
Abstract
Purpose
It is unclear how dietary intake influences the ovarian cancer. The present paper sets out to systematically review and meta-analyze research on dietary intake to identify cases having high- or low-risk ovarian cancer.
Methods
Scopus, PubMed, and Wiley Online Libraries were searched up to the date November 24, 2019. Two reviewers were requested to independently extract study characteristics and to assess the bias and applicability risks with reference to the study inclusion criteria. Meta-analyses were performed to specify the relationship between dietary intake and the risk of ovarian cancer identifying 97 cohort studies.
Results
No significant association was found between dietary intake and risk of ovarian cancer. The results of subgroup analyses indicated that green leafy vegetables (RR = 0.91, 95%, 0.85–0.98), allium vegetables (RR = 0.79, 95% CI 0.64–0.96), fiber (RR = 0.89, 95% CI 0.81–0.98), flavonoids (RR = 0.83, 95% CI 0.78–0.89) and green tea (RR = 0.61, 95% CI 0.49–0.76) intake could significantly reduce ovarian cancer risk. Total fat (RR = 1.10, 95% CI 1.02–1.18), saturated fat (RR = 1.11, 95% CI 1.01–1.22), saturated fatty acid (RR = 1.19, 95% CI 1.04–1.36), cholesterol (RR = 1.13, 95% CI 1.04–1.22) and retinol (RR = 1.14, 95% CI 1.00–1.30) intake could significantly increase ovarian cancer risk. In addition, acrylamide, nitrate, water disinfectants and polychlorinated biphenyls were significantly associated with an increased risk of ovarian cancer.
Conclusion
These results could support recommendations to green leafy vegetables, allium vegetables, fiber, flavonoids and green tea intake for ovarian cancer prevention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
As the seventh most frequently occurring cancer in women, ovarian cancer accounts for 295,414 new cases and 184,799 deaths annually [1] with the scientific history of the disease dating back to more than 150 years ago. Ovarian cancer is subsumed under the category of chronic and degenerative diseases [2]. Epithelial ovarian cancer falls into the category of five histologic subtypes having various molecular alterations, risk factors, cellular origin, pathogenesis, gene expression, and prognosis with the main ovarian cancer characterized by being high-grade serous, clear cell, endometrioid, mucinous and low-grade serous subtypes. Partly due to the heterogeneous nature of ovarian cancer, its etiology is unclear. Numerous carcinogenic mechanisms have been considered for epithelial ovarian cancer. From among these mechanisms, one can refer to incessant ovulation and inflammation, low immunity, hormonal changes, heightened cell senescence and varying glucose homeostasis, de novo fatty acid synthesis and uncontrolled reactive oxygen production. Experimental investigations suggest that surface ovarian epithelial cells contain high 8-oxoguanine levels during ovulation as one of the most salient mutagenic lesions in DNA [3,4,5,6,7,8,9,10,11]. Major molecular mechanisms and signaling pathways are involved in ovarian cancer cell development. The growth factor pathways, the activator of transcription 3 pathway, the nuclear factor kappa-light-chain enhancer of activated B cells (NF-kB) pathway, the proto-oncogene tyrosine protein kinase Src pathway, the mitogen-activated protein kinase pathway, the ErbB activation pathway, the lysophosphatidic acid pathway and the phosphatidylinositol 3-kinases (PI3K) pathway are implicated in ovarian cancer cell growth and differentiation, cell movement and apoptosis, autophagy, metabolic programing, survival, transcription regulation, and angiogenesis, and are directly linked to tumor suppressor and oncogenic genes in ovarian cancer [12,13,14].
Factors related to reproduction, e.g., high parity, oral contraceptive use, high lactation duration, tubal ligation, hysterectomy, oophorectomy, salpingectomy and bilateral salpingo-oophorectomy, have been shown to be related to a lower ovarian cancer risk. Some researchers recommend transvaginal ultrasound together with the serum-based marker CA-125 as a primary ovarian cancer screening tool [3, 7, 15,16,17,18,19].
Numerous factors have been shown to be related to a higher ovarian cancer risk. These factors include obesity, old age, children later or not having a full-term pregnancy, treatment of fertility, post menopause hormone therapy, family history of ovarian cancer, breast cancer, or colorectal cancer, family cancer syndrome, hereditary breast and ovarian cancer syndrome, Peutz–Jeghers syndrome, MUTYH-associated polyposis, PTEN tumor hamartoma syndrome, hereditary non-polyposis colon cancer, hypo activity, smoking and alcohol use. Moreover, some factors exert unknown effects on ovarian cancer risk, e.g., diet, androgens and talcum powder [19,20,21,22,23].
The effect of dietary intake on ovarian cancer is unclear [23]. Since 2013, two reviews assessing the relationship between dietary intake and ovarian cancer have been published [24, 25]. Nevertheless, the inconclusive results necessitated more detailed and in-depth investigations of relationships of dietary intake and ovarian cancer risk. Thus, the present systematic and meta-analysis review aims to furnish an overview of the relation between dietary intake and ovarian cancer.
Methods
The present meta-analysis has been planned, conducted, and reported in accordance with PRISMA (the Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [26].
Inclusion criteria for this review
The inclusion criteria for studies included the following: (1) the research design was a cohort study; (2) the relationship between dietary intake and ovarian cancer was investigated; and (3) the relative risk or hazard ratio with corresponding 95% confidence interval (CI) between the dietary intake and the ovarian cancer risk was documented. As exclusion criteria, conference proceedings, dissertations or abstracts only were excluded.
Search strategies
Related articles from the electronic databases Scopus, PubMed and Wiley Online Library were screened up to the date November 24, 2019. The general search terms of exposure for each of the databases are presented in the Supplementary Tables S1-3 in accordance with WCRF (the World Cancer Research Fund) Specification Manual [27]. References for the articles retrieved and previous systematic reviews investigating the relationship between dietary intake and ovarian cancer risk were searched manually. EndNote X9 citation software was used to import citations (Clarivate Analytics; Boston, MA, USA) as a result of which 25,722 articles were imported into a web-based citation screening platform leaving 18,864 articles for review.
Selection of studies
Subsequent to the removal of duplicates, titles and abstracts of articles were reviewed to specify their relevance with respect to the inclusion and exclusion criteria. In case initial screening revealed suitability of publications, full texts were examined.
Data extraction and management
Data extracted from each study independently by the two researchers AK and FA included: author, year of publication, region/country, study name, investigation period, follow-up period, number of cases and participants, age of participants, dietary assessment and exposure, risk estimates, study outcomes and confounder adjustments.
Assessment of risk of bias and applicability in included studies
The Newcastle–Ottawa Scale (NOS; http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp) was employed to assess the quality of studies included. A maximum of 9 stars could be awarded to each study and a maximum of 2 stars for comparability. The 2 authors (AK and FA) independently assessed the risk of bias. The senior author (AFAR) was consulted with regard to the discrepancies to resolution purposes.
Statistical analysis
The association between dietary intake and the risk of ovarian cancer were our main analytical object. Dietary in this meta-analysis was defined as fruits, vegetables and mushrooms, meats and eggs, dairy products, fats and fatty acids, alcohol, micro/macronutrients and plant-based bioactive compounds, coffee and tea, non-food contaminants and sweets and carbohydrate foods. The random-effects model was used when data were significantly heterogeneous and the fixed-effect model was used when data were homogeneous. Heterogeneity was investigated using the Q and the I2 statistical tests with P value. P < 0.050 was considered statistically significant. Subgroup analyses stratified by types of dietary for each group and geographic region/country were carried out to investigate potential sources of heterogeneity. The STATA/MP 15.1 software (StataCorp LP, College Station, TX, USA) was used for statistical analyses.
Results
Literature retrieval results
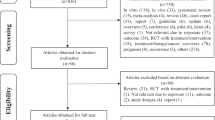
The literature searches initially produced 25,722 records: 11,434 PubMed, 9598 Scopus and 4690 from Wiley Online Library citations. Subsequent to duplicate removal (n = 6858) and application of exclusion criteria (n = 18,864), 114 records were identified as being qualified for full-text review from which 18 were excluded after the application of inclusion and exclusion criteria. The Supplementary Table S4 depicts a list of the excluded full-text articles and justifications for exclusion. This finally led to the inclusion of a total of 97 studies [4, 8, 18, 20, 28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120]. Figure 1 shows detailed information on the selection process.

Study selection process and results in accordance with the PRISMA framework
Characteristics of included studies
The included studies incorporated data analyses using 97 cohorts covering the European Prospective Investigation into Cancer and Nutrition (EPIC) in the Europe (6 studies) [4, 46, 59, 90, 93, 108], Australian Ovarian Cancer Study (AOCS) in the Australia (1 study) [8], Multi-centers studies in the North America and Europe (6 studies) [18, 48, 55, 71, 78, 85], Japan Collaborative Cohort (JACC) Study in the Japan (1 study) [20], NLCS in the Netherlands (7 studies) [28, 39, 44, 54, 73, 96, 117], UK Women’s Cohort Study (UKWCS) in the United Kingdom (1 study) [29], EPIC and the Netherlands Cohort Study (NLCS) in the Netherlands (1 study) [30], Women’s Lifestyle and Health Cohort Study (WLH) in the Sweden (1 study) [31], A Cohort of American Women in the United States (1 study) [32], Oxford Vegetarian Study (OVS) and the EPIC-Oxford Cohort in the United Kingdom (1 study) [33], National Institutes of Health (NIH)-AARP (American Association for Retired Persons) Diet and Health Study in the United States (8 studies) [34, 45, 47, 52, 61, 64, 112, 119], California Teachers Study (CTS) in the United States (3 studies) [35, 36, 69], The Nurses’ Health Study (NHS) in the United States (7 studies) [37, 41, 42, 56, 67, 72, 115], Adventist Health Study (AHS) in the United States (1 study) [38], Swedish Mammography Cohort (SMC) in the Sweden (10 studies) [40, 49, 57, 74, 76, 98, 99, 107, 114, 116], Iowa Women’s Health Study (IWHS) in the United States (8 studies) [43, 75, 87, 95, 101, 106, 109, 118], Mobile Health Clinic of the Social Insurance Institution in the Finland [50], The NHS and NHS II in the United States (5 studies) [51, 58, 79,80,81], Breast Cancer Detection Demonstration Project (BCDDP) Follow-up Cohort in the United States (1 study) [53], Norwegian Counties Study in the Norway (1 study) [60], Women’s Health Initiative (WHI) in the United States (3 studies) [62, 83, 110], Canadian Study of Diet, Lifestyle, and Health (CSDLH) in the Canada (3 studies) [63, 77, 88], Japan Public Health Center-based Prospective (JPHC) Study in the Japan (2 studies) [65, 105], Million Women Study (MWS) in the United Kingdom (1 study) [66], Canadian National Breast Screening Study (CNBSS) in the Canada (6 studies) [68, 70, 84, 86, 97, 120], Women’s Health Study (WHS) in the United States (1 study) [82], Multiethnic Cohort Study (MEC) in the United States (1 study) [89], Norwegian Women and Cancer (NOWAC) Study in the Norway (1 study) [91], Prostate, Lung, Colorectal, and Ovarian (PLCO) Prospective Study in the United States (1 study) [92], Västerbotten Intervention Project (VIP) in the Sweden (1 study) [94], Prospective Cohort Study in Hangzhou in the China (1 study) [100], Norwegian Prospective Study in the Norway (2 study) [102, 103], Seventh-Day Adventists Cohort Study in the United States (1 study) [104], Diet, Cancer and Health (DCH) Cohort in the Denmark (1 study) [111] and (EPIC)-Norfolk Study in the United Kingdom (1 study) [113]. The studies covered periods from 1984 to 2019, with populations ranging from 254 to 1,280,296. Sixty-five studies incorporated participants whose age was both lower and higher than 50 years, 30 studies included people whose age exceeded 50 years and 2 studies were 30–49 years old. Most studies represented incident ovarian cancer outcome, 4 studies had ovarian cancer death outcome [20, 90, 100, 104] and only one study depicted ovarian cancer incidence and death outcome [70]. Thirty-seven studies presented data on relationships for histologic and ovarian cancer subtypes [4, 18, 30, 31, 36, 37, 40, 41, 46, 48, 49, 51, 54,55,56,57,58,59, 61, 62, 64, 67, 71, 72, 76, 78,79,80, 85, 96, 98, 99, 108, 112, 114,115,116]. Thirteen studies furnished data on menopausal status [29, 30, 36, 38, 48, 51, 58, 67, 80, 84, 105, 115, 120]. Nineteen studies conducted the relationship between dietary intake and ovarian cancer risk in postmenopausal women participating [28, 39, 43, 44, 54, 62, 63, 73, 75, 83, 87, 95, 96, 101, 106, 109,110,111, 117].
Assessment of risk of bias
Supplementary Tables S5–13 depict the assessment of risk of bias for the 97 cohort studies undergoing additional meta-analyses. Most studies did not include any missing outcome data, or presented missing data as being insignificant for the study to be assessed at high-risk of attrition bias. The entirety of the included studies was deemed to be at low risk of selective reporting bias considering the fact that all the outcomes mentioned in method sections were incorporated in the results.
Intake of fruits, vegetables and mushrooms and ovarian cancer risk
Supplementary Table S14 shows that 20 cohort studies [4, 8, 18, 20, 28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43] were considered in meta-analysis of the relationship between intake of fruits, vegetables and mushrooms and ovarian cancer risk. Comparison of the highest and lowest intake categories yielded a summary RR of 0.98 (95% CI 0.91–1.05) without heterogeneity (Pheterogeneity = 0.866, I2 = 0.0%) (Fig. 2a). These results suggested no association between intake of fruits, vegetables and mushrooms and ovarian cancer risk (P = 0.513). Results of the subgroup analyses were consistent with the findings of the main analysis; there was no association between intake of fruits and risk of ovarian cancer (Table 1). From among the 20 studies on fruit consumption, 5 revealed a significantly lower risk of ovarian cancer [28, 30, 32, 33, 38] while 15 [4, 8, 18, 20, 29, 31, 34,35,36,37, 39,40,41,42,43] reported non-significant relationships. The results of subgroup analyses indicated that green leafy vegetables (RR = 0.91, 95% CI 0.85–0.98, Pheterogeneity = 0.115, I2 = 35.5%, P = 0.009) and allium vegetables (RR = 0.79, 95% CI 0.64–0.96, Pheterogeneity = 0.996, I2 = 0.0%, P = 0.021) intake could significantly decrease ovarian cancer risk (Table 1). However, there was no significant association between intake of fruits, vegetables and mushrooms and ovarian cancer when subgroup analysis was performed according to geographic location/country (Table 2). From among 20 studies on vegetable consumption, 7 reported a significantly lower risk of ovarian cancer [8, 28, 32, 33, 40, 41, 43], while 11 [4, 18, 29,30,31, 34,35,36,37,38,39] reported no significant relationships. Fairfield et al. [42] reported a moderate risk reduction with high intake of vegetable but this was not found to be statistically significant. In one study [20], a lower ovarian cancer risk was reported with soy bean curd (tofu) consumption while observing a significant higher risk with Chinese cabbage. A lower risk of ovarian cancer was reported with green leafy vegetables [8, 38,39,40, 43], bananas [30], yellow and cruciferous vegetables [32], e.g., broccoli [37] and cabbage and carrots, beets [40] and tomato [38, 40]. Considering the 2 studies [4, 29] on mushrooms consumption, 1 [29] was found to reveal a significantly higher risk, while the other [4] reported no significant relationships. The data are indicative of the fact that no significant associations with histologic subtypes of ovarian cancer are reported with fruit, vegetable and mushroom consumption (Table 1) [4, 18, 30]. No significant relationships were observed with menopausal status and intake of fruits, vegetables and mushrooms RR = 089, 95% CI 0.74–1.07; P = 0.229) [29, 30, 38]. For tomatoes and other fruits, the statistically significant relatively strong effects were larger among postmenopausal women [38].

