
Abstract
Cardiovascular aging is a physiological process affecting all components of the heart. Despite the interest and experimental effort lavished on aging of cardiac cells, increasing evidence is pointing at the pivotal role of extracellular matrix (ECM) in cardiac aging. Structural and molecular changes in ECM composition during aging are at the root of significant functional modifications at the level of cardiac valve apparatus. Indeed, calcification or myxomatous degeneration of cardiac valves and their functional impairment can all be explained in light of age-related ECM alterations and the reciprocal interplay between altered ECM and cellular elements populating the leaflet, namely valvular interstitial cells and valvular endothelial cells, is additionally affecting valve function with striking reflexes on the clinical scenario. The initial experimental findings on this argument are underlining the need for a more comprehensive understanding on the biological mechanisms underlying ECM aging and remodeling as potentially constituting a pharmacological therapeutic target or a basis to improve existing prosthetic devices and treatment options. Given the lack of systematic knowledge on this topic, this review will focus on the ECM changes that occur during aging and on their clinical translational relevance and implications in the bedside scenario.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cardiac valve degeneration represents the most common pathological condition for valve disease and the more frequent indication for surgery in the US and Europe [14]. Mitral valve (MV) and aortic valve (AV) are primarily interested by degeneration, causing severe valve dysfunction with important impact on the overall ventricle function over time [32]. MV is usually affected by a myxomatous degenerative phenomenon leading to severe regurgitation, while the process of calcification more often harnesses AV leaflets, causing different degrees of stenosis with subsequent repercussion on ventricular performance [14]. Aging is associated to a cascade of biological and molecular events that might translate and lead to structural deterioration and functional impairment of cardiac tissues [95]. Despite the interest and experimental effort lavished on aging of cardiac cells, increasing evidence is pointing at the pivotal role of extracellular matrix (ECM) in cardiac aging. ECM does not exert a role of mere support, but is a key factor in the tight interplay with the cellular compartment. Structural and molecular changes in ECM composition during aging are at the root of significant functional modifications at the level of cardiac valve apparatus [17]. Indeed, calcification or myxomatous degeneration of cardiac valves and their functional impairment can all be explained in light of age-related ECM alterations. Valvular interstitial cells (VICs) and valvular endothelial cells (VECs) populating cardiac valves have been reported to be extremely sensitive to tissutal environment and physiological states and their activity is reciprocally influenced by changes in the surrounding matrix substrate [17, 137]. A bivalent mechanism is therefore established in which valve cells actively answer to mechanical load or biochemical signals through phenotype switches resulting in the production of different components of ECM [137]. At the same time, age-related or disease-related ECM changes are able in turn to deeply influence VICs and VECs behavior. Aged valve tissues undergo an ECM remodeling process resulting in fibrillar disarray with an imbalance in the ratio between collagen type I and type III and increased stiffness [159, 161]. Also, augmented concentrations of proteoglycans and glycosaminoglycans throughout the leaflets have also been reported and contribute to increased stiffness in the circumferential direction with subsequent impairment of the elastomechanical properties of the leaflet itself [158]. VICs have been shown to be at the base of ECM changes in elderly valve tissues contributing to myxomatous degeneration or calcification [101, 107]. However, ECM remodeling itself, stimulating the expression of different substrate matrix proteins and altering tissutal organization, influences both VICs and VECs biosynthetic activity eventually favoring leaflet tissutal modifications and therefore the risk of valvular disease [17]. Indeed, as valve ECM remodels during lifetime, the different biochemical composition of the supporting matrix or its simple structural deterioration triggers changes not only in valvular cells phenotype but also in their secretory activity. The age-related ECM remodeling, typical of older leaflets [161], impairs tissutal density and the barrage function of the fibrosa, determining an increased permeation of several VEC-secreted proteins throughout the valve layers. Accumulation of important mediators within the leaflet, as inflammatory or hemostatic proteins, might favor tissutal alteration and calcific nucleation [17].
Undoubtedly the two phenomena of physiological aging and pathological alteration are closely imbricated as they are reciprocal actors in the determinism of the disease. The mechanisms governing these intertwined pathways and the sequence of events leading to pathology is unclear even if it might be reliably speculated that the age-related alterations constitute a background for the development of pathological changes. In this context, the study of genetic factors predisposing to the onset of disease at later stages in life is very important. However, as in a multifactorial disease, the presence of external factors superimposed to a particular genetic background play a fundamental role and is able to trigger the actual “expression” and translation into disease of an underlying pathological potential. Similarly, ECM changes might be considered as an underlying framework on which pathologic changes can establish either affecting the biological activity of VICs and VECs or by means of a reciprocal interaction with them. In support of this, mechanical properties of the ECM and in particular increased degree of its stiffness, as in aged valve, have been shown to modulate and influence the differentiation of VICs to pathological phenotypes in response to biochemical cues [185]. Additionally, the fact that some of the characteristics found in aged valves reflect in different extents the changes observed in diseased valve further support this hypothesis. In a study by Kupari et al., increased circulating levels of collagen type III and I telopeptides were found in aortic stenosis patients [93]. This finding might be associated to the findings of increased collagen type III and I and telopeptides in aged valves as described in details below.
These initial findings clearly suggest the emerging need for a more accurate understanding of the changes occurring in valvular ECM during aging, which have been unjustly underestimated by the current literature. Considering the burden of age-related valve disease on an aging population [116], understanding the interplay between valve cells and ECM and their response to different physiological states appears fundamental to develop noninvasive therapeutic strategies [17] or to optimize existing treatment options. In light of the scarce availability of a comprehensive picture on this topic, this review will focus on changes of ECM components in the aged valves trying to unveil their clinical translational relevance and potential implications in the bedside scenario.
The clinical burden
As a result of the rise in life expectancy and the consequent progression and incidence of age-related valve disease, the need for surgical repair or replacement of degenerated valves is enormously increasing, determining a consistent burden on both surgical activity and general healthcare management [14]. Indeed, the amount of elderly patients requiring surgery is increasing and this subpopulation carries a significant intraoperative and postoperative risk due to their several comorbidities or simply poor general health conditions [31]. Heavily calcified valves, fragile cardiac and aortic tissue, chronic lung and renal disease profoundly affect both the surgical technical aspects and the postoperative care and retrieve from the operation [102]. Cardiac surgery in the elderly is associated with increased mortality, surgical complications, hospitalization time (length of stay, LOS), and usually demands for more complex procedures or combined operations of valve replacement and myocardial revascularization [31].
In mitral valve, aging mainly translates in myxomatous degeneration that determines redundancy and thickening of the leaflets impairing coaptation and mostly causing regurgitation [137]. However, MV annulus calcification or leaflet retraction related to the changes in valve structure is also frequent, especially when associated to previous rheumatic disease. Abnormal age-related activation of myofibroblasts, deeply affecting the dynamic balance between the synthesis and degradation of connective tissue, is known to be at the root of these structural alterations [137]. Additionally, the aging process determines an intrinsic weakening of the whole heart skeleton, and this reflects in the general tendency to dilation of the mitral annulus under hemodynamic load and intraventricular telediastolic pressure [57]. This requires annulus reinforcement with prosthetic rings [62], but considering the natural elasticity and dynamic compliance of the heart, a great effort to simulate the mechanical properties of the skeletal part of the heart is mandatory in this context [35]. Different materials have been used in an attempt to mimic annulus properties, taking into account the redistribution of forces bearing on the leaflet and the annulus following reconstructive plasty of the MV [144].
As far as degenerative AV disease is concerned, stenosis represents the most frequent cause of dysfunction in the elderly with a 2–7 % prevalence, which is in any case destined to rise because of the increasing life expectancy. AV stenosis is characterized by a silent chronic course with a steeper trend in clinical evolution and prognosis after the onset of symptoms [116]. Medical therapy is limited to the relief of symptoms, but is not able to have an impact on actual survival, while the surgical option remains the most effective treatment. However, despite this strategy carries low operative risk, improved survival, and optimal freedom from reoperation in younger patients, the 30-day mortality in patients aged over 80 years increases up to 15 %, with a significant increase in operative and postoperative complications [177]. In the recent years, new minimally invasive strategies are emerging to guarantee the treatment of AV stenosis in high-risk surgical patients (STS Score >10, logistic EuroSCORE >20). Transcatheter aortic valve implantation (TAVI), developed in 1992 by Andersen et al. [10], and clinically introduced in 2002 by Cribier [44], constitutes an option in this subpopulation, allowing avoidance of surgical complications essentially related to open chest operative technique, aortic cross clamping and cardioplegic arrest [102]. Differently from the MV, the major biological obstacle in this framework is represented by the heavy calcium deposition at the level of the connectival network of the leaflets and of the aortic annulus, which is thought to be due to a shift toward an osteoblastic phenotype of the cells within the aortic structure [87, 113].
The biological counterpart
In the physiology of the cardiac valve apparatus, the combined activity of myofibroblasts and connectival degrading enzymes normally warrant a strict regulation of matrix homeostasis within the valve and ensure an adequate functional architecture of the valve itself [148]. In this extent, the highly preserved stratified framework exhibited by the valve internal structure is crucial to meet the biomechanical needs related to the loading forces sustained by the valve over a lifetime. A continuous turnover of ECM is at the biological basis of the valve structure conservation, and is due to the activity of myofibroblast-like cells populating the leaflets, namely valvular interstitial cells (VICs). Also valvular endothelial cells (VECs) have been reported to exert a fundamental action in the maintenance of valve homeostasis, being responsible of hemostatic regulation [30] and displaying close interactions with VICs and valvular ECM [29]. VECs have been shown to actively respond to changes in the surrounding microenvironment via several mechanotransduction pathways [56] and their dysfunction has been claimed to be involved in the initiation of valvular disease [13, 46, 56, 152]. It is known that ECM components are responsible for the accommodation of the hemodynamic repetitive changes occurring throughout the cardiac cycle and that VICs and VECs mediate its continuous remodeling warranting valve durability [136, 137]. Early studies by Schoen et al. demonstrated specific topographical differences in ECM component within the valve [148], which will be discussed separately.
Aortic valve
In the physiological normal AV, the fibrosa (or arterial side) of the leaflet mainly contains type I collagen allowing for maximal coaptation during closure and preventing cusp prolapse, while the ventricularis is characterized by higher content in elastin, which provides better expandability during diastole and elastic recoil during systole. Shock and shear absorption is guaranteed by the hydrophilic proteoglycans present in the spongiosa [148]. Therefore, ECM spatial distribution and composition affect valve function, and alterations at the molecular level of such a delicate balance are able to determine the dysfunction and the morbidity that surgeons encounter at the operative table. Initial studies on explanted degenerated valves from adults demonstrated thickening phenomena with disorganization of collagen fibers, enhanced VICs density and calcifications [124]. An interesting study from Hinton et al. [75] on valvulogenesis, in which a comparison between characteristics of animal valves during embryogenesis and human pediatric diseased aortic valves was performed, showed that the developmental program underlying leaflet remodeling during life includes a precise spatiotemporal coordination of ECM organization and a progressive VIC compartmentalization. Also, increases in collagen content, diameter of collagen fibrils and level of collagen cross-linking were reported in adult compared to fetal porcine heart valves [90]. These balanced mechanisms are disrupted in a pathological valve, underpinning the importance of the historarchitectural organization of ECM in valve pathobiology. Loss of collagen, misorientation and fragmentation of elastin fibers, and VIC disarray (with formation of cellular clusters alternated to cell-free areas in the interstitium) were demonstrated in pathological valves [75].
Valve aging shares several of the features described on pathological degenerated valves. The majority of the changes found in physiologically aged valves seems to be prodromal to the establishment of more defined pathological alterations. Conversely, another number of age-related alterations overlap with the ones described in pathological valves with the boundaries between physiological aging and pathology being very indefinite and the actual translation of these changes in a clinical evident pathological condition being associated to the superimposition of different other factors (genetic predisposition, environment, life-style, controllable risk factors as smoking physical inactivity hypercholesterolemia, uncontrolled hypertension or diabetes, etc.).
More specifically, aging is associated to changes in type I and type III collagen as found in diseases calcified valves [59]. Beside their relative content in AV, their distribution and degree of cross-linking acquire a relevant significance in valve aging. Indeed, after their secretion as propeptides, immature forms of collagen undergo cross-linking mainly at the lysine (Lys) and hydroxylysine (Hyl) residues in the telopeptide regions at both ends of the molecule. Telopeptides further bind with particular helical regions of another molecule to form a divalent immature cross-link, which undergoes a progressive maturation process towards a higher valence of cross-linking. The entity of cross-linking and proportion of telopeptides characterize many of the mechanical properties of the AV.
