
Abstract
Purpose
Total knee arthroplasty (TKA) is a common orthopedic surgery, yet postoperative dissatisfaction persists in around 20% of cases. Robotic total knee arthroplasty (rTKA) promises enhanced precision, but its impact on patient satisfaction compared to conventional TKA remains controversial (cTKA). This systematic review aims to evaluate patient satisfaction post-rTKA and compare outcomes with cTKA.
Methods
Papers from the following databases were identified and reviewed: PubMed, Scopus, Web of Science, and the Cochrane Online Library, using keywords like "Knee replacement," "Total knee arthroplasty," "Robotic," and "Patient satisfaction." Extracted data included patient satisfaction measures, Knee Society Score, Oxford Knee Score, Forgotten Joint Score, SF-36, HSS, and KOOS. Statistical analysis, including odds ratio and 95% CI was performed using R software. Heterogeneity was assessed using Cochrane's Q test.
Results
The systematic review included 17 articles, involving 1148 patients (571 in the rTKA group and 577 in the cTKA group) assessing patient satisfaction following rTKA. An analysis of proportions reveals rTKA satisfaction rate was 95%, while for cTKA, it was 91%. A meta-analysis comparing rTKA and cTKA found no statistically significant difference in patient satisfaction. Additionally, various patient-reported outcome measures (PROMs) were examined, showing mixed results across different studies and follow-up periods.
Conclusions
The results of this study found no difference in patient satisfaction outcomes in the short to mid-term for rTKA compared to conventional methods. This study does not assert superiority for the robotic approach, highlighting the need for careful consideration of various factors influencing outcomes in knee arthroplasty.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Osteoarthritis, including knee osteoarthritis, has become an increasing global challenge, with its burden growing notably in recent years [1,2,3]. Total knee arthroplasty (TKA) is one of the most frequently performed orthopaedic surgeries, with an estimated 1,065,000 patients undergoing the procedure in the United States in 2020. This number is anticipated to reach 3,416,000 by 2040 [4]. While TKA proves to be an effective and viable treatment, approximately 20% of patients express dissatisfaction post-surgery. This dissatisfaction is influenced by various factors, including patients’ expectations before the surgery, the extent of improvement in knee function, and the relief of pain following the procedure [5].
Recently, the introduction of robotic technologies has led to significant improvements in the accuracy and predictability of bone cuts performed during TKA with the intention of accurately restoring alignment, reducing the extent of soft tissue releases required and ultimately improving patient satisfaction and long term outcomes [6]. Currently, there are controversial findings regarding the differences between conventional total knee arthroplasty (cTKA) and rTKA in terms of functional outcomes and patient satisfaction [7, 8]. Some studies have reported a significantly higher proportion of satisfied or very satisfied patients in rTKA compared to conventional methods [9,10,11]. However, other studies have found no significant difference in patient satisfaction between rTKA and cTKA [12, 13]. Additionally, longer operative duration, higher intraoperative costs, and iatrogenic injuries associated with robotic surgeries could potentially have a negative impact on patient satisfaction [14].
The aim of the present study was to systematically review the existing literature on satisfaction rates following rTKA and compare patient satisfaction between rTKA and cTKA.
Methods
This study adhered to the PRISMA guidelines. The study protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the code [CRD42023479878].
Search strategy
A search was conducted across the following databases: PubMed, Scopus, Web of Science (WOS), and the Cochrane Online Library. The search utilized the keywords "Knee replacement," "Total knee arthroplasty," "Robotic," and "Patient satisfaction." Additionally, a manual search of the reference lists of identified articles was performed to uncover any additional relevant studies. The search spanned from the inception of each database to August 2nd, 2023. The complete search strategy was provided in supplementary file (Table S1).
Inclusion and exclusion criteria
Studies were included if they met the following criteria: (1) randomized controlled trials (RCTs), case–control studies, and prospective or retrospective cohorts investigating either unilateral or bilateral primary knee arthroplasty using robotic arm-assisted techniques; (2) provided information about patient satisfaction and preferences; (3) were published in English. The exclusion criteria comprised (1) case reports, letters, correspondents, pilot studies, reviews, editorials, and commentaries; (2) studies with incomplete data on patient satisfaction and (3) revision TKA.
Study selection and data extraction
Two independent reviewers screened the titles and abstracts of all retrieved articles. Full texts were obtained for potentially eligible studies. The two reviewers (SE, AHG), independently assessed the eligibility of each full-text article using the inclusion and exclusion criteria. Disagreements were resolved by consulting a third independent reviewer (AHH).