Forest plot for cohort studies evaluating pooled relative risk (RR) of intake of a fruits, vegetables and mushrooms; b meats and eggs and ovarian cancer risk. OC ovary cancer
Intake of meats and eggs and ovarian cancer risk
Supplementary Table S15 outlines the 17 cohort studies [8, 20, 29, 30, 32, 33, 36, 38, 41, 43,44,45,46,47,48,49,50] considered in the meta-analysis of the relationship between intake of meats and eggs and the risk of ovarian cancer. Figure 2b, reported an association between intake of meats and eggs and the risk of ovarian cancer, and there was no significant increase association (RR = 1.06, 95% CI 0.97–1.16, Pheterogeneity = 0.277, I2 = 15.1%, P = 0.196). A moderate risk increasing was found with intake of red meat, pork, eggs and dried and salted fish and canned tuna but this was not statistically significant. The results indicated that a moderate risk reduction was obtained by intake of fish and fish dishes (Table 1). Results of the subgroup analyses indicated that intake of meats and eggs could increase ovarian cancer risk in United States populations (RR = 1.15, 95% CI 1.10–1.30, Pheterogeneity = 0.426, I2 = 0.5%, P = 0.028) (Table 2). From among the 14 studies [8, 20, 29, 30, 32, 38, 41, 43,44,45,46,47, 49, 50] on total meat consumption, 2 studies revealed a significant higher risk, especially the red and cured or processed meat subgroups [32] and total meat, total beef, poultry [38], and fried meat [50], while 11 [8, 20, 29, 30, 41, 43,44,45,46,47, 49] reported no significant relationships. Two [8, 33] of the 11 studies [8, 20, 29, 30, 32, 33, 38, 44,45,46, 49] on fish consumption and the risk of ovarian cancer found significantly lower risks, while 6 [29, 30, 32, 44, 46, 49] reported no significant relationships. Three studies also found a significant higher risk with dried or salted fish consumption [20], fish [38] and canned tuna [45]. From among the 9 studies [20, 29, 36, 38, 41, 43, 46, 48, 49] on egg consumption, 1 study [43] revealed a statistically significant higher risk, while 7 [20, 29, 36, 38, 46, 48, 49] reported no significant relationships. Bertone et al. [41] reported higher risks of ovarian cancer with frequent egg intake. No significant relationships were reported between histologic subtypes of ovarian cancer and meat and egg consumption [36, 48, 49]. A statistically significant relationship was obtained between serous tumors and total meat and poultry. The RR for total meat and poultry intake was 1.29 (95% CI 1.11–1.50, P = 0.001), suggesting a significant increase association between total meat and poultry consumption and serous ovarian cancer risk [46]. No significant relationships were reported with menopausal status and meat and egg consumption (RR = 1.64, 95% CI 0.83–3.24, P = 0.155) [29, 38]. The statistically significant strong effect reported for meat was larger for postmenopausal women [38].
Intake of dairy products and ovarian cancer risk
The meta-analysis included 17 cohort studies [8, 20, 29, 30, 32, 36, 38, 41, 43, 46, 51,52,53,54,55,56,57] on the relationship between intake of dairy products and the risk of ovarian cancer as detailed in Supplementary Table S16. Dietary intake of dairy products was not significantly associated with the risk of ovarian cancer (RR = 1.01, 95% CI 0.94–1.08, Pheterogeneity = 0.881, I2 = 0.0%, P = 0.762) (Fig. 3a). Subgroup analyses revealed a moderate risk increasing of ovarian cancer with the intake of high-fat dairy products and total cheese; while, a moderate risk reduction was achieved with the intake of low-fat dairy products (Table 1). However, there was no significant association between intake of dairy products and the risk of ovarian cancer when subgroup analysis was performed according to geographic location/country (Table 2). From among the 17 studies on consumption of dairy products, 9 [8, 20, 29, 30, 36, 41, 46, 52, 54] reported no significant relationships. Two studies reported a statistically significant higher risk of dairy products especially all types of milk [32], skim milk and cheese [43] consumption and ovarian cancer. A higher ovarian cancer risk was reported with larger whole fat milk and cheese intake. A low protective relationship has also been reported with low fat milk [38]. Two studies revealed that the intake of lactose was positively but not significantly related with an higher risk [43, 55] with the other 2 studies showing that the intake of lactose was inversely related to ovarian cancer risk [39, 51]. Larger intake of total dairy food was found to be related to a statistically significant lower ovarian cancer risk. A decreased ovarian cancer risk was reported with frequent butter, ice cream, and 2% milk intake [53]. Table 3 presents the results of histologic subtypes and ovarian cancer risk. No significant relationships were found between histologic subtypes of ovarian cancer and dairy product consumption (Table 3) [41, 51, 54,55,56,57]. One study suggested that high lactose or total milk intake was associated with higher endometrioid ovarian cancer risk [51]. Two studies demonstrated that high lactose and dairy product intake, especially milk, is related to the high serous ovarian cancer risk [56, 57]. The RR for intake of dairy products was 0.94 (95% CI 0.80–1.12, P = 0.507), suggesting a no significant association between dairy product consumptions and menopausal status [29, 38, 51]. In the case of cheese, the statistically significant relatively strong effect was larger among postmenopausal women [38].

Forest plot for cohort studies evaluating pooled relative risk (RR) of intake of a dairy products; b dietary fats and fatty acids and ovarian cancer risk. OC ovary cancer
Intake of dietary fats and fatty acids and ovarian cancer risk
Supplementary Table S17 outlines the 18 cohort studies [8, 28,29,30, 32, 35, 36, 38, 41, 43, 44, 48, 51, 54, 58,59,60,61] incorporated in the meta-analysis of the relationship between dietary fats and fatty acids consumption and the risk of ovarian cancer. Intake of dietary fats and fatty acids was not statistically significantly associated with an increased risk of ovarian cancer (RR = 1.06, 95% CI 0.99–1.13, Pheterogeneity = 0.849, I2 = 0.0%, P = 0.084) (Fig. 3b). The subgroup analyses also showed total fat (RR = 1.10, 95% CI 1.02–1.18, Pheterogeneity = 0.435, I2 = 0.6%, P = 0.009), saturated fat (RR = 1.11, 95% CI 1.01–1.22, Pheterogeneity = 0.380, I2 = 6.6%, P = 0.023), saturated fatty acid (RR = 1.19, 95% CI 1.04–1.36, Pheterogeneity = 0.520, I2 = 0.0%, P = 0.010) and cholesterol (RR = 1.13, 95% CI 1.04–1.22, Pheterogeneity = 0.263, I2 = 21.0%, P = 0.002) intake could significantly increase ovarian cancer risk (Table 1). In the subgroup analysis according to geographic location/country, a statistically increased risk for ovarian cancer was observed in the European populations (RR = 1.13, 95% CI 1.00–1.27, Pheterogeneity = 0.821, I2 = 0.0%, P = 0.045) (Table 2). From among the 18 studies on consumption of dietary fats and fatty acids, 12 [28, 29, 32, 35, 36, 38, 41, 43, 48, 51, 59, 60] revealed non-significant relationships with ovarian cancer. Four studies reporting a significant high risk of cholesterol [30, 58], polyunsaturated and saturated fat [30], trans unsaturated fatty acids [44], total dietary fat intake especially from animal sources [58, 61] and ovarian cancer. A weak positive relationship was observed for the intake of polyunsaturated fat [61]. The highest dairy fat intake quintile was related to higher risks as compared with the lowest intake quintile while a positive relationship was not observed for serous epithelial ovarian cancer [54]. A lower risk of ovarian cancer was reported with poly- to mono-unsaturated fat ratio [8] and unsaturated fat [30]; while, a positive relationship was reported between intake of animal and saturated fat [48] and polyunsaturated fat [59] and ovarian cancer risk. Overall, no significant associations were obtained between histologic subtypes of ovarian cancer and consumption of dietary fats and fatty acids (Table 3) [30, 41, 48, 54, 58, 59, 61]. The high dairy fat intake was related to a very low significance increase with the risk of serous ovarian cancer [41]. The positive association between animal fat and cholesterol intakes and risk of ovarian cancer were similar for both serous tumors and non-serous tumors. In addition, the positive association between saturated fat intake and risk of ovarian cancer was observed for non-serous tumors [58]. Total fat and fat originating from animal sources were positively related with the risk of serous ovarian cancer [61]. No significant relationships with menopausal status were reported of intake of dietary fats and fatty acids (RR = 1.03, 95% CI 0.93–1.15, P = 0.532) [29, 30, 38, 48, 51, 58]. A positive association between saturated fat intake and risk of ovarian cancer was reported among postmenopausal women [30].
Alcohol intake and ovarian cancer risk
As Supplementary Table S18 depicts, the meta-analysis of the relation between the intake of alcohol and the risk of ovarian cancer included 20 cohort studies [20, 29, 30, 32, 43, 62,63,64,65,66,67,68,69,70,71,72,73,74,75,76]. Figure 4a, reported no significant association between alcohol intake and the risk of ovarian cancer (RR = 1.00, 95% CI 0.90–1.00, Pheterogeneity = 0.601, I2 = 0.0%, P = 0.985). Subgroup analyses indicated that the intake of wines and spirits was at a moderately increased risk of ovarian cancer, but not statistically significant (Table 1). Subgroup analysis by geographic location/country showed that there was no significant association between the intake of alcohol and the risk of ovarian cancer (Table 2). From among the 20 studies on the intake of alcohol, 11 studies [20, 29, 30, 32, 63, 65,66,67,68, 71, 73] revealed non-significant relationships with 1 study [43] finding decreased risk of ovarian cancer with the intake of alcohol. Chang et al. [69] also reported that the intake of alcohol is unlikely to influence the risk of ovarian cancer, while drinking wine was related to the higher ovarian cancer risk in the year prior to the baseline. Larsson and Wolk [74] asserted that light-to-moderate consumption of wine lowered the ovarian cancer risk. The relationship between alcohol and ovarian cancer varies with the total folate [70, 76] or not by the folate, methionine and pyridoxine intake [72]. Non-significant relationships were found between the histologic subtypes of ovarian cancer and alcohol consumption (Table 3) [62, 64, 71, 76]. Lower consistencies in subtype-specific relationships were reported in terms of the quantity of alcohol intake [64]. The intake of alcohol had a weak positive association with risk of serous ovarian cancer [62]. Non-significant associations were reported between menopausal status and the intake of alcohol [29]. The RR for alcohol intake was 1.12 (95% CI 0.60–2.10, P = 0.723). Results from Kelemen et al. [75] demonstrate that the consumption of alcohol is inversely associated with postmenopausal ovarian cancer, and that the relationship between folate with ovarian cancer varies by the quantity of alcohol consumption.

Forest plot for cohort studies evaluating pooled relative risk (RR) of intake of a alcohol; b micro/macronutrients and plant-based bioactive compounds and ovarian cancer risk. OC ovary cancer
Intake of micro/macronutrients and plant-based bioactive compounds and ovarian cancer risk
As Supplementary Table S19 depicts, the meta-analysis of the relationship between micro/macronutrients and plant-based bioactive compounds intake and the risk of ovarian cancer incorporated 29 cohort studies [8, 29,30,31, 36,37,38, 42, 43, 51,52,53, 55, 68, 70, 72, 75,76,77,78,79,80,81,82,83,84,85,86,87]. Micro/macronutrients and plant-based bioactive compounds intake were not significantly associated with a reduced risk of ovarian cancer (RR = 0.96, 95% CI 0.91–1.01, Pheterogeneity = 0.906, I2 = 0.0%, P = 0.102) (Fig. 4b). The subgroup analyses represent significant decreases in ovarian cancer risk with intake of fiber (RR = 0.89, 95% CI 0.81–0.98, Pheterogeneity = 0.423, I2 = 2.5%, P = 0.014) and flavonoids (RR = 0.83, 95% CI 0.78–0.89, Pheterogeneity = 0.178, I2 = 22.0%, P = 0.0001) (Table 1). In contrast, intake of retinol (RR = 1.14, 95% CI 1.00–1.30, Pheterogeneity = 0.839, I2 = 0.0%, P = 0.048) significantly increased the risk of ovarian cancer. The intake of micro/macronutrients and plant-based bioactive compounds was at a moderately decreased risk of ovarian cancer in the United States, Australia and Canada populations, but not statistically significant (Table 2). From among the 29 studies on micro/macronutrients and plant-based bioactive compound intake, 16 [29, 30, 37, 42, 51, 55, 72, 78, 80,81,82,83,84,85,86,87] non-significant relationships and a positive relationship were reported for supplemental folate and calcium (diet) intake [43]. A lower risk of ovarian cancer was reported with fiber [8], isoflavones [36], kaempferol and flavonoids [37], dairy protein [38], calcium [52, 53], riboflavin [68], folate [70, 76, 77], pyridoxine [77], flavonols and flavanones [79] consumption. Isoflavonoids, coumestrol, total fiber, cereal fiber, or vegetable fiber intake exerted a protective influence for borderline subtype of ovarian cancer, but not for invasive ovarian cancer [31]. A high intake of dietary folate can be influential in lowering the ovarian cancer risk, specifically in alcohol-consuming women [70, 75, 76]. As shown in Table 3, significant positive association was found between intake of micro/macronutrients and plant-based bioactive compounds and endometrioid ovarian tumor risk (RR = 1.08, 95% CI 1.02–1.15; P = 0.015). Non-significant associations between other histologic subtypes of ovarian cancer and consumption of micro/macronutrients and plant-based bioactive compounds were reported [31, 37, 55, 72, 76, 78, 79, 85]. The highest to the lowest quartile of isoflavonoids, coumestrol, total fiber, cereal fiber or vegetable fiber intake differed between the two subtypes of ovarian cancer leading to a protective effect for borderline ovarian cancer but not for invasive cancer [31]. The larger dietary folate was related to a marginally reduced risk and for the serous subtype [72]. Larger intakes of vitamins were related to marginally larger risks of endometrioid tumors, but not other histological types [78]. The relationship for the intake of flavanone was stronger for serous invasive and mildly differentiated tumors as compared to non-serous and less-aggressive tumors [79]. Relationships for histologic subtypes of ovarian cancers were not significantly different for the entirety of carotenoids with the exception of lutein/zeaxanthin that was related to a statistically significant high mucinous ovarian cancer risk [85]. Non-significant associations were obtained with menopausal status and with consumption of micro/macronutrients and plant-based bioactive compounds (RR = 0.88, 95% CI 0.76–1.02; P = 0.093) [29, 38, 51, 80, 84].
Coffee and tea intake and ovarian cancer risk
Supplementary Table S20 suggests that the meta-analysis of the relationship between intake of coffee and tea and the risk of ovarian cancer incorporates 23 cohort studies [8, 29, 30, 36, 37, 67, 88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104]. Figure 5 reported no significant association between coffee and tea intake and the reduced risk of ovarian cancer (RR = 0.89, 95% CI 0.75–1.05, Pheterogeneity = 0.0001, I2 = 71.3%, P = 0.167). The subgroup analyses also showed that green tea consumption significantly decreased the risk of ovarian cancer (RR = 0.61, 95% CI 0.49–0.76, Pheterogeneity = 0.200, I2 = 31.5%, P = 0.0001) (Table 1). As shown in Table 2, a moderately decrease risk was found in the European and United States populations. From among the 23 studies on the consumption of coffee and tea, 13 [8, 29, 30, 36, 88, 91, 93, 94, 98, 101,102,103,104] revealed non-significant relationships. A lower risk of ovarian cancer was reported with tea (non-herbal) [37], caffeinated coffee [67], coffee [89] and tea [92, 96, 99] consumption. Also, Gunter et al. [90], revealed a statistically significant positive relationship between coffee and ovarian cancer mortality. In 1 research investigation [97], a positive relationship was found to exist between coffee consumption and the risk of ovarian cancer. Elevated levels of green tea post-diagnosis consumption can increase ovarian cancer survival rates [100]. No significant associations between histologic subtypes of ovarian cancer and coffee and tea consumption were found (Table 3) [98, 99]. Steevens et al. [96] demonstrated that tea was inversely related with serous tumors, while it was associated with high risk of mucinous and endometrioid tumors. Menopausal status and coffee and tea consumption were not significantly related (RR = 0.99, 95% CI 0.72–1.35; P = 0.939) [29, 67]. Caffeine was found to be inversely related to postmenopausal ovarian cancer; while, it was positively related to premenopausal ovarian cancer [67]. One study [95] indicated that a coffee component other than caffeine, or in conjunction with caffeine, is related with higher risk of ovarian cancer among postmenopausal women drinking five or more than five cups of coffee a day.