In physiological aged valves, a change in the nature of C-terminal telopeptide of collagen type I was reported, supporting the idea of a change in the maturation of cross-links together with an altered collagen turnover [59]. This has been explained by an age-related reduction in the activity of the LH isoenzyme, which is responsible for the hydroxylation of telopeptidyl lysine. At the same time, an overall decrease in the N–terminal telopeptide of type III collagen has been reported in aged valves [59]. Mechanisms underlying these changes are thought to be associated to increased activity of matrix metalloproteinases (MMP-1, MMP-2, MMP-3, MMP-9), their tissue inhibitor-1 and tissue inhibitor, which are mediating an ongoing ECM remodeling process [63, 93, 147].
Additionally, collagen-bound advanced glycation end products (AGEs), arising from non-enzymatic glycation of serum and vascular proteins, have been shown to play a role in the increase of aortic stiffness during aging [135]. AGEs accumulation within the ECM has been shown to induce collagen cross-linking in animals [141]. Additionally, AGEs are recognized by several receptor molecules, with the receptor of AGEs (RAGE) being the most extensively investigated. Its activation leads to a pro-inflammatory state and AGE–RAGE interaction has been shown to be involved in aortic valve changes due to metabolic stress from high fat intake in animal models [77]. These data found a counterpart in the observation that patient with calcific aortic valve stenosis have decreased levels of soluble RAGE, a natural inhibitor of the AGE–RAGE system with anti-atherogenic properties [20]. Interestingly, in animal studies Pioglitazone-mediated RAGEs downregulation attenuated the progression of AV calcification by reducing inflammatory cell infiltration and oxidative stress [100].
All these initial alterations of the main components of ECM, together with abnormal activity of VICs, define a framework that further becomes a theater for the establishment of leaflet calcification normally observed at surgery. However, other ECM components are altered during AV aging. Jian et al. [80] demonstrated increased levels of tenascin-C (a glycoprotein normally expressed in developmental bone tissue and atherosclerotic plaques) in aortic degenerated calcific valves. This protein participates in the physiological mineralization being associated to bone morphogenetic protein (BMP) pathways [103], and is normally expressed in low levels in aged valves in the subendothelial space. Tenascin-C expression might be induced by a number of cytokines as BMP, TGF-beta and TNF-alpha [85], and also by mechanical stress in fibroblasts [145]. Some studies suggested that the accumulation of tenascin-C, induced by several factors as cytokines, or collagen damage, might be prodromal to the progression of aortic valve disease to calcific stenosis. Accumulated tenascin-C in the deeper layers of the valve would up-regulate the expression of MMP-2 and the positive feedback by MMP-2 would induce further accumulation of tenascin-C. This would lead to cellular aggregation and increase in alkaline phosphatase (ALP) expression with subsequent deposition of calcium phosphates [80]. The induction of tenascin-C synthesis in fibroblasts through mechanical stress or collagen damage [145], together with the observation of increased level of this protein in pressure-overloaded valve in elderly hypertensive patients [146], remark the idea that age-related structural changes of the ECM components can constitute a trigger for pathological alterations to occur and further explain the overlap in the biochemical and mechanical features of aged and diseased valves.
As an additional confirmation, osteopontin and BMP were found to be up-regulated in calcified valves together with EGR-1, a transcription factor inducing both tenascin-C and osteopontin [67, 111].
Gene expressions of BMP-2 and ALP were significantly accelerated in AVICs from aged rats [150]. In parallel, ALP activity was found significantly increased in calcified valves [80]. Along with these findings, activity of matrix metalloproteinase type 2 (MMP-2), a gelatinase, was found enhanced in calcified valves [80]. In concert with the previous data, Fondard et al. identified changes in expression of MMP-3, MMP-9 and of their inhibitor, i.e. TIMP-1, in pathological valves [63]. Interestingly, in a study comparing tricuspid aortic valves from elderly patients with and without calcific aortic stenosis, both MMP-2 expression and its gelatinase activity was significantly higher in calcific stenotic valves, suggesting that that MMP-2 is present as a latent pro-enzyme in normal aged valves and turns activated in pathological valves [88]. Also, this observation confirms the idea of age as an underlying background for the establishment of pathology and the finding of the induction of MMP expression through mechanical shear stress, as in stiffened or aged tissues [15], further confirms this hypothesis.
Another interesting ECM component involved in AV degeneration is fibulin-4, a protein known to maintain the structure of the extracellular matrix. Reduction in its expression has been shown to lead to valve thickening and disarrangement of elastic fibers in an animal model [71]. Although the precise mechanism as not been elucidated yet, Hanada et al. associated this protein to perturbation of the TGF-beta signaling [71].
As mentioned above, ECM has been shown to be responsive to shear stress alterations, as testified by changes in the expression and activity of the proteases MMP-2, MMP-9, cathepsin L and cathepsin S, and an abnormal mechanical stimulation was shown to trigger calcification [166]. Altered ECM becomes a pabulum for the infiltration of inflammatory cells or for the phenotype switch of VICs into secreting myofibroblasts, with enhanced ECM deposition. This process is led by an increase in the expression of toll-like receptor (TLR)-2 and TLR-4 and in pro-inflammatory and pro-osteogenic responses [184]. The modulation of the nuclear factor-κB activity [186], of the osteoprotegerin (OPG)/receptor activator of nuclear factor kappa B (RANK)/RANK ligand (RANKL) pathway [83], and of associated signal transduction pathways [53] is thought to subtend the pro-osteogenic drive. Age-related VECs alterations determine lipid penetration and accumulation in areas of damage or inflammatory injury, and permit lipoproteins (LDL) implicated in atherogenesis to subsequently undergo oxidative modifications [121]. These ox-LDLs are cytotoxic and capable of enhancing inflammatory response, through TGF-β1, TNF-α, interleukin (IL)-1β pathways, eventually leading to both fibrotic and calcific processes, with an increase in valve stiffness [53]. The renin–angiotensin system is thought to modify this fibrotic process, since angiotensin-converting enzyme (ACE) and angiotensin-II are up-regulated and their effect on valve myofibroblasts has been shown [119].
In a genomic study, Bossè et al. identified many of the actors involved in calcific degeneration of AV stressing the role of inflammation and matrix remodeling in this context and eventually revealed phenomena of endochondral metaplasia in AV leading to calcification [24]. With this regard, Cappelli et al. have recently reported enhanced activity of gamma-glutamyltransferase (GGT), an enzyme linked to calcium metabolism and atherogenesis, inside the lipid component of valves leaflets by osteoclastic-like resident cells [34]. The findings of this study enlighten a potential link between atherosclerosis-related phenomena and the calcification of AV. Several study reported the association between atherosclerosis and aortic valve stenosis demonstrating as these two conditions share similar mechanisms and clinical risk factors, as age, male gender, hypertension, hyperlipidemia, smoking and diabetes [2, 8, 131]. The majority of these predisposing factors are strongly associated with inflammation and, interestingly, calcification in response to an inflammatory stimulus seems to be a proper feature of aortic valve, as it has not been described in other cardiac valves. In fact, only the aortic VICs exhibited an osteogenic in response to a pro-inflammatory stimulation via TLR-4 resulting in BMP-2 production [179]. The association between the calcification process and inflammation in aortic valve disease has been testified by the observation of inflammatory reaction as an early feature in histologic specimens from aortic stenosis patients [4, 124]. As above-mentioned, lipid accumulation, infiltration of macrophages and lymphocytes represent the substrate activating the calcification cascade [65, 120, 138]. A recent study using positron emission tomography proved that early aortic valve inflammation, prior to hemodynamic impairment, drives the pathophysiologic processes of valve calcification in humans [1], even if remains difficult to distinguish between the cause and the consequence.
Calcification of the aortic valve per se is associated with disruption of the basal membrane, infiltration of inflammatory cells and lipids deposition [58, 110], and cytokines and vesicles released from macrophages may initiate the calcification of the ECM. Conversely, calcium may promote inflammation which in turn would enhance further calcification perpetuating a self-sustained “vicious cycle” [115, 172]. Furthermore, TNFα-mediated oxidative stress causes loss of endothelial protective function of VEC and chronic inflammation sustains fibrogenic and osteogenic activation [60]. The importance of inflammation pathways in the genesis of aortic valve disease has been extensively investigated and confirmed by many studies in recent years. Oxidized lipids are found in calcifying aortic valves, and could promote osteoblastic differentiation of valvular fibroblasts and macrophages via activation of LRP-5/Wnt and Runx2/Cbfa-1 pathways, eventually leading to calcification [118]. Also, the interaction between sphingosine 1-phosphate receptors and TLR-4 signaling leads to a cooperative up-regulation of inflammatory, angiogenic, and osteogenic pathways [61]. TLR-3, NF-κB and ERK1/2 pathways in VICs are also implicated in the pro-osteogenic effects [187]. Interestingly, the presence of numerous proinflammatory cytokines such as TNF-2, BMP molecules, and interleukins such as IL-1β/2/6 has been shown in degenerated diseased aortic valves [104]. Anti-inflammatory effects of Interleukin-1 receptor antagonist are reduced in stenotic valves in respect to normal valves; TGF-β, another anti-inflammatory mediator, is also ubiquitous in diseased valves, especially bound to matrix, and acts as a promoter of ECM fibrosis [97]. In established aortic stenosis, histopathology of the valves shows numerous new blood vessels associated with the expression of angiogenic factors such as vascular endothelial growth factor (VEGF) and endothelial nitric oxide synthase (NOS) [155], however, the origin of endothelial cells seen in this setting is poorly understood. In the early stages of calcific lesion formation, neoangiogenetic capillary sprouts exhibited the endothelial cell markers CD31, CD34 and von-Willebrand factor (vWF) as well as carcinoembryonic antigen cell adhesion molecule-1 (CEACAM1), Tie-2 and angiogenesis inhibitor endostatin indicating angiogenesis as a pathogenic factor in aortic stenosis [36]. In other studies the co-expression in VICs of smooth muscle alpha-actin (α-SMA) and VEGF receptor-2 suggested a mesenchymal-to-endothelial transition in early stage valve lesion with formation of new capillaries with inter-endothelial junctions and partial basement membrane-like structure, reinforcing the role of angiogenesis in the calcification process and valve remodeling [99, 129]. A recent study demonstrated a stretch-mediated activation of inflammatory pathways evaluated using miRNA analysis [128] but the multiple connections between inflammation, hemodynamics and aortic valve pathophysiology are far from being completely elucidated.
Glycosaminoglycans (GAGs) content of AV also changes with age. In a study on porcine valves at different ages, Stephens et al. reported an aging-related increase in the 4-sulfation to 6-sulfation ratio of GAGs, that reversed the compressive tissue phenotype observed in younger AV into a tensile one [158]. Since GAGs are well represented in the central spongiosa layer, it has been speculated that this layer allows to reduce the shearing which results from the differences in motion kinetics of the fibrosa and ventricularis during leaflet deformations [149, 180]. GAGs are hypothesized to contribute substantially to the behavior of the bulk tissue at lower physiological force levels by means of mechanical interactions with the collagen, whereas at higher tissue stress levels, tissue response is dominated by the fully loaded and straightened collagen fibers [171]. The specific arrangement of GAGs within the leaflet, with increased content of water-binding GAGs localized in regions that experience more compression, achieves an important significance in controlling tissue behavior over the cardiac cycle [69, 70]. In an experimental setting, the removal of GAGs from the aortic valve had actually no measureable effect on extensional mechanical properties including peak stretch, hysteresis, or creep. However, in the low force range, hysteresis was markedly reduced after GAG removal. Therefore, GAGs do not play a direct role in modulating the time-dependent tensile properties of valvular tissues, but they are strongly connected with fiber–fiber and fiber–matrix interactions at low forces levels. In this context, GAGs are thought to be important in providing a damping mechanism to reduce leaflet flutter when the leaflet is not under high tensile stress [54]. Considering the role of GAGs, the changes occurring with aging result in increased tensile loading on the aortic leaflet, and may partially explain the age-related decrease in aortic compliance [45].
