
Abstract
Summary
The Danish Fracture Risk Evaluation Model (FREM) was found to predict fracture risk independent of 10-year fracture probability derived with the FRAX® tool including bone mineral density from DXA.
Introduction
FREM was developed from Danish public health registers without DXA information to identify high imminent risk of major osteoporotic fracture (MOF) and hip fracture (HF), while FRAX® estimates 10-year fracture probability from clinical risk factors and femoral neck bone mineral density (BMD) from DXA. The FREM algorithm showed significant 1- and 2-year fracture risk stratification when applied to a clinical population from Manitoba, Canada. We examined whether FREM predicts 10-year fracture risk independent of 10-year FRAX probability computed with BMD.
Methods
Using the Manitoba BMD Program registry, we identified women and men aged ≥ 45 years undergoing baseline BMD assessment. We calculated FREM and FRAX scores, and identified incident fractures over 10 years. Hazard ratios (HRs) for incident fracture were estimated according to FREM quintile, adjusted for FRAX probability. We compared predicted with observed 10-year cumulative fracture probability estimated with competing mortality.
Results
The study population comprised 74,446 women, mean age 65.2 years; 7945 men, mean age 67.5 years. There were 7957 and 646 incident MOF and 2554 and 294 incident HF in women and men, respectively. Higher FREM scores were associated with increased risk for MOF (highest vs middle quintile HRs 1.49 women, 2.06 men) and HF (highest vs middle quintile HRs 2.15 women, 2.20 men) even when adjusted for FRAX. Greater mortality with higher FREM scores attenuated its effect on 10-year fracture probability. In the highest FREM quintile, observed slightly exceeded predicted 10-year probability for MOF (ratios 1.05 in women, 1.49 in men) and HF (ratios 1.29 in women, 1.34 in men).
Conclusions
Higher FREM scores identified women and men at increased fracture risk even when adjusted for FRAX probability that included BMD; hence, FREM provides additional predictive information to FRAX. FRAX slightly underestimated 10-year fracture probability in those falling within the highest FREM quintile.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is characterized by bone fragility and susceptibility to fracture, with substantial health consequences for the individual and society [1]. Although historically osteoporosis has been diagnosed from a bone mineral density (BMD) T-score, in recent years, there has been a shift towards the use of multifactorial fracture prediction tools which typically include BMD in addition to other clinical risk factors [2]. Targeting individuals at high fracture risk for anti-osteoporosis therapy translates into a larger number of fractures prevented (with a lower number needed to treat) compared with treatment based upon BMD alone [3, 4].
The FRAX® tool estimates 10-year fracture probability for major osteoporotic fracture (MOF) and hip fracture (HF) based upon age, sex, a small number of clinical risk factors, and (optionally) femoral neck BMD [5]. The only medical condition considered by FRAX when BMD is included in the calculation is rheumatoid arthritis. A diverse range of “secondary osteoporosis” diagnoses is considered when BMD is unknown and is assumed to mediate their effects through a reduction in BMD. Whether medical diagnoses other than rheumatoid arthritis significantly impact fracture risk independent of FRAX is currently uncertain. Some specific conditions, such as type 2 diabetes mellitus and multiple sclerosis, are FRAX- and BMD-independent risk factors for fracture [5, 6].
The Fracture Risk Evaluation Model (FREM) tool was developed for case-finding of individuals aged 45 years or older at high imminent (1 year) risk of MOF and/or HF [7]. The tool was developed and subsequently validated using administrative data from the Danish Health Registries. FREM consists of a weighted score including age and 38 MOF risk factors for women and 43 risk factors for men, and 32 HF risk factors for both women and men (a complete list is provided in Supplemental Table 1). BMD is not included in the FREM calculation. FREM has also been found to predict 5-year risk of MOF and HF [8]. We recently showed that the FREM algorithm showed significant 1-year and 2-year fracture risk stratification when applied to an independent clinical population from Manitoba, Canada [9]. In that study, FREM performed better than age alone but not as well as FRAX with BMD. Whether FREM, which reflects multiple comorbidities but does not consider BMD, provides fracture risk information independent from FRAX computed with BMD over 10 years has not been investigated. The current analysis was performed to examine whether FREM predicts 10-year incident fracture risk independent of FRAX probability, and might therefore be beneficial for risk stratification beyond FRAX (with BMD) alone.