Forest plot for cohort studies evaluating pooled relative risk (RR) of coffee and tea intake and ovarian cancer risk. OC ovary cancer
Intake of non-food contaminants and ovarian cancer risk
Supplementary Table S21 suggests that the meta-analysis of the relationship between intake of non-food contaminants and the risk of ovarian cancer incorporated 14 cohort studies [105,106,107,108,109,110,111,112,113,114,115,116,117,118]. Intake of non-food contaminants was not significantly associated with the risk of ovarian cancer (RR = 0.98, 95% CI 0.90–1.08, Pheterogeneity = 0.204, I2 = 23.1%, P = 0.740) (Fig. 6a). The results of subgroup analysis demonstrated that intake of acrylamide, nitrate and other non-food contaminants including water disinfectants (dichloroacetic acid, trichloroacetic acid, haloacetic acid 5, haloacetic acid 6, bromochloroacetic acid, bromodicholoromethane, trihalomethanes and chloroform) and polychlorinated biphenyls were significantly associated with an increased risk of ovarian cancer (Table 1). Subgroup analysis by geographic location/country showed that no statistically significant association was found between intake of non-food contaminants and ovarian cancer risk (Table 2). Nine of the 14 studies on non-food contaminant intake, acrylamide [105, 108, 116], atrazine [106], polychlorinated biphenyls [107], cadmium [110, 111, 114], N-nitroso compounds [113] and ovarian cancer risk were not significantly related. Dietary nitrate was inversely related to the risk of ovarian cancer; while dietary nitrite from processed meats was positively related to the risk [109]. In 2 studies, a positive relationship was reported between the risk of ovarian cancer and acrylamide [117] and nitrate [118] intake. The highest intake category of animal sources of nitrite experienced a 34% increase in ovarian cancer risk [112]. Wilson et al. [115] reported a non-statistically significant indication of a higher risk of ovarian cancer among women experiencing the highest acrylamide intakes subsequent to confounder adjustment especially the intake of caffeine. As shown in Table 3, no significant associations between histologic subtypes of ovarian cancer and non-food contaminant intake were obtained [108, 112, 114,115,116]. Non-significant associations were obtained between menopausal status and non-food contaminant intake (RR = 1.10, 95% CI 0.69–1.78; P = 0.686) [105, 115]. The high nitrate quantities in public drinking water and private well use may raise the risk of ovarian cancer among postmenopausal women [109].

Forest plot for cohort studies evaluating pooled relative risk (RR) of intake of a non-food contaminants; b sweets and carbohydrate foods and ovarian cancer risk. OC ovary cancer
Intake of sweets and carbohydrate foods and ovarian cancer risk
Supplementary Table S22 shows that the meta-analysis of the relationship between intake of sweets and carbohydrate foods and risk of ovarian cancer incorporated 8 cohort studies [29, 30, 32, 35, 36, 43, 119, 120]. Intake of sweets and carbohydrate foods was not significantly associated with the risk of ovarian cancer (RR = 1.00, 95% CI 0.88–1.13, Pheterogeneity = 0.101, I2 = 41.6%, P = 0.966) (Fig. 6b). Subgroup analyses of type of sweets and carbohydrate foods reveled no significantly associated with the risk of ovarian cancer (Table 1). In the subgroup analysis based on geographic location/country, no significant association was observed in the subgroups (Table 2). In 5 [29, 30, 32, 35, 36] out of 8 studies on sweet and carbohydrate food intake, non-significant relationships were obtained. In 2 studies, a positive and higher risk of ovarian cancer with carbohydrate intake [43] and diets with high glycemic load values [120] were reported; while in 1 study [119], sugars were found to be inversely related to ovarian cancer risk. No significant association between menopausal status and sweet and carbohydrate food consumption was reported (RR = 1.20, 95% CI 0.65–2.21; P = 0.562) [29, 120].
Discussion
The present meta-analysis is supportive of a significant heterogeneity between dietary intake and ovarian cancer. In general, the authors observed that dietary intake exerts low effects on the risk of ovarian cancer. Some studies evaluated risk by histologic subtypes of ovarian cancer and menopausal status, in this case, the authors observed a less effect of dietary intake. The World Cancer Research Fund Continuous Update Project Report on diet and ovarian cancer risk considers the assertion that diet has a role as only limited and inconclusive as the findings to date are scare and inconsistent [121]. Nevertheless, there is evidence to suggest relationships between diet and ovarian cancer survival [57, 122,123,124,125,126,127,128,129,130].
Intake of fruits, vegetables and mushrooms and ovarian cancer risk
The results emanating from the present meta-analysis demonstrate that vegetable, fruit and mushroom intake exert low effects on reduce risk of ovarian cancer. Previous meta-analyses have documented significant relationships between fruit, vegetable and mushroom consumption and the lower risk of cancer in various anatomical locations [131,132,133,134,135,136].
As rich sources of nutrients and pharmaceutically bioactive compounds, vegetables, fruits, and mushrooms possess anti-carcinogenic properties [32, 34, 39, 134, 135] having antioxidant and anti-proliferative activities, are able to modulate steroid hormone concentrations and metabolism, enzymatic carcinogen detoxification, and to maintain intracellular matrix integrity, to stimulate the immune system and to inhibit metastasis and synthesis and methylation of DNA [32, 34, 39, 135]. The result, which is in agreement with the present systematic review, suggests that vegetable consumption rather than fruit consumption may be more beneficial [24]. Considering the intake of vegetables, previous systemic reviews and meta-analyses of cohort studies documented significant inverse relationships with ovarian cancer [24, 25, 124]. These findings were consistent with the results in specific epidemical studies [4, 8, 24, 25, 38,39,40, 43], which reported inverse associations between intake of green leafy green leafy and allium vegetables and ovarian cancer risk. Consistent with the specific epidemical studies [20, 24, 25, 32, 37,38,39,40], and an earlier meta-analysis [124], we observed a moderately reduce associations of consumption of red/yellow vegetables, broccoli, fruiting vegetables and soybean and risk of ovarian cancer. In 1 study, negative relationships were reported between the ovarian cancer risk and high vegetable intake (Chinese cabbage). The reason may be that the Japanese often consume pickled Chinese cabbage. It is worth mentioning that processing vegetables lowers the levels of micronutrients, e.g., antioxidants and vitamins [20]. Pickled vegetables make it possible for fermentation and growth of fungi and yeasts to take place and do possess the potential to produce carcinogenic N-nitroso compounds and mycotoxins [137, 138].
The anti-carcinogenic bioactivity of constitutive compounds within vegetables and fruits such as glucosinolates, polyphenols, flavonoids (diosmin, hesperidin, flavonols, flavones, anthocyanidins, catechins, flavanones, isoflavones and isoflavonoids), carotenoids and other bioactive compounds, cause apoptosis and hinder cell growth through pleiotropic mechanisms containing the capability to support adjust metabolic reprogramming and anti-inflammatory attributes [82, 139,140,141,142,143]. Phytoestrogens has both estrogenic and antiestrogenic effects and multiple actions within cancer cells [122, 144, 145]. Phytoestrogens inhibit tumor angiogenesis, tyrosine kinase and topoisomerase II. Other signal pathways are mediated by receptors such as GnRH receptor, FSH or LH receptors and GFR which adjust hormone concentrations and the related gene and protein expressions, e.g., protein kinase B (Akt), Raf, caspase3, NF-κB, Bcl-2, inhibit apoptosis, metastasis and cell proliferation of ovarian cancer cells [122, 123]. Organosulfur compounds, substances in allium vegetables, are considered to be associated with cancer protection through modulation of metabolizing enzymes and anti-proliferative activity thus inhibiting cell proliferation and tumor growth [4]. Isothiocyanates which found among the cruciferous vegetables including broccoli are capable of inhibiting metabolic activation and enforcing detoxification of carcinogens, altering apoptosis, protecting against oxidative damage, and producing antiestrogenic effects, probably in synergy with isoflavones [36, 140]. Antagonistic activity of isothiocyanates against cancer is associated with direct or indirect interaction with Nrf2 and NF-κB protein, phosphorylation of EGFR at Tyr1068 and lower phosphorylation of Akt [140, 146, 147].
Previous meta-analyses have reported on the protective role played by dietary carotenoids and ovarian cancer risk [128, 148]. Antioxidants such as carotenoids, vitamin E and vitamin C are considered to be influential in the control of cellular differentiation or proliferation and to affect reactive oxygen species, to initiate lipid peroxidation, inhibitory effect on insulin-like growth factor-1 (IGF-1)-stimulated cell multiplication, cell damage, to disrupt cell signaling and to express all salient events in carcinogenesis [5, 8, 29, 32, 78, 149].
Intake of mushroom was associated with a higher risk of ovarian cancer [29] whose result was contrary to other studies [4, 150]. Medicinal mushrooms can be considered as a source of ergothioneine, selenium, fiber, and several other vitamins and minerals, having anti-tumor and anti-carcinogenic effects by inhibiting NF-κB signaling pathway components [151,152,153]. The salient safety concerns for mushrooms include the toxicity and carcinogenicity of agaritine and its derivatives and their possible contamination with toxic metals [154].
Intake of meats and eggs and ovarian cancer risk
The results emanating from the present meta-analysis demonstrate that meat and egg consumption is less influential on increase risk ovarian cancer. The results from systematic review and meta-analyses suggest that red and processed meat consumption is not related to the ovarian cancer risk [25, 155]. There is other meta-analytical research to indicate that low intake of processed meat and high consumption of poultry and fish can lower the ovarian cancer risk [24, 156]. The results from the present study could provide moderate non-significant support to the idea that a low ovarian cancer risk was associated with high fish consumption. The meta-analysis demonstrated that total fish consumption was not significantly related to ovarian cancer risk [157]. Mechanisms recommended for a relationship between red and processed meat and ovarian cancer include high fat intake, as shown to be associated with high levels of circulating estrogens or mediated through obesity, leading to high biologically active estrogen levels [155]. Preservation, cooking or processing methods may lead to the introduction of mutagens and carcinogens to meat, e.g., N-nitroso compounds, heterocyclic amines and polycyclic aromatic hydrocarbons. Heme iron, more commonly existing in red meat than white meat, is also capable of stimulating endogenous N-nitroso production [24, 155]. Heat-resistant infectious agents can get involved in synergic interactions with the chemical carcinogens [158]. A mechanism for the protective effect of fish intake is the rich source of omega-3 fatty acids and their anti-apoptotic and anti-inflammatory properties [8, 157]. The results from Tavani et al.’s [159] meta-analysis demonstrated that there was a significantly inverse relationship between intake of omega-3 polyunsaturated fatty acid and risk of ovarian cancer. One cohort study [41] and meta-analyses suggest that dietary intake of total omega-3 fatty acids is not significantly related with the ovarian cancer risk [160, 161]. Omega-3 fatty acid anti-proliferative and anti-carcinogenic exerts an effect on epithelial ovarian cancer cell lines [161]. Carcinogenic and mutagenic N-nitroso compounds and heterocyclic amines in processed fish can raise the risk of cancer [157, 161].
Results from epidemiologic cohort studies investigating the relationship between egg intake and ovarian cancer risk are inconclusive. Meta-analyses of observational investigations suggested that dietary egg intake is capable of raising the risk of ovarian cancer [162, 163]. The biological mechanism through which eggs exert a harmful effect on cancer risk probably involves the large cholesterol content and large quantities of protein per energy content in egg [163, 164]. Chlorine, used to wash eggs, interacts with the organic substances within the eggs turning into potentially carcinogenic organochlorines which interrupt estrogen-related pathways [24, 163]. Furthermore, eggs can be considered as a source of heterocyclic amines formed during high-temperature cooking [165].
Intake of dairy products and ovarian cancer risk
In Jeyaraman et al.’s [166] overview of reviews, twenty-six meta-analyses showed no statistically significant associations between all-dairy products, whole milk, milk, low-fat/skim milk, yogurt, cheese, hard cheese, cottage cheese, butter, ice cream or lactose, intake and risk of ovarian cancer. Three meta-analyses showed an increased risk of ovarian cancer with higher consumption of whole milk or lactose exposure. Lu et al.’s [167] meta-analysis demonstrates that total dairy products intake exerts no significant effects on raising the mortality rates of all cancers, while low total dairy intake even lowered the relative risk. Another meta-analysis suggested that high dairy product/constituent intakes, e.g., lactose, can raise the ovarian cancer risk [168]. The authors’ results indicate that consumption of dairy products exerts no statistically significant associations with the ovarian cancer. Inconsistent results from this meta-analysis showed that lactose intake was related to both increased and decreased risk of ovarian cancer [38, 43, 51, 55]. Galactose produced by lactose has been shown to raise the ovarian cancer risk by direct toxicity to the ovarian germ cells. The high dairy product intake is also likely to increase the ovarian cancer risk within the population through genetic or biochemical properties of galactose. The intense impairment of the galactose-1-phosphate uridyltransferase (GALT) gene leads to accumulation of galactose and other metabolites within the body, e.g., the ovary [54,55,56,57, 162, 169,170,171]. These findings indicate that the consumption of high-fat dairy products and total cheese exert moderate but not statistically significantly increased association with the ovarian cancer. The estrogens of cow milk, dairy contaminants, processing or storage of dairy products and dairy additives can raise the risk of cancer [170, 171].
Intake of dietary fats and fatty acids and ovarian cancer risk
Some meta-analytical researches suggest that high dietary fat intake represents a significant risk factor for the development of ovarian cancer [172, 173]. Hou et al.’s [174] meta-analysis reveals non-significant associations between dietary fat and fatty acid intakes and ovarian cancer. In the present review, intake of dietary fats and fatty acids was found to be not statistically significantly associated with an increased risk of ovarian cancer. The subgroup findings indicated that the intake of total fat, saturated fat and fatty acid and cholesterol exerts significantly increased association with the ovarian cancer. Dietary fats were hypothesized to affect ovarian carcinogenesis mainly through hormone-related mechanisms via mitogenic effects on ERα-positive or -negative tumor cells. Obese females suffer from insulin resistance, and concurrent hyperinsulinemia with excess IGF-1 receptor may lead to androgen steroidogenesis and development of tumors [8, 30, 160]. Fatty acid metabolism plays a significant role in ovarian cancer tumorigenesis [11]. Cholesterol can exert an effect on the ovarian cancer risk through high circulating estrogen or progesterone [175].
Alcohol intake and ovarian cancer risk
The results indicate that the intake of alcohol exerts no significant association with the increased risk of ovarian cancer. Previous meta-analytical research demonstrates that the intake of alcohol is not related to a high ovarian cancer risk [175,176,177,178,179,180,181]. Our findings demonstrated that the intake of wines and spirits was at a moderately increased risk of ovarian cancer. Mechanisms of alcohol-related ovarian carcinogenesis include high cumulative estrogen exposure, alteration of gonadotropin levels, promotion of DNA damage, impaired folate metabolism, oxidative stress, acetaldehyde, DNA hypomethylation, inhibition of carcinogen detoxification or clearance, and increased metastatic potential of tumor cells. Antioxidants, e.g., polyphenols and resveratrol contained in red wine, were suggested to justify the inverse relationship between red wine and the ovarian cancer risk [177, 178, 182]. Conversely, alcohol is documented to exert a protective potential against ovarian carcinogenesis through lowering follicle stimulating hormone, luteinizing hormone and gonadotropin levels [182]. Phytochemicals in red wine have varied effects, e.g., cancer preventive and pro-estrogenic activity and genotoxicity [69].
Intake of micro/macronutrients and plant-based bioactive compounds and ovarian cancer risk
The results emanating from the present meta-analysis indicate that micro/macronutrients and plant-based bioactive compounds exert lower effects on reduce risk of ovarian cancer. Consistent with the specific epidemical studies [8, 36, 37, 79], and prior meta-analyses [24, 126, 127, 179], we observed a significantly reduced association of consumption of fiber and flavonoids, and risk of ovarian cancer. The increasing dietary fiber intake can lower the bioavailability of steroid hormones through influencing bacterial macroflora, increasing sex hormone-binding globulin causing smaller circulating levels of unbound or biologically available estrogen, lessening circulating estrogens through inhibition of bile reabsorption, increasing faecal excretion, and increasing the protection of phytoestrogens, which can preclude the development of ovarian cancer [8, 24, 84, 126, 127, 183]. Dietary fiber can exert an effect on inflammation lowering glycemic load and improving insulin sensitivity, favorably regulating IGF-1 [8, 127, 183]. Numerous mechanisms can inhibit ovarian carcinogenesis through flavonoids, e.g., free radical scavenging or enhancing the body’s antioxidant systems, such as through upregulating activity of glutathione S-transferase and other detoxifying enzymes, thus enhancing carcinogen clearance. Flavonoids have also been mentioned to prevent the incorporation of some metabolic precursors, which shows that they could be preventative in DNA, RNA, and/or protein synthesis, and they have been mentioned to incorporate into DNA, according to their similarities with nucleosides structures [184]. Certain flavonoids, e.g., quercetin, luteolin and apigenin, are likely to decrease inflammation through their inhibitory effect on the enzymes cyclooxygenase-2 and inducible nitric oxide synthase which are both salient mediators of inflammatory reactions. Quercetin has the capability to prevent the aromatase activity and topoisomerase I-catalyzed DNA religation [185]. Flavonoids can modulate sex steroid hormone levels through both estrogenic and anti-estrogenic effects. Flavonoids may inhibit proliferation in human cancer cell lines and angiogenesis through suppression of expression of VEGF and triggering the non-apoptotic cell death, interrupting cell signaling and cell cycle and inducing apoptosis [31, 36, 37, 79, 82, 186, 187]. Kaempferol can lower the level of proliferation and significantly decrease the expression of VEGF through suppression of extracellular signal-regulated kinase (ERK)–NFκB–cMyc–p21–VEGF pathway in cancer cells [141, 188]. Taking a molecular viewpoint, flavones and isoflavone can be considered as competitive inhibitors of cytochrome P450 [189].
