
Abstract
Secondary central nervous system (CNS) relapse is a serious and fatal complication of diffuse large B cell lymphoma (DLBCL). Data on secondary CNS (SCNS) relapse were mostly obtained from western countries with limited data from developing countries. We analyzed the data of 2034 newly diagnosed DLBCL patients enrolled into the multi-center registry under Thai Lymphoma Study Group from setting. The incidence, September 2006 to December 2013 to represent outcome from a resource limited pattern, management, and outcome of SCNS relapse were described. The 2-year cumulative incidence (CI) of SCNS relapse was 2.7 %. A total of 729, 1024, and 281 patients were classified as low-, intermediate-, and high-risk CNS international prognostic index (CNS-IPI) with corresponding 2-year CI of SCNS relapse of 1.5, 3.1, and 4.6 %, respectively (p < 0.001). Univariate analysis demonstrated advance stage disease, poor performance status, elevated lactate dehydrogenase, presence of B symptoms, more than one extranodal organ involvement, high IPI, and high CNS-IPI group as predictive factors for SCNS relapse. Rituximab exposure and intrathecal chemoprophylaxis offered no protective effect against SCNS relapse. At the time of analysis, six patients were alive. Median OS in SCNS relapsed patients was significantly shorter than relapsed patients without CNS involvement (13.2 vs 22.6 months) (p < 0.001). Primary causes of death were progressive disease (n = 35, 63.6 %) and infection (n = 9, 16.7 %). In conclusion, although the incidence of SCNS relapse in our cohort was low, the prognosis was dismal. Prophylaxis for SCNS involvement was underused even in high-risk patients. Novel approaches for SCNS relapse prophylaxis and managements are warranted.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the era of immunochemotherapy, treatment outcome of diffuse large B cell lymphoma (DLBCL) has significantly improved. However, approximately 30 % of patients eventually relapsed [1]. Secondary central nervous system (CNS) relapse remains one of the most important cause of treatment failure in DLBCL. The incidence of secondary CNS (SCNS) relapse ranges from 1 to more than 10 % [2–7]. Early data suggested the protective effect of rituximab against SCNS relapse [8]. However, subsequent studies showed conflicting results [3, 5, 7, 9]. Several studies identified varied parameters to stratify risk of SCNS relapse in DLBCL patients. Recently, the German High-Grade Non-Hodgkin’s Lymphoma Study Group (DSHNHL) proposed the simplified model so-called CNS international prognostic index (CNS-IPI) that stratified DLBCL patients into three groups [10] based on the presence of advanced stage, older age (>60 years old), impaired performance status, extranodal involvement more than one site, elevated lactate dehydrogenase, and kidney/adrenal gland involvement. Traditionally, CNS prophylactic intervention by either intrathecal (IT) chemotherapy or high-dose methotrexate (MTx) is incorporated to patients with high-risk features of SCNS relapse although its benefit is not consistently demonstrated [11–13]. Currently, researches describing SCNS relapse, risk stratification model, and management strategies were mostly conducted in western countries. The data of SCNS relapse in Asian countries were limited with most studies reporting results from either single institution or small numbers of patients [4, 14–16]. Herein, we demonstrate the pattern, management, outcome, and applicability of CNS-IPI for SCNS relapse in DLBCL patients from multi-institutional registry in a resource-limited country.
Patients and methods
Thai lymphoma study group (TLSG) is a multi-institutional collaborative panel of hematologists and hematopathologists from 13 major medical centers in Thailand. The detailed information of TLSG was described previously elsewhere [17]. The registry prospectively included newly diagnosed lymphoma patients aged older than 15 years old from all participating centers since September 2006. Detailed information including important baseline characteristics (age at diagnosis, gender, histopathology subtypes based on 2008 World Health Organization (WHO) classification for lymphoproliferative disorders, stage, extranodal organ involvement, lactic acid dehydrogenase (LDH), performance status (PS), international prognostic index (IPI), HIV serology status), frontline treatment modalities, response to first-line treatment, relapse status, salvage treatment, and follow-up data were collected into the web-based registry. Staging procedures at the time of diagnosis were based upon the Thai national guideline, which primarily included computed tomography (CT) or positron emission tomography (PET) and bone marrow biopsy. However, the decisions were left to primary hematologists at each institution. Although there was no exact percentage of patients who had PET-CT for diagnostic staging available in the database, the number of patients who had pre-treatment PET scan during the study period was small due to limited accessibility of PET-CT scan in Thailand. Histopathology or cytology to confirm extranodal organ involvement, except bone marrow, was not mandated but left to providers’ decision. Post-treatment surveillance (choice of imaging modalities, lumbar puncture) was depended upon primary hematologists’ discretion and each institution protocol. Patients were prospectively followed and patients’ status was systematically updated every 12 months by follow-up phone calls or the national census bureau website.