Methods
Study design and population
The study population consisted of all women and men aged 45 years or older with baseline DXA scans recorded in the Manitoba BMD Program registry from January 1, 1996, to March 31, 2016. For those with more than one qualifying examination, only the first was included. DXA-based BMD testing has been managed as an integrated clinical program; criteria for testing have been published and included but are not restricted to the previous fracture, x-ray evidence of osteopenia, high-risk medication use (e.g., glucocorticoids, aromatase inhibitors), conditions associated with osteoporosis (e.g., premature menopause, celiac disease), and age ≥ 65 years in the absence of additional risk factors (for women only) [10]. The DXA database has completeness and accuracy in excess of 99% [11].
The program database of all DXA results has been linked with other provincial population-based computerized health databases through an anonymous personal identifier. Comprehensive healthcare databases in the Manitoba Centre for Health Policy Data Repository include hospitalization discharge summaries, physician claims for services (billings), and vital statistics. Virtually, all residents of the Province of Manitoba, Canada, (population 1.3 million) receive health coverage through a publicly funded system, and encounters with the healthcare system are recorded in these databases. The accuracy and completeness of these databases for fractures have been described elsewhere [12, 13]. This study was approved by the Health Research Ethics Board of the University of Manitoba, and data access was granted by the Health Information Privacy Committee of Manitoba.
Estimation of fracture risk from FREM and FRAX
One-year predicted incidence of MOF and HF after index date was calculated with FREM using up to 10 years of prior hospital and physician claims data (implemented using SAS version 9.4, SAS Institute Inc., Cary, NC, USA) as previously described [9]. Over 93% of the included individuals had at least 10 years of coverage and registry data before their baseline assessment. Each condition considered by FREM was assessed through a combination of hospital discharge abstracts (diagnoses and procedures coded using the International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] prior to 2004 and International Classification of Diseases, Tenth Revision, Canadian Enhancements [ICD-10-CA] thereafter) and physician billing claims (out-patient or in-patient, coded using ICD-9-CM in all years). Crosswalk tables were generated for ICD-9-CM and ICD-10 codes. Each condition was entered as present if there was a single hospitalization diagnosis or multiple physician claims diagnoses (2 or more within a 3-year time period). FREM scores were created based upon hospitalization records (in-patients only) alone (denoted FREM (H)), physician claims alone (FREM (P)), or the combination (FREM (HP)). The coefficients in the Danish FREM score calculation were based on hospital in- and out-patient consults as previously described applying an ICD-9-CM/ICD-10 crosswalk to translate the ICD codes included in FREM [7]. We used all of the original FREM risk factors and their coefficients without modification. FREM was categorized into quintiles (cutoffs for the quintile definitions are provided in Supplemental Table 2). We designated the middle tertile as the referent category since this reflects average comorbidity in the population, whereas lower comorbidity and higher comorbidity (lower and higher tertiles) were hypothesized to be associated with lower and higher risk, respectively.
Ten-year probability of a MOF and HF were calculated using the Canadian FRAX tool (FRAX® Desktop Multi-Patient Entry, version 3.8) as recently described [14]. The Canadian FRAX tool was calibrated using nationwide hip fracture and mortality data [15] and independently validated in the general population [16, 17]. Femoral neck BMD was included in the calculation from hip DXA scans that were performed and analyzed in accordance with manufacturer recommendations. All reporting physicians and supervising technologists are required to maintain DXA certification with the International Society for Clinical Densitometry (ISCD). The program’s quality assurance is under strict supervision by a medical physicist [10]. The seven cross-calibrated instruments used for this study (1 DPX, 3 Prodigy, and 3 iDXA, GE/Lunar Healthcare, Madison WI) exhibited equivalent phantom and in vivo calibration (T-score differences < 0.1), with stable long-term performance (coefficient of variation [CV] < 0.5%) and good in vivo femoral neck BMD reproducibility (test–retest CV 2.3%).
