
Abstract
Purpose
The incidence of oropharyngeal squamous cell carcinoma continues to rise with the majority of patients receiving definitive or adjunctive radiation. For patients with locoregional recurrence after radiation, optimal treatment involves salvage surgery. The aim of this study is to identify factors that predict survival to ultimately improve patient selection for salvage surgery.
Methods
Retrospective cohort study at an NCI-designated cancer center. We analyzed patients with a history of head and neck radiation who presented with persistent/recurrent or second primary disease requiring salvage oropharyngeal resection from 1998–2017 (n = 120). Patients were stratified into three classes based on time to recurrence and presence of laryngopharyngeal dysfunction. Primary outcomes were 5-year overall survival (OS) and disease specific survival (DSS).
Results
Median OS was 27 months (median follow-up 20 months). Five-year OS was 47% for class I (recurrence > 2 years), 26% for class II (recurrence ≤ 2 years), and 0% for class III (recurrence ≤ 2 years and laryngopharyngeal dysfunction), (p < 0.0001). Five-year DSS showed significant differences between classes (p < 0.0001). On multivariate analysis, class remained predictive of OS (p = 0.04– < 0.001) and DSS (p = 0.04–0.001). Adjuvant radiation after salvage surgery with negative margins showed superior OS (71% vs. 28%, p = 0.01) and DSS (83% vs 37%, p = 0.02) compared to surgery alone and was a significant predictor of improved survival on multivariate analysis (HR 0.1, p = 0.04).
Conclusion
This study identified a subset of patients with oropharyngeal cancer recurrence within two years of initial treatment and with laryngopharyngeal dysfunction who have poor outcomes for salvage surgery.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Oropharyngeal squamous cell carcinoma (OPSCC) previously accounted for a quarter of all head and neck cancers [1] and the incidence has continued to rise over the past three decades [2,3,4]. Despite the improved outcomes among patients with HPV-associated OPSCC, recurrence rates remain between 15 and 36% [5,6,7,8]. Even with the advent of novel transoral surgical options, radiation remains a mainstay of primary and adjuvant treatment for patients with locally advanced OPSCC, and the majority (80%) of patients with primary OPSCC will receive radiation as part of their initial treatment [9, 10].
Salvage surgery is the preferred treatment for select patients with recurrent disease or in those who develop a second primary after radiation [11,12,13,14,15,16,17]. Re-irradiation is a possible treatment modality as well, but is associated with considerable risk and lower salvage rates [17, 18]. Despite improved salvage outcomes in HPV-associated OPSCC locoregional failures, treatment of recurrent OPSCC has high morbidity, suboptimal 5-year OS (24–43%) [12, 19,20,21,22] and a formidable burden and cost [19]. Thus, careful patient selection is becoming increasingly important in treatment planning.
Recent studies have identified prognostic factors among patients undergoing treatment for recurrent OPSCC [18, 23,24,25]. Both time to recurrence and comorbidity status have been consistently recognized as predictors of survival in this setting [17, 18, 20, 23,24,25]. Further, while comorbidity scores such as Charlson comorbidity index (CCI) or Eastern Cooperative Oncology Group (ECOG) performance score have been used to predict prognosis [25], in recurrent head and neck cancer patients, laryngopharyngeal dysfunction, defined as pre-treatment tracheostomy or feeding tube dependence, represents a unique marker of functional status that is often predictive of poor outcomes [18, 23,24,25,26]. A recent study by Ward et al. evaluated patient outcomes stratified by disease-free interval and laryngopharyngeal dysfunction in patients undergoing re-irradiation with significant separation of the survival curves [18]. No analogous analysis has evaluated risk stratification in a salvage surgical cohort.
This study aims to identify factors predictive of poor outcomes in patients undergoing salvage oropharyngeal resection after prior head and neck radiation in order to better inform decision-making for patients and clinicians. We hypothesize that a modified class stratification can improve patient selection for surgery or alternative treatment approaches in the recurrent OPSCC setting.