A total of 4371 newly diagnosed lymphoma patients was enrolled into the registry between September 2006 and December 2013. Of all lymphoma patients, 2399 were DLBCL. We analyzed 2034 DLBCL patients who received at least one cycle of CHOP-like protocol (cyclophosphamide, doxorubicin, vincristine, prednisolone) after excluding patients with CNS involvement at diagnosis and patients with primary CNS lymphoma. Relevant data were abstracted from TLSG web-based registry along with further abstraction from medical records. Of 137 patients who were lost to follow-up, the vital status and causes of death were obtained from the Thai national census bureau website.
Definition of terms
-
Progression-free survival: Duration from the diagnosis of DLBCL to the date of first relapse, progression, death, or last follow-up whichever came first.
-
Overall survival: Duration from the diagnosis of DLBCL to the date of death or last follow-up whichever came first.
-
Cumulative incidence of CNS relapse: The incidence of relapse when non-relapse mortality is a competing event.
Statistical analysis
Baseline characteristics were described using median for continuous variables and percentage for categorical variables. Comparison of continuous variables was done by Student’s t test to demonstrate difference between groups. Chi-square test was used to compare categorical variables between groups. CIR was calculated by the Fine and Gray’s method [18]. Death without relapse was considered as a competing event for relapse. Progression-free survival (PFS) and overall survival (OS) were estimated by the Kaplan-Meier method, and p values were calculated using a log-rank test. Univariate and multivariate analyses were performed using Cox proportional hazard regression model. CIR was estimated and displayed graphically by using the cmprsk package in R version 3.2.2. All other statistical analyses were done with the use of the Stata version 13.0 software (Stata Corp LP, College Station, TX). A significance level of p less than 0.05 was used for all analyses.
Results
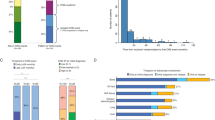
Of 2034 DLBCL who received at least one cycle of CHOP-like chemotherapy (with or without rituximab; Supplementary Table 1), 565 patients (27.8 %) relapsed or progressed after first-line treatment. Supplementary Tables 2 and 3 delineate first-line induction chemotherapy regimens and number of chemotherapy cycles of treated patients in our cohort, respectively. There was a total of 61 CNS relapse (3 %). Two-year cumulative incidence of SCNS relapse “(CIR) was 2.7 % (95 % confident interval (CI) 2.0–3.5 %) (Fig. 1). Median time from diagnosis to SCNS involvement was 8.4 months (interquartile range (IQR) 179–370 days). Table 1 shows baseline characteristics of patients. Compared to patients who did not relapse or relapsed without CNS involvement, patients with SCNS relapse had higher proportion of advanced stage diseases, poor PS, B symptoms, elevated LDH, paranasal sinuses involvement, and higher IPI. Using the CNS-IPI for SCNS relapse risk stratification, 729, 1024, and 281 patients were classified as low-, intermediate-, and high-risk groups. The 2-year CIR of low-, intermediate-, and high-risk CNS-IPI groups were 1.5, 3.1, and 4.6 %, respectively (p < 0.001) (Fig. 2a). Patients who received rituximab along with chemotherapy for induction therapy had comparable CIR of CNS relapse to patients in chemotherapy without rituximab cohort (Fig. 2b).

Cumulative incidence of secondary CNS relapse of all DLBCL patients in our cohort

The cumulative incidence of secondary CNS relapse stratified by the DSHNHL model (a) and rituximab exposure (b)
Of 61 CNS relapsed patients, 47 cases (77 %) were isolated CNS relapse, while 14 had both CNS and systemic relapse. Medical records were available for further review in 54 patients. Most common presentation included headache (n = 30, 55.6 %), focal neurological deficit (n = 17, 31.5 %), and cranial nerve palsy (n = 16, 29.6 %). The site of CNS relapse included 23 isolated brain parenchymal, 25 isolated leptomeningeal, and 7 concomitant parenchymal and leptomeningeal involvement. For 30 patients with brain parenchymal relapse, lesions were predominantly in periventricular and deep gray matter area (n = 13, 43.3 %) followed by lobar involvement (n = 11, 36.7 %). Of 14 patients who had both CNS and systemic relapse, 7, 4, and 3 patients developed systemic relapse at the time, before and after CNS relapse, respectively.
