
Abstract
Data on the risk of lymphatic and hematopoietic neoplasms among workers whose jobs entail high exposure to polycyclic aromatic hydrocarbons (PAH) are sparse, and mainly based on small-size studies. We carried out a systematic review of occupational cohort studies that reported results on incidence or mortality from Hodgkin lymphoma (HL), non-Hodgkin lymphoma (NHL), leukemia or multiple myeloma (MM) among workers exposed to PAH. We computed meta-analytic estimates using a random effect model. Meta-relative risk (meta-RR) was computed separately by each type of neoplasm, job or industry. We identified 41 studies (12 in iron and steel foundries, 11 in aluminum plant, 6 in cokeries, 6 in carbon electrode manufacturing, 2 on asphalt workers, 2 on creosote-exposed workers, 1 on tar distillery workers and 1 evaluating both tar distillery workers and roofers). No significant excess risk of any lymphatic and hematopoietic neoplasms was found among workers employed in jobs or industries entailing high PAH exposure. Among 18 meta-analytic estimates by job or industry and type of neoplasm, 16 were close to unit, i.e., between 0.72 and 1.27, whereas the meta-RR was 1.38 [95 % confidence interval (CI) 0.95–2.01] for HL in foundry workers and 2.01 (95 % CI 0.96–4.22) for NHL in workers exposed to creosote. There was no association between occupation entailing high PAH exposure and risk of MM or leukemia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Polycyclic aromatic hydrocarbons (PAH) are a group of widespread environmental contaminants with genotoxic, mutagenic, teratogenic and carcinogenic effects (IARC 2010). PAH exert their effects binding to a specific aromatic hydrocarbon receptor and through the formation of reactive metabolites that cause genotoxicity and oxidative stress. These pathways are linked to altered Ca2+ homeostasis in T and B cells, leading to disruption of antigen and mitogen signaling as well as initiation of pro-apoptotic events (Burchiel and Luster 2001). In addition, several PAH have immunotoxic activity and may interfere with lymphocytic subpopulations and contribute to promoting lympho-hematopoietic carcinogenesis (Burchiel and Luster 2001).
Occupational exposure to PAH occurs primarily through inhalation, though uptake of PAH through the skin is substantial (Jongeneelen 2001), and high levels were found in biological samples of workers whose jobs entail pyrolysis of coal or use of coal-derived products (Carta et al. 2004; IARC 2010). These workers have an excess risk of respiratory tract, urinary system and skin cancers (Boffetta et al. 1997; Rota et al. 2014; Wagner et al. 2015), but there is only limited evidence of excess risk of lymphatic and hematopoietic neoplasms (Gibbs and Labrèche 2014).
We therefore conducted a systematic review and meta-analysis of the available cohort studies aimed to quantify the relationship between occupational PAH exposure and risk of lymphatic and hematopoietic neoplasms.
Methods
Study identification and data collection
We conducted a meta-analysis in compliance with the guidelines for Meta-analyses and Systematic Reviews of Observational Study (MOOSE) (Stroup et al. 2011). Two authors (PB and GA) carried out a comprehensive literature search in PubMed and EMBASE for articles on cohorts of workers employed in occupational activities related to high PAH exposure, i.e., aluminum production, foundries, coke workers, asphalt-exposed workers, tar distilleries, carbon electrode manufacturing and workers exposed to creosote. We identified relevant articles by searching the following keywords in the title or abstract: cancer, tumor, neoplasm, incidence, mortality, risk, occupation, work, polycyclic aromatic hydrocarbons, PAH, foundry, coke, asphalt, roofing, paving, carbon electrode, creosote, coal, tar and bitumen. The search was conducted on February 24, 2016, without restriction for publication time and languages. Details on the search strategy are reported in the Online resource 1. We identified additional studies manually by searching the references of the articles retrieved by electronic search.
Original articles published in English, Italian or French aiming to evaluate the incidence or mortality risk from Hodgkin lymphoma (HL), non-Hodgkin lymphoma (NHL), multiple myeloma (MM) or leukemia in workers employed in occupational activities related to high PAH exposure were eligible for inclusion in the meta-analysis. When more than one article reported results from the same cohort, we used the most recent and informative one. The quantitative synthesis was performed only if at least two studies were available for a given exposure-outcome association.