Incident fracture ascertainment
Manitoba Health hospital discharge abstracts and physicians claims records in the study population were assessed for the presence of MOF (hip, forearm, clinical vertebral, humerus) diagnosis codes following the BMD assessment up to March 31, 2018, limited to the first 10 years of follow-up, using previously validated algorithms [18, 19]. In addition, hip and forearm fractures were required to have concurrent claims for site-specific orthopedic fixation, reduction, or casting to enhance specificity for an acute fracture event. Traumatic fractures identified using trauma diagnosis codes were excluded from the analyses.
Statistical analysis
All analyses were stratified by sex and baseline age (below age 65 years versus age 65 years and above). Continuous variables were reported as means with standard deviations (SDs) for normally distributed and median (interquartile range) for non-normally distributed variables, and as frequencies with percentages for categorical variables. Pearson correlation coefficients for FRAX and FREM probability measurements were estimated on the log–log scale. We estimated hazard ratios (HRs) with 95% confidence intervals (CI) by Cox regression for incident fracture according to the FREM quintile (referent middle quintile), unadjusted and adjusted for FRAX probability as a continuous covariate (log-transformed due to a skewed distribution). Variance inflation factors in the models were all less than 4, which excluded problematic collinearity between FREM and FRAX [20]. FRAX considers competing mortality and we hypothesized that greater mortality associated with higher FREM scores (greater comorbidity) might mitigate effects on 10-year fracture risk estimated under the FRAX framework. Therefore, we also estimated FRAX-adjusted HRs for death according to the FREM quintile. Finally, we compared predicted with observed 10-year cumulative fracture probability, estimated with competing mortality [21], within each FREM quintile, and estimated calibration ratios with 95% CIs. All statistical analyses were performed with Statistica (Version 13.0, StatSoft Inc, Tulsa, OK).
Results
The characteristics of women and men are summarized in Table 1. The study population comprised 74,446 women, mean age 65.2 years; 7945 men, mean age 67.5 years. There were moderate positive correlations between FREM and FRAX, higher in women versus men (r range 0.67–0.75 for MOF, 0.43–0.59 for hip, all p < 0.001, Supplemental Table 3). During follow-up, there were 7957 and 646 MOF and 2554 and 294 HF in women and men, respectively.
Compared to women and men without incident fracture, incident MOF and incident HF were associated with older age, lower femoral neck T-score, higher FRAX probability, and higher FREM probability (all p < 0.001). A monotonic increase in proportion and rate of incident MOF and HF was seen in women and men with increasing FREM risk quintile, overall and age-stratified (Supplemental Table 4).
Table 2 shows the effect of the FREM quintile on fracture risk after adjusting for FRAX probability, with the middle quintile serving as the referent (unadjusted results in Supplemental Table 5). For FREM (HP), there was a significantly increased risk for MOF among women and men in quintile 4 (HR 1.14, 95% CI 1.06–1.22; 1.46, 95% CI 1.15–1.86) and quintile 5 (HR 1.49, 95% CI 1.38–1.61; 2.06, 95% CI 1.63–2.61) adjusted for FRAX probability. An even larger effect was seen for hip fracture risk, again significantly increased in women and men in quintile 4 (HR 1.44, 95% CI 1.26–1.65; 1.98, 95% CI 1.23–3.17) and quintile 5 (HR 2.15, 95% CI 1.88–2.45; 2.20, 95% CI 1.35–3.59). There was a tendency for HRs to be slightly reduced in quintiles 1 and 2, but this was only statistically significant for MOF risk in men in quintile 1 (HR 0.70, 95% CI 0.54–0.93). Similar trends were seen for FREM (HP) stratified by age (Supplemental Tables 6 and 7) and for FREM (H) and FREM (P) (Table 2).
The lower FREM quintile was associated with lower mortality risk while the higher FREM quintile was associated with increased mortality risk compared with the middle quintile (referent, Supplemental Table 8). FRAX-adjusted HRs for death in the lowest quintile of MOF FREM (HP) was 0.53 (95% CI 0.49–0.57) in women and 0.35 (95% CI 0.30–0.41) in men, versus elevated risk in the highest quintile for women HR 2.98 (95% CI 2.82–3.16) and men 2.83 (95% CI 2.53–3.18). Once again similar trends were seen for FREM (H) and FREM (P).