Pattern of risk-stratified CNS directed prophylaxis
Among 281 patients who were classified as high-risk group, 49 patients (17.4 %) received CNS directed prophylaxis (45 patients received IT chemotherapy and 4 patients received high-dose MTx or high-dose cytarabine containing regimens). A total of 67 (9.2 %) and 113 (11 %) patients in low and intermediate CNS-IPI groups received CNS-directed prophylactic treatments. The percentage of CNS prophylaxis was not different among CNS-IPI groups (p = NS).
Risk factors of CNS relapse
Univariate analysis demonstrated poor PS, elevated LDH level, advanced stage, presence of B symptoms, more than one extranodal organ involvement, certain extranodal sites (paranasal sinuses), high IPI, and high CNS-IPI group as predictive factors for SCNS relapse as summarized in Table 2. Multivariate analysis included that factors with p value < 0.10 from univariate analysis into the model with backward stepwise selection did not demonstrate significant risk factors of CNS relapse but patients who received CNS prophylaxis with IT MTx had higher risk of SCNS relapse (p < 0.001).
Treatment and outcome of patients with secondary CNS relapse
The median follow-up time for living patients was 51 months (interquartile range, 22–75 months). Two-year PFS, OS, and cumulative incidence of all relapse/progression of the entire cohort were 52.5, 62.4, and 26 %, respectively (Supplementary Fig. 1). Median OS of SCNS relapsed patients was significantly shorter than relapsed patients without CNS involvement (13.2 vs 22.6 months, p < 0.001) (Fig. 3). Of 61 patients with CNS relapse, median OS for patients with isolated CNS relapse and concomitant CNS/systemic relapse were 13.2 months (95 % CI 9.9–16.1 months) and 13.6 months (95 % CI 8.1–18.2 months), respectively (p = 0.89). Corresponding 2-year OS were 22.6 and 14.3 %, respectively.

Overall survival compared between patients with CNS relapse and patient without CNS relapse
Of 54 SCNS relapsed patients whose medical records were available for review, 42 patients received CNS-directed therapies (Supplementary Table 4). Of patients who received CNS-directed treatments, 20 received high-dose MTx-containing regimens, and 21 had IT chemotherapy and/or cranial irradiation. Eleven patients responded to the CNS-directed treatments (seven CR, four PR). Only one patient in our cohort had proceeded to autologous hematopoietic stem cell transplantation. Of 11 patients who responded to CNS-directed therapy, 4 patients subsequently relapsed. At the time of statistical analysis, 55 patients (90 %) died. Primary causes of death were progressive disease (n = 35, 63.6 %) and infection (n = 9, 16.7 %).
Discussion
SCNS relapse is one of the most serious events of DLBCL in immunochemotherapy era. The cumulative incidence of SCNS relapse in our study is 2.7 %, which is similar to previous cohorts. Several parameters were associated with higher risk of SCNS relapse such as elevated LDH, poor performance status, disseminated diseases, and certain extranodal organ involvement. Recently, the DSHNHL group proposed the clinical model, called CNS-IPI, to identify DLBCL at risk of SCNS relapse [10, 19]. The model was reproducibly used by a recent report by British Columbia Cancer Agency group [20]. We are able to stratify DLBCL patients into three groups by the risk of CNS relapse based on the CNS-IPI. The incidences of SCNS relapse in low and intermediate CNS-IPI were similar to those recently reported by German and British Columbia groups; however, the incidence of CNS relapse in our high CNS-IPI cohort was much lower compared to other reports [10, 19, 20]. One explanation could be attributed to the difference in the extent of staging procedures at the time of DLBCL diagnosis. CT scan was the primary radiographic investigation, and biopsies of extranodal organs were not mandated. Both factors could affect the distribution of lymphoma staging and CNS-IPI scoring at the time of diagnosis. The difference of CNS relapse incidence could also be a result of difference in CNS relapse diagnostic assessment and loss of follow-up. Since the investigations at relapse, i.e., lumbar puncture was depended upon primary hematologists’ discretion; the incidence of CNS relapse could be underestimated. About 7 % of patients were lost to follow-up. The vital status of these patients including causes of death was obtained from phone calls, and the national census bureau website which could confound the reported incidence of CNS relapse in our study. In addition, a significant proportion of high CNS-IPI patients might be refractory to treatment and could develop systemic relapse very early after treatment courses, especially patients who did not receive rituximab, which could result in early death of these patients prior SCNS relapse. All of abovementioned factors could partly explain the low SCNS relapse incidence of the high-risk CNS-IPI group in our cohort. Despite this contrast, our study demonstrated the applicability of this simple predictive model in the resource-limited setting. Besides clinical parameters, there have been several reports of newer markers, which related to higher risk of SCNS relapse. These markers included cell of origin (COO) [21], double hit/expressed DLBCL (MYC+ and BCL2+) [21], absolute monocyte counts at diagnosis [22], and high total lesion glycolysis at the threshold of 50 % (TLG50) [23]. Although these parameters could improve our ability to identify high-risk patients for SCNS relapse, some of which were difficult to universally obtain in resource-limited countries. In our cohort, 20 patients had pathology reports available for review, 6 (30 %) and 14 (70 %) had germinal center B cell (GCB) and non-GCB subtype, respectively (data not shown). Although it is difficult to make definite conclusion due to missing data, this finding looks concordant with the previous report [21]. Immunohistochemistry of MYC and BCL2 was not available for further analysis. The CNS-IPI will remain a simple yet predictive tool in low socioeconomic countries.