We used the International Classification of Diseases (ICD), Revisions 7th, 8th, 9th and 10th to identify cases to be included in the meta-analysis, i.e., all diagnosis or deaths classified as HL (ICD7–9 codes: 201 or ICD10 code: C81), NHL (ICD7–9 codes: 200, 202 or ICD10 codes: C82–C86, C96), MM (ICD7–9 codes: 203 or ICD10 code: C90), or leukemia (ICD7–9 codes: 204–207 or ICD10 codes: C91–C95).
From the selected studies, we extracted information on the population size, country, occupational activity, period of employment, follow-up duration, reference population, outcome measure (incidence or mortality), number of observed cases or deaths, effect estimates (Standardized Incidence Ratio, SIR, Standardized Mortality Ratio, SMR, Relative risk, RR) and the corresponding 95 % confidence intervals (CIs).
Statistical analysis
The analysis was stratified by job and industry, and whenever possible, by type of lymphatic and hematopoietic neoplasm.
Most studies were based on mortality data. However, some studies reported only results on cancer incidence, and we combined incidence and mortality data in the meta-analysis, under the assumption that PAH exposure does not affect survival from this group of neoplasms.
If original articles did not report risk estimates or confidence intervals, we computed them using raw data.
We considered SMRs, SIRs or RRs as comparable estimates of the relative risk (RR).
As some degree of between-study heterogeneity was anticipated, we computed the meta-RR and the corresponding 95 % CIs through a random effect model. Briefly, each study-specific log(SMR), log(SIR) or log(RR) was weighted by the inverse of its variance plus the between studies variance component τ 2 estimated through the moment estimator (DerSimonian and Laird 1986).
Between-study heterogeneity was assessed by Q statistics based on a Chi-squared test, and inconsistency was measured through the I 2 statistic, representing the proportion of total variation due to between-study variance (Higgins et al. 2003).
When significant between studies heterogeneity (P ≤ 0.20) occurred, we made a sensitivity analyses excluding one study at a time in order to assess the influence of single studies on the final meta-analytic estimate. Moreover, we carried out a separate analysis according to the outcome measure, i.e., incidence and mortality separately.
Publication bias was assessed by visual inspection of funnel plot and by using the Egger’s test (Egger et al. 1997) for asymmetry when at least 10 studies by job or industry and neoplasm type were available (Higgins and Green 2011).
Results
The detailed flow chart of the selection of studies is reported in Fig. 1. A total of 1183 unique papers were identified through database searching. After the exclusion of non-relevant references, 91 articles were assessed for eligibility. Among them, 41 original articles were included in the meta-analysis. A list of excluded articles with reasons for exclusion is given in the Online resource 2.

Flow chart of study selection
Aluminum production
Table 1 gives the main characteristics of 11 studies (Milham 1979; Rochette 1983; Mur et al. 1987; Seldén et al. 1997; Romundstad et al. 2000; Carta et al. 2004; Spinelli et al. 2006; Björ et al. 2008; Sim et al. 2009; Scarnato 2013; Gibbs et al. 2014) reporting incidence or mortality from lymphatic and hematopoietic neoplasms in workers employed in aluminum production plants. Two out of eleven studies found a significant excess risk. Milham (1979) reported a significant increased mortality from NHL (7 cases, SMR 3.16, 95 % CI 1.28–6.55) among 2103 US workers employed in a prebake-type aluminum reduction plant between 1946 and 1962 and followed-up until 1976. Carta et al. (2004) found a significant excess mortality from all lymphatic and hematopoietic neoplasms (8 cases, SMR 2.03, 95 % CI 1.03–4.00) in a cohort of 1152 Italian men workers employed for at least 1 year between 1972 and 1980 in a prebake smelter and followed-up until 2001.
Overall, there were 30 HL cases, 167 NHL cases, 68 MM cases and 112 leukemia cases. Meta-analytic estimates showed a slight borderline significant excess risk of NHL (meta-RR 1.19, 95 % CI 0.98–1.44) among workers employed in aluminum production, while the results for HL (meta-RR 1.20, 95 % CI 0.84–1.72), MM (meta-RR 1.18, 95 % CI 0.93–1.50) and leukemia (meta-RR 1.10, 95 % CI 0.89–1.35) were less indicative of a possible association (Fig. 2).