Although epidemiological studies have suggested an inverse correlation between cancer development and dietary consumption of vitamin A, our results showed that retinol consumption was positively related to the ovarian cancer risk. Retinol and vitamin A derivatives influence cell differentiation, proliferation, and apoptosis and play an important physiologic role in a wide range of biological processes [190].
These findings were consistent with the results in specific epidemical studies [30, 68, 77], which reported significantly/modestly decreased risk associations between intake of thiamin and riboflavin and ovarian cancer. Thiamin may also play a role in carcinogenesis, by their independent roles in DNA synthesis. Additionally, riboflavin can be influential in carcinogenesis as cofactors in folate metabolism [68].
The results from a meta-analysis [191] suggest that large levels of dietary protein consumption are not related to the ovarian cancer risk. Although our results were not statistically significant, we found the lower decrease of diatery proteins with the ovarian cancer risk. A number of dairy product constituents, e.g., proteins and calcium are likely to be responsible for the protective relationships with cancers [38, 52, 53]. For instance, lactoferrin is known for its inhibitory action on cell proliferation and its anti-inflammatory, antioxidant abilities and protection against cancer development and metastasis [192]. Casein, e.g., whey proteins, is capable of enhancing cellular levels of glutathione, an antioxidant. Furthermore, whey proteins can lower cancer risk through elevating hormonal and cell-mediated immune responses [193]. Our findings demonstrated that the intake of calcium and total vitamin D was not significantly related with the ovarian cancer risk. The inadequate calcium intake and low vitamin D status can be considered as salient risk factors in numerous types of cancer [194, 195]. The meta-analysis suggested that higher calcium intake may be inversely related to the ovarian cancer risk [125]. The high calcium intake is likely to raise or lower the ovarian cancer risk. High calcium intakes can depress 1,25-(OH)2D, leading to an enhancement of cellular proliferation and, hence, tumorigenesis [55]. Tissue-specific expression of the CYP27B1-encoded 25-hydroxyvitamin D-1α-hydroxylase and of the extracellular calcium-sensing receptor (CaR) locally produced 1,25(OH)2D3 and extracellular Ca2+ act jointly as main regulators of cellular proliferation, differentiation and function. Therefore, impairment of antimitogenic, proapoptotic and pro-differentiating signaling from the 1,25(OH)2D3-activated vitamin D receptor (VDR) and from the CaR in vitamin D and calcium insufficiency has been suggested in the pathogenesis of the above-mentioned types of cancer [194, 195]. Furthermore, vitamin D has a non-genomic impact, i.e., regulation of calcium and phosphate homeostasis pathways, activating protein kinase C, protein kinase A, PI3K and phospholipase C. The VDR variant is also likely to be involved in ovarian cancer carcinogenesis which expands VDR results in lower NF-kB transcriptional activation, causing lower IL-12 expression and a weaker immune response [195]. Higher calcium levels are characterized by down-regulation of circulating parathyroid hormone, which can lower hepatic and osteoblastic synthesis of IGF-1 [125, 194, 196]. Vitamin D plays a potential role in cell cycle and apoptosis, angiogenesis, invasion and metastasis, inflammatory response and tumor metabolism [190]. No conclusive or strong evidence exists to support the claim made in a large number of review articles that vitamin D exposures lower the ovarian cancer risk occurrence or mortality [7, 197, 198].
Coffee and tea intake and ovarian cancer risk
The results emanating from the present meta-analysis demonstrate that coffee and tea exert less effect on reduced risk of ovarian cancer. Our results demonstrated a significant relationship between green tea consumption and a reduced risk of ovarian cancer. On the other hand, modestly lower risk of ovarian cancer was found regarding total tea intake. Prior meta-analytical research revealed an inverse relationship between tea and green tea consumption and the risk of ovarian cancer [96, 129]. Furthermore, non-significant relationships were obtained between tea and green tea consumption and the risk of ovarian cancer in other meta-analyses [93, 130, 199,200,201]. Tea polyphenols, e.g., catechins, flavanols, theaflavins and thearubigins, are beneficial components of tea which may down-regulate the expression of a variety of tumor genes, causing tumor cell apoptosis, blocking tumor cell cycle, up-regulating the body metabolism, eradicating excess free radicals, influencing the prevention and inhibition of tumors. Some polyphenols may cause tumor cell apoptosis inhibiting tumor angiogenesis [93, 129]. Catechins and gallocatechins, having low quantities of methylxanthines detected mainly in green tea, and theaflavin digallate, a major component of black tea, are the two most effective anti-cancer factors in tea. Signaling proteins affected by epigallocatechin gallate in ovarian cancer, i.e., JUN, FADD, NFKB1, Bcl-2, HIF1α, and MMP, influence the cell cycle, cellular assembly and organization, and DNA replication. The effect of tea varies for the difference in genetic heterogeneity and lifestyle among populations. Moreover, the numerous ingredients in tea may have varying anti-cancer activities and effects on various types and subtypes of ovarian cancer [93, 129, 202, 203].
Consistent with the results emanating from other meta-analytical research studying [93, 96, 130, 204,205,206,207], we suggest no relationship between coffee intake and ovarian cancer. Furthermore, our findings indicated a lower risk of ovarian cancer with intake of decaffeinated coffee and lesser with caffeine. In contrast, a lower positive risk of ovarian cancer was observed with intake of soft drinks. An inverse association between coffee consumption and cancer risks can be mediated by various mechanisms, e.g., hormonal homeostasis, reduction of oxidative stress and DNA damages, detoxification of carcinogens, inhibition of carcinogenesis, and induction of apoptosis. Coffee holds many bioactive components such as polyphenols, caffeine, diterpenes, melanoidins, which lower oxidative stress, exert anti-cancerogenic properties, through triggering defense mechanisms, carcinogenic detoxification, and activation or suppression of onco-suppressors and proto-oncogenes, respectively [204, 205]. A number of studies in the authors’ results assert that coffee consumption can be related to higher ovarian cancer risks [90, 95, 97]. Conversely, coffee also holds acrylamide and caffeine, which exert potential hormonal and carcinogenic effects [93].
Intake of non-food contaminants and ovarian cancer risk
Non-food contaminants exert less effect on increase risk ovarian cancer. These findings were consistent with the results in specific epidemical studies [109, 112, 117, 118], which reported significantly/modestly increased risk associations between intake of acrylamide and nitrate, nitrite and ovarian cancer. The systematic review and meta-analyses of epidemiological investigations suggest that high acrylamide intake levels are strongly related to the ovarian cancer risk [208]. Other extensive systematic review and meta-analysis revealed no increases in the risk of most types of cancer as related to acrylamide exposure [209]. Foods, as sources of acrylamide, hold various nutrients and most foods are high-energy sources, causing obesity and increasing the risk of numerous cancers, and exposure to acrylamide [210]. The major pathway to acrylamide carcinogenesis is through its oxidization to glycidamide, by the Cyp2e1 enzyme system. Acrylamide can play a carcinogenic role in the selected body sites through affecting hormonal balances in addition to their detrimental and mutagenic effects on DNA [105, 108, 117, 208, 210]. The literature on dietary nitrate or nitrite and cancer risk has been expanding but the results have been inconclusive. The meta-analysis of epidemiological investigations revealed that non-significant relationships exist between dietary nitrate or nitrite and ovarian cancer [211]. Nitrate and nitrite can be considered as precursors in the endogenous formation of N-nitroso compounds, potential human carcinogens. Nitrosamides directly alkylate DNA causing tumors in numerous organs, while nitrosamines need to be activated by specific cytochrome P450 enzymes to be carcinogenic. Certain nutrients are likely to influence endogenous N-nitroso compounds formation in the stomach. Conversely, heme iron has been demonstrated to promote total N-nitroso compounds formation. Nevertheless, epidemiologic evidence for these interactions on cancer risk is yet to be evolved. Antioxidants, e.g., vitamins C and E, reveal N-nitroso compounds formation through converting nitrite to nitric oxides lowering the level of N-nitroso compounds-induced DNA adducts [109].
These findings of subgroup analysis showed that intake of dichloroacetic acid, trichloroacetic acid, haloacetic acid 5, haloacetic acid 6, bromochloroacetic acid, bromodicholoromethane, trihalomethanes, chloroform and polychlorinated biphenyls was significantly associated with an increased risk of ovarian cancer. Some studies revealed non-significant relationships between atrazine, polychlorinated biphenyls, cadmium and N-nitroso compound intake and the risk of ovarian cancer [106, 107, 110, 111, 113, 114]. The mechanism of polychlorinated biphenyls works through disruption of hormone-dependent pathways [107]. Generally, the available epidemiological research does not furnish conclusive and scientifically compelling evidence of causality between exposure to atrazine or triazine herbicides and cancer in humans [212]. Atrazine exposure mainly affected antioxidant defenses and, to a lesser degree, lipid, protein, carbohydrates and nucleic acids oxidation processes by cytochrome P450 enzymes, generation of redox-active metabolites and impairment of the electron transport cascades in mitochondria [213, 214]. Numerous mechanisms potentially associate cadmium with cancer, e.g., aberrant gene expression, oxidative stress and inflammation interference with DNA, alterations of DNA methylation and enhanced proliferation, depressed apoptosis or epigenetic alterations [110, 111, 114]. Mechanistic and epidemiologic evidence indicates that estrogen-mimicking contaminants, e.g., the environmental and dietary pollutant cadmium, are likely to contribute to the development of ovarian cancer [111, 114].
Intake of sweets and carbohydrate foods and ovarian cancer risk
The authors observed no significant effect of sweet and carbohydrate food consumption on the ovarian cancer risk. We observed a moderately increased association of consumption of sweets and risk of ovarian cancer. Interestingly, our subgroup analysis consistent with the results in specific epidemical study [119] showed a lower decrease association of consumption of carbohydrates and risk of ovarian cancer. While our results contrast with some studies suggesting that a diet high in carbohydrates increases ovarian cancer risk [43] and ovarian cancer risk null relationships [120], showing that most individual foods and nutrients are not associated with ovarian cancer risk. The positive relationship with high levels of carbohydrate, e.g., sugar intake, may be related to their elevated glycemic index, which has been associated with hyperinsulinemia and lower IGF binding protein concentrations, thus enhancing IGF-1 levels. Increased IGF-1 bioactivity hinders apoptosis, stimulates cell proliferation and sex steroid synthesis and hampers sex-hormone binding globulin synthesis, whose phenomenon can be suggestive of the development of ovarian cancer. Furthermore, the results suggest that the acute glucose fluctuations evoke oxidative stress, accompanied with subsequent oxidative DNA damage, suggestive of cancer development [119, 120, 215,216,217].
We analyzed the association between dietary intake and the risk of ovarian cancer subtypes and menopausal status. We found that endometrioid ovarian cancer incidence was more susceptible to intake of micro/macronutrients and plant-based bioactive compounds. Furthermore, we observed no statistically significant association between menopausal status and dietary intake and the risk of ovarian cancer menopausal status.
The main limitation of our systematic review was the lack of consistency in risk associations between dietary intake and ovarian cancer. Additionally, data evolving for histologic subtypes of ovarian cancer and menopausal status were limited.
Conclusions
The conclusions emanating from the present review reveal the potential effects of dietary intake on ovarian cancer risk. It is likely that the few observed relationships have to do with the multifarious effects of components in dietary intake. Some findings are suggesting the potential for a lower ovarian cancer risk among women consuming green leafy green leafy, allium vegetables, fiber, flavonoids, green tea and possibly vegetables, red/yellow vegetables, broccoli, fruiting vegetables, soybean, fish, low fat dairy products, thiamin, riboflavin, carotenoids and tea. Conversely, for women consuming total fat, saturated fat and fatty acid, cholesterol, retinol, acrylamide and nitrate, dichloroacetic acid, trichloroacetic acid, haloacetic acid 5, haloacetic acid 6, bromochloroacetic acid, bromodicholoromethane, trihalomethanes, chloroform, polychlorinated biphenyls and probably red meat, pork, eggs, dried and salted fish, canned tuna, high-fat dairy products, total cheese, animal fat, dairy fat, wines, spirits, vitamin E and nitrite the risk may increase. In this regard, a global project using both quantitative and qualitative dietary analysis and varied information is needed. This global project must, of necessity, include the specific dietary, composition of food ingredients and human genetic population to assess the role of dietary intake in the risk of ovarian cancer.