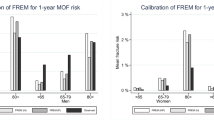
Figure 1 shows cumulative fracture probability for MOF and HF to 10 years (estimated with competing mortality) in women and men stratified by FREM (HP) quintile, both of which demonstrated a stepwise increase. Observed exceeded predicted FRAX 10-year fracture probability for MOF in women in quintile 5 (calibration ratio 1.05, 95% CI 1.01–1.09) and for men in quintile 4 (1.39, 95% CI 1.17–1.61) and quintile 5 (1.49, 95% CI 1.28–1.7). For hip fracture risk, observed exceeded predicted 10-year probability in women for quintile 4 (calibration ratio 1.27, 95% CI 1.15–1.39) and quintile 5 (1.29, 95% CI 1.21–1.37); for men in quintile 5 (1.34, 95% CI 1–1.67).

Predicted (FRAX with BMD) versus observed 10-year incident major osteoporotic fracture (MOF) and hip fracture (HF) risk by FREM (HP) quintile. Calibration ratios representing observed to expected fracture risk are provided with 95% confidence intervals (CI). CIs for FRAX-predicted risk are too small to plot
Discussion
We found that FREM scores that were higher than average (above the middle referent quintile) were associated with increased risk for MOF and hip fracture even after adjustment for FRAX probability with BMD. Hence, FREM provides additional predictive information for identifying high-risk individuals, even if FRAX estimates are known. The risk for the highest quintile was 49–115% greater in women and 106–120% higher for men using FREM (HP). Similar results were seen when FREM was implemented using hospitalization data alone or physician diagnoses alone. FREM score was strongly associated with mortality, and this attenuated its impact on 10-year fracture probability using a FRAX framework which includes competing mortality. Nonetheless, there were subgroups where a higher FREM score still resulted in a clinically meaningful increase in fracture risk above what was predicted from FRAX. This was particularly evident among men in the highest FREM quintile, who had a 49% greater MOF and 34% greater hip fracture risk than predicted from FRAX. There were more modest increases for women in the highest FREM quintile, 5% greater for MOF and 29% greater for hip fracture.
The FREM tool was initially developed for improved identification of individuals at high imminent (1 year) risk of fractures using administrative health data [7], and subsequently shown to predict MOF and hip fractures up to 5 years [8]. The current analysis extends the potential role of FREM as a risk prediction tool, demonstrating that it has utility over a 10-year time horizon. Although not all inputs to FRAX can be captured in population-level administrative data, FREM is a systems-based tool specifically developed for automation within electronic patient record systems using routinely collected population-level administrative data with no need for patient-level data collection. Therefore, depending on the healthcare system in question, FREM could be integrated into electronic patient record systems, or even deployed centrally in a national case-finding strategy to identify those at high fracture risk not receiving treatment for further evaluation. Moreover, by incorporating information on multiple medical diagnoses, it can be used in conjunction with FRAX to refine fracture risk stratification, in particular in individuals with multiple comorbidities not considered by FRAX. This is potentially advantageous where FREM is used as an initial screening tool at the population level since it continues to provide information regarding fracture risk even after BMD and other FRAX risk factors are available. The benefit of anti-fracture therapy in individuals identified as being at high risk from FREM is likely but remains to be directly tested. Population-based screening strategies using FRAX from clinical risk factors to select individuals for refined fracture risk assessment with BMD have been evaluated in three pragmatic clinical trials, and a meta-analysis showed a statistically and clinically significant reduction in all osteoporotic fractures, MOF and HF [22].
Strengths of the study include the large number of individuals for analysis and availability of population-based data linkage for assessment of diagnoses and outcomes. Although based upon a clinical registry, results are likely to be relevant to routine clinical practice since all individuals referred for BMD assessment are captured through the Manitoba BMD Program. Limitations are also acknowledged. Men referred for BMD testing are much more highly selected, and this could be contributing to the larger effects of FREM in men than women. The original FREM description was based upon 15 years of prior healthcare information, whereas the current calculation was based upon 10 years of healthcare information. Subsequent analyses have suggested that this is not critical, and that FREM shows a similar performance when applying a 15-year versus a 5-year look-back [8]. Fracture outcomes were assessed using hospital and physician diagnoses without direct review of x-rays, though definitions have been validated against x-ray in a subset as previously reported [18, 19]. Whether our results will generalize to other countries and populations with different prevalence of medical conditions and baseline fracture risk is uncertain.