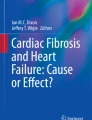
Additionally, a recent study from Balaoing et al. underlined the hemostatic imbalance in old aortic pig valve due to age-related changes in the activity of VECs [17]. Interestingly, these Authors found an increased secretory activity of prothrombotic proteins such as vWF, tissue factor pathway inhibitor (TFPI) and tissue plasminogen activator (tPA) in older valves. This aberrant secretory activity, coupled with the age-related changes in collagen type I and elastin organization, justified the sequestration of the soluble hemostatic protein deeply within the ventricularis part of the AV leaflet, as the barrier function exerted by the aligned collagen fibrils of healthy valves is lost in older valves. Authors demonstrated in vitro that the presence of a large burden of vWF induced a pro-osteogenic activity in the interstitial cells leading to calcific nodule formation [17]. The importance of vWF is supported by the fact that inhibition of the metalloproteinase ADAM-17, the physiologic inactivator of vWF, during mouse development results in perinatal lethality and heart valve abnormalities. Thus, ADAM-17 is required in VECs for proper cell regulation and ECM homeostasis in semilunar valves [183]. The age-related imbalance in hemostatic protein regulation, leading to prothrombotic mediators accumulation within the leaflet and accompanied by the mentioned ECM disarray, might favor the development and progression of aortic calcific disease [17]. In this context, the matrix Gla protein (MGP), a vitamin K-dependent inhibitor of calcification, has been reported to play an important role in the pathogenesis of valve calcific disease. γ-carboxylation of its glutamic acid residual (via vitamin K-dependent γ-carboxylase) activates the protein which in turn binds BMP-2 exerting an inhibitory activity and therefore protecting from vascular and valvular calcification. Undercarboxylated MGP circulating levels have been associated to increased mortality in aortic valve stenosis [176] and Sweatt and colleagues demonstrated reduced levels of carboxylated MGP in valve tissues of old rats establishing a pathological link between aging, ECM valve remodeling and calcific aortic disease [168]. MGP is currently under investigation as an inhibitor of vascular calcification, and lack of this “anti-calcification” protein contributes to the calcification in the aortic valve [178]. The protease calpain-1 has been recently considered as an antagonist of ECM adverse remodeling through inhibition of MMP-2 in rat aortic wall [82], but its importance in aortic leaflet remains to be clarified. ECM changes of the aortic leaflet occurring with aging are summarized in Fig. 1, and a comprehensive schema of all the reported changes together with the possible pathobiological mechanisms in both aged and diseases AV ECM is given in Table 1.

Schematic diagram showing ECM changes in aortic valve leaflets during aging and potential therapeutic approaches to counteract aging processes
Mitral valve
Normal MV structure and function rely on a more complex valvular apparatus including annulus, leaflets and chordae tendinae. Leaflets are composed of four layers, atrialis, spongiosa, fibrosa, and ventricularis. Atrialis, spongiosa and ventricularis are characterized by loose collagen, while the fibrosa is constituted by dense circumferentially aligned collagen providing tensile strength to the valve [92].
Interspersed GAGs within the other layers determine the compressive strength of the leaflet, while the elastin-rich side of the atrialis layer at the level of the inflow side permits to bear considerable stretch and allows for elastic recoil to the original shape during the phases of the cardiac cycle [96].
A specific analysis of GAGs within the valve ECM revealed high concentration of hyaluronan (HA) and hydrated chondroitin/dermatan sulfate proteoglycans in the spongiosa [158], while regularly spaced elastic fibers and circumferentially oriented collagen fibers characterized the thinner ventricularis side. Small leucine-rich proteoglycans (SLRPs) are mostly present in the collagen-rich region, in which they interconnect and provide mechanical support to the fibers [96, 158]. Additionally, there are functional differences in the composition of the free edge of the anterior leaflet, historically named “rough zone”, where the chordae tendineae attach to the valve, and the center of the leaflet referred as the “clear zone”, where no chordae are attached. The latter, experiencing tensile stresses, has a thicker fibrosa layer and shows lower concentration of GAGs, in particular less unsulfated, 6-sulfated, and 4-sulfated glucuronate than the free zone. In the rough zone, designed for compressive load absorption, the spongiosa layer is more represented and contains an overall higher concentration of HA [158]. The posterior or mural leaflet is suited for compressive load bearing and shows similar characteristics to those of the rough zone of the anterior one [69]. Chordae tendineae exert an important action during systole phase and chordal replacement is quite frequently required during surgical repair for degenerative mitral disease, mainly due to age-related alteration in chordal native structural composition. Dense collagen fibers orientated according to the direction of load characterize the core of the chorda, while elastic properties are conferred by elastin present in the outer sheath [5]. SLRPs (such as decorin and biglycan) are found interspersed within the aligned collagen fibers of the chordae [69].
Changes in structural composition accompanying the aging process are at the basis of functional reflexes on the valve itself and often translate into clinical evident morbidity requiring surgical treatment. One of the main findings in degenerated aged MV regards the thickening of the collagen-rich fibrosa layer and the increase in collagen production and remodeling [159]. In 2001, Rabkin et al. [137] perceived that the imbalance between MMPs and cysteine endoproteases (cathepsins), mainly altering collagen features, could play a role in myxomatous degeneration of MV. These observations suggest that the abnormalities of collagen result primarily from excessive collagenolytic activity rather than decreased collagen synthesis. Therefore, the deranged mechanical properties of myxomatous valves result from defective ECM and altered layered architecture. Indeed, collagen derangement has been shown to determine striking defects in the mechanical properties of myxomatous leaflets, leading to loss of tensile strength and inherent weakness. The synergistic effect of intrinsic elastomechanical defects and aberrant stresses engendered by hemodynamic cyclic load on altered and enlarged leaflets contributes to both disease pathogenesis and occurrence of postoperative failure [18]. In this context, David et al. in a multivariate analysis, reported myxomatous changes of the leaflets as the only statistically significant variable predicting the risk for reoperation [47].
In support of the hypothesis of an aberrant ECM remodeling in degenerated valve, it has been demonstrated that VICs maintain an “activated” phenotype and immunohistological co-localization of these cells with enzymes deputed to ECM turnover has been shown [161]. VICs are known to be mechanosensitive, and their synthesis of ECM components influences valve properties. Analysis of markers of VIC activation, such as α-SMA, and collagen synthesis, as heat shock protein-47 (HSP47) and prolyl 4-hydroxylase (P4H), proved that there are age-specific and valve-region-specific changes in VIC phenotype depending on the leaflet regional matrix where the VICs reside [160]. Potential mechanisms underlying tissutal degeneration in MV have been elucidated. Activation of resident interstitial valvular cells seems to be crucial in matrix degeneration. Interstitial valvular cells were found in higher number and expressing increased proteolytic enzymes, such as MMPs, that mediate ECM degradation, in degenerated valves compared with normal valves. Additionally, they have been shown to activate a catalytic state as demonstrated by their immunoreactivity for cathepsins S and K and IL-1β. Co-localization of IL-1β co- with MMP-13 and cathepsin S might additionally indicate that VICs are activated by IL-1β in response to a variety stimuli and modulate the ECM enzymatic breakdown of the connective tissue described in myxomatous valves [137]. Specifically, collagen degradation process is thought to be initiated by interstitial collagenase that operates the breakdown of type I collagen fibrillar network, leading to the generation of fragments which become further accessible to gelatinases, completing collagen catabolization [91]. Collagen type III is conversely more represented in the aged valve [159]. Elastin degradation is in turn performed by cathepsins, in particular cathepsin K, which also exhibits collagenolytic activity [165]. VICs activation and ECM degradation itself trigger the production of a cascade of extracellular and paracrine messengers, such as IL-1, boosting and perpetuating the lytic process also for other components of the leaflet, such as proteoglycans [49, 137]. Indeed, there is a reduction in unsulfated and 6-sulfated glucuronate, as well as a decrease in the ratio of chondroitin sulfate to dermatan sulfate. Conversely, decorin and biglycan have a greater representation in the valve and co-localize with collagen in attempt to lend support to the above-mentioned remodeling occurring throughout aging [158]. In a study on porcine valves, Stephens et al. reported that compressive regions of MV showed an aging-related decrease in the fraction of 4-sulfated GAGs (associated with tension), paralleled by an increase in the fraction of 6-sulfated GAGs (associated with compression), whereas the tensile regions of the MV showed the opposite pattern. The distribution of these changes is not uniform in the degenerated myxomatous MV: the rough zone of the leaflet on the ventricular side, at the attachment of the chordae, is more prone to develop disease together with the interchordal hoodings at the level of the apposition line of the leaflets (the so-called parachute change) [64]. Additionally, the middle section of the leaflets, especially the middle scallop, which is normally undergoing the strongest pressure, shows the greatest incidence of changes [64]. Additionally, the interaction and relative content of GAGs with other ECM components is important in defining the elastomechanical properties of the leaflets and the age-related alterations of ECM further demonstrate the significance of GAGs function in this context. In an animal study on mitral valve, old mice showed increased leaflet stiffness due to increased collagen and matrix fiber alignment. Interestingly in Marfan-like mice deficient in Fbn1 gene, the loss fibrillin, a crucial element in extracellular microfibrils organization and function, produced fiber misalignment and a relative increase in GAGs content, which eventually resulted in myxomatous degeneration [68]. Therefore, the loss of a leading ECM framework constituted by fibrillin, determines an excessive accumulation of GAGs leading to degenerative changes. This finding testifies the importance of an homeostatic balance between structural proteins and load absorption glycans also in non-Marfan conditions, as the deterioration or loss of important structural ECM protein occurs in aging too, as described above. Whether the deregulation of this balance is triggered by an age-related change in VICs secretory activity or by an intrinsic ECM age-related degradation needs to be clarified, but it might play a crucial role in the determinism of disease as shown in the genetic model.
Even if, with advancing age, the layers become microstructurally more delineated [161], the amount of elastin decreases, especially in subjects over the age of 50 [106]. Other important changes seen during aging regard lipids accumulation and calcification throughout the valve. These phenomena represent both a pathogenic moment for age-related degeneration of the valve and an obstacle during valve surgical repair.
Changes in the structural and functional composition of ECM translate in an alteration of the mechanical properties of the valve. Collagen modifications during aging, with particular reference to the augmented cross-linking, together with elastin fragmentation, determine an increase in the overall valve stiffness in both the radial and circumferential directions, leading to permanent tissue stretch with less crimped collagen fibers, analogously to what occurs in valves subjected to glutaraldehyde fixation [26]. Additionally, these changes in ECM composition might underlie another interesting clinical finding elucidated by the group of Levine et al. who demonstrated an adaptive enlargement of the leaflets of chronically insufficient MV in patient with dilated ventricles, therefore bearing longitudinal stress and tethering forces [21]. In support of this clinical evidence, further studies demonstrated that stress application to mitral leaflets are able to induce a switch in VICs phenotype, promoting the synthesis of different ECM patterns with consequent increase in leaflet stiffness [107]. Taken together, these data underpin the importance of age-related alterations of the ECM at the molecular level. ECM abnormalities can be thought as the true origin of the pathological changes responsible for tissutal degeneration and for mechanical/hemodynamic failure of the MV. A careful exploitation of the knowledge achieved in this context might in the future lead to the development of preventive or therapeutic strategies in cardiac disease. ECM changes occurring in mitral leaflets over time are summarized in Fig. 2, and a comprehensive schema of all the reported changes in MV ECM is given in Table 2.

Schematic diagram showing ECM changes in mitral valve leaflets and potential mechanisms underlying valve alterations during aging. Note the progression of changes in extracellular matrix composition and arrangement during aging (blue arrow). Potential therapeutic approaches to counteract age-related alterations and consequences are reported. Note that pharmacologic approaches followed by the question mark indicate only presumably effective treatments, as studies evaluating those compounds are still required
The genetics contribution
The role of genetics in the context of aging and development of valvular disease is being increasingly recognized. Genetic variations may act as a silent substrate which can be triggered by environmental variables to initiate the process of valvular degeneration. The knowledge of the genetic determinants of valvular disease may foster the development of new therapies to prevent, rather than treat, these diseases [94]. Particular interest has been lavished in the study of valvular calcification, however, the exact role of specific genetic variations is still under investigation [22, 79, 133].
Wnt signaling has multiple functions at different stages of heart development, and its signaling sustained by Wnt receptor Lrp5 and stabilized β-catenin has been associated with adult calcific valve disease in humans [7, 32, 138]. The polymorphism rs13290979 of NOTCH gene was significantly associated with adult-onset of aortic stenosis [52], probably via enhanced BMP-2 production and osteogenic differentiation of the interstitial cells [12, 109]. In a study comparing the transcriptional profiles and cellular functions of human aortic VICs and mitral VICs, a higher expression of cardiac-specific transcription factor NKX2-5 and a lower expression of TBX5 were found in aortic VICs compared to mitral VICs [167]. NKX2-5 is an important transcriptional regulator during early embryonic development regulating the conduction system [140], while TBX5 plays a key role in cardiogenesis since its mutations result in Holt–Oram syndrome [19]. TBX5 expression in developing atrioventricular valves and ventricular trabeculae has been shown to account for the structural and functional defects in mitral and tricuspid valves [28, 33] and might represent an important actor in the aging process.
Lipoprotein(a) is known to be a risk factor for coronary artery disease, and several evidences have convincingly shown its causal role in ischemic heart disease due to lipid oxidation and an induction of a prothrombotic state [40, 89]. In a large cohort of patients, one single nucleotide polymorphism in the lipoprotein(a) locus (rs10455872) was associated with aortic valve calcification, and, in prospective analyses, was related to aortic stenosis and aortic valve replacement. Two single nucleotide polymorphisms (SNPs) (rs17659543 and rs13415097) located in vicinity of the proinflammatory gene IL1F9 achieved genomewide significance for mitral annular calcification [169].