The effect of rituximab on SCNS relapse has been conflicting. Early studies suggested protective effect of rituximab on SCNS relapse [8, 11]; however, most of later studies did not demonstrate such finding. Comparing between patients who received rituximab and patients who did not, we did not see the difference in the SCNS relapse incidence between two groups.
The rationale of risk stratifying DLBCL patients for CNS relapse is to adopt CNS prophylactic strategies to the treatment plans to patients who have high-risk features. Our study demonstrated overall low number of patients who received CNS prophylaxis irrespective of their risk of SCNS relapse as stratified by CNS-IPI. This finding could reflect improper CNS prophylactic approach especially in high-risk patients.
When looking at the SCNS prophylactic strategies, the pattern of CNS-directed prophylaxis in our study was limited toward one approach with most patients received IT chemotherapy but very low number of systemic high-dose MTx. The underuse of high-dose MTx for SCNS prophylaxis in our study could partly be explained by limited availability of serum MTx level monitoring in our country. This finding highlights the impact of medical resource on practice patterns in developing countries.
Interestingly, DLBCL patients who received IT chemoprophylaxis in our study along with their induction treatment had significantly higher incidence of SCNS relapse. This finding was likely due to the selection bias of high-risk patients who were more likely to receive IT prophylaxis. On the other hand, it might indirectly inform the lack of benefit of IT chemotherapy as a prophylactic approach for SCNS relapse. Moreover, as the extent of staging work-up and investigations at relapse were left to primary physicians, these facts could affect the distribution of CNS-IPI at diagnosis and underestimate the diagnosis of CNS investigation at the time of relapse thus might explain the lack of benefit of intrathecal chemoprophylaxis. However, Spanish group recently demonstrated the promising outcome of IT liposomal cytarabine for the prevention of SCNS relapse in the cohort of 129 DLBCL patients [24]. The result of that study looked promising with no patients developed SCNS relapse during the median follow-up time of 40.1 months but requires further studies with larger patient samples to reproduce such finding. While most reports recently recommended CNS prophylactic regimen containing high-dose MTx over IT chemotherapy [25–27], we had too small number of patients who received high-dose MTx to draw the definite conclusion. Lastly, our studies confirm dismal outcomes of DLBCL patients who developed SCNS relapse despite improvement in frontline induction therapy in the immunochemotherapy era. Only one patient in our cohort underwent an autologous stem cell transplantation.
The retrospective design is the major limitation of our study. The unavailability of medical record for further review led to missing data in some patients. The diagnosis of CNS involvement at diagnosis and at relapse was not standardized and differed among institutions. This variation could lead to underestimation of the incidence and the diagnostic pattern of SCNS relapse. Small numbers of patients who received CNS prophylaxis limited the power to demonstrate the effect of CNS prophylactic strategies on SCNS relapse. Admitting that the proportion of patients who were treated with rituximab in our cohort was about one third of all patients, this fact might somewhat limit the applicability of the result to certain regions. However, our results reflect the real-world situation of resource-limited countries where drug accessibility has remained one of the major issues. Taking the advantage of limited access to rituximab in our country and by using the principal of comparative effectiveness research method, we could directly compare the effect of rituximab exposure on the SCNS relapse in DLBCL during simultaneous time period unlike other studies that mostly compared the effect of rituximab on CNS relapse incidence from two different periods (i.e., pre-rituximab vs post-rituximab era) of which the association might be confounded by other treatment related factors from two different eras. Our finding emphasized that the benefit of rituximab on CNS involvement is modest. In addition, although there were several reports about risk stratifying models/predictors for CNS relapse in DLBCL, our report is the largest one done in a resource-limited setting.