In summary, higher FREM scores identified women and men at increased fracture risk even when adjusted for FRAX probability that included BMD. The FREM tool acts as a fracture modifier to 10-year fracture probability assessed with the FRAX tool, and hence FREM provides additional information for the prediction of fracture risk when combined with FRAX. This implies that capturing a wider range of medical conditions that are not currently considered by FRAX may have clinical utility. FRAX slightly underestimated 10-year fracture probability in those falling within the highest FREM quintile. Individuals in the highest FREM quintile will have a higher fracture risk than predicted by FRAX with BMD, and may warrant consideration of treatment, especially if they are only slightly below the intervention threshold.
Data availability
Data sharing is not permitted under the Researcher Agreement with Manitoba Health and Seniors Care (MHASC). However, researchers may apply for data access through the Health Research Ethics Board for the University of Manitoba and the Health Information and Privacy Committee of MHASC.
References
Compston JE, McClung MR, Leslie WD (2019) Osteoporosis. The Lancet 393:364–376
Beaudoin C, Moore L, Gagne M, Bessette L, Ste-Marie LG, Brown JP, Jean S (2019) Performance of predictive tools to identify individuals at risk of non-traumatic fracture: a systematic review, meta-analysis, and meta-regression. Osteoporos Int 30:721–740
Kanis JA, McCloskey EV, Harvey NC, Johansson H, Leslie WD (2015) Intervention thresholds and the diagnosis of osteoporosis. J Bone Miner Res 30:1747–1753
Leslie WD, Morin SN, Lix LM, Binkley N (2020) Comparison of treatment strategies and thresholds for optimizing fracture prevention in Canada: a simulation analysis. Arch Osteoporos 15:4
Kanis JA, Harvey NC, Johansson H, Liu E, Vandenput L, Lorentzon M, Leslie WD, McCloskey EV (2020) A decade of FRAX: how has it changed the management of osteoporosis? Aging Clin Exp Res 32:187–196
Bisson EJ, Finlayson ML, Ekuma O, Marrie RA, Leslie WD (2019) Accuracy of FRAX(R) in people with multiple sclerosis. J Bone Miner Res 6(34):1095–1100
Rubin KH, Möller S, Holmberg T, Bliddal M, Søndergaard J, Abrahamsen B (2018) A new fracture risk assessment tool (FREM) based on public health registries. J Bone Miner Res 33:1967–1979
Skjodt MK, Moller S, Hyldig N, Clausen A, Bliddal M, Sondergaard J, Abrahamsen B, Rubin KH (2021) Validation of the fracture risk evaluation model (FREM) in predicting major osteoporotic fractures and hip fractures using administrative health data. Bone 147:115934
Moller S, Skjodt MK, Yan L et al (2022) Prediction of imminent fracture risk in Canadian women and men aged 45 years or older: external validation of the Fracture Risk Evaluation Model (FREM). Osteoporos Int 33:57–66
Leslie WD, Metge C (2003) Establishing a regional bone density program: lessons from the Manitoba experience. J Clin Densitom 6:275–282
Leslie WD, Caetano PA, Macwilliam LR, Finlayson GS (2005) Construction and validation of a population-based bone densitometry database. J Clin Densitom 8:25–30
Roos LL, Mustard CA, Nicol JP, McLerran DF, Malenka DJ, Young TK, Cohen MM (1993) Registries and administrative data: organization and accuracy. MedCare 31:201–212
Roos LL, Walld RK, Romano PS, Roberecki S (1996) Short-term mortality after repair of hip fracture. Do Manitoba elderly do worse? MedCare 34:310–326
Leslie WD, Schousboe JT, Morin SN, Martineau P, Lix LM, Johansson H, McCloskey EV, Harvey NC, Kanis JA (2020) Measured height loss predicts incident clinical fractures independently from FRAX: a registry-based cohort study. Osteoporos Int 31(6):1079–1087
Leslie WD, Lix LM, Langsetmo L et al (2011) Construction of a FRAX(R) model for the assessment of fracture probability in Canada and implications for treatment. Osteoporos Int 22:817–827