Methods
Patient population
This study was approved by the University of Michigan IRBMED (HUM00081554). Inclusion criteria were a history of head and neck radiation with subsequent oropharyngeal resection for recurrent/persistent disease or a second primary disease between 1998 and 2017. Patients with a history of laryngectomy were excluded. Clinical and oncologic data including patient age, sex, body mass index (BMI), primary tumor site, primary and recurrent TNM stages, initial treatment, time to recurrence, smoking status, alcohol use, pre-operative tracheostomy and gastrostomy tube (G-tube) use, HPV status, margin status, and adjuvant therapy for recurrent disease were collected by two independent reviewers. Staging was based on American Joint Committee on Cancer (AJCC) 7th edition [27]. HPV status was determined from path reports and clinical documentation. p16 status was used as a proxy for HPV status when available. Overall and disease specific survival time were defined, a priori, as time from salvage surgery to date of death from any cause, or date of death due to disease, respectively. Disease-free survival was determined from date of salvage surgery to date of recurrence (as determined by biopsy if available, or clinical/radiographic evidence) or death of any cause.
Patients were characterized into a modified three class stratification system based on prior studies by Ward et al. [18]. Class I was defined as patients with an initial disease-free interval greater than 2 years, class II was defined as patients with a disease-free interval less than or equal to 2 years without laryngopharyngeal dysfunction (pre-salvage tracheostomy and/or feeding tube dependence), and class III was defined as patients with a disease-free interval less than or equal to 2 years and laryngopharyngeal dysfunction.
Statistical analysis
Overall survival, disease specific survival and disease-free survival were calculated for the total population. Stratification by class and additional clinical variables was performed using Prism 8 (GraphPad Software Inc; San Diego, CA). Comparison of survival outcomes was completed with Cox-log rank comparison. Multivariate analysis was performed using a backward selected Cox regression model. Factors with a p value ≤ 0.1 on KM analysis were included in the model. Cox-log rank and multivariate analyses were performed with SPSS version 26 software (IBM; Armonk, NY).
Results
Clinical and oncologic characteristics
A total of 120 patients were identified and included. The majority of patients in this cohort were men (69%) with a median age of 61 years at the time of treatment (range 31–84 years). The majority, 61%, of the cohort received radiation for primary OPSCC (74/120), 18% (21/120) for primary oral cavity tumors and the remaining 21% (25/120) for other tumors (i.e. parotid, larynx). HPV status was available for 46% (39/84) of oropharyngeal recurrences. All patients underwent oropharyngeal resection for recurrent/persistent disease or second primary tumors with involvement of the oropharynx.
The median duration between initial radiation treatment and surgery for recurrent disease was 20 months (range 2 months–22 years). Fifty-four percent of patients had stage IV recurrent disease at the time of presentation and 30% had clinically evident nodal disease. All patients underwent salvage oropharyngectomy and the median follow-up time was 20 months (range 4 months–14 years). Patient and disease characteristics are delineated in Table 1.
Survival outcomes
At 5 years there were a total of 75 deaths (63%) and 62 recurrences (52%). The 5-year overall survival for the cohort was 31% with a median survival time of 27 months. Five-year disease specific survival was 42% (median survival time 42 months) and 5-year disease-free survival was 25% (median of 16 months). Kaplan–Meier analysis was performed stratifying by the primary tumor site, initial stage (overall and T,N stages), primary neck dissection, recurrent stage (overall and T,N stages), smoking status, alcohol use, body mass index (BMI), margin status, HPV status, and use of adjuvant radiation. Five-year overall survival and or 5-year disease specific survival were found to be significant when stratifying by primary neck dissection vs. no neck dissection (OS: 50%, 95%CI 32–66% vs. 23%, 95%CI 14–34, p = 0.009, DSS: 54%, 95%CI 34–71% vs. 34%, 95%CI 21–48%, p = 0.08), positive vs. negative recurrent nodal disease (OS: 21%, 95%CI 8–37% vs. 36%, 95%CI 25–47%, p = 0.02, DSS: 24%, 95%CI 10–42% vs. 49%, 95%CI 35–36%, p = 0.004), never smoker vs. current or former smoker (OS: 56%, 95%CI 32–75% vs. 25%, 95%CI 16–35%, p = 0.01, DSS: 64%, 95%CI 38–82% vs. 35%, 95%CI 23–47%, p = 0.05), and BMI above