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68(6):394–424. https://doi.org/10.3322/caac.21492
Vargas AN (2014) Natural history of ovarian cancer. Ecancermedicalscience 8:465. https://doi.org/10.3332/ecancer.2014.465
Daly MB, Dresher CW, Yates MS, Jeter JM, Karlan BY, Alberts DS, Lu KH (2015) Salpingectomy as a means to reduce ovarian cancer risk. Cancer Prev Res (Phila) 8(5):342–348. https://doi.org/10.1158/1940-6207.capr-14-0293
Schulz M, Lahmann PH, Boeing H, Hoffmann K, Allen N, Key TJA, Bingham S, Wirfält E, Berglund G, Lundin E, Hallmans G, Lukanova A, Garcia CM, González CA, Tormo MJ, Quirós JR, Ardanaz E, Larrañaga N, Lund E, Gram IT, Skeie G, Peeters PHM, Van Gils CH, Bas Bueno-De-Mesquita H, Büchner FL, Pasanisi P, Galasso R, Palli D, Tumino R, Vineis P, Trichopoulou A, Kalapothaki V, Trichopoulos D, Chang-Claude J, Linseisen J, Boutron-Ruault MC, Touillaud M, Clavel-Chapelon F, Olsen A, Tjønneland A, Overvad K, Tetsche M, Jenab M, Norat T, Kaaks R, Riboli E (2005) Fruit and vegetable consumption and risk of epithelial ovarian cancer: the European Prospective Investigation into Cancer and Nutrition. Cancer Epidemiol Biomark Prev 14(11 I):2531–2535. https://doi.org/10.1158/1055-9965.epi-05-0159
Tung KH, Wilkens LR, Wu AH, McDuffie K, Hankin JH, Nomura AM, Kolonel LN, Goodman MT (2005) Association of dietary vitamin A, carotenoids, and other antioxidants with the risk of ovarian cancer. Cancer Epidemiol Biomark Prev 14(3):669–676. https://doi.org/10.1158/1055-9965.epi-04-0550
Gifkins D, Olson SH, Paddock L, King M, Demissie K, Lu SE, Kong AN, Rodriguez-Rodriguez L, Bandera EV (2012) Total and individual antioxidant intake and risk of epithelial ovarian cancer. BMC Cancer 12:211. https://doi.org/10.1186/1471-2407-12-211
Reid BM, Permuth JB, Sellers TA (2017) Epidemiology of ovarian cancer: a review. Cancer Biol Med 14(1):9–32. https://doi.org/10.20892/j.issn.2095-3941.2016.0084
Playdon MC, Nagle CM, Ibiebele TI, Ferrucci LM, Protani MM, Carter J, Hyde SE, Neesham D, Nicklin JL, Mayne ST, Webb PM (2017) Pre-diagnosis diet and survival after a diagnosis of ovarian cancer. Br J Cancer 116(12):1627–1637. https://doi.org/10.1038/bjc.2017.120
Wentzensen N, Poole EM, Trabert B, White E, Arslan AA, Patel AV, Setiawan VW, Visvanathan K, Weiderpass E, Adami HO, Black A, Bernstein L, Brinton LA, Buring J, Butler LM, Chamosa S, Clendenen TV, Dossus L, Fortner R, Gapstur SM, Gaudet MM, Gram IT, Hartge P, Hoffman-Bolton J, Idahl A, Jones M, Kaaks R, Kirsh V, Koh WP, Lacey JV Jr, Lee IM, Lundin E, Merritt MA, Onland-Moret NC, Peters U, Poynter JN, Rinaldi S, Robien K, Rohan T, Sandler DP, Schairer C, Schouten LJ, Sjoholm LK, Sieri S, Swerdlow A, Tjonneland A, Travis R, Trichopoulou A, van den Brandt PA, Wilkens L, Wolk A, Yang HP, Zeleniuch-Jacquotte A, Tworoger SS (2016) Ovarian cancer risk factors by histologic subtype: an analysis from the ovarian cancer cohort consortium. J Clin Oncol 34(24):2888–2898. https://doi.org/10.1200/jco.2016.66.8178
Jia D, Nagaoka Y, Katsumata M, Orsulic S (2018) Inflammation is a key contributor to ovarian cancer cell seeding. Sci Rep 8(1):12394. https://doi.org/10.1038/s41598-018-30261-8
Jiang L, Fang X, Wang H, Li D, Wang X (2018) Ovarian cancer-intrinsic fatty acid synthase prevents anti-tumor immunity by disrupting tumor-infiltrating dendritic cells. Front Immunol 9:2927. https://doi.org/10.3389/fimmu.2018.02927
Longuespee R, Boyon C, Desmons A, Vinatier D, Leblanc E, Farre I, Wisztorski M, Ly K, D’Anjou F, Day R, Fournier I, Salzet M (2012) Ovarian cancer molecular pathology. Cancer Metastasis Rev 31(3–4):713–732. https://doi.org/10.1007/s10555-012-9383-7
Harrington BS, Annunziata CM (2019) NF-κB signaling in ovarian cancer. Cancers (Basel) 11(8):1182. https://doi.org/10.3390/cancers11081182
Ghoneum A, Said N (2019) PI3K-AKT-mTOR and NFκB pathways in ovarian cancer: implications for targeted therapeutics. Cancers (Basel) 11(7):949. https://doi.org/10.3390/cancers11070949
Tschernichovsky R, Goodman A (2017) Risk-reducing strategies for ovarian cancer in BRCA mutation carriers: a balancing act. Oncologist 22(4):450–459. https://doi.org/10.1634/theoncologist.2016-0444
Committee on Practice Bulletins–Gynecology C, Park J (2019) Practice Bulletin No 182: Hereditary Breast and Ovarian Cancer Syndrome. Obstet Gynecol 130(3):e110–e126. https://doi.org/10.1097/aog.0000000000002296
Grossman DC, Curry SJ, Owens DK, Barry MJ, Davidson KW, Doubeni CA, Epling JW Jr, Kemper AR, Krist AH, Kurth AE, Landefeld CS, Mangione CM, Phipps MG, Silverstein M, Simon MA, Tseng CW (2018) Screening for ovarian cancer: US Preventive Services Task Force recommendation statement. J Am Med Assoc 319(6):588–594. https://doi.org/10.1001/jama.2017.21926
Koushik A, Hunter DJ, Spiegelman D, Anderson KE, Arslan AA, Beeson WL, Van Den Brandt PA, Buring JE, Cerhan JR, Colditz GA, Fraser GE, Freudenheim JL, Genkinger JM, Goldbohm RA, Hankinson SE, Koenig KL, Larsson SC, Leitzmann M, McCullough ML, Miller AB, Patel A, Rohan TE, Schatzkin A, Smit E, Willett WC, Wolk A, Zhang SM, Smith-Warner SA (2005) Fruits and vegetables and ovarian cancer risk in a pooled analysis of 12 cohort studies. Cancer Epidemiol Biomark Prev 14(9):2160–2167. https://doi.org/10.1158/1055-9965.EPI-05-0218
Alvarez RD, Karlan BY, Strauss JF (2016) Ovarian cancers: evolving paradigms in research and care: report from the Institute of Medicine. Gynecol Oncol 141(3):413–415. https://doi.org/10.1016/j.ygyno.2016.04.541
Sakauchi F, Khan MM, Mori M, Kubo T, Fujino Y, Suzuki S, Tokudome S, Tamakoshi A (2007) Dietary habits and risk of ovarian cancer death in a large-scale cohort study (JACC study) in Japan. Nutr Cancer 57(2):138–145. https://doi.org/10.1080/01635580701274178
Lynch HT, Casey MJ, Snyder CL, Bewtra C, Lynch JF, Butts M, Godwin AK (2009) Hereditary ovarian carcinoma: heterogeneity, molecular genetics, pathology, and management. Mol Oncol 3(2):97–137. https://doi.org/10.1016/j.molonc.2009.02.004
National Comprehensive Cancer Network (NCCN) (2018) NCCN clinical practice guiedlines in oncology (NCCN Guiedlines®) for ovarian cancer including fallopian tube cancer and primary peritoneal cancer, version 2 2018
Ovarian cancer causes, risk factors, and prevention. https://www.cancer.org/cancer/ovarian-cancer/causes-risks-prevention/risk-factors.html. Accessed 11 April 2018
Schulz M, Lahmann PH, Riboli E, Boeing H (2004) Dietary determinants of epithelial ovarian cancer: a review of the epidemiologic literature. Nutr Cancer 50(2):120–140. https://doi.org/10.1207/s15327914nc5002_2
Crane TE, Khulpateea BR, Alberts DS, Basen-Engquist K, Thomson CA (2014) Dietary intake and ovarian cancer risk: a systematic review. Cancer Epidemiol Biomark Prev 23(2):255–273. https://doi.org/10.1158/1055-9965.EPI-13-0515
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097. https://doi.org/10.1371/journal.pmed.1000097
Aune D, Rosenblatt DAN, Chan DSM, Abar L, Vingeliene S, Vieira AR, Greenwood DC, Norat T (2015) Anthropometric factors and ovarian cancer risk: a systematic review and nonlinear dose-response meta-analysis of prospective studies. Int J Cancer 136(8):1888–1898. https://doi.org/10.1002/ijc.29207
Nieuwenhuis L, van den Brandt PA (2019) Nut and peanut butter intake are not directly associated with the risk of endometrial or ovarian cancer: results from a Dutch prospective cohort study. Clin Nutr. https://doi.org/10.1016/j.clnu.2019.09.008
Dunneram Y, Greenwood DC, Cade JE (2018) Diet and risk of breast, endometrial and ovarian cancer: UK Women’s Cohort Study. Br J Nutr. https://doi.org/10.1017/s0007114518003665
Merritt MA, Tzoulaki I, Van Den Brandt PA, Schouten LJ, Tsilidis KK, Weiderpass E, Patel CJ, Tjønneland A, Hansen L, Overvad K, His M, Dartois L, Boutron-Ruault MC, Fortner RT, Kaaks R, Aleksandrova K, Boeing H, Trichopoulou A, Lagiou P, Bamia C, Palli D, Krogh V, Tumino R, Ricceri F, Mattiello A, Bas Bueno-De-Mesquita H, Charlotte Onland-Moret N, Peeters PH, Skeie G, Jareid M, Ramón Quirós J, Obón-Santacana M, Sánchez MJ, Chamosa S, Huerta JM, Barricarte A, Dias JA, Sonestedt E, Idahl A, Lundin E, Wareham NJ, Khaw KT, Travis RC, Ferrari P, Riboli E, Gunter MJ (2016) Nutrient-wide association study of 57 foods/nutrients and epithelial ovarian cancer in the European Prospective Investigation into Cancer and Nutrition study and the Netherlands Cohort Study. Am J Clin Nutr 103(1):161–167. https://doi.org/10.3945/ajcn.115.118588
Hedelin M, Lof M, Andersson TM, Adlercreutz H, Weiderpass E (2011) Dietary phytoestrogens and the risk of ovarian cancer in the women’s lifestyle and health cohort study. Cancer Epidemiol Biomark Prev 20(2):308–317. https://doi.org/10.1158/1055-9965.epi-10-0752
Dolecek TA, McCarthy BJ, Joslin CE, Peterson CE, Kim S, Freels SA, Davis FG (2010) Prediagnosis food patterns are associated with length of survival from epithelial ovarian cancer. J Am Diet Assoc 110(3):369–382. https://doi.org/10.1016/j.jada.2009.11.014
Key TJ, Appleby PN, Spencer EA, Travis RC, Allen NE, Thorogood M, Mann JI (2009) Cancer incidence in British vegetarians. Br J Cancer 101(1):192–197. https://doi.org/10.1038/sj.bjc.6605098
George SM, Park Y, Leitzmann MF, Freedman ND, Dowling EC, Reedy J, Schatzkin A, Hollenbeck A, Subar AF (2009) Fruit and vegetable intake and risk of cancer: a prospective cohort study. Am J Clin Nutr 89(1):347–353. https://doi.org/10.3945/ajcn.2008.26722
Chang ET, Lee VS, Canchola AJ, Dalvi TB, Clarke CA, Reynolds P, Purdie DM, Stram DO, West DW, Ziogas A, Bernstein L, Horn-Ross PL (2008) Dietary patterns and risk of ovarian cancer in the California Teachers Study cohort. Nutr Cancer 60(3):285–291. https://doi.org/10.1080/01635580701733091
Chang ET, Lee VS, Canchola AJ, Clarke CA, Purdie DM, Reynolds P, Anton-Culver H, Bernstein L, Deapen D, Peel D, Pinder R, Ross RK, Stram DO, West DW, Wright W, Ziogas A, Horn-Ross PL (2007) Diet and risk of ovarian cancer in the California Teachers Study cohort. Am J Epidemiol 165(7):802–813. https://doi.org/10.1093/aje/kwk065
Gates MA, Tworoger SS, Hecht JL, De Vivo I, Rosner B, Hankinson SE (2007) A prospective study of dietary flavonoid intake and incidence of epithelial ovarian cancer. Int J Cancer 121(10):2225–2232. https://doi.org/10.1002/ijc.22790
Kiani F, Knutsen S, Singh P, Ursin G, Fraser G (2006) Dietary risk factors for ovarian cancer: the adventist health study (United States). Cancer Causes Control 17(2):137–146. https://doi.org/10.1007/s10552-005-5383-z
Mommers M, Schouten LJ, Goldbohm RA, van den Brandt PA (2005) Consumption of vegetables and fruits and risk of ovarian carcinoma. Cancer 104(7):1512–1519. https://doi.org/10.1002/cncr.21332
Larsson SC, Holmberg L, Wolk A (2004) Fruit and vegetable consumption in relation to ovarian cancer incidence: the Swedish Mammography Cohort. Br J Cancer 90(11):2167–2170. https://doi.org/10.1038/sj.bjc.6601872
Bertone ER, Rosner BA, Hunter DJ, Stampfer MJ, Speizer FE, Colditz GA, Willett WC, Hankinson SE (2002) Dietary fat intake and ovarian cancer in a cohort of US women. Am J Epidemiol 156(1):22–31. https://doi.org/10.1093/aje/kwf008
Fairfield KM, Hankinson SE, Rosner BA, Hunter DJ, Colditz GA, Willett WC (2001) Risk of ovarian carcinoma and consumption of vitamins A, C, and E and specific carotenoids: a prospective analysis. Cancer 92(9):2318–2326. https://doi.org/10.1002/1097-0142(20011101)92:9%3c2318:AID-CNCR1578%3e3.0.CO;2-7
Kushi LH, Mink PJ, Folsom AR, Anderson KE, Zheng W, Lazovich D, Sellers TA (1999) Prospective study of diet and ovarian cancer. Am J Epidemiol 149(1):21–31. https://doi.org/10.1093/oxfordjournals.aje.a009723
Gilsing AMJ, Weijenberg MP, Goldbohm RA, Van Den Brandt PA, Schouten LJ (2011) Consumption of dietary fat and meat and risk of ovarian cancer in the Netherlands Cohort Study. Am J Clin Nutr 93(1):118–126. https://doi.org/10.3945/ajcn.2010.29888
Daniel CR, Cross AJ, Graubard BI, Hollenbeck AR, Park Y, Sinha R (2011) Prospective investigation of poultry and fish intake in relation to cancer risk. Cancer Prev Res 4(11):1903–1911. https://doi.org/10.1158/1940-6207.CAPR-11-0241
Schulz M, Nöthlings U, Allen N, Onland-Moret NC, Agnoli C, Engeset D, Galasso R, Wirfält E, Tjønneland A, Olsen A, Overvad K, Boutron-Ruault MC, Chajes V, Clavel-Chapelon F, Ray J, Hoffmann K, Chang-Claude J, Kaaks R, Trichopoulos D, Georgila C, Zourna P, Palli D, Berrino F, Tumino R, Vineis P, Panico S, Bueno-De-Mesquita HB, Ocké MC, Peeters PHM, Lund E, Gram IT, Skeie G, Berglund G, Lundin E, Hallmans G, González CA, Quirós JR, Dorronsoro M, Martínez C, Tormo MJ, Barricarte A, Bingham S, Khaw KT, Key TJA, Jenab M, Rinaldi S, Slimani N, Riboli E (2007) No association of consumption of animal foods with risk of ovarian cancer. Cancer Epidemiol Biomark Prev 16(4):852–855. https://doi.org/10.1158/1055-9965.EPI-07-0054
Cross AJ, Leitzmann MF, Gail MH, Hollenbeck AR, Schatzkin A, Sinha R (2007) A prospective study of red and processed meat intake in relation to cancer risk. PLoS Med 4(12):e325. https://doi.org/10.1371/journal.pmed.0040325
Genkinger JM, Hunter DJ, Spiegelman D, Anderson KE, Beeson WL, Buring JE, Colditz GA, Fraser GE, Freudenheim JL, Goldbohm RA, Hankinson SE, Koenig KL, Larsson SC, Leitzmann M, McCullough ML, Miller AB, Rodriguez C, Rohan TE, Ross JA, Schatzkin A, Schouten LJ, Smit E, Willett WC, Wolk A, Zeleniuch-Jacquotte A, Zhang SM, Smith-Warner SA (2006) A pooled analysis of 12 cohort studies of dietary fat, cholesterol and egg intake and ovarian cancer. Cancer Causes Control 17(3):273–285. https://doi.org/10.1007/s10552-005-0455-7
Larsson SC, Wolk A (2005) No association of meat, fish, and egg consumption with ovarian cancer risk. Cancer Epidemiol Biomark Prev 14(4):1024–1025. https://doi.org/10.1158/1055-9965.EPI-04-0795