Data were extracted from the included studies by two reviewers (SE, AHG). The extracted data included: year of publication, study design, number of participants, mean age in years, Body Mass Index (BMI), robot brand, mean length of follow-up, patient satisfaction outcome measures, Knee Society Score (KSS), Oxford Knee Score (OKS), Forgotten Joint Score (FJS), Short Form (SF-36) Hospital for Special Surgery (HSS), and Knee Injury and Osteoarthritis Outcome Score (KOOS).
Quality assessment
Two individual reviewers [SE, AHG] assessed the risk of bias. The Joanna Briggs Institute Critical Appraisal Tool (JBI) [15] was employed for estimating the risk of bias in cohort and case series studies. This tool assesses studies with meticulous attention to key factors, including participant selection bias, accuracy of outcome measurement, appropriateness of statistical analysis and reported results selection, and potential bias arising from missing data.
Data synthesis and statistical analysis
Patient satisfaction disparities between rTKA and cTKA were assessed utilizing R software, version 4.2.2, provided by the R Foundation for Statistical Computing in Vienna, Austria (http://www.R-project.org). The analysis involved the Mantel–Haenszel model, presenting the odds ratio (OR) and its corresponding 95% confidence interval (CI). Additionally, proportion analysis was employed, utilizing the inverse variance method to calculate the overall patient satisfaction rate following rTKA. Heterogeneity was determined using Cochrane’s Q test, generating I2. If the P-value of the heterogeneity test was below 0.05 or I2 exceeded 50%, the random-effects model was applied; otherwise, the common-effects model was used. Egger's Regression test and Begg's funnel plot were utilized to evaluate potential publication bias.
Results
Study selection
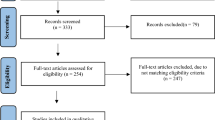
While searching across four databases, including PubMed, Scopus, Web of Science (WOS), and the Cochrane Online Library, a total of 203 articles were identified after eliminating duplicates. The initial assessment focused on titles and abstracts, resulting in 41 articles progressing to the next stage, which entailed a thorough full-text review. Subsequently, a comprehensive examination of the full texts resulted in the inclusion of 17 articles in this systematic review. Among these, nine articles involved a two-group comparison [9,10,11, 16,17,18,19,20,21], focusing on patient satisfaction between cTKA and rTKA, while the remaining eight single-group articles exclusively examined patient satisfaction following rTKA [22,23,24,25,26,27,28,29]. The Prisma chart in Fig. 1 visually illustrates the various stages of the screening process.

PRISMA graph
Quality of assessment
Seven studies utilized a prospective design [9, 11, 17, 18, 21, 24, 26], while the remainder employed a retrospective approach. The JBI critical appraisal tool for cohort and case series studies was employed to assess the quality of the studies. Detailed results of the qualitative assessment for the articles are available in the supplementary file (Tables S2 and S3).
Baseline characteristics
This review analyzed a total of nine comparative studies, involving 1148 patients (571 in the rTKA group and 577 in the cTKA group) [9,10,11, 16,17,18,19,20,21]. Furthermore, eight single-group studies comprised 1533 patients who underwent rTKA [22,23,24,25,26,27,28,29]. Among the eight comparative studies that reported gender distribution, 345 were male, and 743 were female [9,10,11, 16,17,18,19,20]. Across all the articles included, pertaining to patients who underwent rTKA, there were 786 males and 1311 females. The mean age in the comparative studies ranged from 65 to 70.1 years, and among rTKA patients in all included studies, mean age fell within the same range of 65 to 70 years. Mean BMI in the comparative studies ranged from 26.7 to 34.7, while among rTKA patients in all included studies, it ranged from 26.4 to 33.2. The minimum follow-up duration in the included studies was three months, and the maximum was extended to 24 months (Table 1).
Among the studies, the MAKO (Stryker) robotic system was the most frequently employed, and featured in seven studies [11, 18, 20, 23, 24, 27, 28]. Following this, the NAVIO (Smith & Nephew) system was used in three studies [16, 19, 22], the ROBODOC (Curexo) [17, 21] and OMNIBotics (Corin) [25, 26] systems were each utilized in two studies, and the ROSA (Zimmer Biomet) system was used in one study [9] (Table 1).
Overall patient satisfaction rate after rTKA
After performing a proportion analysis on patient satisfaction across 11 articles (comprising 6 single-group studies and five double-group comparative studies) following rTKA, the results indicated that 94% of patients expressed satisfaction with rTKA, with a confidence interval between 92 and 96% (I2 = 54%) (Fig. 2). Notably, Egger's test revealed the presence of publication bias in this analysis (p = 0.0145, Fig. 3). Following a Trim-and-fill analysis, incorporating three additional studies, the patient satisfaction rate was adjusted to 93.2% with a confidence interval spanning from 90.4% to 95.2%.