vs. below 20 (OS: 39%, 95%CI 28–50% vs. 10%, 95%CI 2–27%, p < 0.001, DSS: 46%, 95%CI 33–58% vs. 22%, 95%CI 5–46%, p = 0.04) as shown in Supplemental Fig 1a–d. Further, patients who underwent adjuvant radiation after salvage surgery with negative margins (n = 10) had significantly improved 5-year overall survival (71%, 95%CI 26–92% vs. 28%, 95%CI 19–38%, p = 0.01) and 5-year disease specific survival (83%, 95%CI 27–97 vs. 37%, 95%CI 26–49, p = 0.02) compared to patients who did not receive adjuvant radiation (n = 106) or who received radiation after salvage surgery with positive margins (n = 2) (Supplemental Fig. 1e). Stratification by HPV status was performed and showed no significant difference in 5 year overall survival (50%, 95%CI 27–70% vs. 34%, 95%CI 13–57%, p = 0.30) or disease specific survival (50%, 95%CI 27–70% vs. 46%, 95%CI 17–71%, p = 0.96) between patients with HPV positive and HPV negative disease (supplemental Fig. 2). Stratification by site of recurrent tumor was also performed and revealed no difference in overall survival rates between oral cavity, oropharynx or other sites (supplemental Fig. 3). The remaining clinical variables (primary stage, alcohol use, and margin status) also did not show significant survival differences.
Patterns of failure
Sixty-two patients developed recurrent disease after salvage surgery. Forty-eight patients developed locoregional recurrence (LR) and 24 patients developed distant disease. The 2- and 5-year LR control rates were 59% (95%CI 14–33%) and 48% (95%CI 36–59%), respectively. There was no significant difference in LR control rates when stratified by the use of adjuvant radiation (45% vs. 49%, p = 0.26), supplementary Fig. 4.
Stratification by class
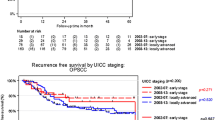
Overall, disease specific, and disease-free survival were then calculated stratifying by recurrent class status as shown in Fig. 1. Five-year overall survival was 47% (95%CI 32–61%), 26% (95%CI 14–40%) and 0% for class I, II and III, respectively. There was a statistically significant difference in overall survival between class I and class II (p = 0.034) and between class II and class III (p = 0.001) as well as between class I and III (p < 0.001) by log rank analysis. Five-year disease specific survival was 57% (95%CI 39–71%), 36% (95%CI 20–52%) and 0% for class I, II and III, respectively. Again there were significant differences between classes (p = 0.046, 0.001 and < 0.001). Five-year disease-free survival was 38% (95%CI 24–52%), 19% (95%CI 8.5–32%) and 0% for class I, II and III, respectively. There were significant differences between each class (p = 0.037, 0.007 and < 0.001).

Five-year overall survival (OS), disease specific survival (DSS) and disease-free survival (DFS) by class
Multivariate analysis
A multivariate, backward selected binary logistic regression model analysis was then performed. Variables with a p value < 0.1 on KM analysis were included in the model and included history of neck dissection for initial disease, smoking status, BMI, recurrent nodal disease, use of adjuvant radiation after salvage surgery, and recurrent class status. Significant predictors of five-year overall and disease specific survival included tobacco use and class status (Table 2). Patients with current or past tobacco use did significantly worse than patients with no history of tobacco use (OS–HR 2.3, 95%CI 1.1–4.6, p = 0.03 and DSS–HR 2.3, 95%CI 1.1–5.3, p = 0.04). Class remained a significant predictor of both OS and DSS. Patients in class III did significantly worse compared to patients in class II (OS–HR 2.9, 95%CI 1.5–5.5, p = 0.001 and DSS–HR 3.1, 95%CI 1.5–6.5, p = 0.002) and compared to patients in class I (OS–HR 3.7, 95%CI 1.9–7.3, p < 0.001 and DSS–HR 4.1, 95%CI 1.8–9.4, p = 0.001). Patients in class II also did worse than patients in class I (OS–HR 1.3, 95%CI 0.7–2.3, p = 0.43 and DSS–HR 1.3, 95%CI 0.7–2.7, p = 0.44), however this was not statistically significant. Use of adjuvant radiation after surgery with negative margins, recurrent nodal status, BMI, and primary neck dissection were not found to be independent predictors of survival on multivariate analysis. As this cohort represents a heterogenous group of patients, a subgroup analysis was performed for patients with primary disease of the oropharynx treated with radiation (without or without surgery) who developed secondary disease (recurrence or second primary) requiring oropharyngectomy. Smoking status, adjuvant radiation with negative margins, recurrent nodal disease and class status were included in the multivariate model and all variables including class status remained independent predictors of OS and DSS in this subgroup (Supplemental Table 1).