Inflammation is a prominent feature of valve calcification and plays an important role in the development of valvular calcification [42]. Therefore, many genes involved in the process of inflammation have been considered to be candidate genes predisposing to valvular calcification. IL-10 is an anti-inflammatory cytokine that is secreted by various cells inhibiting TNF-α production by activated macrophages [175] and its production is genetically regulated [182]. Polymorphisms in the IL-10 gene (rs1800871, rs1800872, rs1801082, rs1800819, rs1800592 and rs1800872) have been found associated with valvular calcification in population studies [9, 66, 123].
Low-density lipoprotein cholesterol (LDL-C) and adult atherosclerosis risk factors are important in the determinism of aortic and mitral valve disease in epidemiologic studies [163, 170], and a large cohort study confirmed that genetic predisposition to elevated LDL-C levels is linked to development of aortic calcific disease and aortic stenosis in the adulthood [153]. Indeed, LDL-C play an important role in the early calcification and mineralization phase through the formation of cholesterol micro-crystals that act as pabulum for initial calcification. Additionally, oxidized-LDL enhances the osteogenic phenotype in valvular cells [76, 126].
Clinical significance
This review underlined the relevance of ECM changes during aging process in heart valves demonstrating its influence on both their mechanical and functional properties and in the development of aged-related disease.
Several findings in this review point at the idea of aging as an underlying background for the establishment of pathology and that age-related structural changes of the ECM components can constitute a trigger for pathological alterations to occur. This might further explain the overlap in the biochemical and mechanical features seen in aged and diseased valves. The factors responsible to determine a shift of this delicate balance towards the disease are numerous and not completely identified, but genetic predisposition, environment, life-style, controllable risk factors are all relevant. From these observations a number of clinical implications and insights might be drawn.
Characterization of ECM modifications associated to aging and to valve disease is crucial in the development of valve substitutes or living tissue engineered constructs. Indeed, in the recently affirming field of detergent-based tissue decellularization for tissue engineering purposes, the importance of protecting and preserving the molecular and structural arrangement of ECM, including both proteins GAGs and regulatory molecules of matrix homeostasis, has been acknowledged [11]. Detergents have been shown to be retained in the ECM affecting cell survival rate when re-cellularization is attempted and the role of specific biochemicals to enhance matrix production and thereby creating a protective environment for the seeded cells while nourishing them, has been advocated [11]. These examples, further remark the importance of ECM and its activity. Additionally, a deep understanding of the mechanism underlying age-related ECM changes is fundamental to optimize and ameliorate currently used prosthetic valves which are widely known to undergo deterioration and aging processes. A close interplay between ECM and cells populating the valve has also been unveiled, enlightening a reciprocal influence on the development and progression of valve disease. VICs and VECs actively contribute to valve remodeling being extremely sensitive to changes of the ECM and of the surrounding hemodynamic environment. Several examples of functional VICs biosynthetic reactions aimed at maintaining valvular tissue homeostasis or compensating functional loss in leaflet mechanical properties have been reported in in vitro studies [17, 92, 107] and in clinical scenarios [21]. In light of such an adaptive mechanism inherent in the biology of the valve itself, pharmacological or molecular means of augmentation and assistance of leaflet remodeling might be developed. It has been suggested that the local delivery of biological mediators able to enhance the endogenous VICs compensating activity might be attractive and enlighten new avenues also in the surgical treatment of valve disease [157].
However, biological changes occurring at the cellular and ECM levels in the aging valve are likely to have an impact also on the clinical management of valve disease. Several pharmacological attempts have been done to inhibit or slow down valvular calcification or degeneration especially in aortic stenosis. Those approaches are mostly based on the concept of an atherosclerosis-like pathogenesis for aortic valve disease, in which an initial valvular lesion due to mechanical or increased shear stress determines lipids deposition resulting in an early subendothelial plaque which further triggers the development of the classic fibrocalcific remodeling. This phenomenon is sustained partially by VICs dysfunction, but is caused mainly by the ECM disarrangement occurring during aging. Indeed, the mentioned disproportion in collagen content and characteristics together with the reduction in elastin and the reported connectival modifications, lead to progressive loss of leaflet and aortic compliance and increase in valvular stiffness rendering the endocardium more prone to pressure or shear-mediated damage [74]. Pharmacological approaches currently tested consist in lipid-based intervention and aim to reduce the biological cascade triggered by lipid deposition [48]. Statins have been firstly used for both their lipid lowering action and for their pleiotropic anti-inflammatory and antioxidant effect with the aim to biologically stabilize the lesions and avoid fibrocalcific progressions. However, the unsatisfactory results of large clinical trials as the SEAS or the SALTIRE put on hold the initial enthusiasms about these compounds [74]. Also, statins failed to demonstrate any impact on aortic valve disease in three prospective randomized trials [37, 43, 142]. Increased presence of angiotensin-converting enzyme (ACE), angiotensin-II, and angiotensin-II type 1 receptor in fibrocalcific valves, together with the proinflammatory effect of the biological pathway sustained by macrophage-associated ACE and mast cell chymase, prompted the clinical use of ACE inhibitors in aortic stenosis. Renin-aldosterone system blockade proved to slow calcium accumulation but, disappointingly, did not show any benefit on stenosis progression [118]. Additionally, bisphosphonates have been shown to have a role in the inhibition of calcium deposition in vascular and valvular tissues in preclinical models. This effect has been claimed to be due to an inhibitory action on the release of calcium phosphate particles from bone [132]. However, nitrogen-containing bisphosphonates exert statin-like actions as they inhibit the farnesyl-pyrophosphate synthase, an enzyme distal to 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase in the cholesterol biosynthesis pathway [41]. Bisphosphonates might therefore share calcium regulating effects and pleiotropic anti-inflammatory actions resulting in appealing tools against valvular calcification. Pretreatment of bioprosthetic valve with bisphosphonate inhibited calcific degeneration [139], but, taking from the MESA study, there was an increase in the risk of calcification in women younger than 65 years [58]. In recent years, monoclonal antibodies targeting specific signal transduction pathways have been used clinically. Since one of the key regulatory roles in leaflet calcification is played by the OPG/RANK/RANKL system, denosumab (an anti-RANKL monoclonal antibody) is a promising pharmacologic approach to prevent aortic valve calcification [53].
Pharmacologic treatment against advanced glycation end products (AGEs) and their receptors has been gradually introduced in preclinical settings and in clinical research, with encouraging results in diabetic patients with cardiovascular disease [114]. In rabbits, inflammation induced by RAGE activation promotes aortic valve calcification, but both inflammation and RAGE expression can be attenuated by pioglitazone, a thiazolidinedione normally used in clinical settings for diabetes [100]. A more profound understanding of AGE role in ECM remodeling might potentially stimulate further research on pharmacologic approaches in the next years.
Aging has been associated to a shift towards a prothrombotic balance in the secretion of hemostatic protein by VECs and the structural disarray typical of old valves contribute to sequester thrombotic mediators within the leaflet. This phenomenon on a side favors the calcific nucleation inside the leaflet, but on the other exposes to an increased risk of valve thrombosis [17]. Additionally, the reduced endothelial expression and release of the leaflet accumulated vWF might justify the clinically reported augmented sensibility of elderly patients to anticoagulant drugs and their reduced clotting ability [143]. Another important lesson from aging-related ECM biology applicable in the clinical scene regards the possible detrimental effect of vitamin K-antagonists in the management of elderly patients in need of anticoagulant treatment or bearing prosthetic valves. Inhibiting vitamin K activity through coumarinic agents blunts γ-carboxylation of MGP leading to a rescue of the BMP-2-mediated osteogenic activity with eventual initiation of the calcific processes. This process has been clinically described but is still poorly understood [78]. A recent study showed that an increase in the decarboxylated, and thus inactive, form of MGP was associated with an increase in vascular calcification [50]. Accurate knowledge on these mechanisms could on a side discourage the use of standard anticoagulant in these patients, and on the other side prompt further research on both alternative anticoagulation options and on prosthetic valve design to avoid the risk of long-term calcification.
However, this delicate balance of cellular activities finds its substrate in the valve ECM which, far to behave as a mere support, is dynamically affected by hemodynamic conditions and aging and exert an active role in the interplay with VIC and VEC providing fundamental biological signaling [184]. The evidence that structural disarray induced by fixation methods in prosthetic valve might lead to premature valve degeneration and failure, supports this idea [23, 122]. Miscomprehension of the significance of ECM role in this context might explain the failure of anti-calcification approaches uniquely directed to the cellular component of valve leaflet and might also explain the contradictory results of the SEAS trial.
However, conclusions of this review are remarking the importance of the ECM in valve aging and might trigger new experimental efforts aimed at controlling or modulating age-related changes of its components to avoid premature degeneration of both native and prosthetic biological valve.
References
Abdelbaky A, Corsini E, Figueroa AL, Subramanian S, Fontanez S, Emami H, Hoffmann U, Narula J, Tawakol A (2015) Early aortic valve inflammation precedes calcification: a longitudinal FDG-PET/CT study. Atherosclerosis 238:165–172. doi:10.1016/j.atherosclerosis.2014.11.026