Knekt P, Steineck G, Jarvinen R, Hakulinen T, Aromaa A (1994) Intake of fried meat and risk of cancer: a follow-up study in Finland. Int J Cancer 59:756–760
Merritt MA, Poole EM, Hankinson SE, Willett WC, Tworoger SS (2014) Dairy food and nutrient intake in different life periods in relation to risk of ovarian cancer. Cancer Causes Control 25(7):795–808. https://doi.org/10.1007/s10552-014-0381-7
Park Y, Leitzmann MF, Subar AF, Hollenbeck A, Schatzkin A (2009) Dairy food, calcium, and risk of cancer in the NIH-AARP Diet and Health Study. Arch Intern Med 169(4):391–401. https://doi.org/10.1001/archinternmed.2008.578
Koralek DO, Bertone-Johnson ER, Leitzmann MF, Sturgeon SR, Lacey JV Jr, Schairer C, Schatzkin A (2006) Relationship between calcium, lactose, vitamin D, and dairy products and ovarian cancer. Nutr Cancer 56(1):22–30. https://doi.org/10.1207/s15327914nc5601_4
Mommers M, Schouten LJ, Goldbohm RA, van den Brandt PA (2006) Dairy consumption and ovarian cancer risk in the Netherlands Cohort Study on Diet and Cancer. Br J Cancer 94(1):165–170. https://doi.org/10.1038/sj.bjc.6602890
Genkinger JM, Hunter DJ, Spiegelman D, Anderson KE, Arslan A, Beeson WL, Buring JE, Fraser GE, Freudenheim JL, Goldbohm RA, Hankinson SE, Jacobs DR Jr, Koushik A, Lacey JV Jr, Larsson SC, Leitzmann M, McCullough ML, Miller AB, Rodriguez C, Rohan TE, Scheuten LJ, Shore R, Smit E, Wolk A, Zhang SM, Smith-Warner SA (2006) Dairy products and ovarian cancer: a pooled analysis of 12 cohort studies. Cancer Epidemiol Biomark Prev 15(2):364–372. https://doi.org/10.1158/1055-9965.EPI-05-0484
Fairfield KM, Hunter DJ, Colditz GA, Fuchs CS, Cramer DW, Speizer FE, Willett WC, Hankinson SE (2004) A prospective study of dietary lactose and ovarian cancer. Int J Cancer 110(2):271–277. https://doi.org/10.1002/ijc.20086
Larsson SC, Bergkvist L, Wolk A (2004) Milk and lactose intakes and ovarian cancer risk in the Swedish Mammography Cohort. Am J Clin Nutr 80(5):1353–1357. https://doi.org/10.1093/ajcn/80.5.1353
Rice MS, Poole EM, Willett WC, Tworoger SS (2019) Adult dietary fat intake and ovarian cancer risk. Int J Cancer. https://doi.org/10.1002/ijc.32635
Merritt MA, Riboli E, Weiderpass E, Tsilidis KK, Overvad K, Tjonneland A, Hansen L, Dossus L, Fagherazzi G, Baglietto L, Fortner RT, Ose J, Steffen A, Boeing H, Trichopoulou A, Trichopoulos D, Lagiou P, Masala G, Sieri S, Mattiello A, Tumino R, Sacerdote C, Bueno-de-Mesquita HB, Onland-Moret NC, Peeters PH, Hjartaker A, Gram IT, Quiros JR, Obon-Santacana M, Molina-Montes E, Huerta Castano JM, Ardanaz E, Chamosa S, Sonestedt E, Idahl A, Lundin E, Khaw KT, Wareham N, Travis RC, Rinaldi S, Romieu I, Chajes V, Gunter MJ (2014) Dietary fat intake and risk of epithelial ovarian cancer in the European Prospective Investigation into Cancer and Nutrition. Cancer Epidemiol 38(5):528–537. https://doi.org/10.1016/j.canep.2014.07.011
Laake I, Carlsen MH, Pedersen JI, Weiderpass E, Selmer R, Kirkhus B, Thune I, Veierød MB (2013) Intake of trans fatty acids from partially hydrogenated vegetable and fish oils and ruminant fat in relation to cancer risk. Int J Cancer 132(6):1389–1403. https://doi.org/10.1002/ijc.27737
Blank MM, Wentzensen N, Murphy MA, Hollenbeck A, Park Y (2012) Dietary fat intake and risk of ovarian cancer in the NIH-AARP Diet and Health Study. Br J Cancer 106(3):596–602. https://doi.org/10.1038/bjc.2011.572
Arthur R, Brasky TM, Crane TE, Felix AS, Kaunitz AM, Shadyab AH, Qi L, Wassertheil-Smoller S, Rohan TE (2019) Associations of a healthy lifestyle index with the risks of endometrial and ovarian cancer among women in the Women’s Health Initiative Study. Am J Epidemiol 188(2):261–273. https://doi.org/10.1093/aje/kwy249
Arthur R, Kirsh VA, Kreiger N, Rohan T (2018) A healthy lifestyle index and its association with risk of breast, endometrial, and ovarian cancer among Canadian women. Cancer Causes Control 29(6):485–493. https://doi.org/10.1007/s10552-018-1032-1
Yang HP, Trabert B, Murphy MA, Sherman ME, Sampson JN, Brinton LA, Hartge P, Hollenbeck A, Park Y, Wentzensen N (2012) Ovarian cancer risk factors by histologic subtypes in the NIH-AARP diet and health study. Int J Cancer 131(4):938–948. https://doi.org/10.1002/ijc.26469
Weiderpass E, Sandin S, Inoue M, Shimazu T, Iwasaki M, Sasazuki S, Sawada N, Yamaji T, Tsugane S (2012) Risk factors for epithelial ovarian cancer in Japan—results from the Japan Public Health Center-based Prospective Study cohort. Int J Oncol 40(1):21–30. https://doi.org/10.3892/ijo.2011.1194
Allen NE, Beral V, Casabonne D, Kan SW, Reeves GK, Brown A, Green J (2009) Moderate alcohol intake and cancer incidence in women. J Natl Cancer Inst 101(5):296–305. https://doi.org/10.1093/jnci/djn514
Tworoger SS, Gertig DM, Gates MA, Hecht JL, Hankinson SE (2008) Caffeine, alcohol, smoking, and the risk of incident epithelial ovarian cancer. Cancer 112(5):1169–1177. https://doi.org/10.1002/cncr.23275
Kabat GC, Miller AB, Jain M, Rohan TE (2008) Dietary intake of selected B vitamins in relation to risk of major cancers in women. Br J Cancer 99(5):816–821. https://doi.org/10.1038/sj.bjc.6604540
Chang ET, Canchola AJ, Lee VS, Clarke CA, Purdie DM, Reynolds P, Bernstein L, Stram DO, Anton-Culver H, Deapen D, Mohrenweiser H, Peel D, Pinder R, Ross RK, West DW, Wright W, Ziogas A, Horn-Ross PL (2007) Wine and other alcohol consumption and risk of ovarian cancer in the California Teachers Study cohort. Cancer Causes Control 18(1):91–103. https://doi.org/10.1007/s10552-006-0083-x
Navarro Silvera SA, Jain M, Howe GR, Miller AB, Rohan TE (2006) Dietary folate consumption and risk of ovarian cancer: a prospective cohort study. Eur J Cancer Prev 15(6):511–515. https://doi.org/10.1097/01.cej.0000220627.54986.bf
Genkinger JM, Hunter DJ, Spiegelman D, Anderson KE, Buring JE, Freudenheim JL, Goldbohm RA, Harnack L, Hankinson SE, Larsson SC, Leitzmann M, McCullough ML, Marshall J, Miller AB, Rodriguez C, Rohan TE, Schatzkin A, Schouten LJ, Wolk A, Zhang SM, Smith-Warner SA (2006) Alcohol intake and ovarian cancer risk: a pooled analysis of 10 cohort studies. Br J Cancer 94(5):757–762. https://doi.org/10.1038/sj.bjc.6603020
Tworoger SS, Hecht JL, Giovannucci E, Hankinson SE (2006) Intake of folate and related nutrients in relation to risk of epithelial ovarian cancer. Am J Epidemiol 163(12):1101–1111. https://doi.org/10.1093/aje/kwj128
Schouten LJ, Zeegers MPA, Goldbohm RA, Van Den Brandt PA (2004) Alcohol and ovarian cancer risk: results from the Netherlands Cohort Study. Cancer Causes Control 15(2):201–209. https://doi.org/10.1023/B:CACO.0000019512.71560.2b
Larsson SC, Wolk A (2004) Wine consumption and epithelial ovarian cancer. Cancer Epidemiol Biomark Prev 13(11Pt1):1823–1824
Kelemen LE, Sellers TA, Vierkant RA, Harnack L, Cerhan JR (2004) Association of folate and alcohol with risk of ovarian cancer in a prospective study of postmenopausal women. Cancer Causes Control 15(10):1085–1093. https://doi.org/10.1007/s10552-004-1546-6
Larsson SC, Giovannucci E, Wolk A (2004) Dietary folate intake and incidence of ovarian cancer: the Swedish mammography cohort. J Natl Cancer Inst 96(5):396–402. https://doi.org/10.1093/jnci/djh061
Arthur RS, Kirsh VA, Rohan TE (2019) Dietary B-vitamin intake and risk of breast, endometrial, ovarian and colorectal cancer among Canadians. Nutr Cancer 71(7):1067–1077. https://doi.org/10.1080/01635581.2019.1597904
Koushik A, Wang M, Anderson KE, van den Brandt P, Clendenen TV, Eliassen AH, Freudenheim JL, Genkinger JM, Håkansson N, Marshall JR, McCullough ML, Miller AB, Robien K, Rohan TE, Schairer C, Schouten LJ, Tworoger SS, Wang Y, Wolk A, Zeleniuch-Jacquotte A, Smith-Warner SA (2015) Intake of vitamins A, C, and E and folate and the risk of ovarian cancer in a pooled analysis of 10 cohort studies. Cancer Causes Control 26(9):1315–1327. https://doi.org/10.1007/s10552-015-0626-0
Cassidy A, Huang T, Rice MS, Rimm EB, Tworoger SS (2014) Intake of dietary flavonoids and risk of epithelial ovarian cancer. Am J Clin Nutr 100(5):1344–1351. https://doi.org/10.3945/ajcn.114.088708
Prescott J, Bertrand KA, Poole EM, Rosner BA, Tworoger SS (2013) Surrogates of long-term vitamin D exposure and ovarian cancer risk in two prospective cohort studies. Cancers (Basel) 5(4):1577–1600. https://doi.org/10.3390/cancers5041577
Kotsopoulos J, Hankinson SE, Tworoger SS (2010) Dietary betaine and choline intake are not associated with risk of epithelial ovarian cancer. Eur J Clin Nutr 64(1):111–114. https://doi.org/10.1038/ejcn.2009.109
Wang L, Lee IM, Zhang SM, Blumberg JB, Buring JE, Sesso HD (2009) Dietary intake of selected flavonols, flavones, and flavonoid-rich foods and risk of cancer in middle-aged and older women. Am J Clin Nutr 89(3):905–912. https://doi.org/10.3945/ajcn.2008.26913
Thomson CA, Neuhouser ML, Shikany JM, Caan BJ, Monk BJ, Mossavar-Rahmani Y, Sarto G, Parker LM, Modugno F, Anderson GL (2008) The role of antioxidants and vitamin A in ovarian cancer: results from the women’s health initiative. Nutr Cancer 60(6):710–719. https://doi.org/10.1080/01635580802233983
Silvera SAN, Jain M, Howe GR, Miller AB, Rohan TE (2007) Dietary fiber intake and ovarian cancer risk: a prospective cohort study. Cancer Causes Control 18(3):335–341. https://doi.org/10.1007/s10552-006-0107-6
Koushik A, Hunter DJ, Spiegelman D, Anderson KE, Buring JE, Freudenheim JL, Goldbohm RA, Hankinson SE, Larsson SC, Leitzmann M, Marshall JR, McCullough ML, Miller AB, Rodriguez C, Rohan TE, Ross JA, Schatzkin A, Schouten LJ, Willett WC, Wolk A, Zhang SM, Smith-Warner SA (2006) Intake of the major carotenoids and the risk of epithelial ovarian cancer in a pooled analysis of 10 cohort studies. Int J Cancer 119(9):2148–2154. https://doi.org/10.1002/ijc.22076
Silvera SA, Jain M, Howe GR, Miller AB, Rohan TE (2006) Carotenoid, vitamin A, vitamin C, and vitamin E intake and risk of ovarian cancer: a prospective cohort study. Cancer Epidemiol Biomark Prev 15(2):395–397. https://doi.org/10.1158/1055-9965.epi-05-0835
Arts IC, Jacobs DR Jr, Gross M, Harnack LJ, Folsom AR (2002) Dietary catechins and cancer incidence among postmenopausal women: the Iowa Women’s Health Study (United States). Cancer Causes Control 13(4):373–382
Arthur R, Kirsh VA, Rohan TE (2018) Associations of coffee, tea and caffeine intake with risk of breast, endometrial and ovarian cancer among Canadian women. Cancer Epidemiol 56:75–82. https://doi.org/10.1016/j.canep.2018.07.013
Park SY, Freedman ND, Haiman CA, Le Marchand L, Wilkens LR, Setiawan VW (2018) Prospective study of coffee consumption and cancer incidence in non-white populations. Cancer Epidemiol Biomark Prev 27(8):928–935. https://doi.org/10.1158/1055-9965.epi-18-0093
Gunter MJ, Murphy N, Cross AJ, Dossus L, Dartois L, Fagherazzi G, Kaaks R, Kühn T, Boeing H, Aleksandrova K, Tjønneland A, Olsen A, Overvad K, Larsen SC, Cornejo MLR, Agudo A, Pérez MJS, Altzibar JM, Navarro C, Ardanaz E, Khaw KT, Butterworth A, Bradbury KE, Trichopoulou A, Lagiou P, Trichopoulos D, Palli D, Grioni S, Vineis P, Panico S, Tumino R, Bueno-De-Mesquita B, Siersema P, Leenders M, Beulens JWJ, Uiterwaal CU, Wallström P, Nilsson LM, Landberg R, Weiderpass E, Skeie G, Braaten T, Brennan P, Licaj I, Muller DC, Sinha R, Wareham N, Riboli E (2017) Coffee drinking and mortality in 10 European countries: a multinational cohort study. Ann Intern Med 167(4):236–247. https://doi.org/10.7326/M16-2945
Lukic M, Licaj I, Lund E, Skeie G, Weiderpass E, Braaten T (2016) Coffee consumption and the risk of cancer in the Norwegian Women and Cancer (NOWAC) Study. Eur J Epidemiol 31(9):905–916. https://doi.org/10.1007/s10654-016-0142-x
Hashibe M, Galeone C, Buys SS, Gren L, Boffetta P, Zhang ZF, La Vecchia C (2015) Coffee, tea, caffeine intake, and the risk of cancer in the PLCO cohort. Br J Cancer 113(5):809–816. https://doi.org/10.1038/bjc.2015.276
Braem MGM, Onland-Moret NC, Schouten LJ, Tjønneland A, Hansen L, Dahm CC, Overvad K, Lukanova A, Dossus L, Floegel A, Boeing H, Clavel-Chapelon F, Chabbert-Buffet N, Fagherazzi G, Trichopoulou A, Benetou V, Goufa I, Pala V, Galasso R, Mattiello A, Sacerdote C, Palli D, Tumino R, Gram IT, Lund E, Gavrilyuk O, Sánchez MJ, Quirós R, Gonzales CA, Dorronsoro M, Huerta Castaño JM, Gurrea AB, Idahl A, Ohlson N, Lundin E, Jirstrom K, Wirfalt E, Allen NE, Tsilidis KK, Kaw KT, Bueno-de-Mesquita HB, Dik VK, Rinaldi S, Fedirko V, Norat T, Riboli E, Kaaks R, Peeters PHM (2012) Coffee and tea consumption and the risk of ovarian cancer: a prospective cohort study and updated meta-analysis. Am J Clin Nutr 95(5):1172–1181. https://doi.org/10.3945/ajcn.111.026393
Nilsson LM, Johansson I, Lenner P, Lindahl B, Van Guelpen B (2010) Consumption of filtered and boiled coffee and the risk of incident cancer: a prospective cohort study. Cancer Causes Control 21(10):1533–1544. https://doi.org/10.1007/s10552-010-9582-x
Lueth NA, Anderson KE, Harnack LJ, Fulkerson JA, Robien K (2008) Coffee and caffeine intake and the risk of ovarian cancer: the Iowa Women’s Health Study. Cancer Causes Control 19(10):1365–1372. https://doi.org/10.1007/s10552-008-9208-8
Steevens J, Schouten LJ, Verhage BAJ, Goldbohm RA, Van Den Brandt PA (2007) Tea and coffee drinking and ovarian cancer risk: results from the Netherlands Cohort Study and a meta-analysis. Br J Cancer 97(9):1291–1294. https://doi.org/10.1038/sj.bjc.6604008
Silvera SA, Jain M, Howe GR, Miller AB, Rohan TE (2007) Intake of coffee and tea and risk of ovarian cancer: a prospective cohort study. Nutr Cancer 58(1):22–27. https://doi.org/10.1080/01635580701307945
Larsson SC, Wolk A (2005) Coffee consumption is not associated with ovarian cancer incidence. Cancer Epidemiol Biomark Prev 14(9):2273–2274. https://doi.org/10.1158/1055-9965.EPI-05-0280
Larsson SC, Wolk A (2005) Tea consumption and ovarian cancer risk in a population-based cohort. Arch Intern Med 165(22):2683–2686. https://doi.org/10.1001/archinte.165.22.2683