Future direction may point toward incorporating novel markers (such as cell of origin, MYC/BCL2 expression/rearrangement, PET CT finding) to clinical factors in order to build more sensitive models and to deliver risk-tailored CNS prophylaxis for DLBCL patients to prevent SCNS relapse.
In conclusion, the result of our study highlights the global view of SCNS relapse in DLBCL and its significance on the treatment of DLBCL in a developing country. It demonstrates the applicability of the CNS-IPI model as a simple tool to identify DLBCL at risk of SCNS relapse. The surprisingly low proportion of high-risk CNS relapse patients who received appropriate CNS prophylaxis in our cohort should urge the national organization to educate the hematologists and enforce the national guideline to deliver better care to DLBCL patients in these regions. Moreover, the findings of our study could lead to a collaborative effort to develop resource-stratified guidelines to improve treatment delivery for DLBCL patients. While accessibility to rituximab has remained a priori in developing countries to improve outcome of DLBCL, the attempt to better stratify patients at risk, appropriately provide prophylactic strategies and treatments of SCNS relapse is an unmet need, which warrants further studies.
References
Friedberg JW (2011) Relapsed/refractory diffuse large B-cell lymphoma. Hematology Am Soc Hematol Educ Program 2011:498–505
Boehme V, Zeynalova S, Kloess M et al (2007) Incidence and risk factors of central nervous system recurrence in aggressive lymphoma--a survey of 1693 patients treated in protocols of the German High-Grade Non-Hodgkin’s Lymphoma Study Group (DSHNHL). Ann Oncol 18:149–157
Deng L, Song Y, Zhu J et al (2013) Secondary central nervous system involvement in 599 patients with diffuse large B-cell lymphoma: are there any changes in the rituximab era? Int J Hematol 98:664–671
Tomita N, Yokoyama M, Yamamoto W et al (2012) Central nervous system event in patients with diffuse large B-cell lymphoma in the rituximab era. Cancer Sci 103:245–251
Villa D, Connors JM, Shenkier TN et al (2010) Incidence and risk factors for central nervous system relapse in patients with diffuse large B-cell lymphoma: the impact of the addition of rituximab to CHOP chemotherapy. Ann Oncol 21:1046–1052
Aviles A, Jesus Nambo M, Neri N (2013) Central nervous system prophylaxis in patients with aggressive diffuse large B cell lymphoma: an analysis of 3,258 patients in a single center. Med Oncol 30:520
Schmitz N, Zeynalova S, Glass B et al (2012) CNS disease in younger patients with aggressive B-cell lymphoma: an analysis of patients treated on the Mabthera International Trial and trials of the German High-Grade Non-Hodgkin Lymphoma Study Group. Ann Oncol 23:1267–1273
Boehme V, Schmitz N, Zeynalova S et al (2009) CNS events in elderly patients with aggressive lymphoma treated with modern chemotherapy (CHOP-14) with or without rituximab: an analysis of patients treated in the RICOVER-60 trial of the German High-Grade Non-Hodgkin Lymphoma Study Group (DSHNHL). Blood 113:3896–3902
Zhang J, Chen B, Xu X (2014) Impact of rituximab on incidence of and risk factors for central nervous system relapse in patients with diffuse large B-cell lymphoma: a systematic review and meta-analysis. Leuk Lymphoma 55:509–514
Schmitz N, Zeynalova S, Nickelsen M, Kansara R, Villa D, Sehn LH, Glass B, Scott DW, Gascoyne RD, Connors JM, Ziepert M, Pfreundschuh M, Loeffler M, Savage KJ (2016) CNS International prognostic index: a risk model for CNS relapse in patients with diffuse large B-Cell lymphoma treated with R-CHOP. J Clin Oncol 34(26):3150–6
Guirguis HR, Cheung MC, Mahrous M et al (2012) Impact of central nervous system (CNS) prophylaxis on the incidence and risk factors for CNS relapse in patients with diffuse large B-cell lymphoma treated in the rituximab era: a single centre experience and review of the literature. Br J Haematol 159:39–49