Results of the meta-analysis: meta-analytic relative risk of lymphatic and hematopoietic neoplasms by job or industry
A moderate between-study heterogeneity was found only for NHL (I 2 = 33 %, P = 0.16). The exclusion of the study by Romunstad et al. 2000, reporting 35 incident cases of NHL led to a significant meta-analytic estimate (meta-RR 1.26, 95 % CI 1.03–1.53) (Online resource 3).
Stratified analysis by outcome measure showed no significant increased risk of HL, multiple myeloma and leukemia for both incidence and mortality (Online resource 4). In contrast, a moderate excess risk of NHL of borderline significance was observed from studies based on mortality (meta-RR 1.30, 95 % CI 1.00–1.68, based on 107 deaths), whereas no association emerged from studies based on incidence (meta-RR 1.01, 95 % CI 0.87–1.18, based on 169 cases).
Iron and steel foundry workers
Table 2 shows the main characteristics of the 12 studies (Decoufle 1979; Andjelkovich 1990; Moulin et al. 1990; Sherson et al. 1991; Rotimi et al. 1993; Sorahan et al. 1994; Hansen 1997; Firth et al. 1999; Park et al. 2005; Hoshuyama 2006; Westberg et al. 2013; Yoon and Ahn 2014) investigating incidence or mortality from lymphatic and hematopoietic neoplasms in foundry workers. An excess risk of leukemia was reported in a cohort study of 5245 workers hired before 1980 at the Anshan Iron and Steel Company located in the northeastern China and followed-up until 1993 (12 cases, SMR 1.98, 95 % CI 1.09–3.60) (Hoshuyama 2006).
Overall, these studies reported 27 HL cases, 57 NHL cases, 23 MM cases and 103 leukemia cases. Meta-analytic estimates indicate a possible association, although non-significant, for HL (meta-RR 1.38, 95 % CI 0.95–2.01), while no association emerges for NHL (meta-RR 0.94, 95 % CI 0.73–1.22), MM (meta-RR 1.00, 95 % CI 0.67–1.51) and leukemia (meta-RR 1.13, 95 % CI 0.93–1.39) (Fig. 2).
No significant between-study heterogeneity was observed for all the meta-analytic estimates.
Visual inspection of the funnel plot and the Egger’s test (P = 0.95) did not suggest publication bias in the meta-analytic estimate of leukemia risk (Online resource 5).
Meta-analytic estimates obtained by excluding the only one study (Westberg et al. 2013) reporting incidence did not significantly change the results of the main analysis (Online resource 4).
Coke workers
The main characteristic of the 6 studies (Davies 1977; Redmond 1979; Swaen et al. 1991; Franco 1993; Costantino 1995; Bye et al. 1998) on coke workers are reported in Table 3.
Only one study from Netherlands, that evaluated the risk of lymphatic and hematopoietic neoplasms in 5659 workers, reported a non-significant excess risk for NHL (4 cases, SMR 3.07, 95 % CI 0.84–7.86) and leukemia (6 cases, SMR 1.63, 95 % CI 0.60–3.55) in coke oven workers and an increased risk for HL in by-products workers (6 cases, SMR 1.86, 95 % CI 0.68–4.05) (Swaen et al. 1991).
Our meta-analysis did not suggest an excess risk either for leukemia (meta-RR 1.16, 95 % CI 0.68–1.98) or for all hematopoietic neoplasms (meta-RR 1.19, 95 % CI 0.91–1.55), although results are based on only 13 leukemia cases and 55 cases of all lymphatic and hematopoietic neoplasms. No significant heterogeneity among studies was found (Fig. 2).
When we omitted the study by Bye et al. (1998) reporting incidence data, the results did not materially change (meta-RR for all lymphatic and hematopoietic neoplasms: 1.22, 95 % CI 0.92–1.60) (Online resource 4).