Fraser LA, Langsetmo L, Berger C et al (2011) Fracture prediction and calibration of a Canadian FRAX® tool: a population-based report from CaMos. Osteoporos Int 22:829–837
Leslie WD, Lix LM, Johansson H, Oden A, McCloskey E, Kanis JA (2010) Independent clinical validation of a Canadian FRAX tool: fracture prediction and model calibration. J Bone Miner Res 25:2350–2358
Lix LM, Azimaee M, Osman BA, Caetano P, Morin S, Metge C, Goltzman D, Kreiger N, Prior J, Leslie WD (2012) Osteoporosis-related fracture case definitions for population-based administrative data. BMC Public Health 12:301
Leslie WD, Epp R, Morin SN, Lix LM (2021) Assessment of site-specific X-ray procedure codes for fracture ascertainment: a registry-based cohort study. Arch Osteoporos 16:107
Steyerberg EW (2008) Clinical prediction models: a practical approach to development, validation, and updating. Springer (New York),
Leslie WD, Lix LM, Wu X, Manitoba Bone Density P (2013) Competing mortality and fracture risk assessment. Osteoporos Int 24:681–688
Merlijn T, Swart KMA, van der Horst HE, Netelenbos JC, Elders PJM (2020) Fracture prevention by screening for high fracture risk: a systematic review and meta-analysis. Osteoporos Int 31:251–257
Acknowledgements
The authors acknowledge the Manitoba Centre for Health Policy (MCHP) for use of data contained in the Population Health Research Data Repository (HIPC Project Number 2016/2017-29). The results and conclusions are those of the authors, and no official endorsement by the MCHP, Manitoba Health and Seniors Care, or other data providers is intended or should be inferred. The results and conclusions are those of the authors, and no official endorsement by Manitoba Health and Seniors Care is intended or should be inferred. This article has been reviewed and approved by the members of the Manitoba Bone Density Program Committee.
Author information
Authors and Affiliations
Contributions
All authors substantially contributed to conception (WDL, BA) and design (WDL, BA), or analysis (WDL, LML, LY) and interpretation of data (all); drafting the article (WDL) or revising it critically for important intellectual content (all); and final approval of the version to be published (all). WDL accepts full responsibility for the work and/or the conduct of the study, had full access to all the data, and controlled the decision to publish.
Corresponding author
Ethics declarations
Conflicts of interest
Michael K. Skjødt: educational grant, UCB and institutional research grant, UCB/Amgen.
Eugene McCloskey: nothing to declare for the context of this paper, but numerous ad hoc consultancies/speaking honoraria and/or research funding from Amgen, Bayer, General Electric, GSK, Fresenius Kabi, Hologic, Lilly, Merck Research Labs, Novartis, Novo Nordisk, Nycomed, Ono, Pfizer, ProStrakan, Roche, Sanofi-Aventis, Servier, Tethys, UCB and Warner-Chilcott.
Nicholas Harvey: nothing to declare for the context of this paper, but has received consultancy/lecture fees/honoraria/grant funding from Alliance for Better Bone Health, Amgen, MSD, Eli Lilly, Servier, Shire, UCB, Consilient Healthcare, Radius Health, Kyowa Kirin and Internis Pharma.
Bo Abrahamsen: institutional research contracts with Novartis, UCB, Kyowa-Kirin. Fees or honoraria from UCB, Amgen, Pharmacosmos.
William Leslie, Lisa Lix, Lin Yan, Helena Johansson, John Kanis, Sören Möller, Katrine Hass Rubin: no conflicts of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Leslie, W.D., Möller, S., Skjødt, M.K. et al. FREM predicts 10-year incident fracture risk independent of FRAX® probability: a registry-based cohort study. Osteoporos Int 33, 1457–1463 (2022). https://doi.org/10.1007/s00198-022-06349-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-022-06349-3