Discussion
While survival for patients with recurrent OPSCC has improved over the past three decades, likely secondary to a rise in HPV-mediated disease, 2 and 5 year overall survival for this cohort remains low [19, 20, 28]. A meta-analysis performed by Goodwin et al. evaluated studies between 1980 and 1990 and revealed a weighted 5-year overall survival of 26% for patients with recurrent OPSCC [19]. A more recent systematic review of the literature performed by Kao et al. published in 2018 found a 5-year OS rate of 30% [20]. Our cohort was comprised of a more heterogenous group of patients with recurrent or second primary disease in the oropharynx or adjacent sites requiring salvage oropharyngectomy, and found a similar median 5-year overall survival rate of 31%.
While salvage surgery was traditionally the primary treatment option for patients with recurrent disease in the oropharynx, recent improvements in radiation techniques have allowed for the possibility of re-irradiation in the setting of recurrent disease [17, 18, 29, 30]. There are no published randomized control trials comparing re-irradiation to salvage surgery and data is limited to comparisons of retrospective cohort studies [17]. However, the recent study by Ward et al. suggests that patients who undergo salvage surgery with negative margins followed by adjuvant radiation have the best outcomes. In our surgical cohort, adjuvant radiation in patients who obtained negative margins also portended improved survival on Kaplan–Meier analysis; however, this was not statistically significant on multivariate Cox regression analysis, likely due to the low number of patients in the radiation group (n = 10).
Regardless of the treatment approach, both salvage surgery and re-irradiation result in significant morbidity and mortality. Goodwin et al. summarized the incidence of minor and major operative complications at 39% and 27%, respectively [19]. Risk of peri-operative mortality is significantly higher in salvage surgery setting compared to primary surgery with rates cited between 1.8 and 8% [12, 19]. The economic burden of salvage treatment is also significant, and has been found to increase with increasing stage of recurrent disease [19].
Given the poor survival outcomes, significant morbidity, and cost of salvage surgery or re-irradiation, it has become increasingly important to identify factors that more reliably predict outcomes in this cohort. There have been numerous studies focused on identifying predictive factors to improve patient counseling and selection. Disease factors including advanced overall and T stage [19, 20, 24, 29, 31, 32], as well as histological grade [33], and close or positive margins [14, 21] have been associated with worse outcomes. Patient factors including male sex [19], older age [17], and alcohol abuse [21] have also been associated with worse survival outcomes. In this study, multivariate analysis revealed that tobacco use (past or present) was associated with both worse overall survival and disease specific survival, consistent with existing published data. While results of the Ward et al. study showed that surgery with negative margins and adjuvant radiation also predicted improved LR control compared to re-irradiation alone, we did not find similar results when comparing adjuvant radiation with salvage surgery alone, suggesting that surgical treatment may be associated with improved LR control.
In the primary setting, HPV status is a significant predictor of survival for OPSCC and is thought to continue to predict improved survival in patients with recurrent disease [34]. However, in our cohort, HPV status did not significantly predict 5-year overall or disease specific survival on Kaplan–Meier survival analysis.