Forest plot displaying the proportion analysis of satisfaction rates among patients who underwent rTKA

Funnel plot of the proportion analysis of satisfaction rates for rTKA
In single-group research, Abhari et al., Daffara et al., and Richards et al. evaluated satisfaction levels using the Likert scale, obtaining mean scores of 4.6, 4.5, and 4.7 out of a possible five, respectively [23, 28, 29]. Additionally, Winnock de Grave et al. documented an average VAS satisfaction score of 8.9, and Turan et al. indicated a score of 8.3 ± 1.5 [16, 22] (Table 2).
Comparing patient satisfaction following rTKA and cTKA
An proportions analysis of comparative studies reveals that the satisfaction rate among patients who underwent rTKA was 95% ([95% CI: 88–98%]; Fig. 4A), while for cTKA patients, it was 91% ([95% CI: 85–95%]; Fig. 4B). A meta-analysis examining patient satisfaction rates after TKA indicates that there is no statistically significant difference between the two groups of rTKA and cTKA (OR [95% CI] = 2.62 [7.73–0.89], I2 = 0%) (Fig. 4C).

Forest plots illustrating proportion analysis of satisfaction rates among patients who underwent rTKA (A) and cTKA (B), along with meta-analysis comparing patient satisfaction rates between rTKA and cTKA (C)
Choi et al. observed no significant disparity in KSS satisfaction and expectation scores among patients who underwent rTKA and cTKA at the three-month postoperative stage. However, at the one-year and two-year follow-up points, the mean scores were higher in the rTKA group [20]. Khlopas et al. reported no difference in the three-month mean of KSS satisfaction and expectation scores between the two groups [18]. Also, Smith et al.'s study noted that the difference in KSS satisfaction score was statistically nonsignificant [11]. Moreover, Turan et al. reported the mean satisfaction score on the Visual Analog Scale (VAS), revealing no significant difference between the two groups [16] (Table 3).
Mulpur et al. divided satisfaction levels into four categories: very satisfied, satisfied, dissatisfied, and very dissatisfied. Their findings showed a notably higher proportion of satisfied patients following rTKA compared to those who underwent cTKA [10]. Likewise, Smith et al., who categorized satisfaction into three levels, observed a significantly greater ratio of very satisfied and satisfied individuals among patients who received rTKA [11] (Table 3).
Another metric for assessing patient satisfaction involves their willingness to undergo surgery again, a topic investigated in studies conducted by Eerens et al. and Kenanidis et al. In Eerens et al.'s study, a larger percentage of patients in the cTKA group expressed a willingness for repeat surgery, suggesting higher satisfaction [19]. In contrast, in Kenanidis et al.'s publication, this percentage was notably elevated in the rTKA group [9] (Table 3).
Liow et al. found that there was no statistically significant difference in the ratio of patients with fulfilled expectations for TKA, both six months and two years after the operation [21] (Table 3).
Song et al. conducted a study involving patients who underwent simultaneous bilateral TKA using both robotic and manual techniques. Before the operation, most patients expressed a preference for cTKA. However, at the three-month follow-up 33.3% favored cTKA, 33.3% preferred rTKA, and 33.3% found both methods equally preferable. In the final follow-up, 20% preferred cTKA, 40% favored rTKA, and 40% found both methods equally appealing [17] (Table 3).
Patient-Reported Outcome Measures (PROMs)
We also examined PROMs as a secondary outcome. Both Song et al. and Choi et al. found no significant disparity in mean WOMAC scores among patients who underwent rTKA and cTKA at three months and one year postoperative stages [17, 20]. However, in Choi et al.'s study, a notable difference emerged at the two-year postoperative follow-up, with the mean score being lower in the rTKA group [20] (Table 4).
In Choi et al.'s study, the initial mean KSS knee score varied between the two groups, but this distinction lost significance by the final follow-up [20]. Also, Liow et al. noted no significant difference. In contrast, Smith et al. found a notably higher mean score in the rTKA group [21]. The average KSS function score in Choi et al.'s study consistently showed significant superiority in the rTKA group across all follow-up periods, a pattern that is similarly evident in Smith et al.'s research [11, 20]. In contrast to these two investigations, the studies conducted by Liow and Khlopas did not reveal any notable differences in this regard [18, 21] (Table 4).
Four studies reported the OKS [9, 10, 16, 21], and among them, only Kenanidis et al.'s study showed a significant difference (in favor of rTKA) [9]. The FJS was also documented in four studies [10, 16, 19, 20], and except for Turan et al.'s study [22], all others indicated a significant advantage for rTKA.