Zhang M, Lee AH, Binns CW, Xie X (2004) Green tea consumption enhances survival of epithelial ovarian cancer. Int J Cancer 112(3):465–469. https://doi.org/10.1002/ijc.20456
Zheng W, Doyle TJ, Kushi LH, Sellers TA, Hong CP, Folsom AR (1996) Tea consumption and cancer incidence in a prospective cohort study of postmenopausal women. Am J Epidemiol 144(2):175–182
Stensvold I, Jacobsen BK (1994) Coffee and cancer: a prospective study of 43,000 Norwegian men and women. Cancer Causes Control 5(5):401–408
Jacobsen BK, Bjelke E, Kvåle G, Heuch I (1986) Coffee drinking, mortality, and cancer incidence: results from a Norwegian prospective study. J Natl Cancer Inst 76(5):823–831
Snowdon DA, Phillips RL (1984) Coffee consumption and risk of fatal cancers. Am J Public Health 74(8):820–823
Kotemori A, Ishihara J, Zha L, Liu R, Sawada N, Iwasaki M, Sobue T, Tsugane S (2018) Dietary acrylamide intake and the risk of endometrial or ovarian cancers in Japanese women. Cancer Sci 109(10):3316–3325. https://doi.org/10.1111/cas.13757
Inoue-Choi M, Weyer PJ, Jones RR, Booth BJ, Cantor KP, Robien K, Ward MH (2016) Atrazine in public water supplies and risk of ovarian cancer among postmenopausal women in the Iowa Women’s Health Study. Occup Environ Med 73(9):582–587. https://doi.org/10.1136/oemed-2016-103575
Donat-Vargas C, Akesson A, Berglund M, Glynn A, Wolk A, Kippler M (2016) Dietary exposure to polychlorinated biphenyls and risk of breast, endometrial and ovarian cancer in a prospective cohort. Br J Cancer 115(9):1113–1121. https://doi.org/10.1038/bjc.2016.282
Obón-Santacana M, Peeters PHM, Freisling H, Dossus L, Clavel-Chapelon F, Baglietto L, Schock H, Fortner RT, Boeing H, Tjønneland A, Olsen A, Overvad K, Menéndez V, Sanchez MJ, Larrañaga N, Castaño JMH, Barricarte A, Khaw KT, Wareham N, Travis RC, Merritt MA, Trichopoulou A, Trichopoulos D, Orfanos P, Masala G, Sieri S, Tumino R, Vineis P, Mattiello A, Bueno-De-Mesquita HB, Onland-Moret NC, Wirfält E, Stocks T, Idahl A, Lundin E, Skeie G, Gram IT, Weiderpass E, Riboli E, Duell EJ (2015) Dietary intake of acrylamide and epithelial ovarian cancer risk in the European prospective investigation into cancer and nutrition (EPIC) cohort. Cancer Epidemiol Biomark Prev 24(1):291–297. https://doi.org/10.1158/1055-9965.EPI-14-0636
Inoue-Choi M, Jones RR, Anderson KE, Cantor KP, Cerhan JR, Krasner S, Robien K, Weyer PJ, Ward MH (2015) Nitrate and nitrite ingestion and risk of ovarian cancer among postmenopausal women in Iowa. Int J Cancer 137(1):173–182. https://doi.org/10.1002/ijc.29365
Adams SV, Quraishi SM, Shafer MM, Passarelli MN, Freney EP, Chlebowski RT, Luo J, Meliker JR, Mu L, Neuhouser ML, Newcomb PA (2014) Dietary cadmium exposure and risk of breast, endometrial, and ovarian cancer in the Women’s Health Initiative. Environ Health Perspect 122(6):594–600. https://doi.org/10.1289/ehp.1307054
Eriksen KT, Halkjær J, Sørensen M, Meliker JR, McElroy JA, Tjønneland A, Raaschou-Nielsen O (2014) Dietary cadmium intake and risk of breast, endometrial and ovarian cancer in Danish postmenopausal women: a prospective cohort study. PloS One 9(6):e100815. https://doi.org/10.1371/journal.pone.0100815
Aschebrook-Kilfoy B, Ward MH, Gierach GL, Schatzkin A, Hollenbeck AR, Sinha R, Cross AJ (2012) Epithelial ovarian cancer and exposure to dietary nitrate and nitrite in the NIH-AARP Diet and Health Study. Eur J Cancer Prev 21(1):65–72. https://doi.org/10.1097/CEJ.0b013e328347622f
Loh YH, Jakszyn P, Luben RN, Mulligan AA, Mitrou PN, Khaw KT (2011) N-nitroso compounds and cancer incidence: the European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk Study. Am J Clin Nutr 93(5):1053–1061. https://doi.org/10.3945/ajcn.111.012377
Julin B, Wolk A, Åkesson A (2011) Dietary cadmium exposure and risk of epithelial ovarian cancer in a prospective cohort of Swedish women. Br J Cancer 105(3):441–444. https://doi.org/10.1038/bjc.2011.238
Wilson KM, Mucci LA, Rosner BA, Willett WC (2010) A prospective study on dietary acrylamide intake and the risk for breast, endometrial, and ovarian cancers. Cancer Epidemiol Biomark Prev 19(10):2503–2515. https://doi.org/10.1158/1055-9965.epi-10-0391
Larsson SC, Akesson A, Wolk A (2009) Long-term dietary acrylamide intake and risk of epithelial ovarian cancer in a prospective cohort of Swedish women. Cancer Epidemiol Biomark Prev 18(3):994–997. https://doi.org/10.1158/1055-9965.epi-08-0868
Hogervorst JG, Schouten LJ, Konings EJ, Goldbohm RA, Van Den Brandt PA (2007) A prospective study of dietary acrylamide intake and the risk of endometrial, ovarian, and breast cancer. Cancer Epidemiol Biomark Prev 16(11):2304–2313. https://doi.org/10.1158/1055-9965.EPI-07-0581
Weyer PJ, Cerhan JR, Kross BC, Hallberg GR, Kantamneni J, Breuer G, Jones MP, Zheng W, Lynch CF (2001) Municipal drinking water nitrate level and cancer risk in older women: the Iowa women’s health study. Epidemiology 12(3):327–338. https://doi.org/10.1097/00001648-200105000-00013
Tasevska N, Jiao L, Cross AJ, Kipnis V, Subar AF, Hollenbeck A, Schatzkin A, Potischman N (2012) Sugars in diet and risk of cancer in the NIH-AARP Diet and Health Study. Int J Cancer 130(1):159–169. https://doi.org/10.1002/ijc.25990
Silvera SAN, Jain M, Howe GR, Miller AB, Rohan TE (2007) Glycaemic index, glycaemic load and ovarian cancer risk: a prospective cohort study. Public Health Nutr 10(10):1076–1081. https://doi.org/10.1017/S1368980007696360
World Cancer Research Fund/American Institute for Cancer Research: diet, nutrition, physical activity and ovarian cancer. Continuous Update Project Expert Report (2018) https://www.wcrf.org/dietandcancer/ovarian-cancer. Accessed 17 May 2019
Qu XL, Fang Y, Zhang M, Zhang YZ (2014) Phytoestrogen intake and risk of ovarian cancer: a meta-analysis of 10 observational studies. Asian Pac J Cancer Prev 15(21):9085–9091. https://doi.org/10.7314/APJCP.2014.15.21.9085
Myung SK, Ju W, Choi HJ, Kim SC (2009) Soy intake and risk of endocrine-related gynaecological cancer: a meta-analysis. BJOG Int J Obs Gynaecol 116(13):1697–1705. https://doi.org/10.1111/j.1471-0528.2009.02322.x
Hu J, Hu Y, Hu Y, Zheng S (2015) Intake of cruciferous vegetables is associated with reduced risk of ovarian cancer: a meta-analysis. Asia Pac J Clin Nutr 24(1):101–109. https://doi.org/10.6133/apjcn.2015.24.1.22
Song X, Li Z, Ji X, Zhang D (2017) Calcium intake and the risk of ovarian cancer: a meta-analysis. Nutrients 9(7):679. https://doi.org/10.3390/nu9070679
Huang X, Wang X, Shang J, Lin Y, Yang Y, Song Y, Yu S (2018) Association between dietary fiber intake and risk of ovarian cancer: a meta-analysis of observational studies. J Int Med Res 46(10):3995–4005. https://doi.org/10.1177/0300060518792801
Xu H, Ding Y, Xin X, Wang W, Zhang D (2018) Dietary fiber intake is associated with a reduced risk of ovarian cancer: a dose-response meta-analysis. Nutr Res 57:1–11. https://doi.org/10.1016/j.nutres.2018.04.011
Li X, Xu J (2014) Meta-analysis of the association between dietary lycopene intake and ovarian cancer risk in postmenopausal women. Sci Rep. https://doi.org/10.1038/srep04885
Zhan X, Wang J, Pan S, Lu C (2017) Tea consumption and the risk of ovarian cancer: a meta-analysis of epidemiological studies. Oncotarget 8(23):37796–37806. https://doi.org/10.18632/oncotarget.16890
Butler LM, Wu AH (2011) Green and black tea in relation to gynecologic cancers. Mol Nutr Food Res 55(6):931–940. https://doi.org/10.1002/mnfr.201100058
Block G, Patterson B, Subar A (1992) Fruit, vegetables, and cancer prevention: a review of the epidemiological evidence. Nutr Cancer 18(1):1–29. https://doi.org/10.1080/01635589209514201
Wu QJ, Yang Y, Vogtmann E, Wang J, Han LH, Li HL, Xiang YB (2013) Cruciferous vegetables intake and the risk of colorectal cancer: a meta-analysis of observational studies. Ann Oncol 24(4):1079–1087. https://doi.org/10.1093/annonc/mds601
Wang Q, Chen Y, Wang X, Gong G, Li G, Li C (2014) Consumption of fruit, but not vegetables, may reduce risk of gastric cancer: results from a meta-analysis of cohort studies. Eur J Cancer 50(8):1498–1509. https://doi.org/10.1016/j.ejca.2014.02.009
Li J, Zou L, Chen W, Zhu B, Shen N, Ke J, Lou J, Song R, Zhong R, Miao X (2014) Dietary mushroom intake may reduce the risk of breast cancer: evidence from a meta-analysis of observational studies. PLoS One 9(4):e93437. https://doi.org/10.1371/journal.pone.0093437
Fabiani R, Minelli L, Rosignoli P (2016) Apple intake and cancer risk: a systematic review and meta-analysis of observational studies. Public Health Nutr 19(14):2603–2617. https://doi.org/10.1017/s136898001600032x
Le Ngoc TN, Oh YK, Lee YJ, Lee YC (2018) Effects of Sparassis crispa in medical therapeutics: a systematic review and meta-analysis of randomized controlled trials. Int J Mol Sci 19(5):1487. https://doi.org/10.3390/ijms19051487
Zhang M, Yang ZY, Binns CW, Lee AH (2002) Diet and ovarian cancer risk: a case-control study in China. Br J Cancer 86(5):712–717. https://doi.org/10.1038/sj.bjc.6600085
Ren JS, Kamangar F, Forman D, Islami F (2012) Pickled food and risk of gastric cancer- a systematic review and meta-analysis of English and Chinese literature. Cancer Epidemiol Biomark Prev 21(6):905–915. https://doi.org/10.1158/1055-9965.epi-12-0202
Russo M, Spagnuolo C, Tedesco I, Russo GL (2010) Phytochemicals in cancer prevention and therapy: truth or dare? Toxins 2(4):517–551. https://doi.org/10.3390/toxins2040517
Soundararajan P, Kim JS (2018) Anti-carcinogenic glucosinolates in cruciferous vegetables and their antagonistic effects on prevention of cancers. Molecules 23(11):2983. https://doi.org/10.3390/molecules23112983
Tanaka T, Makita H, Kawabata K, Mori H, Kakumoto M, Satoh K, Hara A, Sumida T, Tanaka T, Ogawa H (1997) Chemoprevention of azoxymethane-induced rat colon carcinogenesis by the naturally occurring flavonoids, diosmin and hesperidin. Carcinogenesis 18(5):957–965. https://doi.org/10.1093/carcin/18.5.957
Reyes-Farias Marjorie, Carrasco-Pozo Catalina (2019) The anti-cancer effect of quercetin: molecular implications in cancer metabolism. Int J Mol Sci 20(13):3177. https://doi.org/10.3390/ijms20133177
Gunathilake KDPP, Ranaweera KKDS, Vasantha Rupasinghe HP (2018) In vitro anti-inflammatory properties of selected green leafy vegetables. Biomedicines 6(4):107. https://doi.org/10.3390/biomedicines6040107
Kim SH, Choi KC (2013) Anti-cancer effect and underlying mechanism(s) of kaempferol, a phytoestrogen, on the regulation of apoptosis in diverse cancer cell models. Toxicol Res 29(4):229–234. https://doi.org/10.5487/tr.2013.29.4.229
Liu H, Liu J, Wang S, Zeng Z, Li T, Liu Y, Mastriani E, Li QH, Bao HX, Zhou YJ, Wang X, Hu S, Gao S, Qi Y, Shen Z, Wang H, Yu M, Gao T, Johnston RN, Liu SL (2017) Enterolactone has stronger effects than enterodiol on ovarian cancer. J Ovarian Res 10(1):49. https://doi.org/10.1186/s13048-017-0346-z
Sturm C, Wagner AE (2017) Brassica-derived plant bioactives as modulators of chemopreventive and inflammatory signaling pathways. Int J Mol Sci 18(9):1890. https://doi.org/10.3390/ijms18091890
Loganathan S, Kandala PK, Gupta P, Srivastava SK (2012) Inhibition of EGFR-AKT axis results in the suppression of ovarian tumors in vitro and in preclinical mouse model. PloS One 7(8):e43577. https://doi.org/10.1371/journal.pone.0043577
Huncharek M, Klassen H, Kupelnick B (2001) Dietary beta-carotene intake and the risk of epithelial ovarian cancer: a meta-analysis of 3,782 subjects from five observational studies. Vivo 15(4):339–343
Cramer DW, Kuper H, Harlow BL, Titus-Ernstoff L (2001) Carotenoids, antioxidants and ovarian cancer risk in pre- and postmenopausal women. Int J Cancer 94(1):128–134. https://doi.org/10.1002/ijc.1435
Lee AH, Pasalich M, Su D, Tang L, Tran VD, Binns CW (2013) Mushroom intake and risk of epithelial ovarian cancer in Southern Chinese women. Int J Gynecol Cancer 23(8):1400–1405. https://doi.org/10.1097/IGC.0b013e3182a41dd8
Hetland G, Johnson E, Lyberg T, Bernardshaw S, Tryggestad AM, Grinde B (2008) Effects of the medicinal mushroom Agaricus blazei Murill on immunity, infection and cancer. Scand J Immunol 68(4):363–370. https://doi.org/10.1111/j.1365-3083.2008.02156.x
Dai S, Liu J, Sun X, Wang N (2014) Ganoderma lucidum inhibits proliferation of human ovarian cancer cells by suppressing VEGF expression and up-regulating the expression of connexin 43. BMC Complement Altern Med 14:434. https://doi.org/10.1186/1472-6882-14-434
Figueiredo L, Régis WCB (2017) Medicinal mushrooms in adjuvant cancer therapies: an approach to anticancer effects and presumed mechanisms of action. Nutrire 42(1):28. https://doi.org/10.1186/s41110-017-0050-1
Firenzuoli F, Gori L, Lombardo G (2008) The Medicinal mushroom Agaricus blazei Murrill: review of literature and pharmaco-toxicological problems. Evid Based Complement Altern Med 5(1):3–15. https://doi.org/10.1093/ecam/nem007
Wallin A, Orsini N, Wolk A (2011) Red and processed meat consumption and risk of ovarian cancer: a dose-response meta-analysis of prospective studies. Br J Cancer 104(7):1196–1201. https://doi.org/10.1038/bjc.2011.49
Kolahdooz F, Van Der Pols JC, Bain CJ, Marks GC, Hughes MC, Whiteman DC, Webb PM (2010) Meat, fish, and ovarian cancer risk: results from 2 Australian case-control studies, a systematic review, and meta-analysis. Am J Clin Nutr 91(6):1752–1763. https://doi.org/10.3945/ajcn.2009.28415
Jiang PY, Jiang ZB, Shen KX, Yue Y (2014) Fish intake and ovarian cancer risk: a meta-analysis of 15 case-control and cohort studies. PLoS One 9(4):e94601. https://doi.org/10.1371/journal.pone.0094601
zur Hausen H (2012) Red meat consumption and cancer: reasons to suspect involvement of bovine infectious factors in colorectal cancer. Int J Cancer 130(11):2475–2483. https://doi.org/10.1002/ijc.27413