Three additional variables that consistently predict poor survival are time to recurrence, comorbidity scores and functional status [17, 18, 20, 22,23,24,25]. Laryngopharyngeal dysfunction as measured by tracheostomy or feeding tube dependence is a unique predictor of poor outcomes among patients with recurrent head and neck malignancy [18, 25]. Ward et al. used recursive partitioning analysis to define three classes of patients with recurrent OPSCC undergoing re-irradiation [18]. Survival was shown to be significantly different between each class with class III (defined as recurrence less than 2 years with evidence of laryngopharyngeal dysfunction) performing the worst. In this study, we used a modification of this class system to evaluate survival outcomes in the salvage oropharyngectomy setting. The three classes were defined as class I (recurrence greater than 2 years after initial radiation), class II (recurrence less than or equal to 2 years without laryngopharyngeal dysfunction) and class III (recurrence less than or equal to 2 years and evidence of laryngopharyngeal dysfunction). Class status predicted 5 year overall, disease specific and disease-free survival with class III having the worst survival outcomes followed by class II and then class I. On multivariate analysis class status continued to be an independent predictor of overall survival and disease specific survival even when history of neck dissection, recurrent nodal stage, adjuvant radiation, tobacco use, and BMI were taken into account. These findings are similar to the results from the Ward et al. study evaluating re-irradiation [18]. These two studies bring into question the benefit of aggressive salvage treatment for patients with oropharyngeal recurrences, within 2 years from initial treatment, who have tracheostomy or feeding tube dependence pre-salvage.
The decision to proceed with salvage surgery in patients with poor prognosis of head and neck SCC, including salvage oropharyngectomy, is complex and should involve shared decision making between the patient and surgeon. A careful assessment of patient-centered goals and the likelihood of achieving these goals is necessary. In the era of precision oncology, systemic therapies and clinical trials as alternative therapy could be considered. For patients who are deemed surgical candidates, an informed discussion of anticipated outcomes goes beyond an understanding of the general risks and alternatives of the procedure, and instead requires patient specific risk stratification [35,36,37].
Limitations
This study is subject to the biases inherent to any retrospective review. We were unable to obtain radiation doses or fields for primary or recurrent disease in the cohort, and, therefore, this was not included in the analysis. We also included second primaries in addition to recurrent disease which may portend improved prognosis compared to recurrent disease alone [30]. This cohort included patients with recurrent disease in the oropharynx or adjacent subsite with extension requiring salvage oropharyngectomy. As oral cavity, oropharynx and hypopharynx or larynx often portend different prognoses [38], we evaluated overall survival stratification by recurrent tumor site and found no difference in survival outcomes suggesting that the recurrent nature in a previously irradiated bed may play a more important role than recurrent primary site. Additionally, subgroup analysis of only patients with primary oropharynx disease showed similar outcomes to the overall cohort. Further, HPV status was only known for 46% (39/84) of oropharyngeal recurrences. The lack of available HPV status data may explain why HPV status did not reveal to be a significant predictor of survival in our recurrent cohort.
Conclusion
Patients with recurrent head and neck cancer requiring salvage oropharyngectomy who are within 2 years of initial treatment and who experience pre-salvage laryngopharyngeal organ dysfunction demonstrate very poor outcomes. Patients who are able to achieve salvage surgery with negative margins and undergo adjuvant radiation may have improved survival outcomes. These findings can inform more accurate patient selection, risk stratification, and shared decision-making for individuals contemplating salvage oropharyngectomy.