Agmon Y, Khandheria BK, Meissner I, Sicks JR, O’Fallon WM, Wiebers DO, Whisnant JP, Seward JB, Tajik AJ (2001) Aortic valve sclerosis and aortic atherosclerosis: different manifestations of the same disease? Insights from a population-based study. J Am Coll Cardiol 38:827–834. doi:10.1016/s0735-1097(01)01422-x
Aikawa E, Aikawa M, Libby P, Figueiredo JL, Rusanescu G, Iwamoto Y, Fukuda D, Kohler RH, Shi GP, Jaffer FA, Weissleder R (2009) Arterial and aortic valve calcification abolished by elastolytic cathepsin S deficiency in chronic renal disease. Circulation 119:1785–1794. doi:10.1161/circulationaha.108.827972
Aikawa E, Nahrendorf M, Sosnovik D, Lok VM, Jaffer FA, Aikawa M, Weissleder R (2007) Multimodality molecular imaging identifies proteolytic and osteogenic activities in early aortic valve disease. Circulation 115:377–386. doi:10.1161/circulationaha.106.654913
Akhtar S, Meek KM, James V (1999) Ultrastructure abnormalities in proteoglycans, collagen fibrils, and elastic fibers in normal and myxomatous mitral valve chordae tendineae. Cardiovasc Pathol 8:191–201 (S1054-8807(99)00004-6)
Al-Aly Z, Shao JS, Lai CF, Huang E, Cai J, Behrmann A, Cheng SL, Towler DA (2007) Aortic Msx2-Wnt calcification cascade is regulated by TNF-alpha-dependent signals in diabetic Ldlr−/− mice. Arterioscler Thromb Vasc Biol 27:2589–2596. doi:10.1161/atvbaha.107.153668
Alfieri CM, Cheek J, Chakraborty S, Yutzey KE (2010) Wnt signaling in heart valve development and osteogenic gene induction. Dev Biol 338:127–135. doi:10.1016/j.ydbio.2009.11.030
Allison MA, Cheung P, Criqui MH, Langer RD, Wright CM (2006) Mitral and aortic annular calcification are highly associated with systemic calcified atherosclerosis. Circulation 113:861–866. doi:10.1161/circulationaha.105.552844
An Y, Wang YT, Ma YT, Wulasihan M, Huang Y, Adi D, Yang YN, Ma X, Li XM, Xie X, Huang D, Liu F, Chen BD (2015) IL-10 genetic polymorphisms were associated with valvular calcification in Han, Uygur and Kazak populations in Xinjiang, China. PLoS One 10:e0128965. doi:10.1371/journal.pone.0128965
Andersen HR, Knudsen LL, Hasenkam JM (1992) Transluminal implantation of artificial heart valves. Description of a new expandable aortic valve and initial results with implantation by catheter technique in closed chest pigs. Eur Heart J 13:704–708
Andrée B, Bela K, Horvath T, Lux M, Ramm R, Venturini L, Ciubotaru A, Zweigerdt R, Haverich A, Hilfiker A (2014) Successful re-endothelialization of a perfusable biological vascularized matrix (BioVaM) for the generation of 3D artificial cardiac tissue. Basic Res Cardiol 109:441. doi:10.1007/s00395-014-0441-x
Ann EJ, Kim HY, Choi YH, Kim MY, Mo JS, Jung J, Yoon JH, Kim SM, Moon JS, Seo MS, Hong JA, Jang WG, Shore P, Komori T, Koh JT, Park HS (2011) Inhibition of Notch1 signaling by Runx2 during osteoblast differentiation. J Bone Min Res 26:317–330. doi:10.1002/jbmr.227
Armstrong EJ, Bischoff J (2004) Heart valve development: endothelial cell signaling and differentiation. Circ Res 95:459–470. doi:10.1161/01.RES.0000141146.95728.da
Assmann A, Minol JP, Mehdiani A, Akhyari P, Boeken U, Lichtenberg A (2013) Cardiac surgery in nonagenarians: not only feasible, but also reasonable? Interact CardioVasc Thorac Surg 17:340–343. doi:10.1093/icvts/ivt125
Balachandran K, Sucosky P, Jo H, Yoganathan AP (2009) Elevated cyclic stretch alters matrix remodeling in aortic valve cusps: implications for degenerative aortic valve disease. Am J Physiol Heart Circ Physiol 296:H756–H764. doi:10.1152/ajpheart.00900.2008
Balachandran K, Sucosky P, Jo H, Yoganathan AP (2010) Elevated cyclic stretch induces aortic valve calcification in a bone morphogenic protein-dependent manner. Am J Pathol 177:49–57. doi:10.2353/ajpath.2010.090631
Balaoing LR, Post AD, Liu H, Minn KT, Grande-Allen KJ (2014) Age-related changes in aortic valve hemostatic protein regulation. Arterioscler Thromb Vasc Biol 34:72–80. doi:10.1161/ATVBAHA.113.301936
Barber JE, Kasper FK, Ratliff NB, Cosgrove DM, Griffin BP, Vesely I (2001) Mechanical properties of myxomatous mitral valves. J Thorac Cardiovasc Surg 122:955–962. doi:10.1067/mtc.2001.117621
Basson CT, Bachinsky DR, Lin RC, Levi T, Elkins JA, Soults J, Grayzel D, Kroumpouzou E, Traill TA, Leblanc-Straceski J, Renault B, Kucherlapati R, Seidman JG, Seidman CE (1997) Mutations in human TBX5 [corrected] cause limb and cardiac malformation in Holt–Oram syndrome. Nat Genet 15:30–35. doi:10.1038/ng0197-30
Basta G, Corciu AI, Vianello A, Del Turco S, Foffa I, Navarra T, Chiappino D, Berti S, Mazzone A (2010) Circulating soluble receptor for advanced glycation end-product levels are decreased in patients with calcific aortic valve stenosis. Atherosclerosis 210:614–618. doi:10.1016/j.atherosclerosis.2009.12.029
Beaudoin J, Handschumacher MD, Zeng X, Hung J, Morris EL, Levine RA, Schwammenthal E (2013) Mitral valve enlargement in chronic aortic regurgitation as a compensatory mechanism to prevent functional mitral regurgitation in the dilated left ventricle. J Am Coll Cardiol 61:1809–1816. doi:10.1016/j.jacc.2013.01.064
Bella JN, Tang W, Kraja A, Rao DC, Hunt SC, Miller MB, Palmieri V, Roman MJ, Kitzman DW, Oberman A, Devereux RB, Arnett DK (2007) Genome-wide linkage mapping for valve calcification susceptibility loci in hypertensive sibships: the Hypertension Genetic Epidemiology Network Study. Hypertension 49:453–460. doi:10.1161/01.hyp.0000256957.10242.75
Bezuidenhout D, Oosthuysen A, Human P, Weissenstein C, Zilla P (2009) The effects of cross-link density and chemistry on the calcification potential of diamine-extended glutaraldehyde-fixed bioprosthetic heart-valve materials. Biotechnol Appl Biochem 54:133–140. doi:10.1042/ba20090101
Bosse Y, Mathieu P, Pibarot P (2008) Genomics: the next step to elucidate the etiology of calcific aortic valve stenosis. J Am Coll Cardiol 51:1327–1336. doi:10.1016/j.jacc.2007.12.031
Brodeur MR, Bouvet C, Bouchard S, Moreau S, Leblond J, Deblois D, Moreau P (2014) Reduction of advanced-glycation end products levels and inhibition of RAGE signaling decreases rat vascular calcification induced by diabetes. PLoS One 9:e85922. doi:10.1371/journal.pone.0085922
Broom ND, Thomson FJ (1979) Influence of fixation conditions on the performance of glutaraldehyde-treated porcine aortic valves: towards a more scientific basis. Thorax 34:166–176. doi:10.1136/thx.34.2.166
Bruel A, Oxlund H (1996) Changes in biomechanical properties, composition of collagen and elastin, and advanced glycation endproducts of the rat aorta in relation to age. Atherosclerosis 127:155–165. doi:10.1016/s0021-9150(96)05947-3
Bruneau BG, Logan M, Davis N, Levi T, Tabin CJ, Seidman JG, Seidman CE (1999) Chamber-specific cardiac expression of Tbx5 and heart defects in Holt–Oram syndrome. Dev Biol 211:100–108. doi:10.1006/dbio.1999.9298
Butcher JT, Nerem RM (2006) Valvular endothelial cells regulate the phenotype of interstitial cells in co-culture: effects of steady shear stress. Tissue Eng 12:905–915. doi:10.1089/ten.2006.12.905
Butcher JT, Penrod AM, Garcia AJ, Nerem RM (2004) Unique morphology and focal adhesion development of valvular endothelial cells in static and fluid flow environments. Arterioscler Thromb Vasc Biol 24:1429–1434. doi:10.1161/01.ATV.0000130462.50769.5a
Caceres M, Cheng W, De Robertis M, Mirocha JM, Czer L, Esmailian F, Khoynezhad A, Ramzy D, Kass R, Trento A (2013) Survival and quality of life for nonagenarians after cardiac surgery. Ann Thorac Surg 95:1598–1602. doi:10.1016/j.athoracsur.2013.02.034
Caira FC, Stock SR, Gleason TG, McGee EC, Huang J, Bonow RO, Spelsberg TC, McCarthy PM, Rahimtoola SH, Rajamannan NM (2006) Human degenerative valve disease is associated with up-regulation of low-density lipoprotein receptor-related protein 5 receptor-mediated bone formation. J Am Coll Cardiol 47:1707–1712. doi:10.1016/j.jacc.2006.02.040
Camarata T, Krcmery J, Snyder D, Park S, Topczewski J, Simon HG (2010) Pdlim7 (LMP4) regulation of Tbx5 specifies zebrafish heart atrio-ventricular boundary and valve formation. Dev Biol 337:233–245. doi:10.1016/j.ydbio.2009.10.039
Cappelli S, Epistolato MC, Vianello A, Mazzone A, Glauber M, Franzini M, Ottaviano V, Pompella A, Paolicchi A, Tanganelli P (2010) Aortic valve disease and gamma-glutamyltransferase: accumulation in tissue and relationships with calcific degeneration. Atherosclerosis 213:385–391. doi:10.1016/j.atherosclerosis.2010.08.063
Castillo JG, Anyanwu AC, El-Eshmawi A, Adams DH (2014) All anterior and bileaflet mitral valve prolapses are repairable in the modern era of reconstructive surgery. Eur J Cardiothorac Surg 45:139–145. doi:10.1093/ejcts/ezt196
Chalajour F, Treede H, Ebrahimnejad A, Lauke H, Reichenspurner H, Ergun S (2004) Angiogenic activation of valvular endothelial cells in aortic valve stenosis. Exp Cell Res 298:455–464. doi:10.1016/j.yexcr.2004.04.034
Chan KL, Teo K, Dumesnil JG, Ni A, Tam J, Investigators A (2010) Effect of lipid lowering with rosuvastatin on progression of aortic stenosis: results of the aortic stenosis progression observation: measuring effects of rosuvastatin (ASTRONOMER) trial. Circulation 121:306–314. doi:10.1161/CIRCULATIONAHA.109.900027
Chen JH, Simmons CA (2011) Cell-matrix interactions in the pathobiology of calcific aortic valve disease: critical roles for matricellular, matricrine, and matrix mechanics cues. Circ Res 108:1510–1524. doi:10.1161/circresaha.110.234237
Chen JH, Yip CY, Sone ED, Simmons CA (2009) Identification and characterization of aortic valve mesenchymal progenitor cells with robust osteogenic calcification potential. Am J Pathol 174:1109–1119. doi:10.2353/ajpath.2009.080750
Clarke R, Peden JF, Hopewell JC, Kyriakou T, Goel A, Heath SC, Parish S, Barlera S, Franzosi MG, Rust S, Bennett D, Silveira A, Malarstig A, Green FR, Lathrop M, Gigante B, Leander K, de Faire U, Seedorf U, Hamsten A, Collins R, Watkins H, Farrall M (2009) Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med 361:2518–2528. doi:10.1056/NEJMoa0902604
Corrado A, Santoro N, Cantatore FP (2007) Extra-skeletal effects of bisphosphonates. Joint Bone Spine 74:32–38 (S1297-319X(06)00247-8)
Cote N, Mahmut A, Bosse Y, Couture C, Page S, Trahan S, Boulanger MC, Fournier D, Pibarot P, Mathieu P (2013) Inflammation is associated with the remodeling of calcific aortic valve disease. Inflammation 36:573–581. doi:10.1007/s10753-012-9579-6
Cowell SJ, Newby DE, Prescott RJ, Bloomfield P, Reid J, Northridge DB, Boon NA, Scottish Aortic S, IoRI Lipid Lowering Trial (2005) A randomized trial of intensive lipid-lowering therapy in calcific aortic stenosis. N Engl J Med 352:2389–2397. doi:10.1056/NEJMoa043876
Cribier A, Eltchaninoff H, Bash A, Borenstein N, Tron C, Bauer F, Derumeaux G, Anselme F, Laborde F, Leon MB (2002) Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: first human case description. Circulation 106:3006–3008. doi:10.1161/01.cir.0000047200.36165.b8
Dainese L, Guarino A, Micheli B, Biagioli V, Polvani G, Maccari F, Volpi N (2013) Aortic valve leaflet glycosaminoglycans composition and modification in severe chronic valve regurgitation. J Heart Valve Dis 22:484–490
David Merryman W (2010) Mechano-potential etiologies of aortic valve disease. J Biomech 43:87–92. doi:10.1016/j.jbiomech.2009.09.013
David TE, Armstrong S, Sun Z, Daniel L (1993) Late results of mitral valve repair for mitral regurgitation due to degenerative disease. Ann Thorac Surg 56:7–12. doi:10.1016/0003-4975(93)90396-y (discussion 13–14)