In Kenanidis et al.'s study, the mean SF-36 Physical Component Summary (PCS) was notably higher in the rTKA group [9]. Conversely, Liow et al.'s study did not indicate any significant differences in either PCS or Mental Component Summary (MCS) [21] (Table 4).
At three months and one year postoperatively, Song et al. found no significant difference in the mean HSS scores between the two groups [17]. Likewise, in Turan et al.'s study, none of the components of the KOOS exhibited significant differences between the two groups [16] (Table 4).
Discussion
Patient satisfaction is an important component of decision-making in orthopaedic surgery [30, 31]. While significant focus has been placed on comparing the radiological and clinical outcomes of rTKA with cTKA, patient satisfaction and patient-reported outcomes stand as critical metrics in surgical decision-making [32, 33]. Results of this study suggest that rTKA is a reliable method with high levels of patient satisfaction. Additionally, the level of satisfaction in cTKA was high and close to that in rTKA. The results of this study suggest that rTKA and cTKA achieve comparable results in these domains.
rTKA is a reliable and safe method in total knee replacement that has achieved satisfactory results in radiological and clinical outcomes [34,35,36,37]. Literature shows that utilizing robotic assistance in TKA can achieve more precise radiological outcomes. rTKA comes with significantly fewer outliers in component positioning in the femoral coronal and tibial sagittal axes and mechanical alignment [34]. Such outcome measures reflect the success of the operation in achieving the desired component position and alignment. Although proper alignment and soft tissue balancing are crucial for maintaining knee function, the extent to which observed differences in these measures affect the final clinical outcomes and patient satisfaction is debatable [38, 39].
Several studies indicate that functional outcomes and implant survivorship can be affected by improved accuracy in alignment and implant positioning. However, a long-term follow-up, seems to be needed in order to notice differences in these outcomes [38]. Most current evidence comparing rTKA and cTKA for patient satisfaction consisted of a short follow-up length, with a maximum duration of two years in our included studies. Additionally, newer robotic systems, claiming improved technical properties, have not been in use long enough to provide medium or long term results.
Most studies which examine the results of rTKA and cTKA show similar results, with rTKA showing slightly better functional and range of motion goals than cTKA [34, 35, 37]. The majority of the studies comparing the two techniques argue that improved radiological outcomes following rTKA, may not be clinically meaningful in the short- to mid-term follow-up [34, 35, 37]. Also, no remarkable difference seems to exist regarding the rate of complications associated with both techniques [34]. Aside from slight differences in blood loss, post-surgery drainage, operative time, and periprosthetic joint infection [8, 21, 36, 40], evidence comparing complication rates between these methods does not robustly favor one over the other.
The previous systematic review and meta-analysis performed by Zhang et al. showed better PROMs for rTKA based on KSS and WOMAC scores, while still arguing that no minimal clinically important difference (MCID) was notable [8]. Since there is a great heterogeneity in the tools used to evaluate PROMs in the included studies, a meta-analysis was not feasible in our study. On the other hand, while some studies reported significantly better outcomes for rTKA [9,10,11, 19, 20], others suggested comparable results [16,17,18, 21]. Also, no significant difference in PROMs between the two techniques were observed in the current study.
An essential consideration when comparing rTKA with cTKA could be the diversity and lack of consistent reporting in alignment and balancing techniques across various studies. Other factors such as surgeon experience, pre operative discussions with the patients and biases based on funding sources for studies need to be considered as these all potentially influence results.
The idea of implementing a uniform alignment approach in all cases of TKA has been challenged recently [41, 42]. While mechanical alignment is the most utilized surgical alignment goal for TKA, a more personalized goal accounting for the constitutional alignment of each patient may be the key to addressing patient dissatisfaction [43]. Since rTKA has been successful in fulfilling the objectives of mechanical alignment with high precision, improving patient satisfaction may involve understanding the significance of presurgical knee morphology. The true potential of technological advancements such as robotic and computer assistance [44] may emerge by defining more personalized surgical goals rather than solely attempting to optimize the precision of the currently defined single target alignment.
In contrast to TKA, robotic-assisted uni-compartment arthroplasty (rUKA) was associated with better patient satisfaction in our previous review [45]. Several factors may contribute to this difference. Firstly, the importance of highly optimizing alignment and soft tissue balance may differ between procedures. A successful outcome in UKA largely depends on both precision of implant alignment and soft tissue balance [46, 47], while TKA seems to tolerate variability in component alignment to some extent [38, 48, 49]. Importantly, studies comparing rUKA and conventional manual uni-compartment arthroplasty (mUKA) mostly consisted of longer follow-up durations [45], which could unravel the clinical effect of radiological precision achieved by robotic assistance. However, such a hypothesis could be easily challenged with findings regarding the long-term studies on PROMs following robotic-assisted total hip arthroplasty (THA), which still indicate comparable results with the conventional method [50]. The potential effect of variety in the recruited robotic systems in these operations should also be kept in mind.