References
Ferlay J, Soerjomataram I, Dikshit R et al (2015) Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 136(5):E359–386
Chaturvedi AK, Engels EA, Pfeiffer RM et al (2011) Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J Clin Oncol 29(32):4294–4301
Pytynia KB, Dahlstrom KR, Sturgis EM (2014) Epidemiology of HPV-associated oropharyngeal cancer. Oral Oncol 50(5):380–386
Sturgis EM, Cinciripini PM (2007) Trends in head and neck cancer incidence in relation to smoking prevalence: an emerging epidemic of human papillomavirus-associated cancers? Cancer 110(7):1429–1435
Faraji F, Eisele DW, Fakhry C (2017) Emerging insights into recurrent and metastatic human papillomavirus-related oropharyngeal squamous cell carcinoma. Laryngosc Investig Otolaryngol 2(1):10–18
Nguyen-Tan PF, Zhang Q, Ang KK et al (2014) Randomized phase III trial to test accelerated versus standard fractionation in combination with concurrent cisplatin for head and neck carcinomas in the Radiation Therapy Oncology Group 0129 trial: long-term report of efficacy and toxicity. J Clin Oncol 32(34):3858–3866
Taneja C, Allen H, Koness RJ, Radie-Keane K, Wanebo HJ (2002) Changing patterns of failure of head and neck cancer. Arch Otolaryngol Head Neck Surg 128(3):324–327
Lassen P, Eriksen JG, Hamilton-Dutoit S, Tramm T, Alsner J, Overgaard J (2009) Effect of HPV-associated p16INK4A expression on response to radiotherapy and survival in squamous cell carcinoma of the head and neck. J Clin Oncol 27(12):1992–1998
Network NCC (2019) Head and Neck Cancers (Version 2.2019). https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck_blocks.pdf. Accessed 7 Apr 2019
Haughey BH, Sinha P (2012) Prognostic factors and survival unique to surgically treated p16+ oropharyngeal cancer. Laryngoscope 122(Suppl 2):S13–33
Agra IM, Filho JG, Martins EP, Kowalski LP (2010) Second salvage surgery for re-recurrent oral cavity and oropharynx carcinoma. Head Neck 32(8):997–1002
Gehanno P, Depondt J, Guedon C, Kebaili C, Koka V (1993) Primary and salvage surgery for cancer of the tonsillar region: a retrospective study of 120 patients. Head Neck 15(3):185–189
Gilbert H, Kagan AR (1974) Recurrence patterns in squamous cell carcinoma of the oral cavity, pharynx, and larynx. J Surg Oncol 6(5):357–380
Patel SN, Cohen MA, Givi B et al (2016) Salvage surgery for locally recurrent oropharyngeal cancer. Head Neck 38(Suppl 1):E658–664
Pradhan SA, Rajpal RM, Kothary PM (1980) Surgical management of postradiation residual/recurrent cancer of the base of the tongue. J Surg Oncol 14(3):201–206
Taguchi T, Nishimura G, Takahashi M et al (2016) Treatment results and prognostic factors for advanced squamous cell carcinoma of the head and neck treated with salvage surgery after concurrent chemoradiotherapy. Int J Clin Oncol 21(5):869–874
Zafereo ME, Hanasono MM, Rosenthal DI et al (2009) The role of salvage surgery in patients with recurrent squamous cell carcinoma of the oropharynx. Cancer 115(24):5723–5733
Ward MC, Riaz N, Caudell JJ et al (2018) Refining patient selection for reirradiation of head and neck squamous carcinoma in the IMRT Era: a multi-institution cohort study by the MIRI collaborative. Int J Radiat Oncol Biol Phys 100(3):586–594
Goodwin WJ Jr (2000) Salvage surgery for patients with recurrent squamous cell carcinoma of the upper aerodigestive tract: when do the ends justify the means? Laryngoscope 110(3 Pt 2 Suppl 93):1–18
Kao SS, Ooi EH (2018) Survival outcomes following salvage surgery for oropharyngeal squamous cell carcinoma: systematic review. J Laryngol Otol 132(4):299–313
Nichols AC, Kneuertz PJ, Deschler DG et al (2011) Surgical salvage of the oropharynx after failure of organ-sparing therapy. Head Neck 33(4):516–524
Philouze P, Peron J, Poupart M, Pujo K, Buiret G, Ceruse P (2017) Salvage surgery for oropharyngeal squamous cell carcinomas: a retrospective study from 2005 to 2013. Head Neck 39(9):1744–1750
Riaz N, Hong JC, Sherman EJ et al (2014) A nomogram to predict loco-regional control after re-irradiation for head and neck cancer. Radiother Oncol 111(3):382–387
Stell PM (1991) Time to recurrence of squamous cell carcinoma of the head and neck. Head Neck 13(4):277–281
Tanvetyanon T, Padhya T, McCaffrey J et al (2009) Prognostic factors for survival after salvage reirradiation of head and neck cancer. J Clin Oncol 27(12):1983–1991