De Vecchis R, Di Biase G, Esposito C, Ciccarelli A, Cioppa C, Giasi A, Ariano C, Cantatrione S (2013) Statin use for nonrheumatic calcific aortic valve stenosis: a review with meta-analysis. J Cardiovasc Med (Hagerstown) 14:559–567. doi:10.2459/JCM.0b013e3283587267
Decker RS, Dingle JT (1982) Cardiac catabolic factors: the degradation of heart valve intercellular matrix. Science 215:987–989. doi:10.1126/science.6818687
Delanaye P, Krzesinski JM, Warling X, Moonen M, Smelten N, Medart L, Pottel H, Cavalier E (2014) Dephosphorylated-uncarboxylated Matrix Gla protein concentration is predictive of vitamin K status and is correlated with vascular calcification in a cohort of hemodialysis patients. BMC Nephrol 15:145. doi:10.1186/1471-2369-15-145
Derbali H, Bosse Y, Cote N, Pibarot P, Audet A, Pepin A, Arsenault B, Couture C, Despres JP, Mathieu P (2010) Increased biglycan in aortic valve stenosis leads to the overexpression of phospholipid transfer protein via Toll-like receptor 2. Am J Pathol 176:2638–2645. doi:10.2353/ajpath.2010.090541
Ducharme V, Guauque-Olarte S, Gaudreault N, Pibarot P, Mathieu P, Bosse Y (2013) NOTCH1 genetic variants in patients with tricuspid calcific aortic valve stenosis. J Heart Valve Dis 22:142–149
Dweck MR, Boon NA, Newby DE (2012) Calcific aortic stenosis: a disease of the valve and the myocardium. J Am Coll Cardiol 60:1854–1863. doi:10.1016/j.jacc.2012.02.093
Eckert CE, Fan R, Mikulis B, Barron M, Carruthers CA, Friebe VM, Vyavahare NR, Sacks MS (2013) On the biomechanical role of glycosaminoglycans in the aortic heart valve leaflet. Acta Biomater 9:4653–4660. doi:10.1016/j.actbio.2012.09.031
Edep ME, Shirani J, Wolf P, Brown DL (2000) Matrix metalloproteinase expression in nonrheumatic aortic stenosis. Cardiovasc Pathol 9:281–286. doi:10.1016/s1054-8807(00)00043-0
El-Hamamsy I, Balachandran K, Yacoub MH, Stevens LM, Sarathchandra P, Taylor PM, Yoganathan AP, Chester AH (2009) Endothelium-dependent regulation of the mechanical properties of aortic valve cusps. J Am Coll Cardiol 53:1448–1455. doi:10.1016/j.jacc.2008.11.056
El Khoury G, Noirhomme P, Verhelst R, Rubay J, Dion R (2000) Surgical repair of the prolapsing anterior leaflet in degenerative mitral valve disease. J Heart Valve Dis 9:75–80 (discussion 81)
Elmariah S, Mohler ER 3rd (2010) The pathogenesis and treatment of the valvulopathy of aortic stenosis: beyond the SEAS. Curr Cardiol Rep 12:125–132. doi:10.1007/s11886-010-0089-6
Eriksen HA, Satta J, Risteli J, Veijola M, Vare P, Soini Y (2006) Type I and type III collagen synthesis and composition in the valve matrix in aortic valve stenosis. Atherosclerosis 189:91–98. doi:10.1016/j.atherosclerosis.2005.11.034
Farrar EJ, Huntley GD, Butcher J (2015) Endothelial-derived oxidative stress drives myofibroblastic activation and calcification of the aortic valve. PLoS One 10:e0123257. doi:10.1371/journal.pone.0123257
Fernandez-Pisonero I, Lopez J, Onecha E, Duenas AI, Maeso P, Crespo MS, Roman JA, Garcia-Rodriguez C (2014) Synergy between sphingosine 1-phosphate and lipopolysaccharide signaling promotes an inflammatory, angiogenic and osteogenic response in human aortic valve interstitial cells. PLoS One 9:e109081. doi:10.1371/journal.pone.0109081
Filsoufi F, Carpentier A (2007) Principles of reconstructive surgery in degenerative mitral valve disease. Semin Thorac Cardiovasc Surg 19:103–110. doi:10.1053/j.semtcvs.2007.04.003
Fondard O, Detaint D, Iung B, Choqueux C, Adle-Biassette H, Jarraya M, Hvass U, Couetil JP, Henin D, Michel JB, Vahanian A, Jacob MP (2005) Extracellular matrix remodelling in human aortic valve disease: the role of matrix metalloproteinases and their tissue inhibitors. Eur Heart J 26:1333–1341. doi:10.1093/eurheartj/ehi248
Fornes P, Heudes D, Fuzellier JF, Tixier D, Bruneval P, Carpentier A (1999) Correlation between clinical and histologic patterns of degenerative mitral valve insufficiency: a histomorphometric study of 130 excised segments. Cardiovasc Pathol 8:81–92 (S1054880798000210)
Freeman RV, Otto CM (2005) Spectrum of calcific aortic valve disease: pathogenesis, disease progression, and treatment strategies. Circulation 111:3316–3326. doi:10.1161/circulationaha.104.486738
Gaudreault N, Ducharme V, Lamontagne M, Guauque-Olarte S, Mathieu P, Pibarot P, Bosse Y (2011) Replication of genetic association studies in aortic stenosis in adults. Am J Cardiol 108:1305–1310. doi:10.1016/j.amjcard.2011.06.050
Ghazvini-Boroujerdi M, Clark J, Narula N, Palmatory E, Connolly JM, DeFelice S, Xu J, Jian B, Hazelwood S, Levy RJ (2004) Transcription factor Egr-1 in calcific aortic valve disease. J Heart Valve Dis 13:894–903
Gould RA, Sinha R, Aziz H, Rouf R, Dietz HC 3rd, Judge DP, Butcher J (2012) Multi-scale biomechanical remodeling in aging and genetic mutant murine mitral valve leaflets: insights into Marfan syndrome. PLoS One 7:e44639. doi:10.1371/journal.pone.0044639
Grande-Allen KJ, Calabro A, Gupta V, Wight TN, Hascall VC, Vesely I (2004) Glycosaminoglycans and proteoglycans in normal mitral valve leaflets and chordae: association with regions of tensile and compressive loading. Glycobiology 14:621–633. doi:10.1093/glycob/cwh076
Gupta V, Tseng H, Lawrence BD, Grande-Allen KJ (2009) Effect of cyclic mechanical strain on glycosaminoglycan and proteoglycan synthesis by heart valve cells. Acta Biomater 5:531–540. doi:10.1016/j.actbio.2008.10.009
Hanada K, Vermeij M, Garinis GA, de Waard MC, Kunen MG, Myers L, Maas A, Duncker DJ, Meijers C, Dietz HC, Kanaar R, Essers J (2007) Perturbations of vascular homeostasis and aortic valve abnormalities in fibulin-4 deficient mice. Circ Res 100:738–746. doi:10.1161/01.RES.0000260181.19449.95
Helske S, Syvaranta S, Kupari M, Lappalainen J, Laine M, Lommi J, Turto H, Mayranpaa M, Werkkala K, Kovanen PT, Lindstedt KA (2006) Possible role for mast cell-derived cathepsin G in the adverse remodelling of stenotic aortic valves. Eur Heart J 27:1495–1504. doi:10.1093/eurheartj/ehi706
Helske S, Syvaranta S, Lindstedt KA, Lappalainen J, Oorni K, Mayranpaa MI, Lommi J, Turto H, Werkkala K, Kupari M, Kovanen PT (2006) Increased expression of elastolytic cathepsins S, K, and V and their inhibitor cystatin C in stenotic aortic valves. Arterioscler Thromb Vasc Biol 26:1791–1798. doi:10.1161/01.atv.0000228824.01604.63
Hermans H, Herijgers P, Holvoet P, Verbeken E, Meuris B, Flameng W, Herregods MC (2010) Statins for calcific aortic valve stenosis: into oblivion after SALTIRE and SEAS? An extensive review from bench to bedside. Curr Probl Cardiol 35:284–306. doi:10.1016/j.cpcardiol.2010.02.002
Hinton RB Jr, Lincoln J, Deutsch GH, Osinska H, Manning PB, Benson DW, Yutzey KE (2006) Extracellular matrix remodeling and organization in developing and diseased aortic valves. Circ Res 98:1431–1438. doi:10.1161/01.RES.0000224114.65109.4e
Hirsch D, Azoury R, Sarig S, Kruth HS (1993) Colocalization of cholesterol and hydroxyapatite in human atherosclerotic lesions. Calcif Tissue Int 52:94–98. doi:10.1007/bf00308315
Hofmann B, Yakobus Y, Indrasari M, Nass N, Santos AN, Kraus FB, Silber RE, Simm A (2014) RAGE influences the development of aortic valve stenosis in mice on a high fat diet. Exp Gerontol 59:13–20. doi:10.1016/j.exger.2014.05.001
Holden RM, Sanfilippo AS, Hopman WM, Zimmerman D, Garland JS, Morton AR (2007) Warfarin and aortic valve calcification in hemodialysis patients. J Nephrol 20:417–422
Horne BD, Camp NJ, Muhlestein JB, Cannon-Albright LA (2004) Evidence for a heritable component in death resulting from aortic and mitral valve diseases. Circulation 110:3143–3148. doi:10.1161/01.cir.0000147189.85636.c3
Jian B, Jones PL, Li Q, Mohler ER 3rd, Schoen FJ, Levy RJ (2001) Matrix metalloproteinase-2 is associated with tenascin-C in calcific aortic stenosis. Am J Pathol 159:321–327. doi:10.1016/S0002-9440(10)61698-7
Jian B, Narula N, Li QY, Mohler ER 3rd, Levy RJ (2003) Progression of aortic valve stenosis: TGF-beta1 is present in calcified aortic valve cusps and promotes aortic valve interstitial cell calcification via apoptosis. Ann Thorac Surg 75:457–465. doi:10.1016/s0003-4975(02)04312-6 (discussion 465–456)
Jiang L, Zhang J, Monticone RE, Telljohann R, Wu J, Wang M, Lakatta EG (2012) Calpain-1 regulation of matrix metalloproteinase 2 activity in vascular smooth muscle cells facilitates age-associated aortic wall calcification and fibrosis. Hypertension 60:1192–1199. doi:10.1161/HYPERTENSIONAHA.112.196840
Kaden JJ, Bickelhaupt S, Grobholz R, Haase KK, Sarikoc A, Kilic R, Brueckmann M, Lang S, Zahn I, Vahl C, Hagl S, Dempfle CE, Borggrefe M (2004) Receptor activator of nuclear factor kappaB ligand and osteoprotegerin regulate aortic valve calcification. J Mol Cell Cardiol 36:57–66 (S0022282803002967)
Kaden JJ, Bickelhaupt S, Grobholz R, Vahl CF, Hagl S, Brueckmann M, Haase KK, Dempfle CE, Borggrefe M (2004) Expression of bone sialoprotein and bone morphogenetic protein-2 in calcific aortic stenosis. J Heart Valve Dis 13:560–566
Kaden JJ, Dempfle CE, Grobholz R, Fischer CS, Vocke DC, Kilic R, Sarikoc A, Pinol R, Hagl S, Lang S, Brueckmann M, Borggrefe M (2005) Inflammatory regulation of extracellular matrix remodeling in calcific aortic valve stenosis. Cardiovasc Pathol 14:80–87. doi:10.1016/j.carpath.2005.01.002
Kaden JJ, Dempfle CE, Grobholz R, Tran HT, Kilic R, Sarikoc A, Brueckmann M, Vahl C, Hagl S, Haase KK, Borggrefe M (2003) Interleukin-1 beta promotes matrix metalloproteinase expression and cell proliferation in calcific aortic valve stenosis. Atherosclerosis 170:205–211. doi:10.1016/s0021-9150(03)00284-3
Kaden JJ, Kilic R, Sarikoc A, Hagl S, Lang S, Hoffmann U, Brueckmann M, Borggrefe M (2005) Tumor necrosis factor alpha promotes an osteoblast-like phenotype in human aortic valve myofibroblasts: a potential regulatory mechanism of valvular calcification. Int J Mol Med 16:869–872. doi:10.3892/ijmm.16.5.869
Kaden JJ, Vocke DC, Fischer CS, Grobholz R, Brueckmann M, Vahl CF, Hagl S, Haase KK, Dempfle CE, Borggrefe M (2004) Expression and activity of matrix metalloproteinase-2 in calcific aortic stenosis. Z Kardiol 93:124–130. doi:10.1007/s00392-004-1021-0
Kamstrup PR, Tybjaerg-Hansen A, Steffensen R, Nordestgaard BG (2009) Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. JAMA 301:2331–2339. doi:10.1001/jama.2009.801
Kasyanov V, Moreno-Rodriguez RA, Kalejs M, Ozolanta I, Stradins P, Wen X, Yao H, Mironov V (2013) Age-related analysis of structural, biochemical and mechanical properties of the porcine mitral heart valve leaflets. Connect Tissue Res 54:394–402. doi:10.3109/03008207.2013.823954
Krane SM, Byrne MH, Lemaitre V, Henriet P, Jeffrey JJ, Witter JP, Liu X, Wu H, Jaenisch R, Eeckhout Y (1996) Different collagenase gene products have different roles in degradation of type I collagen. J Biol Chem 271:28509–28515. doi:10.1074/jbc.271.45.28509
Kunzelman KS, Cochran RP, Murphree SS, Ring WS, Verrier ED, Eberhart RC (1993) Differential collagen distribution in the mitral valve and its influence on biomechanical behaviour. J Heart Valve Dis 2:236–244
Kupari M, Laine M, Turto H, Lommi J, Werkkala K (2013) Circulating collagen metabolites, myocardial fibrosis and heart failure in aortic valve stenosis. J Heart Valve Dis 22:166–176
LaHaye S, Lincoln J, Garg V (2014) Genetics of valvular heart disease. Curr Cardiol Rep 16:487. doi:10.1007/s11886-014-0487-2
Lakatta EG (2003) Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: part III: cellular and molecular clues to heart and arterial aging. Circulation 107:490–497. doi:10.1161/01.cir.0000048894.99865.02