Our study was subject to some limitations. This review only encompassed the short- to mid-term patient satisfaction outcomes. Therefore, studies with longer durations may help reveal any notable differences among these techniques. Second, many key aspects of the procedures other than the use of robotic assistance (e.g., alignment and balancing methods, surgeon experience both in terms of years of practice and volume of procedures) were not considered in most studies, limiting the interpretability of such comparisons. Achieving optimal outcomes in rTKA may necessitate relatively different alignment approaches than those available in conventional methods. Additionally, due to the high degree of heterogeneity of included studies in the tools used for assessing PROMs, a meta-analysis was not feasible to draw robust conclusions. Finally, the extent to which utilizing different robotic systems could impact the outcome could not be determined. Although the majority of the studies reporting better outcomes for rTKA had utilized either MAKO or NAVIO robotic systems, other studies reporting similar results to cTKA with the same systems were also present.
In conclusion, rTKA achieves reliable and acceptable patient satisfaction in short- to mid-term follow-up, comparable to the outcomes of conventional TKA. rTKA has been associated with improved precision of bone cuts and radiological outcomes. Patient satisfaction is a complex construct, and uniform measurements among studies are crucial for sound judgement [51, 52].
Data availability
A sheet of extracted data from the included articles is available upon request; please contact the corresponding author for access.
Code availability
All statistical analyses were performed using R software, version 4.2.2, provided by the R Foundation for Statistical Computing in Vienna, Austria (http://www.R-project.org).
References
Hoveidaei AH, Nakhostin-Ansari A, Chalian M, Roshanshad A, Khonji MS, Mashhadiagha A, Pooyan A, Citak M (2023) Burden of knee osteoarthritis in the Middle East and North Africa (MENA): an epidemiological analysis from 1990 to 2019. Arch Orthop Trauma Surg 143(10):6323–6333. https://doi.org/10.1007/s00402-023-04852-8
Hoveidaei AH, Nakhostin-Ansari A, Hosseini-Asl SH, Khonji MS, Razavi SE, Darijani SR, Citak M (2023) Increasing burden of hip osteoarthritis in the Middle East and North Africa (MENA): an epidemiological analysis from 1990 to 2019. Arch Orthop Trauma Surg 143(6):3563–3573. https://doi.org/10.1007/s00402-022-04582-3
Hoveidaei AH, Nakhostin-Ansari A, Chalian M, Razavi SE, Khonji MS, Hosseini-Asl SH, Darijani SR, Pooyan A, LaPorte DM (2023) Burden of hand osteoarthritis in the Middle East and North Africa (MENA): an epidemiological analysis from 1990 to 2019. J Hand Surg Am 48(3):245–256. https://doi.org/10.1016/j.jhsa.2022.11.016
Singh JA, Yu S, Chen L, Cleveland JD (2019) Rates of total joint replacement in the United States: future projections to 2020–2040 using the national inpatient sample. J Rheumatol 46:1134–1140. https://doi.org/10.3899/jrheum.170990
Gunaratne R, Pratt DN, Banda J, Fick DP, Khan RJK, Robertson BW (2017) Patient dissatisfaction following total knee arthroplasty: a systematic review of the literature. J Arthroplasty 32:3854–3860. https://doi.org/10.1016/j.arth.2017.07.021
Shatrov J, Parker D (2020) Computer and robotic - assisted total knee arthroplasty: a review of outcomes. J Exp Orthop 7:70. https://doi.org/10.1186/s40634-020-00278-y
Parel PM, Manyak GA, Carvajal JA, Abraham T, Al Rashid M (2022) An early-stage comparison of functional outcomes following robotic-assisted versus conventional total knee arthroplasty: a systematic review and meta-analysis. J Arthrosc Joint Surg 9:77–85. https://doi.org/10.4103/jajs.jajs_75_22
Zhang J, Ndou WS, Ng N, Gaston P, Simpson PM, Macpherson GJ, Patton JT, Clement ND (2022) Robotic-arm assisted total knee arthroplasty is associated with improved accuracy and patient reported outcomes: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc 30:2677–2695. https://doi.org/10.1007/s00167-021-06464-4