Birkeland AC, Rosko AJ, Beesley L et al (2017) Preoperative tracheostomy is associated with poor disease-free survival in recurrent laryngeal cancer. Otolaryngol Head Neck Surg 157(3):432–438
Edge SB, Compton CC (2010) The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 17:1471–1474
Bachar GY, Goh C, Goldstein DP, O'Sullivan B, Irish JC (2010) Long-term outcome analysis after surgical salvage for recurrent tonsil carcinoma following radical radiotherapy. Eur Arch Oto-rhino-laryngol 267(2):295–301
Garofalo MC, Haraf DJ (2002) Reirradiation: a potentially curative approach to locally or regionally recurrent head and neck cancer. Curr Opin Oncol 14(3):330–333
Spencer SA, Harris J, Wheeler RH et al (2001) RTOG 96-10: reirradiation with concurrent hydroxyurea and 5-fluorouracil in patients with squamous cell cancer of the head and neck. Int J Radiat Oncol Biol Phys 51(5):1299–1304
Culie D, Benezery K, Chamorey E et al (2015) Salvage surgery for recurrent oropharyngeal cancer: post-operative oncologic and functional outcomes. Acta Otolaryngol 135(12):1323–1329
Kim J, Kim S, Albergotti WG et al (2015) Selection of ideal candidates for surgical salvage of head and neck squamous cell carcinoma: effect of the Charlson-age comorbidity index and oncologic characteristics on 1-year survival and hospital course. JAMA Otolaryngol Head Neck Surg 141(12):1059–1065
Kasler M, Fodor J, Oberna F, Major T, Polgar C, Takacsi-Nagy Z (2008) Salvage surgery for locoregional failure after definitive radiotherapy for base of tongue cancer. In vivo (Athens, Greece) 22(6):803–806
Fakhry C, Westra WH, Li S et al (2008) Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst 100(4):261–269
Bossi P, Alfieri S, Strojan P et al (2019) Prognostic and predictive factors in recurrent and/or metastatic head and neck squamous cell carcinoma: a review of the literature. Crit Rev Oncol/Hematol 137:84–91
Qureshi HA, Abouyared M, Barber B, Houlton JJ (2019) Surgical options for locally advanced oropharyngeal cancer. Curr Treat Opt Oncol 20(5):36
Taylor JMG, Shuman AG, Beesley LJ (2019) Individualized prognostic calculators in the precision oncology era. Oncotarget 10(4):415–416
Hamoir M, Holvoet E, Ambroise J, Lengele B, Schmitz S (2017) Salvage surgery in recurrent head and neck squamous cell carcinoma: oncologic outcome and predictors of disease free survival. Oral Oncol 67:1–9
Acknowledgements
MEH was supported by the National Institutes of Health (T32 DC005356). JCB was supported in part by the American Cancer Society (132034-RSG-18-062-01-TBG). SBC was supported by the National Institutes of Health/National Cancer Institute (K08CA226350-02).
Author information
Authors and Affiliations
Contributions
Conceptualization: MES, AJR, MEHN; methodology: MES, AJR and MEHN; data acquisition: MEHN, JB, FW, PS, MM, KAC, KMM, CLS, SAM, MEP, CRB, GTW, AGS, SBC, DBC, AJR, and MES; supervision: MES, AJR; formal analysis and investigation: MES, AJR, and MEHN; writing—original draft preparation: MEHN; writing—review and editing: MEHN, JB, CTH, JCB, FW, PS, MM, KAC, KMM, CLS, SAM, MEP, CRB, GTW, AGS, SBC, DBC, AJR, and MES; supervision: MES, AJR.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to disclose.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee, University of Michigan Institutional Review Board (HUM00081554), and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
405_2020_5913_MOESM2_ESM.pdf
Supplemental fig. 1: Five-year Overall Survival (OS) and disease specific survival (DSS) stratified by A) primary neck dissection, B) recurrent nodal status, C) tobacco use, D) BMI, and E) use of radiation after salvage surgery with negative margins (PDF 83 kb)
405_2020_5913_MOESM3_ESM.pdf
Supplemental fig. 2: five-year overall survival (OS) and disease specific survival (DSS) stratified by HPV status (PDF 66 kb)
Rights and permissions
About this article

Cite this article
Heft Neal, M.E., Brennan, J., Haring, C.T. et al. Predictors of survival in patients undergoing oropharyngeal surgery for cancer recurrence after radiation therapy. Eur Arch Otorhinolaryngol 277, 2085–2093 (2020). https://doi.org/10.1007/s00405-020-05913-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-020-05913-z