Latif N, Sarathchandra P, Taylor PM, Antoniw J, Yacoub MH (2005) Localization and pattern of expression of extracellular matrix components in human heart valves. J Heart Valve Dis 14:218–227
Lee JH, Meng X, Weyant MJ, Reece TB, Cleveland JC Jr, Fullerton DA (2011) Stenotic aortic valves have dysfunctional mechanisms of anti-inflammation: implications for aortic stenosis. J Thorac Cardiovasc Surg 141:481–486. doi:10.1016/j.jtcvs.2010.11.002
Lee TC, Midura RJ, Hascall VC, Vesely I (2001) The effect of elastin damage on the mechanics of the aortic valve. J Biomech 34:203–210. doi:10.1016/s0021-9290(00)00187-1
Li C, Xu S, Gotlieb AI (2013) The progression of calcific aortic valve disease through injury, cell dysfunction, and disruptive biologic and physical force feedback loops. Cardiovasc Pathol 22:1–8. doi:10.1016/j.carpath.2012.06.005
Li F, Cai Z, Chen F, Shi X, Zhang Q, Chen S, Shi J, Wang DW, Dong N (2012) Pioglitazone attenuates progression of aortic valve calcification via down-regulating receptor for advanced glycation end products. Basic Res Cardiol 107:306. doi:10.1007/s00395-012-0306-0
Lin SL, Liu CP, Young ST, Lin M, Chiou CW (2005) Age-related changes in aortic valve with emphasis on the relation between pressure loading and thickened leaflets of the aortic valves. Int J Cardiol 103:272–279. doi:10.1016/j.ijcard.2004.08.079
Litmathe J, Feindt P, Kurt M, Gams E, Boeken U (2011) Aortic valve replacement in octogenarians: outcome and predictors of complications. Hellenic J Cardiol 52:211–215
Mackie EJ, Murphy LI (1998) The role of tenascin-C and related glycoproteins in early chondrogenesis. Microsc Res Tech 43:102–110. doi:10.1002/(sici)1097-0029(19981015)43:2<102:aid-jemt3>3.3.co;2-k
Mahler GJ, Butcher JT (2011) Inflammatory regulation of valvular remodeling: the good(?), the bad, and the ugly. Int J Inflamm 2011:721419. doi:10.4061/2011/721419
Mathieu P, Voisine P, Pepin A, Shetty R, Savard N, Dagenais F (2005) Calcification of human valve interstitial cells is dependent on alkaline phosphatase activity. J Heart Valve Dis 14:353–357
McDonald PC, Wilson JE, McNeill S, Gao M, Spinelli JJ, Rosenberg F, Wiebe H, McManus BM (2002) The challenge of defining normality for human mitral and aortic valves: geometrical and compositional analysis. Cardiovasc Pathol 11:193–209 (S1054880701001028)
Merryman WD, Youn I, Lukoff HD, Krueger PM, Guilak F, Hopkins RA, Sacks MS (2006) Correlation between heart valve interstitial cell stiffness and transvalvular pressure: implications for collagen biosynthesis. Am J Physiol Heart Circ Physiol 290:H224–H231. doi:10.1152/ajpheart.00521.2005
Midwood KS, Valenick LV, Hsia HC, Schwarzbauer JE (2004) Coregulation of fibronectin signaling and matrix contraction by tenascin-C and syndecan-4. Mol Biol Cell 15:5670–5677. doi:10.1091/mbc.E04-08-0759
Miller JD, Weiss RM, Heistad DD (2011) Calcific aortic valve stenosis: methods, models, and mechanisms. Circ Res 108:1392–1412. doi:10.1161/circresaha.110.234138
Mohler ER 3rd (2000) Are atherosclerotic processes involved in aortic-valve calcification? Lancet 356:524–525. doi:10.1016/s0140-6736(00)02572-1
Mohler ER 3rd, Adam LP, McClelland P, Graham L, Hathaway DR (1997) Detection of osteopontin in calcified human aortic valves. Arterioscler Thromb Vasc Biol 17:547–552. doi:10.1161/01.atv.17.3.547
Mohler ER 3rd, Gannon F, Reynolds C, Zimmerman R, Keane MG, Kaplan FS (2001) Bone formation and inflammation in cardiac valves. Circulation 103:1522–1528. doi:10.1161/01.cir.103.11.1522
Monzack EL, Masters KS (2011) Can valvular interstitial cells become true osteoblasts? A side-by-side comparison. J Heart Valve Dis 20:449–463
Nenna A, Nappi F, Avtaar Singh SS, Sutherland FW, Di Domenico F, Chello M, Spadaccio C (2015) Pharmacologic approaches against advanced glycation end products (AGEs) in diabetic cardiovascular disease. Res Cardiovasc Med 4:e26949. doi:10.5812/cardiovascmed.4(2)2015.26949
New SE, Goettsch C, Aikawa M, Marchini JF, Shibasaki M, Yabusaki K, Libby P, Shanahan CM, Croce K, Aikawa E (2013) Macrophage-derived matrix vesicles: an alternative novel mechanism for microcalcification in atherosclerotic plaques. Circ Res 113:72–77. doi:10.1161/circresaha.113.301036
Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M (2006) Burden of valvular heart diseases: a population-based study. Lancet 368:1005–1011. doi:10.1016/S0140-6736(06)69208-8
Nozynski J, Zakliczynski M, Konecka-Mrowka D, Zakliczynska H, Pijet M, Zembala-Nozynska E, Lange D, Zembala M (2013) Advanced glycation end products and lipofuscin deposits share the same location in cardiocytes of the failing heart. Exp Gerontol 48:223–228. doi:10.1016/j.exger.2012.09.002
O’Brien KD (2006) Pathogenesis of calcific aortic valve disease: a disease process comes of age (and a good deal more). Arterioscler Thromb Vasc Biol 26:1721–1728. doi:10.1161/01.ATV.0000227513.13697.ac
O’Brien KD, Shavelle DM, Caulfield MT, McDonald TO, Olin-Lewis K, Otto CM, Probstfield JL (2002) Association of angiotensin-converting enzyme with low-density lipoprotein in aortic valvular lesions and in human plasma. Circulation 106:2224–2230. doi:10.1161/01.cir.0000035655.45453.d2
Olsson M, Dalsgaard CJ, Haegerstrand A, Rosenqvist M, Ryden L, Nilsson J (1994) Accumulation of T lymphocytes and expression of interleukin-2 receptors in nonrheumatic stenotic aortic valves. J Am Coll Cardiol 23:1162–1170. doi:10.1016/0735-1097(94)90606-8
Olsson M, Thyberg J, Nilsson J (1999) Presence of oxidized low density lipoprotein in nonrheumatic stenotic aortic valves. Arterioscler Thromb Vasc Biol 19:1218–1222. doi:10.1161/01.atv.19.5.1218
Oosthuysen A, Zilla PP, Human PA, Schmidt CA, Bezuidenhout D (2006) Bioprosthetic tissue preservation by filling with a poly(acrylamide) hydrogel. Biomaterials 27:2123–2130. doi:10.1016/j.biomaterials.2005.10.008
Ortlepp JR, Schmitz F, Mevissen V, Weiss S, Huster J, Dronskowski R, Langebartels G, Autschbach R, Zerres K, Weber C, Hanrath P, Hoffmann R (2004) The amount of calcium-deficient hexagonal hydroxyapatite in aortic valves is influenced by gender and associated with genetic polymorphisms in patients with severe calcific aortic stenosis. Eur Heart J 25:514–522. doi:10.1016/j.ehj.2003.09.006
Otto CM, Kuusisto J, Reichenbach DD, Gown AM, O’Brien KD (1994) Characterization of the early lesion of ‘degenerative’ valvular aortic stenosis. Histol immunohistochemical studies. Circulation 90:844–853. doi:10.1161/01.cir.90.2.844
Pacifici R, Carano A, Santoro SA, Rifas L, Jeffrey JJ, Malone JD, McCracken R, Avioli LV (1991) Bone matrix constituents stimulate interleukin-1 release from human blood mononuclear cells. J Clin Invest 87:221–228. doi:10.1172/jci114975
Parhami F, Morrow AD, Balucan J, Leitinger N, Watson AD, Tintut Y, Berliner JA, Demer LL (1997) Lipid oxidation products have opposite effects on calcifying vascular cell and bone cell differentiation. A possible explanation for the paradox of arterial calcification in osteoporotic patients. Arterioscler Thromb Vasc Biol 17:680–687. doi:10.1161/01.atv.17.4.680
Passmore M, Nataatmadja M, Fung YL, Pearse B, Gabriel S, Tesar P, Fraser JF (2015) Osteopontin alters endothelial and valvular interstitial cell behaviour in calcific aortic valve stenosis through HMGB1 regulation. Eur J Cardiothorac Surg 48:e20–e29. doi:10.1093/ejcts/ezv244
Patel V, Carrion K, Hollands A, Hinton A, Gallegos T, Dyo J, Sasik R, Leire E, Hardiman G, Mohamed SA, Nigam S, King CC, Nizet V, Nigam V (2015) The stretch responsive microRNA miR-148a-3p is a novel repressor of IKBKB, NF-kappaB signaling, and inflammatory gene expression in human aortic valve cells. FASEB J 29:1859–1868. doi:10.1096/fj.14-257808
Perrotta I, Moraca FM, Sciangula A, Aquila S, Mazzulla S (2015) HIF-1alpha and VEGF: immunohistochemical profile and possible function in human aortic valve stenosis. Ultrastruct Pathol 39:198–206. doi:10.3109/01913123.2014.991884
Poggio P, Grau JB, Field BC, Sainger R, Seefried WF, Rizzolio F, Ferrari G (2011) Osteopontin controls endothelial cell migration in vitro and in excised human valvular tissue from patients with calcific aortic stenosis and controls. J Cell Physiol 226:2139–2149. doi:10.1002/jcp.22549
Pohle K, Maffert R, Ropers D, Moshage W, Stilianakis N, Daniel WG, Achenbach S (2001) Progression of aortic valve calcification: association with coronary atherosclerosis and cardiovascular risk factors. Circulation 104:1927–1932. doi:10.1161/hc4101.097527
Price PA, Faus SA, Williamson MK (2001) Bisphosphonates alendronate and ibandronate inhibit artery calcification at doses comparable to those that inhibit bone resorption. Arterioscler Thromb Vasc Biol 21:817–824. doi:10.1161/01.atv.21.5.817
Probst V, Le Scouarnec S, Legendre A, Jousseaume V, Jaafar P, Nguyen JM, Chaventre A, Le Marec H, Schott JJ (2006) Familial aggregation of calcific aortic valve stenosis in the western part of France. Circulation 113:856–860. doi:10.1161/circulationaha.105.569467
Qin X, Corriere MA, Matrisian LM, Guzman RJ (2006) Matrix metalloproteinase inhibition attenuates aortic calcification. Arterioscler Thromb Vasc Biol 26:1510–1516. doi:10.1161/01.ATV.0000225807.76419.a7
Qiu H, Depre C, Ghosh K, Resuello RG, Natividad FF, Rossi F, Peppas A, Shen YT, Vatner DE, Vatner SF (2007) Mechanism of gender-specific differences in aortic stiffness with aging in nonhuman primates. Circulation 116:669–676. doi:10.1161/CIRCULATIONAHA.107.689208
Rabkin-Aikawa E, Farber M, Aikawa M, Schoen FJ (2004) Dynamic and reversible changes of interstitial cell phenotype during remodeling of cardiac valves. J Heart Valve Dis 13:841–847
Rabkin E, Aikawa M, Stone JR, Fukumoto Y, Libby P, Schoen FJ (2001) Activated interstitial myofibroblasts express catabolic enzymes and mediate matrix remodeling in myxomatous heart valves. Circulation 104:2525–2532. doi:10.1161/hc4601.099489
Rajamannan NM, Subramaniam M, Rickard D, Stock SR, Donovan J, Springett M, Orszulak T, Fullerton DA, Tajik AJ, Bonow RO, Spelsberg T (2003) Human aortic valve calcification is associated with an osteoblast phenotype. Circulation 107:2181–2184. doi:10.1161/01.cir.0000070591.21548.69
Rapoport HS, Connolly JM, Fulmer J, Dai N, Murti BH, Gorman RC, Gorman JH, Alferiev I, Levy RJ (2007) Mechanisms of the in vivo inhibition of calcification of bioprosthetic porcine aortic valve cusps and aortic wall with triglycidylamine/mercapto bisphosphonate. Biomaterials 28:690–699. doi:10.1016/j.biomaterials.2006.09.029
Reamon-Buettner SM, Borlak J (2010) NKX2-5: an update on this hypermutable homeodomain protein and its role in human congenital heart disease (CHD). Hum Mutat 31:1185–1194. doi:10.1002/humu.21345
Reddy GK (2004) AGE-related cross-linking of collagen is associated with aortic wall matrix stiffness in the pathogenesis of drug-induced diabetes in rats. Microvasc Res 68:132–142. doi:10.1016/j.mvr.2004.04.002
Rossebo AB, Pedersen TR, Boman K, Brudi P, Chambers JB, Egstrup K, Gerdts E, Gohlke-Barwolf C, Holme I, Kesaniemi YA, Malbecq W, Nienaber CA, Ray S, Skjaerpe T, Wachtell K, Willenheimer R, Investigators S (2008) Intensive lipid lowering with simvastatin and ezetimibe in aortic stenosis. N Engl J Med 359:1343–1356. doi:10.1056/NEJMoa0804602
Russmann S, Gohlke-Barwolf C, Jahnchen E, Trenk D, Roskamm H (1997) Age-dependent differences in the anticoagulant effect of phenprocoumon in patients after heart valve surgery. Eur J Clin Pharmacol 52:31–35. doi:10.1007/s002280050245
