 150:306–319. https://doi.org/10.1016/j.envres.2016.06.019
Zhang Y, Dong S, Wang H, Tao S, Kiyama R (2016b) Biological impact of environmental polycyclic aromatic hydrocarbons (ePAHs) as endocrine disruptors. Environ Pollut 213:809–824. https://doi.org/10.1016/j.envpol.2016.03.050
Zhang Z, Yan W, Chen Q, Zhou N, Xu Y (2019) The relationship between exposure to particulate matter and breast cancer incidence and mortality: a meta-analysis. Medicine (Baltimore) 98:e18349. https://doi.org/10.1097/md.0000000000018349
Acknowledgements
We should thank Dr. Junyi Xin for the support of data analysis and revising the article.
Funding
This study was supported in part by the National Key R&D Program of China (Grants 2017YFC0211600, 2017YFC0211605), Collaborative Innovation Center for Cancer Personalized Medicine, and Priority Academic Program Development of Jiangsu Higher Education Institutions (Public Health and Preventive Medicine).
Author information
Authors and Affiliations
Contributions
QG and XW conducted the literature search and data extraction. QG edited the manuscript and generated the figures and tables, which were revised by HC. HC provided overall supervision. All authors were involved in writing the manuscript and agreed on the final version of the submitted manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.


Supplementary figure 2. Estimates of breast cancer risk in relation to a 10 μg/m3 increment exposure in PM
2.5. CI, confidence interval; RR, relative risk (JPG 87 kb)

Supplementary figure 3. Estimates of breast cancer risk in relation to a 10 μg/m3 increment exposure in PM
10. CI, confidence interval; RR, relative risk (JPG 76 kb)

Supplementary figure 4. Funnel plots on PM exposure and breast cancer risk with pseudo 95% confidence limits. (a)PM
2.5 and breast cancer incidence; (b) PM2.5 and breast cancer mortality; (c) PM10 and breast cancer incidence. (JPG 61 kb)
Rights and permissions
About this article

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cite this article
Guo, Q., Wang, X., Gao, Y. et al. Relationship between particulate matter exposure and female breast cancer incidence and mortality: a systematic review and meta-analysis. Int Arch Occup Environ Health 94, 191–201 (2021). https://doi.org/10.1007/s00420-020-01573-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-020-01573-y