Kridel R, Dietrich PY (2011) Prevention of CNS relapse in diffuse large B-cell lymphoma. Lancet Oncol 12:1258–1266
Kumar A, Vanderplas A, LaCasce AS et al (2012) Lack of benefit of central nervous system prophylaxis for diffuse large B-cell lymphoma in the rituximab era: findings from a large national database. Cancer 118:2944–2951
Shimazu Y, Notohara K, Ueda Y (2009) Diffuse large B-cell lymphoma with central nervous system relapse: prognosis and risk factors according to retrospective analysis from a single-center experience. Int J Hematol 89:577–583
Tai WM, Chung J, Tang PL et al (2011) Central nervous system (CNS) relapse in diffuse large B cell lymphoma (DLBCL): pre- and post-rituximab. Ann Hematol 90:809–818
Yamamoto W, Tomita N, Watanabe R et al (2010) Central nervous system involvement in diffuse large B-cell lymphoma. Eur J Haematol 85:6–10
Intragumtornchai T, Bunworasate U, Siritanaratkul N et al (2013) Inferior progression-free survival for Thai patients with diffuse large B-cell lymphoma treated under Universal Coverage Scheme: the impact of rituximab inaccessibility. Leuk Lymphoma 54:83–89
Cheng SC, Fine JP, Wei LJ (1998) Prediction of cumulative incidence function under the proportional hazards model. Biometrics 54:219–228
Schmitz N, Zeynalova S, Nickelsen M et al (2013) A new prognostic model to assess the risk of CNS disease in patients with aggressive B-cell lymphoma. Hematol Oncol 31:96–150
Savage KJ, Zeynalova S, Kansara RR et al (2014) Validation of a prognostic model to assess the risk of CNS disease in patients with aggressive B-cell lymphoma. Blood 124:394–394
Savage KJ, Slack GW, Mottok A et al (2016) Impact of dual expression of MYC and BCL2 by immunohistochemistry on the risk of CNS relapse in DLBCL. Blood 127:2182–2188
Nitta H, Terui Y, Yokoyama M et al (2015) Absolute peripheral monocyte count at diagnosis predicts central nervous system relapse in diffuse large B-cell lymphoma. Haematologica 100:87–90
Song YS, Lee WW, Lee JS, Kim SE (2015) Prediction of central nervous system relapse of diffuse large B-cell lymphoma using pretherapeutic [18F]2-fluoro-2-deoxyglucose (FDG) positron emission tomography/computed tomography. Medicine (Baltimore) 94, e1978
Gonzalez-Barca E, Canales M, Salar A et al (2016) Central nervous system prophylaxis with intrathecal liposomal cytarabine in a subset of high-risk patients with diffuse large B-cell lymphoma receiving first line systemic therapy in a prospective trial. Ann Hematol 95:893–899
Cheah CY, Herbert KE, O’Rourke K et al (2014) A multicentre retrospective comparison of central nervous system prophylaxis strategies among patients with high-risk diffuse large B-cell lymphoma. Br J Cancer 111:1072–1079
Ferreri AJ, Bruno-Ventre M, Donadoni G et al (2014) Risk-tailored CNS prophylaxis in a mono-institutional series of 200 patients with diffuse large B-cell lymphoma treated in the rituximab era. Br J Haematol
Fletcher CD, Kahl BS (2014) Central nervous system involvement in diffuse large B-cell lymphoma: an analysis of risks and prevention strategies in the post-rituximab era. Leuk Lymphoma 55:2228–2240
Acknowledgment
The authors acknowledge the collective contribution of the medical, nursing, and administrative staff of each member center of Thai Lymphoma Study Group.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Ethical statements
The institutional review board committee at each participation site approved the study. All patients provided informed consent granting the investigator to abstract their medical information for research purposes.
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
ᅟ(DOCX 384 kb)
Rights and permissions
About this article

Cite this article
Wudhikarn, K., Bunworasate, U., Julamanee, J. et al. Secondary central nervous system relapse in diffuse large B cell lymphoma in a resource limited country: result from the Thailand nationwide multi-institutional registry. Ann Hematol 96, 57–64 (2017). https://doi.org/10.1007/s00277-016-2848-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-016-2848-y