Tavani A, Pelucchi C, Parpinel M, Negri E, Franceschi S, Levi F, La Vecchia C (2003) n-3 polyunsaturated fatty acid intake and cancer risk in Italy and Switzerland. Int J Cancer 105(1):113–116. https://doi.org/10.1002/ijc.11018
Qiu W, Lu H, Qi Y, Wang X (2016) Dietary fat intake and ovarian cancer risk: a meta-analysis of epidemiological studies. Oncotarget 7(24):37390–37406. https://doi.org/10.18632/oncotarget.8940
Hoang T, Myung SK, Pham TT (2018) Dietary intake of omega-3 fatty acids and endocrine-related gynecological cancer: a meta-analysis of observational studies. Cancer Res Treat. https://doi.org/10.4143/crt.2018.473
Zeng ST, Guo L, Liu SK, Wang DH, Xi J, Huang P, Liu DT, Gao JF, Feng J, Zhang L (2015) Egg consumption is associated with increased risk of ovarian cancer: evidence from a meta-analysis of observational studies. Clin Nutr 34(4):635–641. https://doi.org/10.1016/j.clnu.2014.07.009
Keum N, Lee DH, Marchand N, Oh H, Liu H, Aune D, Greenwood DC, Giovannucci EL (2015) Egg intake and cancers of the breast, ovary and prostate: a dose-response meta-analysis of prospective observational studies. Br J Nutr 114(7):1099–1107. https://doi.org/10.1017/S0007114515002135
Hu J, La Vecchia C, de Groh M, Negri E, Morrison H, Mery L (2012) Dietary cholesterol intake and cancer. Ann Oncol 23(2):491–500. https://doi.org/10.1093/annonc/mdr155
Layton DW, Bogen KT, Knize MG, Hatch FT, Johnson VM, Felton JS (1995) Cancer risk of heterocyclic amines in cooked foods: an analysis and implications for research. Carcinogenesis 16(1):39–52. https://doi.org/10.1093/carcin/16.1.39
Jeyaraman MM, Abou-Setta AM, Grant L, Farshidfar F, Copstein L, Lys J, Gottschalk T, Desautels D, Czaykowski P, Pitz M, Zarychanski R (2019) Dairy product consumption and development of cancer: an overview of reviews. BMJ Open 9(1):e023625. https://doi.org/10.1136/bmjopen-2018-023625
Lu W, Chen H, Niu Y, Wu H, Xia D, Wu Y (2016) Dairy products intake and cancer mortality risk: a meta-analysis of 11 population-based cohort studies. Nutr J 15(1):91. https://doi.org/10.1186/s12937-016-0210-9
Larsson SC, Orsini N, Wolk A (2006) Milk, milk products and lactose intake and ovarian cancer risk: a meta-analysis of epidemiological studies. Int J Cancer 118(2):431–441. https://doi.org/10.1002/ijc.21305
Centeno V, de Barboza GD, Marchionatti A, Rodriguez V, Tolosa de Talamoni N (2009) Molecular mechanisms triggered by low-calcium diets. Nutr Res Rev 22(2):163–174. https://doi.org/10.1017/s0954422409990126
Davoodi H, Esmaeili S, Mortazavian AM (2013) Effects of milk and milk products consumption on cancer: a review. Compr Rev Food Sci Food Saf 12(3):249–264. https://doi.org/10.1111/1541-4337.12011
Amiri M, Diekmann L, von Köckritz-Blickwede M, Naim HY (2015) The diverse forms of lactose intolerance and the putative linkage to several cancers. Nutrients 7(9):7209–7230. https://doi.org/10.3390/nu7095332
Huncharek M, Kupelnick B (2001) Dietary fat intake and risk of epithelial ovarian cancer: a meta-analysis of 6,689 subjects from 8 observational studies. Nutr Cancer 40(2):87–91. https://doi.org/10.1207/s15327914nc402_2
Sadeghi A, Shab-Bidar S, Parohan M, Djafarian K (2019) Dietary fat intake and risk of ovarian cancer: a systematic review and dose-response meta-analysis of observational studies. Nutr Cancer 71(6):939–953. https://doi.org/10.1080/01635581.2019.1595049
Hou R, Wu QJ, Gong TT, Jiang L (2015) Dietary fat and fatty acid intake and epithelial ovarian cancer risk: evidence from epidemiological studies. Oncotarget 6(40):43099–43119. https://doi.org/10.18632/oncotarget.5525
Tania M, Khan MA, Song Y (2010) Association of lipid metabolism with ovarian cancer. Curr Oncol 17(5):6–11
Bagnardi V, Blangiardo M, La Vecchia C, Corrao G (2001) A meta-analysis of alcohol drinking and cancer risk. Br J Cancer 85(11):1700–1705. https://doi.org/10.1054/bjoc.2001.2140
Webb PM, Purdie DM, Bain CJ, Green AC (2004) Alcohol, wine, and risk of epithelial ovarian cancer. Cancer Epidemiol Biomark Prev 13(4):592–599
Kim HS, Kim JW, Shouten LJ, Larsson SC, Chung HH, Kim YB, Ju W, Park NH, Song YS, Kim SC, Kang SB (2010) Wine drinking and epithelial ovarian cancer risk: a meta-analysis. J Gynecol Oncol 21(2):112–118. https://doi.org/10.3802/jgo.2010.21.2.112
Rota M, Pasquali E, Scotti L, Pelucchi C, Tramacere I, Islami F, Negri E, Boffetta P, Bellocco R, Corrao G, La Vecchia C, Bagnardi V (2012) Alcohol drinking and epithelial ovarian cancer risk. A systematic review and meta-analysis. Gynecol Oncol 125(3):758–763. https://doi.org/10.1016/j.ygyno.2012.03.031
de Menezes RF, Bergmann A, Thuler LC (2013) Alcohol consumption and risk of cancer: a systematic literature review. Asian Pac J Cancer Prev 14(9):4965–4972
Yan-Hong H, Jing L, Hong L, Shan-Shan H, Yan L, Ju L (2015) Association between alcohol consumption and the risk of ovarian cancer: a meta-analysis of prospective observational studies. BMC Public Health 15(1):223. https://doi.org/10.1186/s12889-015-1355-8
Ugai T, Kelemen LE, Mizuno M, Ong JS, Webb PM, Chenevix-Trench G, Wicklund KG, Doherty JA, Rossing MA, Thompson PJ, Wilkens LR, Carney ME, Goodman MT, Schildkraut JM, Berchuck A, Cramer DW, Terry KL, Cai H, Shu XO, Gao YT, Xiang YB, Van Den Berg D, Pike MC, Wu AH, Pearce CL, Matsuo K (2018) Ovarian cancer risk, ALDH2 polymorphism and alcohol drinking: Asian data from the Ovarian Cancer Association Consortium. Cancer Sci 109(2):435–445. https://doi.org/10.1111/cas.13470
Zheng B, Shen H, Han H, Han T, Qin Y (2018) Dietary fiber intake and reduced risk of ovarian cancer: a meta-analysis. Nutr J 17(1):99. https://doi.org/10.1186/s12937-018-0407-1
So FV, Guthrie N, Chambers AF, Moussa M, Carroll KK (1996) Inhibition of human breast cancer cell proliferation and delay of mammary tumourigenesis by flavonoids and citrus juices. Nutr Cancer 26(2):167–181. https://doi.org/10.1080/01635589609514473
Guthrie N, Carroll KK (1998) Inhibition of mammary cancer by citrus flavonoids. Adv Exp Med Biol 439:227–236. https://doi.org/10.1007/978-1-4615-5335-9_16
Sak K (2015) In vitro cytotoxic activity of flavonoids on human ovarian cancer cell lines. Cancer Sci Res 2(1):1–13. https://doi.org/10.15226/csroa.2015.00112
Mohammadi V, Dehghani S, Larijani B, Azadbakht L (2016) Ovarian cancer risk and nonisoflavone flavonoids intake: a systematic review of epidemiological studies. J Res Med Sci 21:123. https://doi.org/10.4103/1735-1995.196605
Luo H, Rankin GO, Juliano N, Jiang BH, Chen YC (2012) Kaempferol inhibits VEGF expression and in vitro angiogenesis through a novel ERK-NFkappaB-cMyc-p21 pathway. Food Chem 130(2):321–328. https://doi.org/10.1016/j.foodchem.2011.07.045
Kao YC, Zhou C, Sherman M, Laughton CA, Chen S (1998) Molecular basis of the inhibition of human aromatase (estrogen synthetase) by flavone and isoflavone phytoestrogens: a site-directed mutagenesis study. Environ Health Perspect 106(2):85–92. https://doi.org/10.1289/ehp.9810685
Pang Y, Wang W (2018) Dietary protein intake and risk of ovarian cancer: evidence from a meta-analysis of observational studies. Biosci Rep. https://doi.org/10.1042/bsr20181857
Ward PP, Paz E, Conneely OM (2005) Multifunctional roles of lactoferrin: a critical overview. Cell Mol Life Sci 62(22):2540–2548. https://doi.org/10.1007/s00018-005-5369-8
Bounous G (2000) Whey protein concentrate (WPC) and glutathione modulation in cancer treatment. Anticancer Res 20(6C):4785–4792
Peterlik M, Grant WB, Cross HS (2009) Calcium, vitamin D and cancer. Anticancer Res 29(9):3687–3698
Guo H, Guo J, Xie W, Yuan L, Sheng X (2018) The role of vitamin D in ovarian cancer: epidemiology, molecular mechanism and prevention. J Ovarian Res 11(1):1–8. https://doi.org/10.1186/s13048-018-0443-7
McCarty MF (2000) Parathyroid hormone may be a cancer promoter- an explanation for the decrease in cancer risk associated with ultraviolet light, calcium, and vitamin D. Med Hypotheses 54(3):475–482. https://doi.org/10.1054/mehy.1999.0880
Cook LS, Neilson HK, Lorenzetti DL, Lee RC (2010) A systematic literature review of vitamin D and ovarian cancer. Am J Obstet Gynecol 203(1):70.e71–70.e78. https://doi.org/10.1016/j.ajog.2010.01.062
Yin L, Grandi N, Raum E, Haug U, Arndt V, Brenner H (2011) Meta-analysis: circulating vitamin D and ovarian cancer risk. Gynecol Oncol 121(2):369–375. https://doi.org/10.1016/j.ygyno.2011.01.023
Zhou B, Yang L, Wang L, Shi Y, Zhu H, Tang N, Wang B (2007) The association of tea consumption with ovarian cancer risk: a meta-analysis. Am J Obstet Gynecol 197(6):594-e 591–596. https://doi.org/10.1016/j.ajog.2007.05.027
Oppeneer SJ, Robien K (2011) Tea consumption and epithelial ovarian cancer risk: a systematic review of observational studies. Nutr Cancer 63(6):817–826. https://doi.org/10.1080/01635581.2011.594210
Zhang YF, Xu Q, Lu J, Wang P, Zhang HW, Zhou L, Ma XQ, Zhou YH (2015) Tea consumption and the incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Eur J Cancer Prev 24(4):353–362. https://doi.org/10.1097/CEJ.0000000000000094
Xinqiang S, Mu Z, Lei C, Mun LY (2017) Bioinformatics analysis on molecular mechanism of green tea compound epigallocatechin-3-gallate against ovarian cancer. Clin Transl Sci 10(4):302–307. https://doi.org/10.1111/cts.12470
Schulze J, Melzer L, Smith L, Teschke R (2017) Green tea and its extracts in cancer prevention and treatment. Beverages 3(1):17. https://doi.org/10.3390/beverages3010017
Wang A, Wang S, Zhu C, Huang H, Wu L, Wan X, Yang X, Zhang H, Miao R, He L, Sang X, Zhao H (2016) Coffee and cancer risk: a meta-analysis of prospective observational studies. Sci Rep 6:33711. https://doi.org/10.1038/srep33711
Berretta M, Micek A, Lafranconi A, Rossetti S, Di Francia R, De Paoli P, Rossi P, Facchini G (2018) Coffee consumption is not associated with ovarian cancer risk: a dose-response meta-analysis of prospective cohort studies. Oncotarget 9(29):20807–20815. https://doi.org/10.18632/oncotarget.24829
Yu X, Bao Z, Zou J, Dong J (2011) Coffee consumption and risk of cancers: a meta-analysis of cohort studies. BMC Cancer 11:96. https://doi.org/10.1186/1471-2407-11-96
Salari-Moghaddam A, Milajerdi A, Surkan PJ, Larijani B, Esmaillzadeh A (2019) Caffeine, type of coffee, and risk of ovarian cancer: a dose-response meta-analysis of prospective studies. J Clin Endocrinol Metab 104(11):5349–5359. https://doi.org/10.1210/jc.2019-00637
Pelucchi C, Bosetti C, Galeone C, La Vecchia C (2015) Dietary acrylamide and cancer risk: an updated meta-analysis. Int J Cancer 136(12):2912–2922. https://doi.org/10.1002/ijc.29339
Pelucchi C, La Vecchia C, Bosetti C, Boyle P, Boffetta P (2011) Exposure to acrylamide and human cancer- a review and meta-analysis of epidemiologic studies. Ann Oncol 22(7):1487–1499. https://doi.org/10.1093/annonc/mdq610
Virk-Baker MK, Nagy TR, Barnes S, Groopman J (2014) Dietary acrylamide and human cancer: a systematic review of literature. Nutr Cancer 66(5):774–790. https://doi.org/10.1080/01635581.2014.916323
Xie L, Mo M, Jia HX, Liang F, Yuan J, Zhu J (2016) Association between dietary nitrate and nitrite intake and sitespecific cancer risk: evidence from observational studies. Oncotarget 7(35):56915–56932. https://doi.org/10.18632/oncotarget.10917
Sathiakumar N, MacLennan PA, Mandel J, Delzell E (2011) A review of epidemiologic studies of triazine herbicides and cancer. Crit Rev Toxicol 41(Suppl 1):1–34. https://doi.org/10.3109/10408444.2011.554793
Semren TZ, Zunec S, Pizent A (2018) Oxidative stress in triazine pesticide toxicity: a review of the main biomarker findings. Arh Hig Rada Toksikol 69(2):109–125. https://doi.org/10.2478/aiht-2018-69-3118
Huang P, Yang J, Ning J, Wang M, Song Q (2015) Atrazine triggers DNA damage response and induces DNA double-strand breaks in MCF-10A cells. Int J Mol Sci 16(7):14353–14368. https://doi.org/10.3390/ijms160714353
Mulholland HG, Murray LJ, Cardwell CR, Cantwell MM (2008) Dietary glycaemic index, glycaemic load and endometrial and ovarian cancer risk: a systematic review and meta-analysis. Br J Cancer 99(3):434–441. https://doi.org/10.1038/sj.bjc.6604496
Qin B, Moorman PG, Alberg AJ, Barnholtz-Sloan JS, Bondy M, Cote ML, Funkhouser E, Peters ES, Schwartz AG, Terry P, Schildkraut JM, Bandera EV (2015) Dietary carbohydrate intake, glycaemic load, glycaemic index and ovarian cancer risk in African-American women. Br J Nutr 115(4):694–702. https://doi.org/10.1017/S0007114515004882
Cui X, Rosner B, Willett WC, Hankinson SE (2010) Dietary fat, fiber, and carbohydrate intake and endogenous hormone levels in premenopausal women. Horm Cancer 1(5):265–276. https://doi.org/10.1007/s12672-010-0050-6
Doldo E, Costanza G, Agostinelli S, Tarquini C, Ferlosio A, Arcuri G, Passeri D, Scioli MG, Orlandi A (2015) Vitamin A, cancer treatment and prevention: the new role of cellular retinol binding proteins. BioMed Res Int. https://doi.org/10.1155/2015/624627
Acknowledgements
We thank Universiti Putra Malaysia for access to Scopus, PubMed, and Wiley Online Libraries.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors have made substantial contributions to the conception and design of the study. AFAR, AK and FA conducted the search and data extraction; AK and FA collected the data; AK and FA analyzed the data and wrote the manuscript. All authors read and approved the final content.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Ethical approval was not obtained as the data emanated from previously published studies.
Informed consent
Informed consent of patients was not obtained as the data emanated from previously published studies.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Khodavandi, A., Alizadeh, F. & Razis, A.F.A. Association between dietary intake and risk of ovarian cancer: a systematic review and meta-analysis. Eur J Nutr 60, 1707–1736 (2021). https://doi.org/10.1007/s00394-020-02332-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-020-02332-y