Workers in plant of carbon electrode manufacturing
The main characteristic of the 6 studies (Teta et al. 1987; Moulin et al. 1989; Gustavsson 1995; Donato et al. 2000; Mori 2002; Merlo et al. 2004) on carbon electrode manufacturing workers are reported in Table 3. A non-significant excess risk of lymphatic and hematopoietic neoplasms was reported in a cohort of 2213 US workers at work in 1974 and followed-up until 1983 (Teta et al. 1987) (12 cases, SMR 1.76, 95 % CI 0.91–3.08) and in a small cohort of 332 Japanese workers employed for more than 5 years between 1951 and 1974 in a graphite electrode manufacturing plant which had been in operation since 1934 in Nishinomiya City and followed-up until 1988 (4 cases, SMR 3.46, 95 % CI 0.94–8.86) (Mori 2002).
Meta-analytic estimate did not show a significant excess risk of all lymphatic and hematopoietic neoplasms (meta-RR 1.14, 95 % CI 0.68–1.89, based on 30 cases). However, the I 2 statistic (I 2 = 51 %, P = 0.08) and the leave-one-out sensitivity analysis indicated a moderate between-study heterogeneity. In fact, the exclusion of the study by Moulin et al. (1989), reporting incidence, resulted in a borderline significant increased risk of all lymphatic and hematopoietic neoplasms (meta-RR 1.53, 95 % CI 0.99–2.37, based on 29 deaths) (Online resource 3). Similarly, excluding the study by Donato et al. (2000), the meta-RR for all lymphatic and hematopoietic neoplasms was 1.67 (95 % CI 0.98–2.85) (Online resource 3).
Asphalt workers and roofers
Table 4 gives the main characteristic of the 3 studies (Hammond et al. 1976; Swaen and Slangen 1997; Boffetta et al. 2003) focused on asphalt workers and roofers included in the meta-analysis. Notably, an international epidemiological studies carried out in seven European countries and in Israel (Boffetta et al. 2003) including a total of 29,820 male asphalt workers did not find an excess significant risk of all lymphatic and hematopoietic neoplasms considered (SMR for HL, 1.24 95 % CI 0.54–2.45, SMR for NHL, 0.78 95 % CI 0.49–1.17, SMR for multiple myeloma, 0.70 95 % CI 0.36–1.22, SMR for leukemia, 0.78, 95 % CI 0.52–1.12).
No significant excess risk was observed (Fig. 2) when pooling the results of 2 studies for HL (Swaen and Slangen 1997; Boffetta et al. 2003) (meta-RR 1.24, 95 % CI 0.64–2.44, based on 8 cases), 2 studies for NHL (Swaen and Slangen 1997; Boffetta et al. 2003) (meta-RR 1.22, 95 % CI 0.38–3.94, based on 25 cases), 2 (Swaen and Slangen 1997; Boffetta et al. 2003) studies for MM (meta-RR 0.72, 95 % CI 0.42–1.23, based on 13 cases) and 3 studies (Hammond et al. 1976; Swaen and Slangen 1997; Boffetta et al. 2003) for leukemia (meta-RR 1.15, 95 % CI 0.64–2.05, based on 44 cases).
Between-study heterogeneity was found for NHL and leukemia, but data were scanty and did not allow to investigate possible sources of between-study heterogeneity.
Workers in tar distilleries
The main characteristics of the two studies (Moulin et al. 1988; Swaen and Slangen 1997) in tar distillery workers are reported in Table 4. A study from France on 983 workers employed before 1970 and followed-up until 1984 did not report any cases of leukemia (Moulin et al. 1988). Three leukemia cases and no cases of HL, NHL or MM were observed in a study from Netherlands on 907 workers employed between 1947 and 1980 and followed-up until 1988 (Swaen and Slangen 1997).
No significant excess risk was found pooling the results of two studies that reported a total of 3 cases of leukemia among tar distillery workers (meta-RR 0.99, 95 % CI 0.35–2.83) (Fig. 2).
Workers exposed to creosote
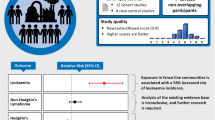
The main characteristics of the two studies (Karlehagen et al. 1992; Wong and Harris 2005) on creosote-exposed workers are reported in Table 4. The study by Karlehagen et al. 1992 included 922 men workers employed for least 1 year during the period 1950–1975 at 13 plants in Sweden and Norway. A non-significant excess risk of HL (2 observed cases, SIR 2.00, 95 % CI 0.24–7.23) and NHL (6 observed cases, SIR: 1.89, 95 % CI 0.69–412) were found, while no increased risk of leukemia was reported on the basis of 2 observed cases (SIR 0.64, 95 % CI 0.08–2.31). The more recent retrospective cohort study by Wong and Harris 2005 conducted on 2179 employees in 11 US plants observed a non-significant excess risk of all lymphatic and hematopoietic neoplasms combined (13 observed deaths, SMR 1.80, 95 % CI 0.72–3.71) and a significant excess risk of MM only in a cohort of hourly workers (6 observed deaths, SMR 4.01, 95 % CI 1.47–8.73). These workers were involved in a broad range of production and maintenance activities, with a higher potential for exposure to wood preservatives than the salaried employees.