Kenanidis E, Paparoidamis G, Milonakis N, Potoupnis M, Tsiridis E (2023) Comparative outcomes between a new robotically assisted and a manual technique for total knee arthroplasty in patients with osteoarthritis: a prospective matched comparative cohort study. Eur J Orthop Surg Traumatol 33:1231–1236. https://doi.org/10.1007/s00590-022-03274-3
Mulpur P, Masilamani ABS, Prakash M, Annapareddy A, Hippalgaonkar K, Reddy AVG (2022) Comparison of patient reported outcomes after robotic versus manual total knee arthroplasty in the same patient undergoing staged bilateral knee arthroplasty. J Orthop 34:111–115. https://doi.org/10.1016/j.jor.2022.08.014
Smith AF, Eccles CJ, Bhimani SJ, Denehy KM, Bhimani RB, Smith LS, Malkani AL (2021) Improved patient satisfaction following robotic-assisted total knee arthroplasty. J Knee Surg 34:730–738. https://doi.org/10.1055/s-0039-1700837
Albelooshi A, Hamie M, Bollars P, Althani S, Salameh R, Almasri M, Schotanus MGM, Meshram P (2023) Image-free handheld robotic-assisted technology improved the accuracy of implant positioning compared to conventional instrumentation in patients undergoing simultaneous bilateral total knee arthroplasty, without additional benefits in improvement of clinical outcomes. Knee Surg Sports Traumatol Arthrosc 31:4833–4841. https://doi.org/10.1007/s00167-023-07523-8
Clement ND, Galloway S, Baron YJ, Smith K, Weir DJ, Deehan DJ (2023) Robotic Arm-assisted versus Manual (ROAM) total knee arthroplasty: a randomized controlled trial. Bone Joint J 105-b:961–970. https://doi.org/10.1302/0301-620x.105b9.Bjj-2023-0006.R3
Nogalo C, Meena A, Abermann E, Fink C (2023) Complications and downsides of the robotic total knee arthroplasty: a systematic review. Knee Surg Sports Traumatol Arthrosc 31:736–750. https://doi.org/10.1007/s00167-022-07031-1
Munn Z, Barker TH, Moola S, Tufanaru C, Stern C, McArthur A, Stephenson M, Aromataris E (2020) Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI Evid Synth 18:2127–2133. https://doi.org/10.11124/jbisrir-d-19-00099
Turan K, Camurcu Y, Kezer M, Uysal Y, Kizilay YO, Ucpunar H, Temiz A (2023) A comparison of robotic-assisted and manual techniques in restricted kinematically aligned total knee arthroplasty: coronal alignment improvement with no significant clinical differences. Knee Surg Sports Traumatol Arthrosc 31:4673–4679. https://doi.org/10.1007/s00167-023-07426-8
Song EK, Seon JK, Park SJ, Jung WB, Park HW, Lee GW (2011) Simultaneous bilateral total knee arthroplasty with robotic and conventional techniques: a prospective, randomized study. Knee Surg Sports Traumatol Arthrosc 19:1069–1076. https://doi.org/10.1007/s00167-011-1400-9
Khlopas A, Sodhi N, Hozack WJ, Chen AF, Mahoney OM, Kinsey T, Orozco F, Mont MA (2020) Patient-reported functional and satisfaction outcomes after robotic-arm-assisted total knee arthroplasty: early results of a prospective multicenter investigation. J Knee Surg 33:685–690. https://doi.org/10.1055/s-0039-1684014
Eerens W, Bollars P, Henckes ME, Schotanus M, Mievis J, Janssen D (2022) Improved joint awareness two years after total knee arthroplasty with a handheld image-free robotic system. Acta Orthop Belg 88:47–52. https://doi.org/10.52628/88.1.07
Choi BS, Kim SE, Yang M, Ro DH, Han HS (2023) Functional alignment with robotic-arm assisted total knee arthroplasty demonstrated better patient-reported outcomes than mechanical alignment with manual total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 31:1072–1080. https://doi.org/10.1007/s00167-022-07227-5
Liow MHL, Goh GS, Wong MK, Chin PL, Tay DK, Yeo SJ (2017) Robotic-assisted total knee arthroplasty may lead to improvement in quality-of-life measures: a 2-year follow-up of a prospective randomized trial. Knee Surg Sports Traumatol Arthrosc 25:2942–2951. https://doi.org/10.1007/s00167-016-4076-3
Turan K, Camurcu Y, Kezer M, Uysal Y, Kizilay YO, Temiz A (2023) Preliminary outcomes of kinematically aligned robot-assisted total knee arthroplasty with patient-specific cartilage thickness measurement. J Robot Surg 17:979–985. https://doi.org/10.1007/s11701-022-01503-9