Santarpino G, Pfeiffer S, Fischlein T (2012) First-in-man implantation of a Sorin Memo 3D ring: mitral annular flexibility is still preserved at 5 years of follow-up! Int J Cardiol 159:e23–e24. doi:10.1016/j.ijcard.2011.11.072
Sarasa-Renedo A, Tunc-Civelek V, Chiquet M (2006) Role of RhoA/ROCK-dependent actin contractility in the induction of tenascin-C by cyclic tensile strain. Exp Cell Res 312:1361–1370. doi:10.1016/j.yexcr.2005.12.025
Satta J, Melkko J, Pollanen R, Tuukkanen J, Paakko P, Ohtonen P, Mennander A, Soini Y (2002) Progression of human aortic valve stenosis is associated with tenascin-C expression. J Am Coll Cardiol 39:96–101. doi:10.1016/s0735-1097(01)01705-3
Satta J, Oiva J, Salo T, Eriksen H, Ohtonen P, Biancari F, Juvonen TS, Soini Y (2003) Evidence for an altered balance between matrix metalloproteinase-9 and its inhibitors in calcific aortic stenosis. Ann Thorac Surg 76:681–688. doi:10.1016/s0003-4975(03)00529-0 (discussion 688)
Schoen FJ (1997) Aortic valve structure-function correlations: role of elastic fibers no longer a stretch of the imagination. J Heart Valve Dis 6:1–6
Schoen FJ, Levy RJ (1999) Founder’s Award, 25th Annual Meeting of the Society for Biomaterials, perspectives. Providence, RI, April 28–May 2, 1999. Tissue heart valves: current challenges and future research perspectives. J Biomed Mater Res 47:439–465. doi:10.1002/(sici)1097-4636(19991215)47:4<439:aid-jbm1>3.3.co;2-f
Seya K, Yu Z, Kanemaru K, Daitoku K, Akemoto Y, Shibuya H, Fukuda I, Okumura K, Motomura S, Furukawa K (2011) Contribution of bone morphogenetic protein-2 to aortic valve calcification in aged rat. J Pharmacol Sci 115:8–14. doi:10.1254/jphs.10198fp
Silver FH, Horvath I, Foran DJ (2002) Mechanical implications of the domain structure of fiber-forming collagens: comparison of the molecular and fibrillar flexibilities of the alpha1-chains found in types I-III collagen. J Theor Biol 216:243–254. doi:10.1006/jtbi.2002.2542
Simmons CA (2009) Aortic valve mechanics: an emerging role for the endothelium. J Am Coll Cardiol 53:1456–1458. doi:10.1016/j.jacc.2008.12.052
Smith JG, Luk K, Schulz CA, Engert JC, Do R, Hindy G, Rukh G, Dufresne L, Almgren P, Owens DS, Harris TB, Peloso GM, Kerr KF, Wong Q, Smith AV, Budoff MJ, Rotter JI, Cupples LA, Rich S, Kathiresan S, Orho-Melander M, Gudnason V, O’Donnell CJ, Post WS, Thanassoulis G (2014) Association of low-density lipoprotein cholesterol-related genetic variants with aortic valve calcium and incident aortic stenosis. JAMA 312:1764–1771. doi:10.1001/jama.2014.13959
Smith KE, Metzler SA, Warnock JN (2010) Cyclic strain inhibits acute pro-inflammatory gene expression in aortic valve interstitial cells. Biomech Model Mechanobiol 9:117–125. doi:10.1007/s10237-009-0165-2
Soini Y, Salo T, Satta J (2003) Angiogenesis is involved in the pathogenesis of nonrheumatic aortic valve stenosis. Hum Pathol 34:756–763. doi:10.1016/s0046-8177(03)00245-4
Soini Y, Satta J, Maatta M, Autio-Harmainen H (2001) Expression of MMP2, MMP9, MT1-MMP, TIMP1, and TIMP2 mRNA in valvular lesions of the heart. J Pathol 194:225–231. doi:10.1002/path.850
Spadaccio C, Gutermann H, Dion R (2014) Mitral valvuloplasty: when the art of repair meets the biological science. J Heart Valve Dis 23:299–301
Stephens EH, Chu CK, Grande-Allen KJ (2008) Valve proteoglycan content and glycosaminoglycan fine structure are unique to microstructure, mechanical load and age: relevance to an age-specific tissue-engineered heart valve. Acta Biomater 4:1148–1160. doi:10.1016/j.actbio.2008.03.014
Stephens EH, de Jonge N, McNeill MP, Durst CA, Grande-Allen KJ (2010) Age-related changes in material behavior of porcine mitral and aortic valves and correlation to matrix composition. Tissue Eng Part A 16:867–878. doi:10.1089/ten.TEA.2009.0288
Stephens EH, Durst CA, West JL, Grande-Allen KJ (2011) Mitral valvular interstitial cell responses to substrate stiffness depend on age and anatomic region. Acta Biomater 7:75–82. doi:10.1016/j.actbio.2010.07.001
Stephens EH, Grande-Allen KJ (2007) Age-related changes in collagen synthesis and turnover in porcine heart valves. J Heart Valve Dis 16:672–682
Stephens EH, Saltarrelli JG, Baggett LS, Nandi I, Kuo JJ, Davis AR, Olmsted-Davis EA, Reardon MJ, Morrisett JD, Grande-Allen KJ (2011) Differential proteoglycan and hyaluronan distribution in calcified aortic valves. Cardiovasc Pathol 20:334–342. doi:10.1016/j.carpath.2010.10.002
Stewart BF, Siscovick D, Lind BK, Gardin JM, Gottdiener JS, Smith VE, Kitzman DW, Otto CM (1997) Clinical factors associated with calcific aortic valve disease. Cardiovascular Health Study. J Am Coll Cardiol 29:630–634
Sucosky P, Balachandran K, Elhammali A, Jo H, Yoganathan AP (2009) Altered shear stress stimulates upregulation of endothelial VCAM-1 and ICAM-1 in a BMP-4- and TGF-beta1-dependent pathway. Arterioscler Thromb Vasc Biol 29:254–260. doi:10.1161/atvbaha.108.176347
Sukhova GK, Shi GP, Simon DI, Chapman HA, Libby P (1998) Expression of the elastolytic cathepsins S and K in human atheroma and regulation of their production in smooth muscle cells. J Clin Invest 102:576–583. doi:10.1172/JCI181
Sun L, Rajamannan NM, Sucosky P (2013) Defining the role of fluid shear stress in the expression of early signaling markers for calcific aortic valve disease. PLoS One 8:e84433. doi:10.1371/journal.pone.0084433
Sun W, Zhao R, Yang Y, Wang H, Shao Y, Kong X (2013) Comparative study of human aortic and mitral valve interstitial cell gene expression and cellular function. Genomics 101:326–335. doi:10.1016/j.ygeno.2013.03.004
Sweatt A, Sane DC, Hutson SM, Wallin R (2003) Matrix Gla protein (MGP) and bone morphogenetic protein-2 in aortic calcified lesions of aging rats. J Thromb Haemost 1:178–185. doi:10.1046/j.1538-7836.2003.00023.x
Thanassoulis G, Campbell CY, Owens DS, Smith JG, Smith AV, Peloso GM, Kerr KF, Pechlivanis S, Budoff MJ, Harris TB, Malhotra R, O’Brien KD, Kamstrup PR, Nordestgaard BG, Tybjaerg-Hansen A, Allison MA, Aspelund T, Criqui MH, Heckbert SR, Hwang SJ, Liu Y, Sjogren M, van der Pals J, Kalsch H, Muhleisen TW, Nothen MM, Cupples LA, Caslake M, Di Angelantonio E, Danesh J, Rotter JI, Sigurdsson S, Wong Q, Erbel R, Kathiresan S, Melander O, Gudnason V, O’Donnell CJ, Post WS (2013) Genetic associations with valvular calcification and aortic stenosis. N Engl J Med 368:503–512. doi:10.1056/NEJMoa1109034
Thanassoulis G, Massaro JM, Cury R, Manders E, Benjamin EJ, Vasan RS, Cupple LA, Hoffmann U, O’Donnell CJ, Kathiresan S (2010) Associations of long-term and early adult atherosclerosis risk factors with aortic and mitral valve calcium. J Am Coll Cardiol 55:2491–2498. doi:10.1016/j.jacc.2010.03.019
Thornton G, Frank C, Shrive N (2001) Ligament creep behavior can be predicted from stress relaxation by incorporating fiber recruitment. J Rheol 45:493–507. doi:10.1122/1.1343877
Tintut Y, Patel J, Parhami F, Demer LL (2000) Tumor necrosis factor-alpha promotes in vitro calcification of vascular cells via the cAMP pathway. Circulation 102:2636–2642. doi:10.1161/01.cir.102.21.2636
Tremble P, Chiquet-Ehrismann R, Werb Z (1994) The extracellular matrix ligands fibronectin and tenascin collaborate in regulating collagenase gene expression in fibroblasts. Mol Biol Cell 5:439–453. doi:10.1091/mbc.5.4.439
Tucker RP, Chiquet-Ehrismann R (2009) The regulation of tenascin expression by tissue microenvironments. Biochim Biophys Acta 1793:888–892. doi:10.1016/j.bbamcr.2008.12.012
Turner DM, Williams DM, Sankaran D, Lazarus M, Sinnott PJ, Hutchinson IV (1997) An investigation of polymorphism in the interleukin-10 gene promoter. Eur J Immunogenet 24:1–8. doi:10.1111/j.1365-2370.1997.tb00001.x
Ueland T, Gullestad L, Dahl CP, Aukrust P, Aakhus S, Solberg OG, Vermeer C, Schurgers LJ (2010) Undercarboxylated matrix Gla protein is associated with indices of heart failure and mortality in symptomatic aortic stenosis. J Intern Med 268:483–492. doi:10.1111/j.1365-2796.2010.02264.x
Vahanian A, Iung B (2012) The new ESC/EACTS guidelines on the management of valvular heart disease. Arch Cardiovasc Dis 105:465–467. doi:10.1016/j.acvd.2012.09.001
Venardos N, Bennett D, Weyant MJ, Reece TB, Meng X, Fullerton DA (2015) Matrix Gla protein regulates calcification of the aortic valve. J Surg Res. doi:10.1016/j.jss.2015.04.076
Venardos N, Nadlonek NA, Zhan Q, Weyant MJ, Reece TB, Meng X, Fullerton DA (2014) Aortic valve calcification is mediated by a differential response of aortic valve interstitial cells to inflammation. J Surg Res 190:1–8. doi:10.1016/j.jss.2014.03.051
Vyavahare N, Ogle M, Schoen FJ, Zand R, Gloeckner DC, Sacks M, Levy RJ (1999) Mechanisms of bioprosthetic heart valve failure: fatigue causes collagen denaturation and glycosaminoglycan loss. J Biomed Mater Res 46:44–50. doi:10.1002/(sici)1097-4636(199907)46:1<44:aid-jbm5>3.3.co;2-4
Wang D, Zeng Q, Song R, Ao L, Fullerton DA, Meng X (2014) Ligation of ICAM-1 on human aortic valve interstitial cells induces the osteogenic response: a critical role of the Notch1-NF-kappaB pathway in BMP-2 expression. Biochim Biophys Acta 1843:2744–2753. doi:10.1016/j.bbamcr.2014.07.017
Westendorp RG, Langermans JA, Huizinga TW, Elouali AH, Verweij CL, Boomsma DI, Vandenbroucke JP (1997) Genetic influence on cytokine production and fatal meningococcal disease. Lancet 349:170–173. doi:10.1016/s0140-6736(05)63055-3
Wilson CL, Gough PJ, Chang CA, Chan CK, Frey JM, Liu Y, Braun KR, Chin MT, Wight TN, Raines EW (2013) Endothelial deletion of ADAM17 in mice results in defective remodeling of the semilunar valves and cardiac dysfunction in adults. Mech Dev 130:272–289. doi:10.1016/j.mod.2013.01.001
Yang X, Fullerton DA, Su X, Ao L, Cleveland JC Jr, Meng X (2009) Pro-osteogenic phenotype of human aortic valve interstitial cells is associated with higher levels of Toll-like receptors 2 and 4 and enhanced expression of bone morphogenetic protein 2. J Am Coll Cardiol 53:491–500. doi:10.1016/j.jacc.2008.09.052
Yip CY, Chen JH, Zhao R, Simmons CA (2009) Calcification by valve interstitial cells is regulated by the stiffness of the extracellular matrix. Arterioscler Thromb Vasc Biol 29:936–942. doi:10.1161/atvbaha.108.182394
Zeng Q, Song R, Ao L, Weyant MJ, Lee J, Xu D, Fullerton DA, Meng X (2013) Notch1 promotes the pro-osteogenic response of human aortic valve interstitial cells via modulation of ERK1/2 and nuclear factor-kappaB activation. Arterioscler Thromb Vasc Biol 33:1580–1590. doi:10.1161/ATVBAHA.112.300912
Zhan Q, Song R, Zeng Q, Yao Q, Ao L, Xu D, Fullerton DA, Meng X (2015) Activation of TLR3 induces osteogenic responses in human aortic valve interstitial cells through the NF-kappaB and ERK1/2 pathways. Int J Biol Sci 11:482–493. doi:10.7150/ijbs.10905
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This work was supported in part by MIUR-PRIN “Engineering physiologically and pathologically relevant organ models for the investigation of age-related diseases” (Grant # 2010J8RYS7).
Conflict of interest
None declared.
Rights and permissions
About this article

Cite this article
Spadaccio, C., Mozetic, P., Nappi, F. et al. Cells and extracellular matrix interplay in cardiac valve disease: because age matters. Basic Res Cardiol 111, 16 (2016). https://doi.org/10.1007/s00395-016-0534-9
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00395-016-0534-9