The meta-analytic estimates did not indicate any increased risk of leukemia (meta-RR 1.27, 95 % CI 0.45–3.55, based on 7 cases), while a borderline significant excess risk of NHL emerged (meta-RR 2.01, 95 % CI 0.96–4.22, based on 7 cases) (Fig. 2).
Discussion
Our meta-analysis indicates that in general workers whose jobs entail a high PAH exposure did not have a significant excess risk of lymphatic and hematopoietic neoplasms.
Meta-analytic estimates suggest a possible association for some combinations of neoplasm and job or industry, such as workers exposed to creosote or aluminum workers and risk of NHL, or foundry workers and risk of HL. However, these associations did not reach the level of statistical significance.
To our knowledge, this is the first attempt to pool quantitatively the existing data on the association between occupational activities related to high PAH exposure and lymphatic and hematopoietic neoplasms. The existing data come from individual studies that for the most part have low power to detect any association, since the incidence of these neoplasms is relatively low. Therefore, our meta-analysis was able to quantify an association that single studies could not adequately estimate by substantially increasing the number of cases.
Only 4 studies out of the 41 studies identified in this meta-analysis found a significant increased risk of lymphatic and hematopoietic neoplasms: 2 articles that reported excess risk of all lymphatic and hematopoietic neoplasms in aluminum plant workers (Milham 1979; Carta et al. 2004), one study that found increased risk of leukemia in iron and steel foundry workers (Hoshuyama 2006) and one study that found excess risk of MM in creosote-exposed workers (Wong and Harris 2005). Moreover, in the study by Spinelli et al. (2006) on aluminum plant workers NHL risk increased with increasing levels of benzo-(alfa)-pyrene (BaP) in workplace air, suggesting a dose-risk relationship.
In our meta-analysis, we could not verify a dose-risk relationship because only a minority of the studies included in the meta-analysis quantified PAH exposure through environmental or biological monitoring (Moulin et al. 1989; Gustavsson 1995; Bye et al. 1998; Romundstad et al. 2000; Mori 2002; Carta et al. 2004; Spinelli et al. 2006). However, a reliable quantification of PAH exposure on individual basis is challenging since exposure levels vary depending on industry, work category, country and time period. Some workers may have changed their work category even in the same industry and then may have been exposed to different amount of PAH during the period of observation.
Air sampling data from some of the studies included in the meta-analysis showed a high inhalation exposure in the aluminum production industry, with air PAH concentrations up to 1000 µg/m3 in the work environment of some job categories employed in plant operating the Soderberg process prior to 1985 (Romundstad et al. 2000), while levels ranged up to 41.8 µg/m3 for total PAHs and 1.9 µg/m3 for BaP in an aluminum production plant operating in Italy since 1972 (Carta et al. 2004). In a coke plant in Norway that operated from 1964 to 1988, the PAH levels ranged between 0 and 300 μg/m3 (Bye et al. 1998), and there was some evidence of a trend toward lower exposures over time in western Europe and the US, but no adequate estimates were available from Asian and eastern European countries (IARC 2010). Exposure to PAH differed considerably between and within graphite electrode plant. BaP mean levels have been reported to vary between 0.46 μg/m3 in one French plant (Moulin et al. 1989), 11.5 μg/m3 in a Japanese plant (Mori 2002), and 40 μg/m3 a Swedish plant (Gustavsson 1995).
Studies not included in the meta-analysis suggest high PAHs exposure also in foundry workers, with a Danish study reporting a mean total PAHs air concentration of 10.5 µg/m3 (Omland et al. 1994), and in paving and roofing involving coal-tar pitch, where exposures varied widely between sites (IARC 2010). In one study (Zey 1983), the majority of exposures were below the limits of detection; in another study (Behrens and Liss 1984), exposures ranged up to 64.5 μg/m3 for BaP.