Richards JA, Williams MD, Gupta NA, Kitchen JM, Whitaker JE, Smith LS, Malkani AL (2022) No difference in PROMs between robotic-assisted CR versus PS total knee arthroplasty: a preliminary study. J Robot Surg 16:1209–1217. https://doi.org/10.1007/s11701-021-01352-y
Probst T, Akalin ER, Giannouchos A, Schnurr C (2022) Learning curves of robotic technology in an orthopedic teaching hospital. Orthopadie (Heidelb) 51:739–747. https://doi.org/10.1007/s00132-022-04287-w
Lee GC, Wakelin E, Randall A, Plaskos C (2021) Can a robot help a surgeon to predict a good total knee arthroplasty? Bone Joint J 103-b:67-73. https://doi.org/10.1302/0301-620x.103b6.Bjj-2020-2305.R1
Keggi JM, Wakelin EA, Koenig JA, Lawrence JM, Randall AL, Ponder CE, DeClaire JH, Shalhoub S, Lyman S, Plaskos C (2021) Impact of intra-operative predictive ligament balance on post-operative balance and patient outcome in TKA: a prospective multicenter study. Arch Orthop Trauma Surg 141:2165–2174. https://doi.org/10.1007/s00402-021-04043-3
Winnock de Grave P, Luyckx T, Claeys K, Tampere T, Kellens J, Müller J, Gunst P (2022) Higher satisfaction after total knee arthroplasty using restricted inverse kinematic alignment compared to adjusted mechanical alignment. Knee Surg Sports Traumatol Arthrosc 30:488–499. https://doi.org/10.1007/s00167-020-06165-4
Daffara V, Zambianchi F, Bazzan G, Matveitchouk N, Berni A, Piacentini L, CuoghiCostantini R, Catani F (2023) No difference in clinical outcomes between functionally aligned cruciate-retaining and posterior-stabilized robotic-assisted total knee arthroplasty. Int Orthop 47:711–717. https://doi.org/10.1007/s00264-023-05693-1
Abhari S, Rhea EB, Arrington DD, Smith LS, Yakkanti MR, Malkani AL (2023) Is there a difference in proms between morbidly obese patients and nonobese patients following primary total knee arthroplasty? Arthroplast Today 22:101169. https://doi.org/10.1016/j.artd.2023.101169
Hoveidaei AH, Roshanshad A, Vosoughi AR (2021) Clinical and radiological outcomes after arthrodesis of the first metatarsophalangeal joint. Int Orthop 45:711–719
Swarup I, Henn CM, Gulotta LV, Henn RF III (2019) Patient expectations and satisfaction in orthopaedic surgery: a review of the literature. J Clin Orthop trauma 10:755–760
Smith MJ, Choma TJ (2017) Patient satisfaction in musculoskeletal medicine. Curr Rev Musculoskelet Med 10:207–211. https://doi.org/10.1007/s12178-017-9403-x
Graham B, Green A, James M, Katz J, Swiontkowski M (2015) Measuring patient satisfaction in orthopaedic surgery. JBJS 97:80–84. https://doi.org/10.2106/jbjs.N.00811
Onggo JR, Onggo JD, De Steiger R, Hau R (2020) Robotic-assisted total knee arthroplasty is comparable to conventional total knee arthroplasty: a meta-analysis and systematic review. Arch Orthop Trauma Surg 140:1533–1549. https://doi.org/10.1007/s00402-020-03512-5
Ruangsomboon P, Ruangsomboon O, Pornrattanamaneewong C, Narkbunnam R, Chareancholvanich K (2023) Clinical and radiological outcomes of robotic-assisted versus conventional total knee arthroplasty: a systematic review and meta-analysis of randomized controlled trials. Acta Orthop 94:60–79. https://doi.org/10.2340/17453674.2023.9411
Mancino F, Cacciola G, Malahias MA, De Filippis R, De Marco D, Di Matteo V, A G, Sculco PK, Maccauro G, De Martino I (2020) What are the benefits of robotic-assisted total knee arthroplasty over conventional manual total knee arthroplasty? A systematic review of comparative studies. Orthop Rev (Pavia) 12:8657.https://doi.org/10.4081/or.2020.8657
Agarwal N, To K, McDonnell S, Khan W (2020) Clinical and radiological outcomes in robotic-assisted total knee arthroplasty: a systematic review and meta-analysis. J Arthroplasty 35:3393-3409.e3392. https://doi.org/10.1016/j.arth.2020.03.005
Ritter MA, Davis KE, Meding JB, Pierson JL, Berend ME, Malinzak RA (2011) The effect of alignment and BMI on failure of total knee replacement. J Bone Joint Surg Am 93:1588–1596. https://doi.org/10.2106/jbjs.J.00772
Choong PF, Dowsey MM, Stoney JD (2009) Does accurate anatomical alignment result in better function and quality of life? Comparing conventional and computer-assisted total knee arthroplasty. J Arthroplasty 24:560–569. https://doi.org/10.1016/j.arth.2008.02.018