The advances in technology reduced considerably PAH exposure (Romundstad et al. 2000), however, some job categories are still exposed to high PAH levels, even in a recent period (Unwin et al. 2006).
Moreover, some industries, such as iron, steel, aluminum and asphalt industry, entail exposure to other carcinogens beyond PAH, including formaldehyde, aromatic amines, benzene and asbestos (Seldén et al. 1997; Westberg et al. 2013).
We were unable to control for potential confounding factors, such as socioeconomic status, infections and other environmental factors, or because the information was not available or because was not used in the analysis due to the small number of cases (Spinelli et al. 2006). Socioeconomic conditions and prevalence of lifestyle and environmental risk factors are likely to differ among local areas, and the choice of regional or national population as reference might have biased the results. To avoid potential problems related to the use of the national population as reference, a few studies used workers who had the same employment process but a different exposure status: from three of these studies on foundry workers generally emerged an excess risk (Hansen 1997; Hoshuyama 2006; Yoon and Ahn 2014) while three studies on coke workers reported inconsistent results (Redmond 1979; Swaen et al. 1991; Costantino 1995).
Despite including all available studies, the limited number of cases gathered in this meta-analysis might have not allowed to detect relatively small risk differences among workers exposed to PAHs. This is particularly true for the risk of MM in foundries, leukemia in coke plants and tar distilleries and NHL and leukemia in creosote-exposed workers, where the number of observed cases was below 20. The small number of cases prevented us to carry out subgroup analyses by country, time period, reference population, period of employment, duration of exposure or job category.
Although we did not found definite evidence of an association between any occupational exposure to PAH and risk of any lymphatic and hematopoietic neoplasm, future studies should evaluate dose-risk relationships on the basis of additional follow-up and should be focused on those workers with very high PAH exposure.
In conclusion, the results of our meta-analysis and the epidemiological evidence available up to date do not support a significant excess risk of lymphatic and hematopoietic neoplasms among workers whose job entails a high PAH exposure.
References
Andjelkovich D (1990) Mortality of iron foundry workers. J Occup Med 32:529–540
Behrens V, Liss G (1984) Fisher Body Plant, Roofing Site, Hamilton, Ohio (Health Hazard Evaluation Report, No. HETA-84-062-1552), National Institute of Occupational Safety and Health, Cincinnati, OH
Björ O, Damber L, Edström C, Nilsson T (2008) Long-term follow-up study of mortality and the incidence of cancer in a cohort of workers at a primary aluminum smelter in Sweden. Scand J Work Environ Health 34:463–470. doi:10.5271/sjweh.1293
Boffetta P, Jourenkova N, Gustavsson P (1997) Cancer risk from occupational and environmental exposure to polycyclic aromatic hydrocarbons. Cancer Causes Control 8:444–472
Boffetta P, Burstyn I, Partanen T et al (2003) Cancer mortality among European asphalt workers: an international epidemiological study. II. Exposure to bitumen fume and other agents. Bitumen 43:18–27
Burchiel SW, Luster MI (2001) Signaling by environmental polycyclic aromatic hydrocarbons in human lymphocytes. Clin Immunol 98:2–10. doi:10.1006/clim.2000.4934
Bye T, Romundstad PPR, Rønneberg A, Hilt B (1998) Health survey of former workers in a Norwegian coke plant: part 2. Cancer incidence and cause specific mortality. Occup Environ Med 55:622–626
Carta P, Aru G, Cadeddu C et al (2004) Mortality for pancreatic cancer among aluminium smelter workers in Sardinia, Italy. G Ital Med Lav Ergon 26:83–89
Costantino J (1995) Occupationally related cancer risk among coke oven workers: 30 years of follow up. J Occup Environ Med 37:597–604. doi:10.1017/CBO9781107415324.004
Davies GM (1977) A mortality study of coke oven workers in two South Wales integrated steelworks. Br J Ind Med 34:291–297
Decoufle P (1979) Mortality patterns among workers in a gray iron foundry. Am J Epidemiol 109:667–675
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7(3):177–188. doi:10.1016/0197-2456(86)90046-2
Donato F, Monarca S, Marchionna G et al (2000) Mortality from cancer and chronic respiratory diseases among workers who manufacture carbon electrodes. Occup Environ Med 57:484–487
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634. doi:10.1136/bmj.316.7129.469
Firth HM, Elwood JM, Cox B, Herbison GP (1999) Historical cohort study of a New Zealand foundry and heavy engineering plant. Occup Environ Med 56(2):134–138
Franco F (1993) Mortality in the coke oven plant of Carrara, Italy. Med del Lav 84:443–447. doi:10.1017/CBO9781107415324.004
Gibbs GW, Labrèche F (2014) Cancer risks in aluminum reduction plant workers. J Occup Environ Med 56:S40–S59
Gibbs GW, Labrèche F, Busque M-A, Duguay P (2014) Mortality and cancer incidence in aluminum smelter workers: a 5 year update. J Occup Environ Med 56:739–764
Gustavsson P (1995) Surveillance of mortality and cancer incidence among swedish graphite electrode workers. Environ Res 70:7–10
Hammond EC, Selikoff IJ, Lawther PL, Seidman H (1976) Inhalation of benzpyrene and cancer in man. Ann NY Acad Sci 271:116–124
Hansen ES (1997) A cohort mortality study of foundry workers. Am J Ind Med 32:223–233
Higgins J, Green S (eds) (2011) Cochrane handbook for systematic reviews of interventions version 5.1.0 [updated March 2011]. The cochrane collaboration. www.cochrane-handbook.org
Higgins JPT, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560. doi:10.1136/bmj.327.7414.557
Hoshuyama T (2006) Mortality of iron–steel workers in Anshan, China: a retrospective cohort study. J Univ Occup Environ Health 12:193–202
IARC (2010) IARC monographs on the evaluation of carcinogenic risks to humans: some non-heterocyclic polycyclic aromatic hydrocarbons and some related exposures. Iarc Monogr Eval Carcinog Risks Hum 92:1–868
Jongeneelen FJ (2001) Benchmark guideline for urinary 1-hydroxypyrene as biomarker of occupational exposure to polycyclic aromatic hydrocarbons. Ann Occup Hyg 45:3–13. doi:10.1016/S0003-4878(00)00009-0
Karlehagen S, Andersen A, Ohlson CG (1992) Cancer incidence among creosote-exposed workers. Scand J Work Environ Health 18:26–29. doi:10.5271/sjweh.1612
Merlo DF, Garattini S, Gelatti U et al (2004) A mortality cohort study among workers in a graphite electrode production plant in Italy. Occup Environ Med. doi:10.1136/oem.2003.009357
Milham S (1979) Mortality in aluminum reduction plant workers. J Occup Environ Med 21:475–480. doi:10.1017/CBO9781107415324.004
Mori I (2002) Cancer mortality among man-made graphite electrode manufacturing workers: results of 38 year follow up. Occup Env Med 59:473–480. doi:10.1136/oem.59.7.473
Moulin J, Mur J, Wild P et al (1988) Mortality study among coal tar distillery workers. Rev Epidemiol Santé Publ 36:99–107
Moulin JJ, Wild P, Mur JM et al (1989) Risk of lung, larynx, pharynx and buccal cavity cancers among carbon electrode manufacturing workers. Scand J Work Environ Health 15:30–37. doi:10.5271/sjweh.1885
Moulin JJ, Portefaix P, Wild P et al (1990) Mortality study among workers producing ferroalloys and stainless steel in France. Br J Ind Med 47:537–543. doi:10.1136/oem.47.8.537
Mur JM, Moulin JJ, Meyer-Bisch C et al (1987) Mortality of aluminium reduction plant workers in France. Int J Epidemiol 16:257–264
Omland O, Sherson D, Hansen AM et al (1994) Exposure of iron foundry workers to polycyclic aromatic hydrocarbons: benzo(a)pyrene-albumin adducts and 1-hydroxypyrene as biomarkers for exposure. Occup Environ Med 51:513–518