Cho KJ, Seon JK, Jang WY, Park CG, Song EK (2019) Robotic versus conventional primary total knee arthroplasty: clinical and radiological long-term results with a minimum follow-up of ten years. Int Orthop 43:1345–1354. https://doi.org/10.1007/s00264-018-4231-1
Rivière C, Lazic S, Boughton O, Wiart Y, Vïllet L, Cobb J (2018) Current concepts for aligning knee implants: patient-specific or systematic? EFORT Open Rev 3:1–6. https://doi.org/10.1302/2058-5241.3.170021
Donaldson J, Joyner J, Tudor F (2015) Current controversies of alignment in total knee replacements. Open Orthop J 9:489–494. https://doi.org/10.2174/1874325001509010489
Hirschmann MT, Moser LB, Amsler F, Behrend H, Leclerq V, Hess S (2019) Functional knee phenotypes: a novel classification for phenotyping the coronal lower limb alignment based on the native alignment in young non-osteoarthritic patients. Knee Surg Sports Traumatol Arthrosc 27:1394–1402. https://doi.org/10.1007/s00167-019-05509-z
Shatrov J, Parker D (2020) Computer and robotic – assisted total knee arthroplasty: a review of outcomes. J Exp Orthop 7:70. https://doi.org/10.1186/s40634-020-00278-y
Hoveidaei AH, Esmaeili S, Ghaseminejad-Raeini A, Pirahesh SK, Hoveidaei A, Sandiford NA, Lahner N, Citak M (2023) Patient satisfaction following robotic unicompartmental knee arthroplasty: A systematic review and meta-analysis. Technol Health Care Preprint 1–10. https://doi.org/10.3233/THC-231216
Khow YZ, Liow MHL, Lee M, Chen JY, Lo NN, Yeo SJ (2021) Coronal alignment of fixed-bearing unicompartmental knee arthroplasty femoral component may affect long-term clinical outcomes. J Arthroplasty 36:478–487. https://doi.org/10.1016/j.arth.2020.07.070
Khow YZ, Liow MHL, Lee M, Chen JY, Lo NN, Yeo SJ (2021) The effect of tibial and femoral component coronal alignment on clinical outcomes and survivorship in unicompartmental knee arthroplasty. Bone Joint J 103-B:338–346. https://doi.org/10.1302/0301-620x.103b2.Bjj-2020-0959.R1
Parratte S, Pagnano MW, Trousdale RT, Berry DJ (2010) Effect of postoperative mechanical axis alignment on the fifteen-year survival of modern, cemented total knee replacements. J Bone Joint Surg Am 92(12):2143–9. https://doi.org/10.2106/JBJS.I.01398
Howell SM, Howell SJ, Kuznik KT, Cohen J, Hull ML (2013) Does A kinematically aligned total knee arthroplasty restore function without failure regardless of alignment category? Clin Orthop Relat Res® 471
Bargar WL, Parise CA, Hankins A, Marlen NA, Campanelli V, Netravali NA (2018) Fourteen year follow-up of randomized clinical trials of active robotic-assisted total hip arthroplasty. J Arthroplasty 33:810–814. https://doi.org/10.1016/j.arth.2017.09.066
Halawi MJ, Jongbloed W, Baron S, Savoy L, Williams VJ, Cote MP (2019) Patient dissatisfaction after primary total joint arthroplasty: the patient perspective. J Arthroplasty 34:1093–1096. https://doi.org/10.1016/j.arth.2019.01.075
Kahlenberg CA, Nwachukwu BU, McLawhorn AS, Cross MB, Cornell CN, Padgett DE (2018) Patient satisfaction after total knee replacement: a systematic review. HSS J® 14:192–201. https://doi.org/10.1007/s11420-018-9614-8
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
A.H.H..: Study design, search string development, data analysis, writing manuscript; S.E.: Paper screening, data extraction; A.G.R.: Paper screening, Data extraction; K.P.: writing manuscript; M.S.F.: writing manuscript; N.A.S.: manuscript review; M.C.: Study design, final supervision, manuscript review; All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Consent for publication
Not applicable.
Informed consent
Not applicable.
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Hoveidaei, A.H., Esmaeili, S., Ghaseminejad-Raeini, A. et al. Robotic assisted Total Knee Arthroplasty (TKA) is not associated with increased patient satisfaction: a systematic review and meta-analysis. International Orthopaedics (SICOT) 48, 1771–1784 (2024). https://doi.org/10.1007/s00264-024-06206-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-024-06206-4