Park RM, Ahn YS, Stayner LT et al (2005) Mortality of iron and steel workers in Korea. Am J Ind Med 48:194–204. doi:10.1002/ajim.20197
Redmond C (1979) Cancer experience among coke by-product workers. J Environ Pathol Toxicol 2:75–96
Rochette HE (1983) Mortality studies among aluminum plant workers: potrooms and carbon department. J Occup Med 25:549–557
Romundstad P, Andersen A, Haldorse T (2000) Cancer incidence among workers in the Norwegian silicon carbide industry. Am J Epidemiol 153:978–986. doi:10.1093/aje/153.10.978
Rota M, Bosetti C, Boccia S et al (2014) Occupational exposures to polycyclic aromatic hydrocarbons and respiratory and urinary tract cancers: an updated systematic review and a meta-analysis to 2014. Arch Toxicol 88:1479–1490. doi:10.1007/s00204-014-1296-5
Rotimi C, Austin H, Delzell E et al (1993) Retrospective follow-up study of foundry and engine plant workers. Am J Ind Med 24:485–498
Scarnato C (2013) Mortality study in secondary aluminum foundry workers. Eur J Oncol 17:205–212. doi:10.1017/CBO9781107415324.004
Seldén AI, Westberg HB, Axelson O (1997) Cancer morbidity in workers at aluminum foundries and secondary aluminum smelters. Am J Ind Med 32:467–477
Sherson D, Svane O, Lynge E (1991) Cancer incidence among foundry workers in denmark. Arch Environ Health Int J 46:75–81
Sim MR, Del Monaco A, Hoving JL et al (2009) Mortality and cancer incidence in workers in two Australian prebake aluminium smelters. Occup Environ Med 66:464–470
Sorahan T, Faux AM, Cooke MA (1994) Mortality among a cohort of United Kingdom steel foundry workers with special reference to cancers of the stomach and lung, 1946–90. Occup Environ Med 51:316–322
Spinelli JJ, Demers PA, Le ND et al (2006) Cancer risk in aluminum reduction plant workers (Canada). Cancer Causes Control 17:939–948
Stroup DF, Berlin JA, Morton SC et al (2011) Meta-analysis of observational studies. JAMA 283:2008–2012. doi:10.1001/jama.283.15.2008
Swaen GMH, Slangen JMM (1997) Mortality in a group of tar distillery workers and roofers. Int Arch Occup Environ Health 70:133–137. doi:10.1007/s004200050197
Swaen GM, Slangen JJ, Volovics A et al (1991) Mortality of coke plant workers in The Netherlands. Br J Ind Med 48:130–135. doi:10.1136/oem.48.2.130
Teta MJ, Ott MG, Schnatter AR (1987) Population based mortality surveillance in carbon products manufacturing plants. Br J Ind Med 44:344–350
Unwin J, Cocker J, Scobbie E, Chambers H (2006) An assessment of occupational exposure to polycyclic aromatic hydrocarbons in the UK. Ann Occup Hyg 50:395–403. doi:10.1093/annhyg/mel010
Wagner M, Bolm-Audorff U, Hegewald J, Fishta A, Schlattmann P, Schmitt J, Seidler A (2015) Occupational polycyclic aromatic hydrocarbon exposure and risk of larynx cancer: a systematic review and meta-analysis. Occup Environ Med 72(3):226–233
Westberg H, Andersson L, Bryngelsson IL et al (2013) Cancer morbidity and quartz exposure in Swedish iron foundries. Int Arch Occup Environ Health 86:499–507
Wong O, Harris F (2005) Retrospective cohort mortality study and nested case-control study of workers exposed to creosote at 11 wood-treating plants in the United States. J Occup Environ Med 47:683–697
Yoon JH, Ahn YS (2014) Cause-specific mortality due to malignant and non-malignant disease in Korean foundry workers. PLoS ONE. doi:10.1371/journal.pone.0088264
Zey JN (1983) Roofing Construction, Houston, Texas (Health Hazard Evaluation Report No. HETA-83-210-1887), National Institute of Occupational Safety and Health, Cincinnati, OH
Acknowledgments
MR received a fellowship from the Italian Foundation for Research on Cancer (FIRC).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Alicandro, G., Rota, M., Boffetta, P. et al. Occupational exposure to polycyclic aromatic hydrocarbons and lymphatic and hematopoietic neoplasms: a systematic review and meta-analysis of cohort studies. Arch Toxicol 90, 2643–2656 (2016). https://doi.org/10.1007/s00204-016-1822-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00204-016-1822-8